Introduction
Breast cancer is the most frequently diagnosed
cancer globally and is the leading cause of cancer-related death in
women (1). Breast cancer screening
programmes and improved treatment of primary tumors have
contributed significantly to reducing overall mortality rates.
However, clinical management of patients with metastatic
progression is much less comprehensively structured. The ovarian
metastases are sufficiently uncommon that they may be overlooked in
the differential diagnosis of genital tract disorders (2). Same metastatic lesions are clearly
secondary metastasis of breast cancer in patients with disseminated
disease, while other tumors may be confused with primary neoplasms.
This latter group represents the tumors with high aggressiveness as
metastasis to the cervix uteri (2,3). It is
important to identify these secondary neoplasms early for
therapeutic considerations. This case report shows the complexities
when issues of metastatic disease are considered and the consequent
need to differential diagnostic with histology.
Case report
An 86-year-old female patient was hospitalized in
the Geriatric Unit of Louis Mourier Hospital, Colombes, for anemia
associated with an inflammatory syndrome and abdominal pain with
menorrhagia, in December 2016. The patient was treated with
adjuvant hormonal therapy (letrozole), following right mastectomy
and axillary lymphadenectomy for invasive ductal cell carcinoma
(T2N0M0) of the breast 2 years prior.
An abdominal ultrasound examination revealed a
significant uterine mass (59×40 mm) with irregular contours and
abnormal vascularization, with associated discrete increase of the
blood level of cancer antigen 15-3 to 34 kU/l (normal range, <30
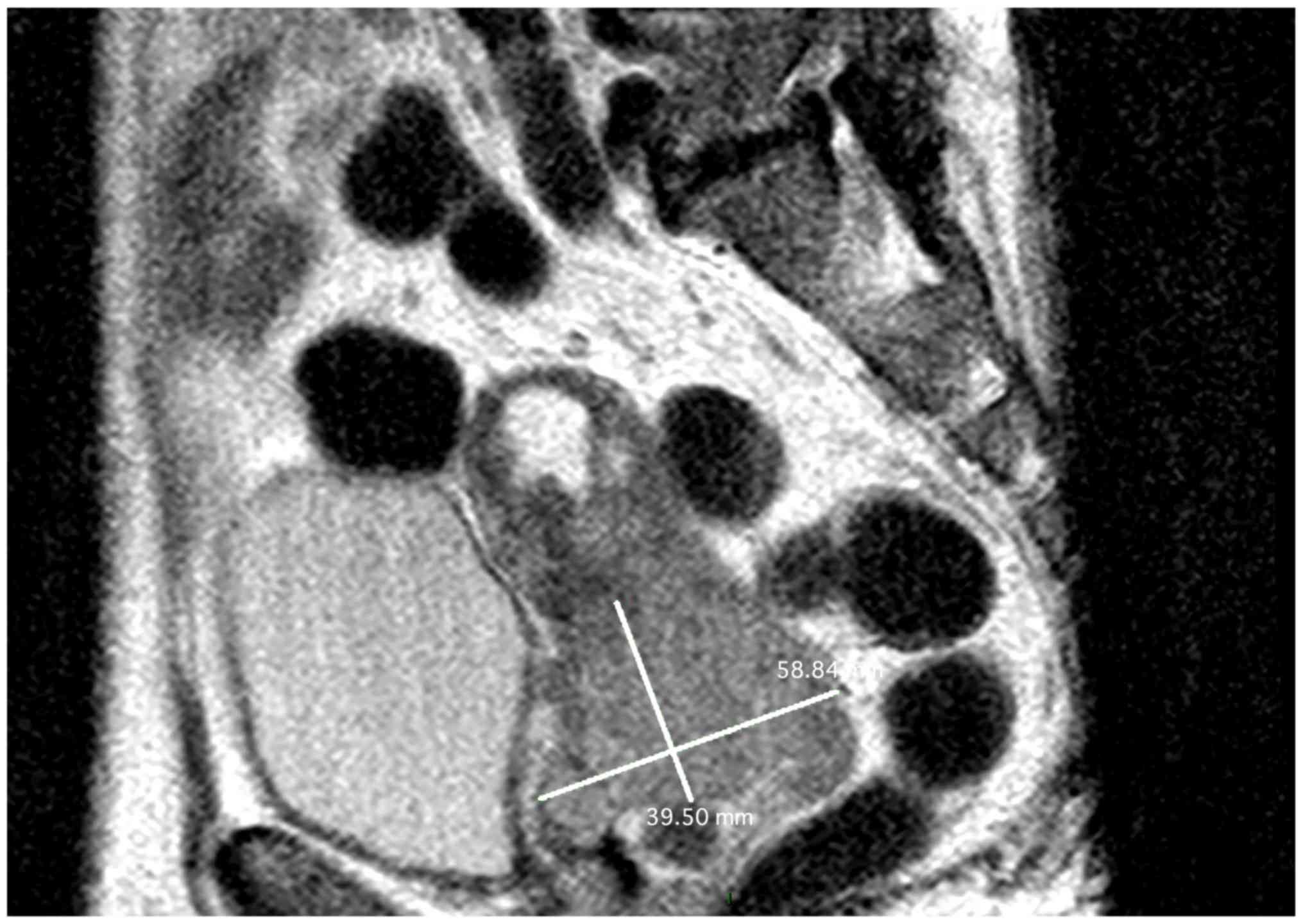
kU/l). The computed tomography (CT) scan confirmed the uterine mass
was situated next to the bladder and had irregular endometrium,
with multiple para-aortic lymphadenopathies. The morphological
assessment was completed by magnetic resonance imaging (MRI), which
revealed myometrial encroachment >50% on the right parametrium
and adnexa, and iliac nodes (Fig.
1). Positron emission tomography (PET)-CT revealed multiple
metastases in the sub-diaphragmatic para-aortic lymph nodes, the
left hilum and left adrenal gland, with diffuse bone metastases and
peritoneal carcinomatosis.
A cervical biopsy was performed and the histological
and immunohistochemical analysis (CK7-positive, CK20-negative,
anti-E-cadherin-positive, hormone receptor-negative and human
epidermal growth factor receptor 2-negative) confirmed this cancer
as a secondary lesion of primary ductal cell breast carcinoma, but
with a negative hormone profile, compatible with disease
progression during hormonal therapy. Unfortunately, considering the
multiple comorbidities, performance status score of 3 and the quick
deterioration of the patient's clinical condition, supportive care
was provided until the patient succumbed in July 2017.
Discussion
Metastasis of non-gynaecological tumours to the
cervix is a rare event, and metastasis from breast cancer is even
rarer. Only a few such cases have been described in the literature
to date, so the true incidence of breast cancer metastasis to
cervix is unknown (2–4). Mazur et al in 1984 analysed 325
metastatic female genital neoplasms, only 52 of which were found to
be metastases from breast carcinomas, but no cervical metastasis
from breast cancer was included (5).
More recently, Cumming et al reported that younger women are
at a higher risk for breast cancer metastasis to gynaecological
sites, than from cervix metastasis (6).
We herein present the case of a breast cancer
relapse as cervical metastasis 2 years after surgical treatment for
breast cancer, followed by treatment with letrozole. This
progression was accompanied by a modification of the metastatic
relapse hormonal status. In fact, the negatification of the
hormonal status indicates disease progression during adjuvant
hormonal therapy.
It is imperative to differentiate breast cancer
metastasis from primary carcinoma of the genital tract, but this
differentiation may be difficult due to several reasons:
Non-specific symptoms at presentation, long disease-free interval,
inconclusive radiological findings, and adenocarcinoma
histopathology. Imaging (CT or MRI scan) was not sufficient for
differential diagnosis in the present case, as the tumour mimicked
primary metastatic ovarian carcinoma. Immunohistological analysis,
particularly staining with anti-E-cadherin, were required for the
differential diagnosis.
It has been reported in the literature that younger
women are more likely to develop breast cancer relapse with
gynaecological metastasis compared with geriatric patients. Thus,
it is imperative that all patients with a history of breast cancer
presenting with gynaecological symptoms undergo biopsy of the
relapse site. In order to make the right diagnosis, histological
analysis is key in differentiating between primary and metastatic
disease.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AT and YB collected imaging data, performed part of
the measurements, analysed data and wrote the manuscript. LB
performed the imaging analyses. ML carried out the design of the
study and writing of the manuscript. The final version of the
manuscript has been read and approved by all authors.
Ethics approval and consent to
participate
The protocol was approved by The Ethics Committee
and Institutional Review Board of AP-HP Hospital Louis Mourier
(Colombes, France).
Consent for publication
The patient consent to the publication data and
associated image.
Competing interests
Author declares no conflict of interest.
References
|
1
|
Forouzanfar MH, Foreman KJ, Delossantos
AM, Lozano R, Lopez AD, Murray CJ and Naghavi M: Breast and
cervical cancer in 187 countries between 1980 and 2010: a
systematic analysis. Lancet. 378:1461–1484. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cruz PT: Mammary carcinoma with metastasis
to the cervix uteri. Del Med J. 26:304–305. 1954.PubMed/NCBI
|
|
3
|
Muñoz-Iglesias J, Uña-Gorospe J,
Allende-Riera A, De Sequera-Rahola M and Cárdenas-Negro C:
Unsuspected uterine metastasis of breast carcinoma diagnosed by
18F-FDG PET/CT. Clin Nucl Med. 38:e441–e442. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Benkerroum Z, Babahabib A, Kouach J,
Chahdi H, Al Bouzidi A, Rehali Moussaoui D and Dehayni M:
Metrorrhagia disclosing a synchronous bilateral breast cancer:
Report of a case. Gynécol Obstét Fertil. 42:360–364. 2014.(In
French). View Article : Google Scholar
|
|
5
|
Mazur MT, Hsueh S and Gersell DJ:
Metastases to the female genital tract. Analysis of 325 cases.
Cancer. 53:1978–1984. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cummings MC, Simpson PT, Reid LE,
Jayanthan J, Skerman J, Song S, Reed McCart AE, Kutasovic JR, Morey
AL, Marquart L, et al: Metastatic progression of breast cancer:
Insights from 50 years of autopsies. J Pathol. 232:23–31. 2014.
View Article : Google Scholar : PubMed/NCBI
|