Introduction
Angiomyolipomas (AMLs) are rare mesenchymal solid
tumors that consist of variable proportions of adipose tissue,
smooth muscle cells and blood vessels. In 2002, AMLs were included
in perivascular epithelioid cell neoplasms (PEComas) by the World
Health Organization (1,2). According to the dominant cell type,
AMLs maybe further divided into epithelioid, spindle-cell and
intermediate subtypes. AMLs are usually benign tumors, most often
encountered in the kidney, whereas the liver is the most frequent
extrarenal site. Extrarenal occurrence of AML is quite uncommon,
with ~600 cases of hepatic AMLs reported in the literature to date
(3). Hepatic epithelioid AML (HEAML)
is a particular type of AML that was first reported by Yamasaki
et al in 2000 (4), with no
more than 80 cases reported worldwide to date (5). HEAML, which was generally considered to
be benign in the past, has malignant potential according to several
reports (6). However, the natural
history of this type of tumor has not yet been elucidated. There
are no pathognomonic clinical, laboratory or radiological
characteristics of HEAML; thus, it may easily be mistaken for other
types of hepatic tumors, and the rate of misdiagnosis is very
high.
A small number of reported cases exhibit malignant
characteristics, such as invasive growth pattern, vascular invasion
and local recurrence after curative surgical resection, as well as
distant metastases. The growth rate and the presence of atypical
cells are more critical for estimating the malignant potential of
this type of tumor rather than size alone. Early diagnosis of HEAML
plays a fundamental role in treatment, which may be challenging due
to its atypical characteristics. We herein report the case of an
atypical HEAML and conduct a systematic review of the relevant
literature.
Case report
A 43-year-old Caucasian male patient visited his
general practitioner due to a productive cough persisting for >2
months. Chest X-ray and laboratory tests revealed no specific
pathological signs, and the physician suggested a chest computed
tomography (CT) scan for further evaluation, which revealed
multiple chronic obstructive pulmonary lesions and an incidental
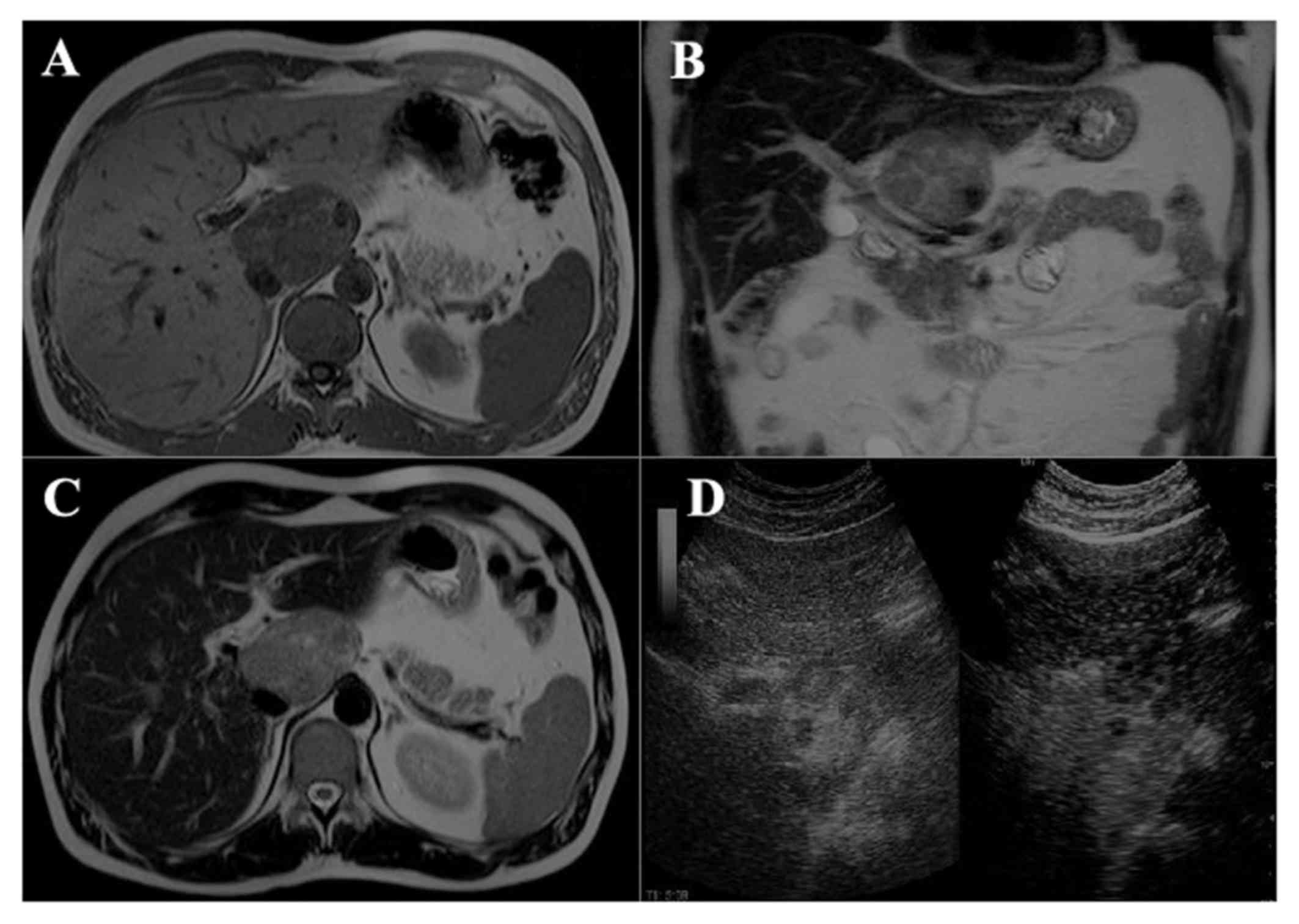
liver lesion. More specifically, the CT scan revealed a
well-demarcated lesion, 7 cm in maximum diameter, located in the
caudate lobe. The lesion exhibited heterogeneous enhancement
following intravenous contrast administration and appeared to
compress the intrahepatic portion of the inferior vena cava,
without invading it. An abdominal magnetic resonance imaging (MRI)
scan confirmed the findings of the CT (Fig. 1A-C). The hepatic lesion exhibited
regular borders with areas of fatty tissue, and demonstrated early
washout of the intravenous contrast medium and low attenuation in
the portal phase. The possibility of hepatocellular carcinoma (HCC)
at that time could not be excluded. Due to inconclusive
cross-sectional imaging, a contrast-enhanced ultrasound examination
was performed and revealed a hemodynamic behavior mimicking focal
nodular hyperplasia (Fig. 1D).
Physical examination revealed no abnormalities. Laboratory studies,
including α-fetoprotein (AFP) and carcinoembryonic antigen (CEA)
levels, were within the normal range; the hepatitis virus markers
were all negative.
Due to the inability of imaging studies to identify
the true nature of the lesion and, more importantly, exclude
malignancy, curative resection was performed. The patient underwent
left hepatectomy with additional resection of segment I. The
postoperative course was uneventful and the patient was discharged
on the 7th postoperative day.
The tumor mainly consisted of two morphologically
distinct components. The first component consisted of an admixture
of adipocytes, abnormal blood vessels, perivascular epithelioid
cells and sheets of foamy cells. These findings were considered to
be foci of typical (classical) AML. In abrupt transition with this
element, a second component with different morphology was
identified. In particular, some tumor areas were composed of sheets
of medium- to large-sized cells with epithelioid morphology. In
addition, the cells exhibited vesicular nuclei with prominent
nucleoli and eosinophilic cytoplasm (epithelioid AML). Focally,
cells with bizarre nuclei, multinucleated forms and giant cells
were identified. Mitoses were extremely rare. Tumor necrosis or
vessel invasion were not detected. Furthermore, areas with cells
with ‘clear’ morphology were identified. The latter areas were
diagnosed as ‘clear-cell’ AML.
Immunohistochemically, the neoplastic cells
expressed melanocytic markers, such as melan-A (Dako; Agilent
Technologies, Inc., Santa Clara, CA, USA, clone A103, 1:150) and
human melanoma black (HMB)-45 (Dako, clone HMB45, 1:150), while
HepPar-1 (Dako; Agilent Technologies, Inc., clone OCH1E5, 1:20),
S-100 (Thermo Fisher Scientific Inc., Waltham, MA, USA, clone
4C4.9, 1:800) and c-Kit (Dako; Agilent Technologies, Inc., rabbit,
1:600) were negative. The marker of cellular proliferation Ki-67
(Dako; Agilent Technologies, Inc, clone MIB-1, 1:100) was positive
in ~5% of neoplastic cells.
The atypical histological characteristics in the
present case included focal cellular pleomorphism, cellular atypia
and large tumor size (>5 cm). The morphological and
immunohistochemical findings were consistent with HEAML, including
an element of ‘typical’ AML. No adjuvant treatment was administered
postoperatively. The follow-up of the patient included medical
history and physical examination every 3 months for the first year
initially and every 6 months afterwards, along with abdominal MRI
scan at 3, 6, 12 and 24 months. The patient remained asymptomatic
and disease-free 2 years following the operation.
Discussion
In 2002, the World Health Organization recognized
PEComas as a different entity, including neoplasms with
perivascular epithelioid differentiation. PEComas include AMLs,
lymphangioleiomyomatosis and clear-cell ‘sugar’ tumors (7). EAML is a type of AML composed almost
exclusively of epithelioid cells, abnormal blood vessels and few or
no adipocytes (8). The clinical
characteristics of this type of tumor are usually silent, whereas
their natural history has not yet been elucidated. The majority of
reported cases are incidentally discovered during routine check-ups
or while conducting imaging examinations for other conditions.
According to previous studies, the majority of the patients are
asymptomatic, whereas patients with hepatic AML (HAML) may complain
of abdominal discomfort (9–12). Tuberous sclerosis is associated with
over half of the cases of renal AML and 5-15% of the cases of HAML
(13). The majority of the patients
have no history of liver disease or abnormalities in laboratory
tests, and the tumor serum markers, including CEA, AFP and
carbohydrate antigen 19-9, are usually within the normal range.
HAML is a heterogeneous tumor, which makes its
distinction from various liver neoplasms based on imaging
challenging, despite the advanced techniques currently available.
Most HAMLs are misdiagnosed as malignant or focal liver lesions.
Accurate diagnosis based on imaging studies alone is rare. On
ultrasonography, HAMLs appear as heterogeneously hyperechoic
masses. CT and MRI have similar diagnostic accuracy rates, and both
have a higher diagnostic accuracy compared with ultrasound
(14). The presence of fatty areas
and solid tissue components is a common presentation of HAML on CT
or MRI. However, the presence of adipose tissue is unreliable,
since HCCs may also contain fat (9).
Other useful imaging characteristics on CT or MRI discriminating
between HAML and HCC are the presence of early draining during the
portal venous phase, a peripheral rim of decreased enhancement and
the absence of a tumor capsule in the hypervascular hepatic tumor
(9,15). The CT findings of HEAML, however, are
related to the absence of adipose tissue in the lesions. In
addition, recognizing imaging characteristics such as lack of a
tumor capsule and hypervascularity, with central punctiform or
filiform vessels as a characteristic enhancement may help
distinguish HEAML from other hepatic tumors (16); however, only 25-52% of preoperative
diagnoses are correct (17,18). Thus, despite the advances in imaging
studies, histological diagnosis is necessary for treatment
planning.
Differential diagnosis includes high-grade HCC,
cholangiocarcinoma and rare sarcomas, such as epithelioid
leiomyosarcoma of the liver. The morphological and
immunohistochemical findings are usually sufficient for
distinguishing these entities. HCC may display clear-cell changes,
but immunohistochemically is positive for hepatocyte antigen.
Cholangiocarcinoma is an adenocarcinoma and is characterized by the
presence of atypical glands and glandular elements. Such neoplastic
formations were not found in the present case. Epithelioid
leiomyosarcoma may display clear-cell changes, but the tumor cells
are negative for melanocytic markers. In the present case,
malignant melanoma was excluded due to the lack of S-100
expression. Finally, gastrointestinal stromal tumors usually
express the c-Kit marker, which was not observed in our case.
Furthermore, the identification of the well-differentiated
component of (typical) AML, strongly favors the diagnosis of EAML
(19–21).
Atypical characteristics of EAML include a variety
of macroscopic and histological findings, such as the size of the
tumor (>5 cm), high mitotic rate, presence of atypical mitotic
figures, vascular invasion, necrosis and cellular pleomorphism
(2,7,22,23). In
the present case, the large size of the tumor, cellular
pleomorphism and atypical cells were evident, supporting the
diagnosis of ‘atypical’ EAML.
The majority of HAMLs are considered to be benign,
although several cases exhibiting malignant behavior have been
reported, including tumor growth, presence of atypical cells,
recurrence after surgical resection, metastasis and invasive growth
into the liver parenchyma and alongside the vessels (24). Malignant transformation is considered
to occur mostly in the epithelioid type (25). The first malignant AML was reported
in 2000 by Dalle et al (6).
The exact prevalence of malignant AML remains unknown. Most studies
state that there have been ~6 cases of malignant AML reported in
the literature to date. To the best of our knowledge, there have
been 19 reported cases of malignant AML that are included in this
review (5,6,26–40).
Since the first case reported by Dalle et al (6), 18 more cases were reported thereafter.
As summarized in Table I, 10 of
those cases were HEAMLs, and only 3 were typical AMLs. The
remaining 6 reported cases of malignant AML do not include an exact
description of their cellular components. The recurrence-free
survival in those cases ranges from 5 to 108 months. All patients
with HEAML underwent surgery. The median age of this population was
~37 years. The majority of the patients with malignant HEAML were
female (6/10). In 6 of the patients with malignant HEAML the mass
was located in the right hepatic lobe and in the remaining cases it
was in the left hepatic lobe.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Authors, year | Sex/age (years) | Epithelioid type | Location | Type of surgery | Metastasis | Re-op (yes/no) | Death (months) | RFS (months) | (Refs.) |
|---|
| Liu et al,
2016 | M/34 | Yes | Left lobe | Left lobectomy | NA | NA | NA | NA | (5) |
| Liu et al,
2016 | F/31 | Yes | Right lobe | Right lobectomy | NA | NA | NA | NA | (5) |
| Dalle et
al | F/70 | Yes | Right lobe | Right
trisegmenectomy | Yes (liver) | No | NA | AW | (6) |
| Mizuguchi et
al, 2004 | F/49 | Yes | Right lobe | Extended right
trisegmentectomy | NA | NA | NA | NA | (26) |
| Flemming et
al, 2000 | F/51 | Yes | Left lobe | Left lobectomy | No | Yes | No | 36 | (27) |
| Rouquie et al,
2006 | F/67 | Yes | Left lobe | Left lobectomy | NA | NA | NA | NA | (28) |
| Kamimura et
al, 2010 | M/52 | Yes | S3-S4 | Left lobectomy | No | No | No | AW | (29) |
| Fukuda et
al, 2016 | M/58 | Yes | S5 | Anterior
segmentectomy | Yes (lungs) | Yes | No | 36 | (30) |
| Deng et al,
2008 | M/30 | Yes | Right lobe | Right
lobectomy | Yes (pancreas and
lungs) | No | Yes (42) | AW | (31) |
| Parfitt et
al, 2006 | F/60 | Yes | Right lobe | Right
lobectomy | Yes (trapezius
muscle, liver, lung, pancreas) | Yes | No | 108 | (32) |
| Hu et al,
2011 | NA/NA | NA | NA | NA | Yes | No | Yes (14) | AW | (33) |
| Kobayashi et
al, 2013 | F/46 | No | Right lobe | Right
lobectomy | NA | No | No | 5 | (34) |
| Yang et al,
2007 | F/37 | NA | Left lobe | Extended left
lobectomy | No | No | Yes (9) | 6 | (35) |
| Nguyen et
al, 2008 | F/43 | No | Left lobe | Left lobectomy and
caudate lobe resection | Yes (peritoneum,
gastrohepaticomentum, retroperitoneal space) | Yes | Yes (8) | 6 | (36) |
| Croquet et
al, 2000 | NA/NA | NA | NA | NA | NA | NA | NA | 72 | (37) |
| Ding et al,
2011 | F/31 | NA | Right lobe | Right
lobectomy | No | No | Yes (7) | 72 | (38) |
| Wang et al,
2015 | F/37 | No | Left lobe | Left lobectomy | Yes (liver) | Yes | NA | NA | (39) |
| Xu et al,
2009 | F/NA | NA | Left lobe | Left lobectomy | Yes | NA | NA | NA | (40) |
| Xu et al,
2009 | NA/NA | NA | NA | NA | Yes | NA | NA | NA | (40) |
A systematic review by Klompenhouwer et al
suggested that, when the diagnosis of HAML based on imaging is
certain, conservative management is recommended (3). The first surveillance imaging according
to this review may be performed 1 year after diagnosis, with
biennial follow-up thereafter. However, when the diagnosis is
uncertain, biopsy must be performed. If biopsy is inconclusive or
shows epithelioid characteristics, resection is indicated. Thus,
the presence of epithelioid characteristics in AML is an additional
indication for resection.
Although HAMLs were previously considered to be
benign, surgeons should be aware of their malignant potential. When
the diagnosis is uncertain or when epithelioid or atypical
characteristics are found on preoperative biopsy, resection is
indicated due to the high probability of malignancy; an aggressive
approach contributes to diagnostic accuracy and definitive cure in
cases of malignancy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Ethics approval and consent to
participate
Not applicable.
Consent for publication
Written informed consent was obtained from the
patient for the publication of any associated data and accompanying
images.
Authors' contributions
ZG, NM, IDK and PT made substantial contributions to
data collection; histopathological analysis and the collection of
images were conducted by AL and GL. Literature searching was
performed by ZG and PT. ZG, NM, IDK and GCS drafted the manuscript;
GCS reviewed the manuscript for intellectually important content.
All the authors have read and approved the final version of this
manuscript.
Competing interests
The authors declare that they have no competing
interests to disclose.
References
|
1
|
Fletcher CD, Unni KK and Mertens F: World
Health Organization Classification of Tumors of Pathology and
Genetics: Tumors of Soft Tissue and Bone. 4. IARC Press; Lyon,
France: 2002
|
|
2
|
Folpe AL and Kwiatkowski DJ: Perivascular
epithelioid cell neoplasms: Pathology and pathogenesis. Hum Pathol.
41:1–15. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Klompenhouwer AJ, Verver D, Janki S,
Bramer WM, Doukas M, Dwarkasing RS, de Man RA and IJzermans JNM:
Management of hepatic angiomyolipoma: A systematic review. Liver
Int. 37:1272–1280. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yamasaki S, Tanaka S, Fujii H, Matsumoto
T, Okuda C, Watanabe G and Suda K: Monotypic epithelioid
angiomyolipoma of the liver. Histopathol. 36:451–456. 2000.
View Article : Google Scholar
|
|
5
|
Liu J, Zhang CW, Hong DF, Tao R, Chen Y,
Shang MJ and Zhang YH: Primary hepatic epithelioid angiomyolipoma:
A malignant potential tumor which should be recognized. World J
Gastroenterol. 22:4908–4917. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dalle I, Sciot R, de Vos R, Aerts R, van
Damme B, Desmet V and Roskams T: Malignant angiomyolipoma of the
liver: A hitherto unreported variant. Histopathol. 36:443–450.
2000. View Article : Google Scholar
|
|
7
|
Hornick JL and Fletcher CD: PEComa: What
do we know so far? Histopathol. 48:75–82. 2006. View Article : Google Scholar
|
|
8
|
Mai KT, Perkins DG and Collins JP:
Epithelioid cell variant of renal angiomyolipoma. Histopathol.
28:277–280. 1996. View Article : Google Scholar
|
|
9
|
Cai PQ, Wu YP, Xie CM, Zhang WD, Han R and
Wu PH: Hepatic angiomyolipoma: CT and MR imaging findings with
clinical-pathologic comparison. Abdom Imaging. 38:482–489. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nonomura A, Enomoto Y, Takeda M, Takano M,
Morita K and Kasai T: Angiomyolipoma of the liver: A reappraisal of
morphological features and delineation of new characteristic
histological features from the clinicopathological findings of 55
tumours in 47 patients. Histopathol. 61:863–880. 2012. View Article : Google Scholar
|
|
11
|
Yang L, Xu Z, Dong R, Fan J, Du Y, Zhang
Y, Wang X, Cheng X and Guo J: Is surgery necessary for patients
with hepatic angiomyolipoma? Retrospective analysis from eight
Chinese cases. J Gastroenterol Hepatol. 28:1648–1653.
2013.PubMed/NCBI
|
|
12
|
Yang X, Li A and Wu M: Hepatic
angiomyolipoma: Clinical, imaging and pathological features in 178
cases. Med Oncol. 30:4162013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsui WM, Colombari R, Portmann BC, Bonetti
F, Thung SN, Ferrell LD, Nakanuma Y, Snover DC, Bioulac-Sage P and
Dhillon AP: Hepatic angiomyolipoma: A clinicopathologic study of 30
cases and delineation of unusual morphologic variants. Am J Surg
Pathol. 23:34–48. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yang XY: Hepatic angiomyolipoma:
Radiologic-pathologic correlation and clinical features in 178
cases. HPB. 15:1042013.PubMed/NCBI
|
|
15
|
Wang SY, Kuai XP, Meng XX, Jia NY and Dong
H: Comparison of MRI features for the differentiation of hepatic
angiomyolipoma from fat-containing hepatocellular carcinoma. Abdom
Imaging. 39:323–333. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ji JS, Lu CY, Wang ZF, Xu M and Song JJ:
Epithelioid angiomyolipoma of the liver: CT and MRI features. Abdom
Imaging. 38:309–314. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Krebs S, Esposito I, Lersch C, Gaa J,
Schmid RM and Ebert O: Preoperative radiological characterization
of hepatic angiomyolipoma using magnetic resonance imaging and
contrast-enhanced ultrasonography: A case report. J Med Case Rep.
26:4812011. View Article : Google Scholar
|
|
18
|
Chang Z, Zhang JM, Ying JQ and Ge YP:
Characteristics and treatment strategy of hepatic angiomyolipoma: A
series of 94 patients collected from four institutions. J
Gastrointestin Liver Dis. 20:65–69. 2011.PubMed/NCBI
|
|
19
|
Choi WT, Ramachandran R and Kakar S:
Immunohistochemical approach for the diagnosis of a liver mass on
small biopsy specimens. Hum Pathol. 63:1–13. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen ZE and Lin F: Application of
immunohistochemistry in gastrointestinal and liver neoplasms: New
markers and evolving practice. Arch Pathol Lab Med. 139:14–23.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Geller SA, Dhall D and Alsabeh R:
Application of immunohistochemistry to liver and gastrointestinal
neoplasms: Liver, stomach, colon, and pancreas. Arch Pathol Lab
Med. 132:490–499. 2008.PubMed/NCBI
|
|
22
|
Mete O and van der Kwast TH: Epithelioid
angiomyolipoma: A morphologically distinct variant that mimics a
variety of intra-abdominal neoplasms. Arch Pathol Lab Med.
135:665–670. 2011.PubMed/NCBI
|
|
23
|
Folpe AL, Mentzel T, Lehr HA, Fisher C,
Balzer BL and Weiss SW: Perivascular epithelioid cell neoplasms of
soft tissue and gynecologic origin: A clinicopathologic study of 26
cases and review of the literature. Am J Surg Pathol. 29:1558–1575.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kamimura K, Nomoto M and Aoyagi Y: Hepatic
angiomyolipoma: Diagnostic findings and management. Int J Hepatol.
2012:4107812012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nese N, Martignoni G, Fletcher CD, Gupta
R, Pan CC, Kim H, Ro JY, Hwang IS, Sato K, Bonetti F, et al: Pure
epithelioid PEComas (so-called epithelioid angiomyolipoma) of the
kidney: A clinicopathologic study of 41 cases: Detailed assessment
of morphology and risk stratification. Am J Surg Pathol.
35:161–176. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mizuguchi T, Katsuramaki T, Nobuoka T,
Nishikage A, Oshima H, Kawasaki H, Kimura S, Satoh M and Hirata K:
Growth of hepatic angiomyolipoma indicating malignant potential. J
Gastroenterol Hepatol. 19:1328–1330. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Flemming P, Lehmann U, Becker T,
Klempnauer J and Kreipe H: Common and epithelioid variants of
hepatic angiomyolipoma exhibit clonal growth and share a
distinctive immunophenotype. Hepatology. 32:213–217. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rouquie D, Eggenspieler P, Algayres JP,
Béchade D, Camparo P and Baranger B: Malignant-like angiomyolipoma
of the liver: Report of one case and review of the literature. Ann
Chir. 131:pp. 338–341. 2006, (In French). View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kamimura K, Oosaki A, Sugahara S, Mori S,
Moroda T, Satoh O, Morita T, Kimura K, Kamura T, Nomoto M and
Aoyagi Y: Malignant potential of hepatic angiomyolipoma: Case
report and literature review. Clin J Gastroenterol. 3:104–110.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Fukuda Y, Omiya H, Takami K, Mori K,
Kodama Y, Mano M, Nomura Y, Akiba J, Yano H, Nakashima O, et al:
Malignant hepatic epithelioid angiomyolipoma with recurrence in the
lung 7 years after hepatectomy: A case report and literature
review. Surg Case Rep. 2:312016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Deng YF, Lin Q, Zhang SH, Ling YM, He JK
and Chen XF: Malignant angiomyolipoma in the liver: A case report
with pathological and molecular analysis. Pathol Res Pract.
204:911–918. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Parfitt JR, Bella AJ, Izawa JI and Wehrli
BM: Malignant neoplasm of perivascular epithelioid cells of the
liver. Arch Pathol Lab Med. 130:1219–1222. 2006.PubMed/NCBI
|
|
33
|
Hu WG, Lai EC, Liu H, Li AJ, Zhou WP, Fu
SY, Pan ZY, Huang G, Lei Y, Lau WY and Wu MC: Diagnostic
difficulties and treatment strategy of hepatic angiomyolipoma.
Asian J Surg. 34:158–162. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kobayashi Y, Kamimura K, Nomoto M,
Sugitani S and Aoyagi Y: Immunohistochemical character of hepatic
angiomyolipoma: For its management. Case Rep Med. 2013:2981432013.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yang CY, Ho MC, Jeng YM, Hu RH, Wu YM and
Lee PH: Management of hepatic angiomyolipoma. J Gastrointest Surg.
11:452–457. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Nguyen TT, Gorman B, Shields D and Goodman
Z: Malignant hepatic angiomyolipoma: Report of a case and review of
literature. Am J Surg Pathol. 32:pp. 793–798. 2008, View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Croquet V, Pilette C, Aubé C, Bouju B,
Oberti F, Cervi C, Arnaud JP, Rousselet MC, Boyer J and Calès P:
Late recurrence of a hepatic angiomyolipoma. Eur J Gastroenterol
Hepatol. 12:579–582. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ding GH, Liu Y, Wu MC, Yang GS, Yang JM
and Cong WM: Diagnosis and treatment of hepatic angiomyolipoma. J
Surg Oncol. 103:807–812. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Wang WT, Li ZQ, Zhang GH, Guo Y and Teng
MJ: Liver transplantation for recurrent posthepatectomy malignant
hepatic angiomyolipoma: A case report. World J Gastroenterol.
21:3755–3758. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Xu PJ, Shan Y, Yan FH, Ji Y, Ding Y and
Zhou ML: Epithelioid angiomyolipoma of the liver: Cross-sectional
imaging findings of 10 immunohistochemically-verified cases. World
J Gastroenterol. 15:4576–4581. 2009. View Article : Google Scholar : PubMed/NCBI
|