Introduction
The possibility of applying targeted therapies in
oncology introduced a new era of tailor-made treatments for breast
cancer. The currently available therapies are indicated based on
the morphological and genetic characteristics of the tumor
(1,2). Novel molecular techniques of gene
expression profiling and microarray analysis enabled the
identification of distinct invasive breast cancer (IBC) molecular
subtypes, such as luminal A, luminal B, tumors enriched with human
epidermal growth factor receptor 2 (HER-2) and triple-negative
tumors. Luminal A is a subtype positive for estrogen and
progesterone receptors (ER and PR, respectively) and
HER-2-negative, with low levels of Ki-67 expression. Luminal B is
also positive for ER and PR, but negative or positive for HER-2,
and with high levels of Ki-67. Triple-negative (or basal-like)
tumors are ER- and PR-negative, as well as HER-2 negative. Finally,
HER-2-enriched tumors are ER- and PR-negative, but HER-2-positive.
These subtypes are useful in clinical management, since they bear
distinct prognoses and predictive responses to targeted therapy
(3–7). ER-positive tumors are associated with a
better prognosis and are prone to respond well to hormone therapy
(3–5)
in terms of disease-free and overall survival (7,8), while
patients with triple-negative tumors have a poor prognosis
(6).
In clinical practice, immunohistochemical profiling
including three important breast cancer markers (ER, PR and HER-2
status) is used to determine breast cancer subtypes (1,3–5,9), and
this panel is currently considered the best choice for breast
cancer predictive pathological evaluation (1). However, although molecular profiling
provides important prognostic indicators, breast cancer risk
stratification remains a challenge for certain subtypes, such as
the triple-negative subtype, which is the most complex (3–6) and is
usually associated with a more aggressive tumor behavior and worse
prognosis (6).
Research efforts in molecular microarray
sub-stratification identified new subcategories within
triple-negative cancers (6,10). Among those, the ‘claudin-low’
subcategory has emerged as one of the most aggressive breast cancer
profiles (11–13), being correlated to an enriched
stem-cell component phenotype (11,12,14).
Claudins are cell adhesion molecules and components
of the tight junction complex, which regulate permeability between
cells and maintain cell-cell integrity (15,16), and
their role in carcinogenesis and progression to metastasis
currently constitutes an active research focus (17). Claudins are known to act as barriers
for the diffusion of solutes between epithelial cells,
participating in the regulation of water transportation, ions and
certain macromolecules. Therefore, it is a reasonable hypothesis
that claudins are likely to be involved in carcinogenesis (18).
The absence or low expression of claudins is
associated with cancer development and reduced survival, due to the
disruption of these tight junctions (19,20). The
‘claudin-low’ subtype of breast cancer is characterized by the
reduced expression of claudin mRNAs, mainly claudins 3, 4 and 7
(11,12,14,20).
Claudin expression deregulation has been previously implicated in
cancer and is associated with metastasis and cancer progression
(15,17), and low expression of claudins has
been correlated to worse prognosis in breast cancer when assessed
by RNA-based tests (14,17).
However, the claudin superfamily of integral
membrane proteins is composed of numerous isotypes (15,16,18), and
there is some heterogeneity in study results when claudin subtypes
are evaluated. Claudin 1 has been identified as a novel survival
factor in basal-like breast cancers, as downregulation of claudin 1
was shown to induce cell death in breast cancer cell lines
(17). High claudin 4 expression has
been associated with worse breast cancer-specific, recurrence-free
and overall survival, even in patients receiving adjuvant tamoxifen
therapy (21). In triple-negative
breast cancer cases, downregulation of claudin 7 (13,22) or a
combination of high expression of CLDN4 with low expression of
CLDN7, were identified as predictive factors of worse prognosis
(19).
In this context, the aim of the present study was to
verify whether the addition of claudin immunoexpression evaluation
to the immunohistochemical profile standard panel for patients with
breast cancer would improve its prognostic assessment potential.
Our objective, therefore, was to determine whether the expression
of claudins 4 and 7 (the main claudins specifically expressed in
human breast tissue) in tumor microarray (TMA) analysis would be
associated with survival and prognostic outcomes in a large cohort
of patients with breast tumors of different molecular subtypes
(luminal A, HER-2 and triple-negative).
Materials and methods
Design, setting and ethics
This diagnostic study was conducted in a large
referral center for cancer treatment in Brazil, a philanthropic
hospital, following approval of the local Ethics Committee. The
hospital obtained informed consent forms from all patients and
controls for using archived tissues for research at any time.
Patient anonymity was guaranteed.
Tumor samples and clinical data
The study used archived tumor samples from all
consecutive female patients who were diagnosed with IBC of no
specific type (not otherwise specified, NOS) between January 1980
and December 2001 in Hospital A.C. Camargo (São Paulo, SP, Brazil).
Patient characteristics are presented in Table I. Among these tumor samples,
formalin-fixed and paraffin-embedded samples with paraffin blocks
suitable for immunohistochemistry analysis, with a registry of
clinical data in the medical records and follow-up information,
were selected.
 | Table I.Clinical and pathological
characteristics of 803 breast cancer patients. |
Table I.
Clinical and pathological
characteristics of 803 breast cancer patients.
|
Characteristics | Patient no.
(%) |
|---|
| Age, years [median
(range)] | 54 (24–96) |
| Hormonal
status |
|
|
Postmenopausal | 317 (39.5) |
| Pathological
staging | 486 (60.5) |
| II | 395 (49.2) |
|
III | 350 (43.2) |
| IV | 58 (7.2) |
| Histological
grade |
|
| I | 103 (12.2) |
| II | 480 (59.8) |
|
III | 218 (27.1) |
| Missing
data | 2 (0.2) |
| Nuclear grade |
|
| 1 | 6 (0.7) |
| 2 | 249 (31.0) |
| 3 | 546 (68.0) |
| Tumor size |
|
|
T1+T2 | 394 (49.1) |
|
T3+T4 | 409 (50.9) |
| Lymph node
metastasis |
|
|
pN0 | 268 (33.1) |
|
pN+ | 524 (65.3) |
| Missing
data | 12 (1.1) |
| Molecular subgroup
of the primary tumor |
|
| Luminal
A | 500 (62.3) |
|
HER-2 | 114 (14.2) |
|
Triple-negative | 179 (22.3) |
| Missing
data | 10 (1.2) |
From these cases, four TMA blocks were built for
analysis, as described below. Two experienced pathologists (AFL and
FAS) reviewed all cases to confirm the diagnosis, histological
grade and the nuclear grade according to the criteria of the
Nottingham system (23), and cases
were individually discussed to reach consensus when necessary.
TMA construction
The construction of TMAs followed standard
procedures, as previously described (24). Briefly, 1-mm diameter cylinders from
selected tumor areas of the donor paraffin blocks were extracted
and inserted in order into the receptor blocks (Beecher
Instruments, Silver Spring, MD, USA). Each case was sampled twice
and all cylinders were distributed in four new blocks and stored at
4°C. Subsequently, 4-µm sections were prepared for each marker for
immunohistochemistry analysis. Healthy breast tissues were also
collected and confirmed as negative for breast cancer on
microscopic analysis to be used as controls (n=4, aged 50–75
years). These negative controls were selected among patients who
had undergone plastic surgery for aesthetic purposes, and whose
examination results excluded cancer.
Immunohistochemical staining
Each TMA slide was stained with the following
antibodies: Anti-ER (clone SP1; rabbit monoclonal, monoclonal,
anti-human estrogen receptor, clone SP1; cat. no. MA1-39540; 1:50;
Thermo Fisher Scientific, Inc., Waltham, MA, USA), anti-PR (clone
PgR636; monoclonal mouse anti-human progesterone receptor; Clone
PgR 636; cat. no. M3569; 1:500; Dako Agilent Technologies, Inc.,
Santa Clara, CA, USA), anti-HER-2 (polyclonal rabbit anti-human;
c-erbB-2 Oncoprotein; cat. no. A048529-2; 1:2,000; Dako; Agilent
Technologies, Inc), claudin 7 (polyclonal rabbit anti human; cat.
no. PA1-37474; 1:400), claudin 4 (claudin 4 monoclonal antibody
anti human clone 3E2C1; cat. no. 32-9400; 1:200, and claudin 4
polyclonal antibody anti human clone ZMD.306; cat. no. 36-4800;
1:200) (all from Invitrogen; Thermo Fisher Scientific Inc.), CD44
(monoclonal antibody anti human clone DF1485, 1:100; cat. no.:
MAB5315; 1:100; Abnova, Taipei, Taiwan) and CD24 (monoclonal
antibody anti human clone C-20; 1:100; cat. no. SC7034 clone C-20;
1:100; Santa Cruz Biotechnology, Inc., Dallas, TX, USA).
In order to standardize the immunohistochemical
staining for the primary antibodies, the antigen retrieval method
(equipment for humid heat, pH and type of buffer), the dilution of
primary antibodies and the visualization system were optimized.
Paraffin-embedded sections and breast tumor array sections were
deparaffinized in xylene and rehydrated through graded
ethanols.
For deparaffinization, the slides containing the
histological sections were kept in the oven for 24 h at 60°C and
then were immersed in xylene at 60°C for 20 min. They were then
immersed in xylol at room temperature for 20 min and then
rehydrated in ethanol in decreasing concentrations: 100% for 30
sec, 85% for 30 sec and 70% for 30 sec.
Following deparaffinization and rehydration of the
TMA sections, antigen retrieval was performed in a pressure cooker
(until boiling, which occurs at ~60°C in São Paulo) using sodium
citrate buffer (pH6) as retrieval solution. Following primary
antibody incubation (for 0 min at 25°C) and a polymer-peroxidase
(Leica Microsystem GmbH, Wetzlar, Germany) amplification step was
performed. No secondary antibody was employed. Antigen detection
was carried out in a solution containing 3,3′-diaminobenzidine
(Sigma-Aldrich; Merck KGaA, Darmstadt, Germany) and 6%
H2O2.
Counterstaining with Harris hematoxylin was
performed, at 25°C for 30 sec including positive controls in each
staining reaction. The positive controls consisted of normal breast
and neoplastic tissue known to express each of the antigens of
interest. The primary antibody was omitted as a negative control in
the same sample. All slides were observed in a light microscope
(DM300; Leica Microsystems GmbH).
Immunohistochemistry analysis
In order to classify the tumors into breast cancer
subtypes, ER and PR were evaluated according to Allred scoring
(25). Immunoreactivity ≤2 (or
<1% of positive tumor cells) was considered as a negative result
for ER and PR.
Luminal A was considered as ER- and PR-positive and
HER-2-negative, with low levels of Ki-67 expression (<14%);
luminal B was considered as positive for ER and PR, positive for
HER-2 (3+/3), with a Ki-67 index >14%; triple-negative (or
basal-like) tumors were ER-, PR- and HER-2-negative.
For HER-2 samples, the presence of reactivity in
<10% of the tumor cells was scored as 0, and cases in which
there was barely perceptible focal membranous staining were scored
as 1; weak to moderate staining observed in >10% of the tumor
cells was scored as 2, and a strong complete membranous staining
continuously in >10% of the tumor cells was scored as 3. We
considered the result to be positive only if the score was 3,
according to American Society of Clinical Oncology of American
Pathologists recommendations update (26,27).
In the CD24/44 evaluation, the specimens with
<10% of positive cells were considered as CD24/44-negative, and
as positive when the membranes were stained in a distinct, thin
pattern, limited to the membrane, without cytoplasmic or nuclear
reactivity for CD44, CD24, claudins 4 and 7. CD24 is mainly
detected in the cytoplasm. A HercepTest model was used for
reporting results, and the scoring was as follows: 0, totally
negative; 1+, 1–10% positive neoplastic cells; 2+, moderate
staining in 10–30% of neoplastic cells; and 3+, >30% of strongly
reactive neoplastic cells. Normal breast tissue usually exhibits a
2+ pattern of claudin 7 expression and 1+ or 0 for CD24 and CD44.
Therefore, 3+ was considered as overexpression of these markers in
the present study.
As regards the claudin expression detection and
classification methods, our analysis was based on the Lanigan et
al study (21), which reported a
0–3+ pattern of claudin expression, and also previous studies of
our group (28), stating that ‘CD44
and claudin-7 were considered positive when membranes were stained
in a distinct and delicate pattern without reactive cytoplasm or
nuclei. We used a HercepTest model for reporting results and the
scoring was: 0, totally negative; 1+, 1–10% positive neoplastic
cells; 2+, moderate staining in 10–30% of neoplastic cells; and 3+,
>30% of strongly reactive neoplastic cells. CD24 was detected
mainly in the cytoplasm and scoring was conducted as for CD44.’
This assay was performed once per patient.
Statistical analysis
Data were presented as numbers (n) and percentage of
cases. Associations between the immunohistochemical expressions and
important clinicopathological variables were investigated using the
Chi-squared test (χ2). Survival probabilities were
estimated by the univariate Kaplan-Meier method for univariate
analysis and survival curves were compared using the log-rank test
(Mantel-Haenszel method). SSPS version 10.0 for Windows (SPSS Inc.,
Chicago, IL, USA) was used for the analyses.
Results
Clinicopathological characteristics of
the patients
During the study period, 880 patients with IBC were
identified in our archives, and tissue samples and follow-up data
were available for 803 of those patients. Further analysis of
immunostained samples allowed for inclusion of 793 suitable cases
in this study. The distribution of cases according to the clinical
and pathological variables and ER, PR and HER-2 immunoexpression is
shown in Table I. The present series
included 500 cases with a luminal profile, 114 with HER-2
expression, and 179 triple-negative cases. In all these IBC cases,
treatment involved mastectomy, radiotherapy and axillary lymph node
dissection. ER-positive patients received hormone therapy, and the
remaining were treated with chemotherapy. The median follow-up
period was 70 months. At the final follow-up (July, 2007), 425
patients remained alive and 378 had succumbed to the disease.
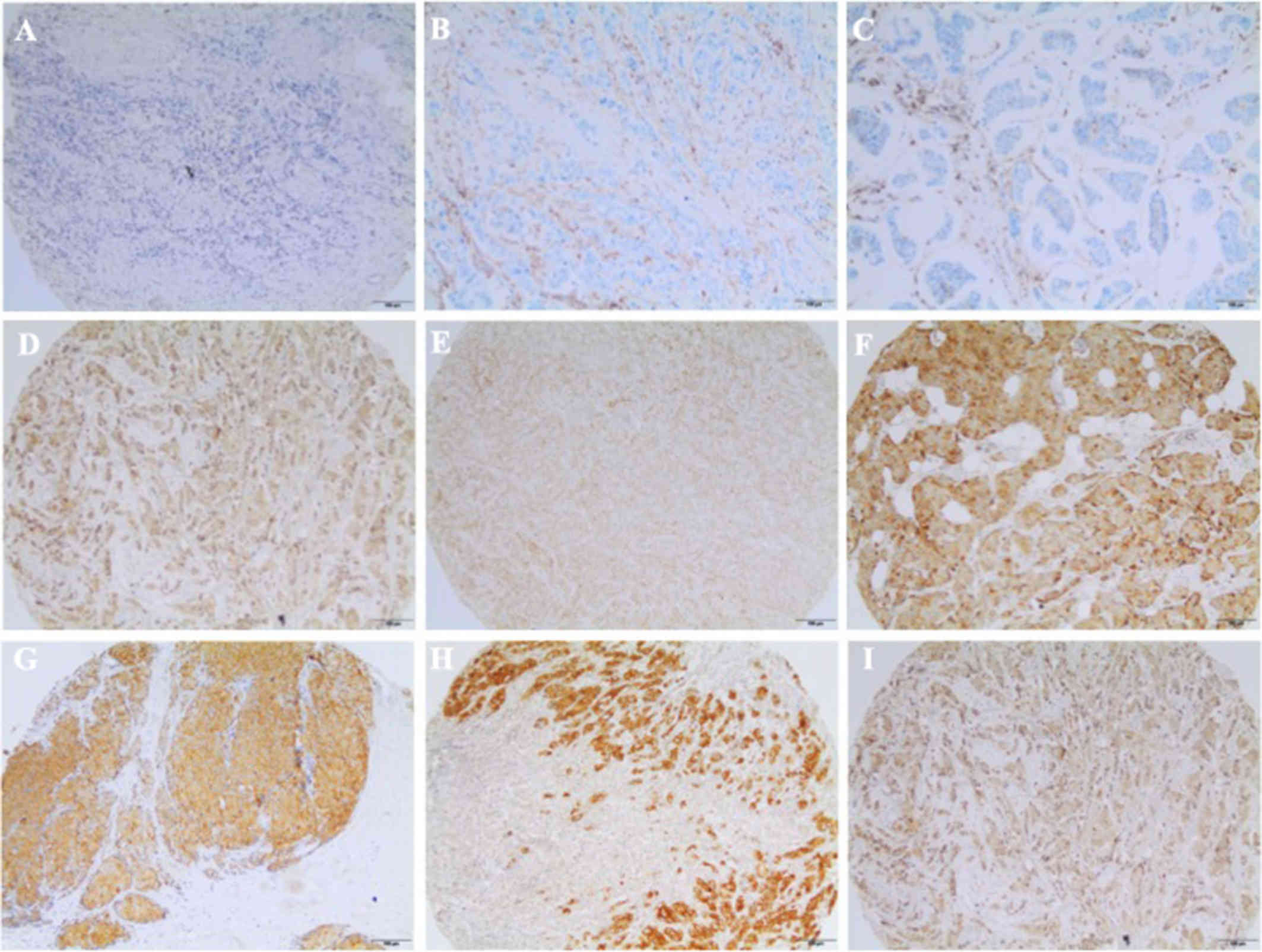
Claudin expression in primary breast
carcinomas
The claudin status according to immunohistochemistry
expression is presented in Table
II. The majority of cases (62.6%) exhibited preserved claudin 4
or 7 expression and 46% were claudin 7-positive. Over 73% of the
cases were positive for claudins 4 or 7, and only 15.7% were
negative for both claudins. Claudin 4 staining was restricted to
epithelial cells and concentrated at the cell membrane, whereas
claudin 7 exhibited a non-diffuse and punctate distribution.
Examples of CD24, CD44 and claudin 4 and 7 immunostaining are shown
in Fig. 1.
| Table II.Frequency of claudin 4 and 7 and
CD44/CD24 protein expression in primary breast carcinomas. |
Table II.
Frequency of claudin 4 and 7 and
CD44/CD24 protein expression in primary breast carcinomas.
| Biomarkers | Patient no.
(%) |
|---|
| Claudin 4 |
|
|
Negative | 288 (35.9) |
|
Positive | 503 (62.6) |
| Missing
data | 12 (1.5) |
| Claudin 7 |
|
|
Negative | 355 (44.2) |
|
Positive | 369 (46.0) |
| Missing
data | 79 (9.8) |
| CD44/CD24 |
|
|
−/− | 285 (35.5) |
|
+/+ | 126 (15.7) |
|
−/+ | 256 (31.9) |
| +/-
(stem cells) | 82 (10.2) |
| Missing
data | 54 (6.7) |
CD24/44 expression analysis revealed only 10.2% of
cases with stem cell profile (CD44-positive/CD24-negative). The
pattern of CD44 expression was mainly membranous, whereas CD24 was
expressed predominantly in the cytoplasm.
No associations were observed between claudin 7
expression and the presence of ER/PR and HER-2. Claudin 7
expression was also not found to be associated with clinical or
pathological variables, such as stage, tumor size or lymph node
status in TMA analysis (Tables III
and IV).
| Table III.Correlation between the expression of
biomarkers in breast carcinoma and prognostic factors. |
Table III.
Correlation between the expression of
biomarkers in breast carcinoma and prognostic factors.
|
| Markers |
|---|
|
|
|
|---|
|
| Claudin 4 | Claudin 7 |
|---|
|
|
|
|
|---|
| Clinicopathological
data | Negative | Positive | Negative | Positive |
|---|
| Histological grade,
n (%) |
| I | 37 (36.6) | 64 (63.4) | 47 (50.0) | 47 (50.0) |
| II | 197 (41.6) | 197 (58.4) | 214 (49.9) | 215 (50.1) |
|
III | 54 (25.2) | 160 (74.8) | 94 (47.0) | 106 (53.0) |
|
|
P<0.001 | P=0.78 |
| Nuclear grade, n
(%) |
| 1 | 3 (50.0) | 3 (50.0) | 2 (33.3) | 4 (66.7) |
| 2 | 112 (45.7) | 133 (54.3) | 118 (51.8) | 110 (48.2) |
| 3 | 173 (32.2) | 365 (67.8) | 235 (48.0) | 255 (52.0) |
|
| P=0.001 | P=0.47 |
| Tumor stage, n
(%) |
| T1 +
T2 | 144 (37.1) | 244 (62.9) | 175 (48.7) | 184 (51.3) |
| T3 +
T4 | 144 (35.7) | 259 (64.3) | 180 (49.3) | 185 (50.7) |
|
| P=0.71 | P=0.88 |
| Lymph nodes, n
(%) |
|
Negative | 110 (41.7) | 154 (58.3) | 118 (49.4) | 121 (50.6) |
|
Positive | 175 (34.0) | 340 (66.0) | 232 (48.8) | 243 (51.2) |
|
| P=0.04 | P=0.94 |
| Pathological stage,
n (%) |
| II | 147 (38.0) | 240 (62.0) | 179 (49.7) | 181 (50.3) |
|
III | 118 (34.0) | 229 (66.0) | 158 (49.5) | 161 (50.5) |
| IV | 23 (40.4) | 34 (59.6) | 18 (40.0) | 27 (60.0) |
|
| P=0.44 | P=0.46 |
| Estrogen receptor,
n (%) |
|
Negative | 82 (30.1) | 190 (69.9) | 130 (52.6) | 117 (47.4) |
|
Positive | 204 (39.5) | 313 (60.5) | 224 (44.2) | 251 (52.8) |
|
| P=0.01 | P=0.18 |
| Progesterone
receptor, n (%) |
|
Negative | 143 (32.9) | 231 (67.1) | 198 (49.6) | 201 (50.4) |
|
Positive | 143 (40.3) | 212 (53.7) | 156 (48.3) | 167 (51.7) |
|
| P=0.037 | P=0.76 |
| HER-2, n (%) |
|
Negative | 262 (37.9) | 429 (62.1) | 301 (48.9) | 314 (51.1) |
|
Positive | 21 (18.4) | 93 (81.6) | 51 (49.5) | 52 (50.5) |
|
|
P<0.001 | P=0.92 |
| CD44/CD24, n
(%) |
|
−/− | 111 (39.4) | 171 (60.6) | 168 (64.4) | 171 (60.6) |
|
+/+ | 47 (37.9) | 77 (62.1) | 47 (37.3) | 79 (62.7) |
|
−/+ | 80 (32.0) | 170 (68.0) | 83 (33.5) | 165 (66.5) |
|
+/- | 25 (30.5) | 57 (69.5) | 52 (65.8) | 27 (34.2) |
|
| P=0.22 |
P<0.001 |
| Table IV.Association between claudin 4 and
claudin 7 expression, molecular subgroups and CD44/CD24 expression
in invasive ductal breast carcinomas. |
Table IV.
Association between claudin 4 and
claudin 7 expression, molecular subgroups and CD44/CD24 expression
in invasive ductal breast carcinomas.
|
| Claudin
4-positive |
| Claudin
7-positive |
|
|---|
|
|
|
|
|
|
|---|
| Variables | N (%) | OR | CI (95%) | P-value | N (%) | OR | CI (95%) | P-value |
|---|
| Molecular
subgroup |
| Luminal
A | 293 (58.6) | – | – |
| 239 (65.3) | – | – |
|
|
HER-2 | 93 (18.6) | 3.0 | 1.8–4.99 |
<0.001 | 52 (14.2) | 0.91 | 0.59–1.40 | 0.68 |
|
Triple-negative | 114 (22.8) | 1.22 | 0.86–1.76 | 0.26 | 75 (20.5) | 0.77 | 0.54–1.10 | 0.16 |
| CD44/CD24 |
|
−/− | 171 (36.0) | – | – | – | 93 (25.5) | – | – |
|
|
+/+ | 77 (16.2) | 1.06 | 0.69–1.64 | 0.78 | 79 (21.7) | 3.04 | 1.95–4.72 |
<0.001 |
|
−/+ | 170 (35.8) | 1.38 | 0.96–1.97 | 0.08 | 165 (45.3) | 3.59 | 2.49–5.17 |
<0.001 |
|
+/- | 57 (12.0) | 1.48 | 0.87–2.51 | 0.15 | 27 (7.4) | 0.94 | 0.55–1.59 | 0.81 |
However, claudin 4 expression exhibited a direct
association with histological and nuclear grade. The same
progressive accumulation of claudin 4-positive cases was associated
with lymph node status, meaning that, proportionally, more claudin
4-positive cases were concentrated at the positive lymph node
category (Table III).
Among the ER-positive cases, which comprised the
majority of the patients, 60.5% were claudin 4-positive. However,
almost 70% of the ER-negative cases were also associated with
preserved claudin 4 expression (P=0.01). Similarly, although 53.7%
of the PR-positive cases were claudin 4-positive, a high number of
tumors (67.1%) stained positive in the PR-negative samples
(P=0.037). However, positive claudin 4 expression was more
prevalent among HER-2 positive tumors (P<0.001) (Tables III and IV).
The frequency of claudin 4 and 7 expression in
several combinations of CD44 and CD24 phenotypes was next analyzed.
Claudin 4 expression exhibited no differences in frequency between
possible combinations, while claudin 7 positivity was associated
with the CD44+/CD24+ and
CD44−/CD24+ phenotypes in the sample
(P=0.001) (Tables III and IV).
The expression of claudins 4 and 7 in breast
carcinomas was examined according to previously defined subtypes of
breast cancer patients. Claudin 4 was less expressed in the luminal
A and triple-negative subtypes and exhibited the highest frequency
of positive expression in HER-2-enriched tumors, whereas claudin 7
positivity was not associated with any of the breast cancer
subtypes (Tables IV and V). When the presence of the
CD44+/CD24− phenotype was investigated, we
observed that the stem cell phenotype was not related to the
defined subgroups.
| Table V.Distribution of protein expression
pattern according to molecular groups of locally advanced invasive
ductal breast carcinomas. |
Table V.
Distribution of protein expression
pattern according to molecular groups of locally advanced invasive
ductal breast carcinomas.
| Variables | Luminal A | HER-2 |
Triple-negative | P-value |
|---|
| Claudin 4, n
(%) |
|
Negative | 199 (70.3) | 21 (7.4) | 63 (22.3) | 0.001 |
|
Positive | 293 (58.6) | 93 (18.6) | 114 (22.8) |
|
| Claudin 7, n
(%) |
|
Negative | 214 (60.8) | 51 (14.5) | 87 (24.7) | 0.37 |
|
Positive | 239 (65.3) | 52 (14.2) | 75 (20.5) |
|
| CD44, n (%) |
|
Negative | 338 (61.3) | 75 (13.6) | 138 (25.0) | 0.02 |
|
Positive | 141 (68.1) | 34 (16.4) | 32 (15.5) |
|
| CD24, n (%) |
|
Positive | 228 (62.3) | 58 (15.8) | 80 (21.9) | 0.62 |
|
Negative | 242 (64.0) | 51 (13.5) | 85 (22.5) |
|
| CD44/CD24 |
|
+/+ | 171 (60.4) | 45 (15.9) | 67 (23.7) | 0.11 |
|
+/- | 84 (68.4) | 21 (17.1) | 18 (14.6) |
|
|
−/+ | 157 (61.8) | 30 (11.8) | 67 (26.4) |
|
|
−/− | 56 (68.3) | 13 (15.9) | 13 (15.9) |
|
We then investigated the possible prognostic value
of claudin 4 and 7 expression. Considering all patients, claudin
immunoexpression profile was not able to distinguish between
patients with better or worse prognosis. As seen in Tables VI and VII, claudin 4 and 7 expression profiles
were not associated with overall survival or disease-free interval.
Among triple-negative cases (Table
VIII) and luminal cases (Table
IX), the immunoexpression of claudin 4 and 7 did not indicate
clinical evolution; this was also true for the HER-2 subgroup
(Table X; P=0.09).
| Table VI.Univariate analysis considering
overall survival of breast cancer patients. |
Table VI.
Univariate analysis considering
overall survival of breast cancer patients.
| Variables | Number of
patients | Median survival
(years) | 95% confidence
interval | P-value |
|---|
| Pathological
stage |
| II | 395 | Not achieved | Not determined |
<0.001 |
|
III | 350 | 6.0 | 4.9–7.1 |
|
| IV | 58 | 2.0 | 1.4–2.6 |
|
| HER-2 |
|
Negative | 679 | 12.0 | 9.8–14.2 | 0.008 |
|
Positive | 114 | 5.0 | 0.6–9.4 |
|
| Estrogen
receptor |
|
Negative | 275 | 6.0 | 4.2–7.8 |
<0.001 |
|
Positive | 525 | 14.0 | 12.0–15.9 |
|
| Progesterone
receptor |
|
Negative | 440 | 8.0 | 6.1–9.9 |
<0.001 |
|
Positive | 360 | 16.0 | 12.8–19.2 |
|
| Molecular
subgroups |
| Luminal
A | 500 | 14.0 | 12.0–15.9 |
<0.001 |
|
HER-2 | 114 | 5.0 | 0.6–9.4 |
|
|
Triple-negative | 179 | 6.0 | 3.8–8.2 |
|
| Claudin 4 |
|
Negative | 288 | 10.0 | 7.2–12.8 | 0.49 |
|
Positive | 503 | 12.0 | 9.7–14.3 |
|
| Claudin 7 |
|
Negative | 355 | 11.0 | 8.6–13.4 | 0.97 |
|
Positive | 369 | 12.0 | 9.3–14.7 |
|
| CD44/CD24 |
|
−/− | 285 | 13.0 | 10.3–15.8 | 0.65 |
|
−/+ | 256 | 11.0 | 8.4–13.6 |
|
|
+/- | 82 | 9.0 | 5.4–12.6 |
|
|
+/+ | 126 | 12.0 | 9.5–14.5 |
|
| Table VII.Univariate analysis considering
disease-free survival of breast cancer patients. |
Table VII.
Univariate analysis considering
disease-free survival of breast cancer patients.
| Variables | Number of
patients | Median survival
(years) | 95% confidence
interval | P-value |
|---|
| Pathological
stage |
| II | 395 | 21.0 | ND |
<0.001 |
|
III | 350 | 5.0 | 4.0–6.0 |
|
| HER-2 |
|
Negative | 632 | 16.0 | 9.8–14.2 | 0.009 |
|
Positive | 106 | 8.0 | Not determined |
|
| Estrogen
receptor |
|
Negative | 248 | 8.0 | 2.1–13.8 |
<0.001 |
|
Positive | 497 | Not achieved | Not determined |
|
| Progesterone
receptor |
|
Negative | 403 | 10.0 | 5.7–14.3 |
<0.001 |
|
Positive | 342 | NA | Not determined |
|
| Molecular
subgroups |
| Luminal
A | 474 | Not achieved | Not determined |
<0.001 |
|
HER-2 | 106 | 8.0 | Not determined |
|
|
Triple-negative | 158 | 10.0 | 3.7–16.3 |
|
| Claudin 4 |
|
Negative | 265 | 14.0 | 9.9–18.1 | 0.76 |
|
Positive | 469 | 21.0 | 8.0–34.0 |
|
| Claudin 7 |
|
Negative | 337 | Not achieved | Not determined | 0.18 |
|
Positive | 342 | 16.0 | Not determined |
|
| CD44/CD24 |
|
−/− | 271 | Not achieved | Not determined | 0.93 |
|
−/+ | 231 | Not achieved | Not determined |
|
|
+/- | 78 | 16.0 | 4.8–27.2 |
|
|
+/+ | 120 | 16.0 | 9.9–22.0 |
|
| Table VIII.Univariate analysis considering
triple-negative breast cancer patients. |
Table VIII.
Univariate analysis considering
triple-negative breast cancer patients.
| Variables | Number of
patients | Median survival
(years) | 95% confidence
interval | P-value |
|---|
| Overall
survival |
| Claudin 4 |
|
|
| 0.56 |
|
Negative | 63 | 5.0 | 2.9–7.08 |
|
|
Positive | 114 | 6.0 | 2.3–9.6 |
|
| Claudin 7 |
|
|
| 0.82 |
|
Negative | 87 | 6.0 | 3.13–8.87 |
|
|
Positive | 75 | 16.0 | 3.0–10.95 |
|
| Disease-free
survival |
| Claudin 4 |
|
|
| 0.35 |
|
Negative | 57 | 6.0 | 2.2–9.8 |
|
|
Positive | 99 | 15.0 | 7.3–22.6 |
|
| Claudin 7 |
|
|
| 0.79 |
|
Negative | 79 | 15.0 | 3.23–26.8 |
|
|
Positive | 63 | Not achieved | Not determined |
|
| Table IX.Univariate analysis considering
luminal breast cancer patients. |
Table IX.
Univariate analysis considering
luminal breast cancer patients.
| Variables | Number of
patients | Median survival
(years) | 95% confidence
interval | P-value |
|---|
| Overall
survival |
| Claudin 4 |
|
|
| 0.39 |
|
Negative | 199 | 11.0 | 7.8–14.2 |
|
|
Positive | 293 | 14.0 | 11.8–16.3 |
|
| Claudin 7 |
|
|
| 0.82 |
|
Negative | 214 | 13.0 | 10.3–15.8 |
|
|
Positive | 239 | Not achieved | Not determined |
|
| Disease-free
survival |
| Claudin 4 |
|
|
| 0.70 |
|
Negative | 185 | 16.0 | 11.9–20.0 |
|
|
Positive | 281 | Not achieved | Not determined |
|
| Claudin 7 |
|
|
| 0.28 |
|
Negative | 206 | Not achieved | Not determined |
|
|
Positive | 229 | Not achieved | Not determined |
|
| Table X.Univariate analysis considering
HER-2-positive breast cancer patients. |
Table X.
Univariate analysis considering
HER-2-positive breast cancer patients.
| Variables | Number of
patients | Median survival
(years) | 95% confidence
interval | P-value |
|---|
| Overall
survival |
| Claudin 4 |
|
|
| 0.51 |
|
Negative | 21 | 4.0 | 2.7–5.3 |
|
|
Positive | 93 | 10.0 | 3.4–16.6 |
|
| Claudin 7 |
|
|
| 0.27 |
|
Negative | 51 | 11.0 | Not determined |
|
|
Positive | 52 | 4.0 | 0.0–8.0 |
|
| Disease-free
survival |
| Claudin 4 |
|
|
| 0.88 |
|
Negative | 20 | 4.0 | Not determined |
|
|
Positive | 86 | 8.0 | Not determined |
|
| Claudin 7 |
|
|
| 0.09 |
|
Negative | 50 | Not achieved | Not determined |
|
|
Positive | 48 | 3.0 | 1.4–4.5 |
|
Discussion
In the present study, 803 IBCs were evaluated for
claudin 4 and 7 immunohistochemical expression, in search for the
possible role of these claudins as prognostic indicators, beyond
breast cancer subtype profiling. The distribution of subtypes in
our sample (62% luminal, 14% HER-2-positive and 22%
triple-negative) reflected the distribution in the literature
(4,29). However, in the present study, what is
referred to as ‘claudin-low’ status (herein defined by the low
expression of claudins 4 and 7) was not found to be associated with
the triple-negative-like IBC subtype. We consider the status of any
individual claudin to play a limited role in determining prognosis
or providing predictive information in luminal A, HER-2 and
triple-negative breast cancer subtypes, whereas it is of little
value to the routine immunohistochemistry panel investigation for
patients with breast cancer. Although suggested to act as a tumor
supressor, high levels of claudin 1 have been observed in the
aggressive triple-negative or basal-like cancer subtype (30,31); in
addition, the downregulation of claudin 1 has been found to be
associated with ER positivity and poor prognosis (31,32).
Indeed, the individual expression of claudins has
been reported to be limited and controversial (33). Claudins 4 and 7 are the most commonly
identified in breast tissue (33),
and both have been reported as potential markers for clinical
outcomes (21,31,34–37). In
the present study, although the majority of the evaluated IBC cases
exhibited preserved claudin 4 and 7 expression, (62 and 46%,
respectively) the distribution of the claudin-low or negative cases
did not correspond to the triple-negative molecular profile. Only
15.7% of the patients in this study were negative for both
claudins, and this frequency is consistent with that reported in
the literature (11,14,38,39).
Claudin 4-negative cases (36% of our total cases)
were more common among the luminal profile cases (ER+,
PR+ and HER-2−), with a smaller amount in the
triple-negative subtype, followed by the HER-2 expression enriched
subgroup. The same pattern was verified on negative claudin 7
results, although without statistical significance. The most
important finding in this study is the inverse association between
claudin 4 and ER/PR expression, which indicates that he majority of
claudin-negative cases (71.3%) were actually clustered among the
ER-positive cases, or luminal subtype. Szasz et al (40) also suggested that claudin 4 was less
expressed in luminal cancers.
Myal et al (41) proposed a ‘claudin-high’ subtype,
which comprises ER-negative tumors exhibiting high claudin 4
expression. Some studies (21,30,36,39)
reported that claudin 4 was associated with shorter disease-free
survival in the luminal cancer group, an association not confirmed
in our series. However, this feature must be further investigated
in multivariate analyses in order to estimate the possible
contribution of other prognostic variables in the association.
However, Lu et al (13) defined different criteria for
considering cases as ‘claudin-low’: For these authors, five
subtypes of claudins (1,3,4,7 and 8)
should be altered for the status to be named ‘claudin-low’, and the
authors reported that only 3% of claudin-low tumors belonged to the
luminal phenotype. However, in the evaluation of other claudin-low
characteristics in our study, such as the cancer stem cell-like
phenotype in the negative cases, no association was found between
the absence of claudin 4 and CD44+/CD24− and
unfavorable prognostic parameters, including overall and
disease-free survival.
Unexpectedly, previous results associating low
claudin 4 expression with a better prognosis, particularly in
patients with luminal subtypes of breast cancer, have been reported
(40). Paradoxically, claudin 4
positivity in our series was associated with poor prognostic
factors, such as higher tumor grade, presence of positive lymph
nodes and ER/PR negativity, which is in agreement with previous
reports (13,21,31,40).
Some prior studies have demonstrated that
immunohistochemical expression of claudin 4 was associated with the
basal phenotype (30,42) and triple-negative subtype (43). However, our results indicated that
claudin 4 was mostly found among cases with the HER-2 subtype, and
this finding is in agreement with others reports (22). These findings were substantiated by a
logistic regression analysis, which found claudin 4 positivity to
be significantly associated with HER-2 positivity. However, our
findings were not indicative of a correlation between claudin
expression and unfavorable prognosis.
There was no statistically significant association
between the expression of claudin 7 and any of the
clinicopathological parameters evaluated in our cases,
contradicting previous studies reporting increased claudin 7
expression in ER-positive and decreased expression in ER-negative
breast tumors, or an association with high histological grade
(13,34,44,45).
Preliminary results of our group were previously reported in a
smaller number of cases, showing that claudin 7 was associated with
shorter recurrence-free interval (28). However, in the present study, which
included a larger number of cases, there was no observed
association of claudin 7 with worse prognosis in the univariate
analysis. Other authors demonstrated a distinct prognostic role for
claudins 1, 4 and 7 in other studies including a smaller number of
patients (13,21,37,40).
If the triple-negative subtype is prone to exhibit
lack of adhesion molecules, particularly claudins, it may be
hypothesized that epithelial-to-mesenchymal transition, frequently
described in this context, may explain this phenomenon. The focus
of this study has been on claudins 4 and 7, and it was concluded
that the absence of these two distinct types of claudins did not
confer a worse prognosis or lower survival rate in our series. It
appears that cell adhesion abnormalities and aggressive behavior
are not dependent on one single class of these proteins (46).
Triple-negative tumors are difficult to subclassify,
as they are a very heterogeneous group. Since Hennessy et al
(11) identified a potentially
highly aggressive subtype of triple-negative breast cancers as
‘claudin-low’, efforts have been focused on differentiating those
cases from the less severe triple-negative cancers. Recently, ER,
PR and HER-2, the immunohistochemically detected tumor markers that
are known to be of great value in the treatment of breast cancer,
were incorporated into the AJCC Breast TNM Staging System (47) to refine prognosis. It would be very
useful if claudin protein expression, based on reproducible
immunohistochemical assays, could accurately identify the cases
with worse prognosis among all triple-negative tumors. However, it
appears that the protein expression in paraffin-embedded tissues
does not reflect the claudin RNA level determined by microarray
and, therefore, is not considered a safe evaluation for
prognosis.
As the majority of data on claudin-low breast
cancers were reported among triple-negative cases, particularly in
metaplastic carcinomas, we attempted to determine whether claudin
expression at the protein level can differentiate cases with worse
prognosis within breast cancer molecular subtypes. Our results
demonstrated that claudin 4 and 7 status was not indicative of a
better or worse outcome within breast cancer subtypes. Some of the
reports linking metaplastic carcinoma to claudin expression were
based on immunohistochemistry results (22). Moreover, by assessing the presence of
a given protein by immunohistochemistry within the tumor, the
result is ensured to reflect neoplastic cells rather than normal
tissue contamination. This is particularly important for claudin
identification, since the claudin-low phenotype or the absence or
claudin expression as a result will not be affected by the presence
of stromal desmoplastic tissue samples. Unavailability of
immunohistochemistry data may hinder the evaluation of the
molecular subtypes, as the materials may not be sufficient for TMA
analysis (20).
In summary, our results indicated that, despite
claudin 4 positivity being correlated with poor prognostic factors,
such as increased tumor grade, presence of positive lymph nodes and
ER/PR negativity, claudin-low cases (including low expression of
claudins 4 and 7) evaluated by immunohistochemistry did not
correspond to triple-negative breast cancer molecular profile.
Therefore, individual evaluation of claudin expression alone may
not allow for an accurate correlation with the triple-negative
subtype of the disease.
Acknowledgements
The authors wish to thank Dr Mônica Maria Agata
Stiepcich for compiling clinical data from TMA and Dr Maria Dirley
Ferreira de Souza Begnami for performing the immunohystochemical
reactions for claudins 4 and 7.
Funding
This study received financial support from FAPESP
(Fundação de Amparo à Pesquisa do Estado de São Paulo) and CNPq
(Conselho Nacional de Desenvolvimento Científico e
Tecnológico).
Availability of data and materials
All the data reported in the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
AFL, FAS and MMB designed the study and wrote the
manuscript. AFL, FSP, SN, RMR collected and analyzed data. All the
authors have reviewed the manuscript critically and approved the
final version of this manuscript.
Ethics approval and consent to
participate
The present study was conducted following approval
of the local Ethics Committee. The hospital obtained informed
consent forms from all patients for using archived tissues for
research at any time. Patient anonymity was guaranteed.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Marchio C, Balmativola D, Castiglione R,
Annaratone L and Sapino A: Predictive diagnostic pathology in the
target therapy era in breast cancer. Curr Drug Targets. 18:4–12.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mardekian SK, Bombonati A and Palazzo JP:
Ductal carcinoma in situ of the breast: The importance of
morphologic and molecular interactions. Hum Pathol. 49:114–23.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sørlie T, Perou CM, Tibshirani R, Aas T,
Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey
SS, et al: Gene expression patterns of breast carcinomas
distinguish tumor subclasses with clinical implications. Proc Natl
Acad Sci USA. 98:10869–10874. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
El-Rehim Abd DM, Ball G, Pinder SE, Rakha
E, Paish C, Robertson JF, Macmillan D, Blamey RW and Ellis IO:
High-throughput protein expression analysis using tissue microarray
technology of a large well-characterised series identifies
biologically distinct classes of breast cancer confirming recent
cDNA expression analyses. Int J Cancer. 116:340–350. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cheang MC, Chia SK, Voduc D, Gao D, Leung
S, Snider J, Watson M, Davies S, Bernard PS, Parker JS, et al: Ki67
index, HER2 status, and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tang P and Tse GM: Immunohistochemical
surrogates for molecular classification of breast carcinoma: A 2015
update. Arch Pathol Lab Med. 140:806–814. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hagemann IS: Molecular testing in breast
cancer: A guide to current practices. Arch Pathol Lab Med.
140:815–824. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tan W, Li Q, Chen K, Su F, Song E and Gong
C: Estrogen receptor beta as a prognostic factor in breast cancer
patients: A systematic review and meta-analysis. Oncotarget.
7:10373–10385. 2016.PubMed/NCBI
|
|
9
|
Matsumoto A, Jinno H, Ando T, Fujii T,
Nakamura T, Saito J, Takahashi M, Hayashida T and Kitagawa Y:
Biological markers of invasive breast cancer. Jpn J Clin Oncol.
46:99–105. 2016.PubMed/NCBI
|
|
10
|
Lehmann U, Albat C and Kreipe H:
High-resolution quantitative methylation analysis of microRNA genes
using Pyrosequencing™. Methods Mol Biol. 878:229–240. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hennessy BT, Gonzalez-Angulo AM,
Stemke-Hale K, Gilcrease MZ, Krishnamurthy S, Lee JS, Fridlyand J,
Sahin A, Agarwal R, Joy C, et al: Characterization of a naturally
occurring breast cancer subset enriched in
epithelial-to-mesenchymal transition and stem cell characteristics.
Cancer Res. 69:4116–4124. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lin X, Shang X, Manorek G and Howell SB:
Regulation of the epithelial-mesenchymal transition by claudin-3
and claudin-4. PLoS One. 8:e674962013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lu S, Singh K, Mangray S, Tavares R, Noble
L, Resnick MB and Yakirevich E: Claudin expression in high-grade
invasive ductal carcinoma of the breast: Correlation with the
molecular subtype. Mod Pathol. 26:485–495. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Prat A, Parker JS, Karginova O, Fan C,
Livasy C, Herschkowitz JI, He X and Perou CM: Phenotypic and
molecular characterization of the claudin-low intrinsic subtype of
breast cancer. Breast Cancer Res. 12:R682010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Singh AB and Dhawan P: Claudins and
cancer: Fall of the soldiers entrusted to protect the gate and keep
the barrier intact. Semin Cell Dev Biol. 42:58–65. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Khan N and Asif AR: Transcriptional
regulators of claudins in epithelial tight junctions. Mediators
Inflamm. 2015:2198432015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Achari C, Winslow S and Larsson C: Down
regulation of CLDND1 induces apoptosis in breast cancer cells. PLoS
One. 10:e01303002015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Iravani O, Yip GW, Thike AA, Chua PJ,
Scully Jane O, Tan PH and Bay BH: Prognostic significance of
Claudin 12 in estrogen receptor-negative breast cancer. J Clin
Pathol. 69:878–883. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Katayama A, Handa T, Komatsu K, Togo M,
Horiguchi J, Nishiyama M and Oyama T: Expression patterns of
claudins in patients with triple-negative breast cancer are
associated with nodal metastasis and worse outcome. Pathol Int.
67:404–413. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dias K, Dvorkin-Gheva A, Hallett RM, Wu Y,
Hassell J, Pond GR, Levine M, Whelan T and Bane AL: Claudin-low
breast cancer; clinical and pathological characteristics. PLoS One.
12:e01686692017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lanigan F, McKiernan E, Brennan DJ,
Hegarty S, Millikan RC, McBryan J, Jirstrom K, Landberg G, Martin
F, Duffy MJ and Gallagher WM: Increased claudin-4 expression is
associated with poor prognosis and high tumour grade in breast
cancer. Int J cancer. 124:2088–2097. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gerhard R, Ricardo S, Albergaria A, Gomes
M, Silva AR, Logullo ÂF, Cameselle-Teijeiro JF, Paredes J and
Schmitt F: Immunohistochemical features of claudin-low intrinsic
subtype in metaplastic breast carcinomas. Breast. 21:354–360. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rakha EA, El-Sayed ME, Lee AH, Elston CW,
Grainge MJ, Hodi Z, Blamey RW and Ellis IO: Prognostic significance
of nottingham histologic grade in invasive breast carcinoma. J Clin
Oncol. 26:3153–3158. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mangone FR, Brentani MM, Nonogaki S,
Begnami MD, Campos AH, Walder F, Carvalho MB, Soares FA, Torloni H,
Kowalski LP and Federico MH: Overexpression of Fos-related
antigen-1 in head and neck squamous cell carcinoma. Int J Exp
Pathol. 86:205–212. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Allred DC, Harvey JM, Berardo M and Clark
GM: Prognostic and predictive factors in breast cancer by
immunohistochemical analysis. Mod Pathol. 11:155–168.
1998.PubMed/NCBI
|
|
26
|
Wolff AC, Hammond ME, Hicks DG, Dowsett M,
McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M,
Fitzgibbons P, et al: Recommendations for human epidermal growth
factor receptor 2 testing in breast cancer: American Society Of
Clinical Oncology/College of American Pathologists clinical
practice guideline update. Arch Pathol Lab Med. 138:241–256. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wolff AC, Hammond ME, Hicks DG, Dowsett M,
McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M,
Fitzgibbons P, et al: Recommendations for human epidermal growth
factor receptor 2 testing in breast cancer: American Society of
Clinical Oncology/College of American Pathologists clinical
practice guideline update. J Clin Oncol. 31:3997–4013. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bernardi MA, Logullo AF, Pasini FS,
Nonogaki S, Blumke C, Soares FA and Brentani MM: Prognostic
significance of CD24 and claudin-7 immunoexpression in ductal
invasive breast cancer. Oncol Rep. 27:28–38. 2012.PubMed/NCBI
|
|
29
|
Carey LA, Perou CM, Livasy CA, Dressler
LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S,
et al: Race, breast cancer subtypes, and survival in the Carolina
breast cancer study. JAMA. 295:2492–2502. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Blanchard AA, Zelinski T, Xie J, Cooper S,
Penner C, Leygue E and Myal Y: Identification of claudin 1
transcript variants in human invasive breast cancer. PLoS One.
11:e01633872016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Blanchard AA, Skliris GP, Watson PH,
Murphy LC, Penner C, Tomes L, Young TL, Leygue E and Myal Y:
Claudins 1, 3, and 4 protein expression in ER negative breast
cancer correlates with markers of the basal phenotype. Virchows
Arch. 454:647–656. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Morohashi S, Kusumi T, Sato F, Odagiri H,
Chiba H, Yoshihara S, Hakamada K, Sasaki M and Kijima H: Decreased
expression of claudin-1 correlates with recurrence status in breast
cancer. Int J Mol Med. 20:139–143. 2007.PubMed/NCBI
|
|
33
|
Kwon MJ: Emerging roles of claudins in
human cancer. Int J Mol Sci. 14:18148–18180. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kominsky SL, Argani P, Korz D, Evron E,
Raman V, Garrett E, Rein A, Sauter G, Kallioniemi OP and Sukumar S:
Loss of the tight junction protein claudin-7 correlates with
histological grade in both ductal carcinoma in situ and invasive
ductal carcinoma of the breast. Oncogene. 22:2021–2033. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Soini Y: Expression of claudins 1, 2, 3,
4, 5 and 7 in various types of tumours. Histopathology. 46:551–560.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Tokés AM, Kulka J, Paku S, Szik A, Páska
C, Novák PK, Szilák L, Kiss A, Bögi K and Schaff Z: Claudin-1, −3
and −4 proteins and mRNA expression in benign and malignant breast
lesions: a research study. Breast Cancer Res. 7:R296–R305. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kolokytha P, Yiannou P, Keramopoulos D,
Kolokythas A, Nonni A, Patsouris E and Pavlakis K: Claudin-3 and
claudin-4: Distinct prognostic significance in triple-negative and
luminal breast cancer. Appl Immunohistochem Mol Morphol.
22:125–131. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Prat A and Perou CM: Deconstructing the
molecular portraits of breast cancer. Mol Oncol. 5:5–23. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Sabatier R, Finetti P, Guille A, Adelaide
J, Chaffanet M, Viens P, Birnbaum D and Bertucci F: Claudin-low
breast cancers: Clinical, pathological, molecular and prognostic
characterization. Mol Cancer. 13:2282014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Szasz AM, Nemeth Z, Gyorffy B, Micsinai M,
Krenacs T, Baranyai Z, Harsanyi L, Kiss A, Schaff Z, Tokes AM and
Kulka J: Identification of a claudin-4 and E-cadherin score to
predict prognosis in breast cancer. Cancer Sci. 102:2248–2254.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Myal Y, Leygue E and Blanchard AA: Claudin
1 in breast tumorigenesis: Revelation of a possible novel ‘claudin
high’ subset of breast cancers. J Biomed Biotechnol.
2010:9568972010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kulka J, Szász AM, Németh Z, Madaras L,
Schaff Z, Molnár IA and Tokés AM: Expression of tight junction
protein claudin-4 in basal-like breast carcinomas. Pathol Oncol
Res. 15:59–64. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Prat A, Karginova O, Parker JS, Fan C, He
X, Bixby L, Harrell JC, Roman E, Adamo B, Troester M and Perou CM:
Characterization of cell lines derived from breast cancers and
normal mammary tissues for the study of the intrinsic molecular
subtypes. Breast Cancer Res Treat. 142:237–255. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Sauer T, Pedersen MK, Ebeltoft K and Naess
O: Reduced expression of Claudin-7 in fine needle aspirates from
breast carcinomas correlate with grading and metastatic disease.
Cytopathology. 16:193–198. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Park D, Kåresen R, Axcrona U, Noren T and
Sauer T: Expression pattern of adhesion molecules ((E-cadherin,
alpha-, beta-, gamma-catenin and claudin-7), their influence on
survival in primary breast carcinoma, and their corresponding
axillary lymph node metastasis. APMIS. 115:52–65. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Farahani E, Patra HK, Jangamreddy JR,
Rashedi I, Kawalec M, Pariti Rao RK, Batakis P and Wiechec E: Cell
adhesion molecules and their relation to (cancer) cell stemness.
Carcinogenesis. 35:747–759. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Giuliano AE, Connolly JL, Edge SB,
Mittendorf EA, Rugo HS, Solin LJ, Weaver DL, Winchester DJ and
Hortobagyi GN: Breast cancer-major changes in the American Joint
Committee on Cancer eighth edition cancer staging manual. CA Cancer
J Clin. 67:290–303. 2017. View Article : Google Scholar : PubMed/NCBI
|