Introduction
Intraosseous calcaneal lipoma was first described in
1976 (1). This type of lesion is a
rare benign bone tumor that is commonly asymptomatic, and is
usually incidentally discovered on radiographs performed for
unrelated disorders. Intraosseous calcaneal lipoma remains a poorly
characterized tumor for orthopedic surgeons, and its etiology is
completely unknown (2,3). The indications for surgery and optimal
surgical modalities remain controversial. We herein report a case
of a large intraosseous lipoma of the calcaneus in a middle-aged
man following a hindfoot injury.
Case report
A 36-year-old male construction worker visited
Ruijin Hospital North (Shanghai, China) in November 2014, with a
complaint of dull pain in his left heel over the last 5 months. The
patient reported spraining his hindfoot 5 months ago and visiting a
local hospital immediately after the injury. Plain-film radiographs
were normal, and the emergency physician initially managed the
sprain with rest and analgesics. However, the pain increased
gradually over the next 5 months and the patient visited our
Orthopedics Department.
Physical examination revealed mild tenderness in the
left heel, without evidence of a palpable mass or soft tissue
edema. The range of motion of both ankles and subtalar joints were
within the normal range. The laboratory blood tests and urine
analysis results were all normal.
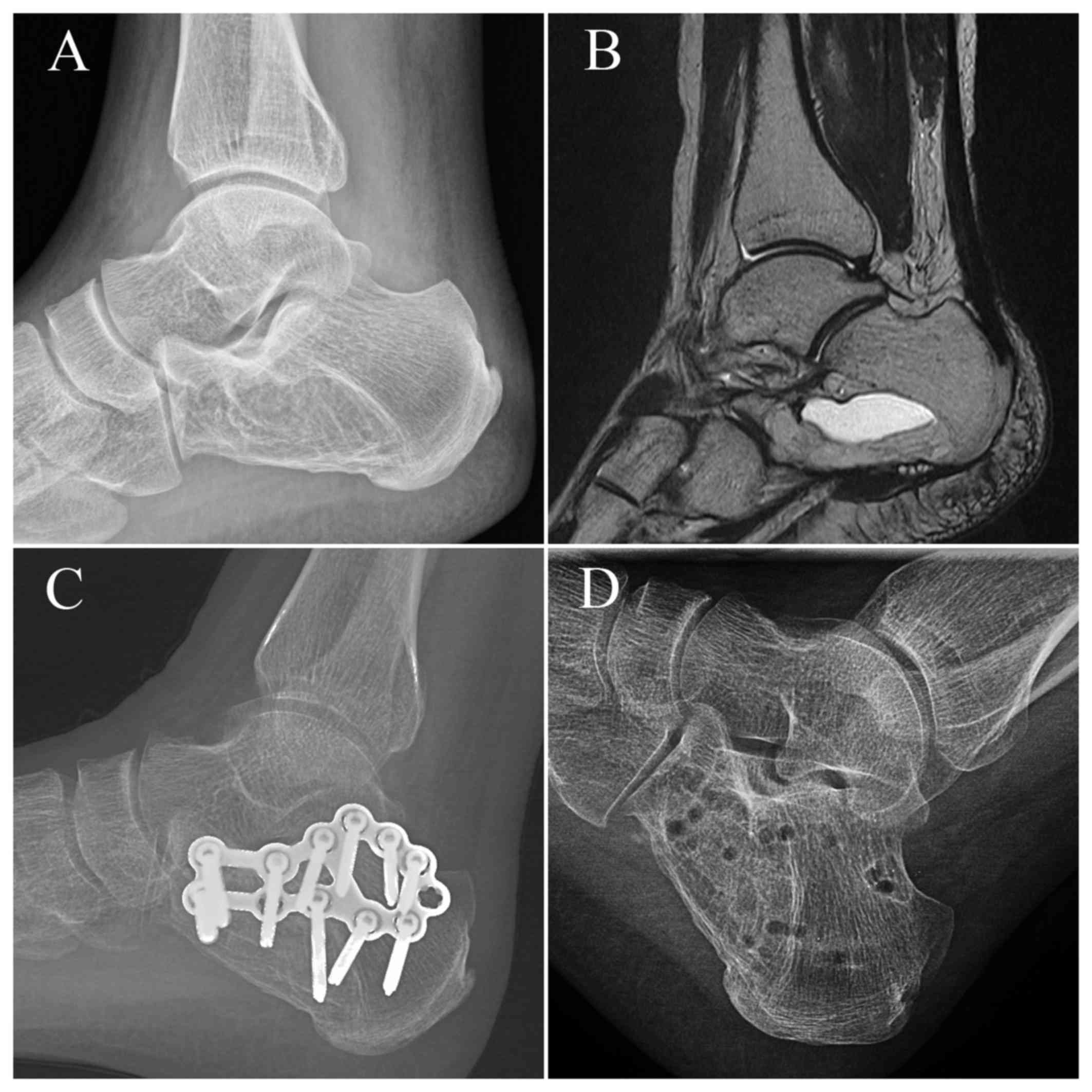
Plain-film radiographs revealed a large,
well-defined lytic lesion sized ~2.5×3 cm in size (Fig. 1A). A magnetic resonance imaging (MRI)
scan of the left foot revealed a large cyst in the central portion
of the calcaneus. T1-weighted MRI revealed an intramedullary lesion
with a signal intensity equal to that of subcutaneous fat.
T2-weighted images also displayed an intramedullary lesion with a
hyperintense signal (Fig. 1B). On
the basis of the clinical and typical diagnostic imaging findings,
a diagnosis of intraosseous calcaneal lipoma was made, and the
patient subsequently underwent surgery.
Surgery was performed under general anesthesia, with
the patient placed in the lateral position. Using a lateral
approach, the lateral wall of the calcaneus was exposed. When the
cyst was decorticated, curettage of the intraosseous lipoma was
thoroughly performed and the defect was filled with an artificial
bone substitute. Due to the large bone defect and fragile cortical
bone after curettage, an anatomically shaped plate was fixed to the
lateral wall of the calcaneus after grafting (Fig. 1C). The entire specimen was sent to
the Pathology Department for histological diagnosis. The wound was
closed in anatomical layers, and the foot was dressed with
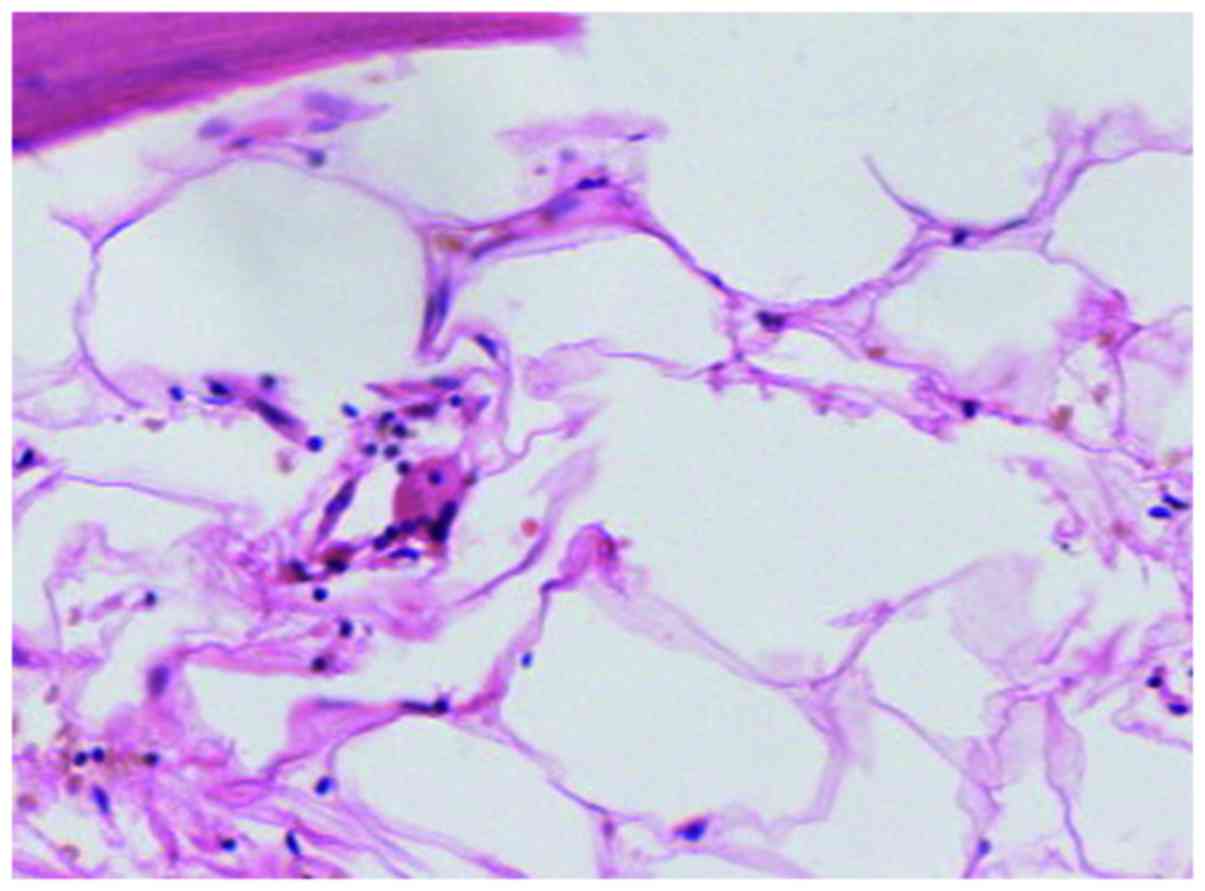
pressure. The postoperative pathological findings included
hyperplasia of adipose cells and blood vessels, with medullary
trabecular bone. Intraosseous calcaneal lipoma was therefore
confirmed (Fig. 2).
The heel pain improved immediately after the
surgery, and the wound healed successfully. At 14 months after
surgery, radiographs revealed that the lesion had healed well. The
internal fixation was surgically removed (Fig. 1D). An MRI performed at that time
displayed partial osseous integration of the calcium phosphate bone
graft substitute, without evidence of tumor recurrence.
Discussion
Intraosseous lipoma is a benign bone tumor that is
rather uncommon, despite the abundance of adipose connective tissue
in the bone marrow (1). Patients
with intraosseous lipomas are often asymptomatic, and several cases
are incidentally discovered. The etiology of intraosseous calcaneal
lipoma remains unclear, although several hypotheses have been
proposed, including healing bone infarction and post-traumatic
secondary bone reaction (2,3). In the present study, the patient
noticed increasing pain following a hindfoot trauma. It was
therefore hypothesized that a traumatic lesion may be a
predisposing factor in this case.
Intraosseous calcaneal lipoma is usually located
between the anterior and middle third of the calcaneus, also
referred to as the neutral triangle. This area is devoid of the
trabecular network crossing the calcaneus (4). However, the lesion in the present case
was larger compared with those previously reported. In addition,
the lesion extended to the full breadth of the calcaneus
lateromedially in the coronal plane, and occupied ~75% of the
anteroposterior length of the calcaneus.
Intraosseous calcaneal lipoma cannot be diagnosed
using plain radiographs alone. If the radiographs show an
osteolytic and well-circumscribed lesion with a thin sclerotic rim,
this may be misdiagnosed as a simple bone cyst, aneurysmal bone
cyst, giant cell tumor, or non-ossifying fibroma (5–7). Biopsy
for histopathological analysis is optimal, but invasive (8). Recently, with high-quality imaging
modalities such as computed tomography or MRI, intramedullary
lipomas and other bone lesions may be diagnosed without the need
for bone biopsy (9,10). Identification of the fat component
signal on MRI is diagnostic of an intraosseous lipoma on the basis
of the high signal intensity on both T1- and T2-weighted sequences,
and obvious signal reduction on fat suppression images (10,11).
Asymptomatic small cysts in non-weight-bearing areas
may be observed for progression, but the natural course remains
unknown. The most appropriate treatment for intraosseous calcaneal
lipoma is likely to depend on symptoms, location and size (12–14).
Intraosseous calcaneal lipoma ‘of critical size’ has been defined
as a lesion extending the full breadth of the calcaneus in the
coronal plan, and occupying ≥30% of the anteroposterior length of
the calcaneus (15).
Curettage and grafting is the standard surgical
approach to the treatment of these benign lesions. The conventional
treatment is curettage of the lesions with bone grafting, followed
by external fixation in the ankle joint. However, in the present
case, the intraosseous calcaneal lipoma was larger compared with
those previously reported. Curettage of the lesion created a
considerable bone defect, which reduces bone strength. The middle
part of the calcaneus plays an important role in force
transmission. Thus, internal fixation materials are crucial for the
reconstruction of the anatomy.
In the present case, internal fixation combined with
bone grafting after curettage of the lesion was proven to be an
effective and safe treatment choice for the large interosseous
calcaneal lipoma.
References
|
1
|
Poussa M and Holmström T: Intraosseous
lipoma of the calcaneus. Report of a case and a short review of the
literature. Acta Orthop Scand. 47:570–574. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schatz SG, Dipaola JD, D'Agostino A, Hanna
R and Quinn SF: Intraosseous lipoma of the calcaneus. J Foot Surg.
31:381–384. 1992.PubMed/NCBI
|
|
3
|
Greenspan A, Raiszadeh K, Riley GM and
Matthews D: Intraosseous lipoma of the calcaneus. Foot Ankle Int.
18:53–56. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Muramatsu K, Tominaga Y, Hashimoto T and
Taguchi T: Symptomatic intraosseous lipoma in the calcaneus.
Anticancer Res. 34:963–966. 2014.PubMed/NCBI
|
|
5
|
Karthik K and Aarthi S: Intraosseous
lipoma of the calcaneus mimicking plantar fascitis. Foot Ankle
Surg. 17:e25–e27. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mandl P, Mester A and Balint PV: A black
hole in a bone - intraosseous lipoma. J Rheumatol. 36:434–436.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Revenga Martínez M, Corral Bachiller FJ,
García Rubio J, Beltrán Muñoz M and Mendoza Zea AC: [Cystic lesion
of the calcaneus. Intraosseous lipoma]. Reumatol Clin. 3:139–142.
2007.[Cystic lesion of the calcaneus. Intraosseous lipoma].
PubMed/NCBI
|
|
8
|
Rose RE and Golding T: Intraosseous
lipoma. Is a biopsy necessary? West Indian Med J. 55:291–292. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ketyer S, Brownstein S and Cholankeril J:
CT diagnosis of intraosseous lipoma of the calcaneus. J Comput
Assist Tomogr. 7:546–547. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Richardson AA, Erdmann BB, Beier-Hanratty
S, Lautz D, Jacobs PM, Julsrud ME and Ringstrom JB: Magnetic
resonance imagery of a calcaneal lipoma. J Am Podiatr Med Assoc.
85:493–496. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Genchi V, Scialpi M, Scarciolla G, Dimauro
F and Trigona A: Intraosseous lipoma of the calcaneus.
Characterization with computerized tomography and magnetic
resonance in a case. Radiol Med. 99:86–88. 2000.(In Italian).
PubMed/NCBI
|
|
12
|
Bagatur AE, Yalcinkaya M, Dogan A, Gur S,
Mumcuoglu E and Albayrak M: Surgery is not always necessary in
intraosseous lipoma. Orthopedics. 33:2010.PubMed/NCBI
|
|
13
|
Neuber M, Heier J, Vordemvenne T and
Schult M: [Surgical indications in intraosseous lipoma of the
calcaneus. Case report and critical review of the literature].
Unfallchirurg. 107:59–63. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bertram C, Popken F and Rütt J:
Intraosseous lipoma of the calcaneus. Langenbecks Arch Surg.
386:313–317. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pogoda P, Priemel M, Linhart W, Stork A,
Adam G, Windolf J, Rueger JM and Amling M: Clinical relevance of
calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin
Orthop Relat Res. 424:202–210. 2004. View Article : Google Scholar
|