Introduction
Hepatocellular carcinoma (HCC) is the sixth most
common neoplasm and the third most frequent cause of cancer
mortality (1). Treatment strategy is
determined based on liver function, number of tumors, tumor size,
vascular invasion and extrahepatic metastases (2,3). The
first approach in the management of HCC is to determine if either
hepatic resection or liver transplantation is feasible. As the
majority of HCC cases develop in patients with cirrhosis, surgical
interventions may become challenging. Patients with a small
solitary tumor and very well preserved liver function are the best
candidates for hepatic resection. Liver transplantation is most
beneficial for patients who are not good candidates for resection,
particularly those with Milan criteria (solitary tumor ≤5 cm and up
to three nodules ≤3 cm) (4);
however, donor shortage greatly limits its applicability.
Percutaneous ablation is the most frequently used treatment;
however, its effectiveness is limited by tumor size and
localization (5). In patients with
multiple tumors without vascular invasion or extrahepatic
metastases not amenable to curative treatments, chemoembolization
may provide survival benefit. Findings of randomized trials of
sorafenib have demonstrated survival benefits for patients with
advanced HCC (6,7), suggesting that molecular-targeted
therapies could be effective in this chemoresistant cancer.
Notable advances in surgical procedures and imaging
modalities have improved the outcome of patients with HCC (8). However, the long-term prognosis remains
unsatisfactory due to a high incidence of recurrence even after
curative resection of HCC, with a 5-year actuarial recurrence rate
of >80% (9–12). The main prognostic factors following
hepatic resection for HCC include the stage of the cancer, vascular
invasion, the number of tumors and liver function (5). As liver function correlates well with
the degree of liver fibrosis (13,14),
there is a need to develop accurate and reliable noninvasive means
to assess the severity of liver fibrosis. The aspartate
aminotransferase to platelet ratio index (APRI) is a simple
noninvasive index, and may be used to predict significant fibrosis
and cirrhosis in patients with chronic hepatitis C (15–17).
APRI was reported to predict postoperative prognosis for solitary
small hepatitis B-related HCC (18).
The present study aimed to analyze whether APRI could predict the
prognosis following hepatic resection for HCC in general.
Patients and methods
Patient selection
The present retrospective study was approved by the
Ethics Committee of The Jikei University School of Medicine (Tokyo,
Japan). Between January 2000 and December 2011, 186 patients with
HCC underwent hepatic resection at the Department of Surgery, Jikei
University Hospital (Tokyo, Japan). Of these, 24 patients were
excluded for the following reasons: A total of 11 patients had
difficult pathological diagnosis due to complete necrosis by
preoperative transcatheter arterial chemoembolization; 9 patients
had additional procedures for other malignancies; 3 patients lost
their lives due to other disease; and 1 patient did not have an
indocyanine green test due to iodine allergy, leaving the remaining
162 patients for the present study. All patients underwent
macroscopic curative resection for HCC. The patient characteristics
are listed in Table I.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Factor | Ratio or median | Range |
|---|
| Sex
(male:female) | 138:24 | – |
| Age, years | 63 | 29–82 |
| Virus type
(NBNC:HBV:HCV:HBV+HCV) | 53:43:64:2 | – |
| Total bilirubin,
mg/dl | 0.8 | 0.1–3.0 |
| Albumin, g/dl | 3.9 | 2.5–5.0 |
| Aspartate
aminotransferase, IU/l | 38 | 8–261 |
| Alanine
aminotransferase, IU/l | 36 | 9–269 |
| Platelet,
×103/µl | 15.1 | 5.1–50.7 |
| Prothrombin time,
% | 90 | 54–100 |
| Retention rate of
indocyanine green at 15 min, % | 12 | 2–51 |
| Child-Pugh (A:B) | 150:12 | – |
| Liver damage
(A:B) | 124:38 | – |
| Aspartate
aminotransferase to platelet ratio index | 0.58 | 0.101–5.918 |
| Surgery
(anatomical:partial) | 93:69 | – |
| Estimated blood
loss, ml | 745 | (0–25, 770) |
| Surgery time,
min | 365 | 100-1,030 |
| Perioperative blood
transfusion of red cell concentrates (present:absent) | 47:115 | – |
| Perioperative blood
transfusion of fresh frozen plasma (present:absent) | 55:107 | – |
| Maximum diameter of
tumor, cm | 3.5 | 0.9–18.0 |
| Number of tumors
(solitary:multiple) | 132:30 | – |
| Vascular invasion
(present:absent) | 40:122 | – |
| Differentiation
(well or moderately:poorly) | 147:15 | – |
| Liver cirrhosis
(present:absent) | 70:92 | – |
| Union for
International Cancer Control | 99:48:7:6:1:1 | – |
| TNM classification
(stage I:II:IIIA:IIIB:IIIC:IVB) |
|
|
APRI was calculated as the ratio of [(aspartate
aminotransferase/upper limit of normal value: 45 IU/l)/platelet
counts (×103/µl)] ×100. In general, the extent of
hepatic resection was determined based on the retention rate of
indocyanine green at 15 min (ICG-R15) before surgery (19). The type of resection was classified
into two types: Anatomical resection (trisegmentectomy, extended
lobectomy, lobectomy, segmentectomy or subsegmentectomy) and
non-anatomical resection. The use of blood products and the dose
were determined, as previously described (20). Tumor staging was based on the TNM
stage classified by the Union for International Cancer Control
(UICC) (21).
Univariate and multivariate analyses
of disease-free and overall survival following hepatic resection,
and clinicopathological factors
Initially, the relationship between
clinicopathological variables and disease-free survival and overall
survival following hepatic resection was investigated by univariate
and multivariate analysis. The clinicopathological variables
consisted of the following 15 factors: Age, sex, type of hepatitis
virus, serum total bilirubin, serum albumin, prothrombin time (PT),
ICG-R15, Child-Pugh classification (22), APRI, type of resection, surgery time,
estimated blood loss, perioperative blood transfusion o f red cell
concentrates (RCC), differentiation of tumor and TNM stage.
Determination of cut-off value of
variables
Some clinicopathological continuous variables were
classified into two groups for the log-rank test and the Cox
proportional hazard regression models, as follows: Age, <60 or
≥60 years; albumin, ≤3.5 or <3.5 g/dl; PT, ≤80 or >80%;
ICG-R15, <15 or ≥15%, according to previous studies (22,23); and
serum total bilirubin, <1.4 or ≥1.4 mg/dl, based on the normal
limit in our facility. The median of variables in operative factors
was classified as follows: Surgery time, <360 or ≥360 min; and
estimated blood loss, <745 or ≥745 ml. A cut-off value of APRI
was determined by a receiver operating curve (ROC) of APRI, which
was 0.45.
Assessment of clinicopathological
variables and APRI
The subjects were classified into two groups: APRI,
<0.45 or ≥0.45. Subsequently, patients' characteristics were
analyzed in relation to APRI, using the following 18 factors: Age,
sex, type of hepatitis virus, serum total bilirubin, serum albumin,
PT%, ICG-R15, Child-Pugh classification, type of resection,
estimated blood loss, surgery time, perioperative blood transfusion
of RCC, differentiation, liver cirrhosis and UICC TNM stage.
The recurrence of HCC was defined as newly detected
hypervascular hepatic or extrahepatic tumors by ultrasonography,
computed tomography, magnetic resonance image or angiography with
or without increase in serum a-fetoprotein, or protein induced by
vitamin K absence or antagonist-II. For recurrent HCC in the liver,
repeated hepatic resection, local ablation therapy, transarterial
chemoembolization or molecular target therapy (sorafenib) was given
based on hepatic functional reserve judged mainly by ICG-R15.
Extrahepatic recurrence was mainly treated conservatively, except
for solitary lung metastasis or adrenal gland metastasis, provided
that the primary HCC was controlled. In such a circumstance,
limited partial resections were performed.
Statistical analysis
Data were expressed as the mean ± standard deviation
or median (minimum to maximum). Univariate analysis was performed
using the non-paired Student's t-test and Chi-square test. Analysis
of disease-free and overall survival was performed using the
log-rank test. Factors that significantly influenced disease-free
or overall survival were then used in the Cox proportional
regression model for multivariate analysis. P<0.05 was
considered to indicate a statistically significant difference. The
accuracy of APRI for pathological liver cirrhosis was determined by
calculating the area under the curve from corresponding receiver
curves (AUROC) using SPSS 17.0 for Windows, (SPSS. Inc., Chicago,
IL, USA). The AUROC was expressed as plots of the test sensitivity
vs. 1-speificity.
Results
Clinical patient characteristics
The background characteristics of the 162 patients
are summarized in Table I. There
were 138 men and 24 women. The median age was 63 years (range,
29–82 years). The majority of patients had hepatitis C virus (HCV)
infection (n=64), followed by those without HCV or hepatitis B
virus (HBV) infection (n=53) and those with HBV infection (n=43).
The majority of patients were in Child-Pugh grade A and liver
damage grade A. The median APRI was 0.576 (range 0.101–5.918) and
70 patients (43.2%) had the pathological diagnosis of liver
cirrhosis.
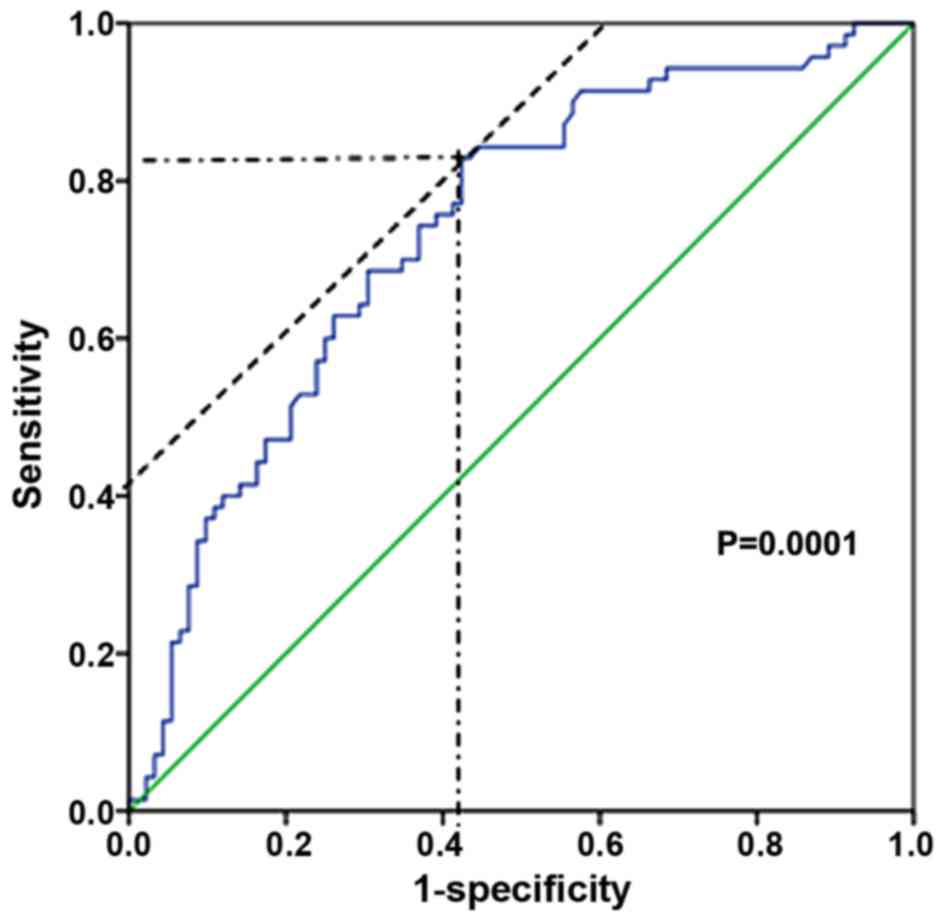
Cut-off value of APRI using a ROC
A cut-off value of APRI was determined by a ROC of
APRI, which predicted liver cirrhosis based on pathological
diagnosis (Fig. 1). APRI yielded
high AUROC with a level of 0.736 at a cut-off value of 0.45
(sensitivity, 0.829; 1-specificity, 0.424).
Variables associated with overall and
disease-free survival in univariate and multivariate analyses
Table II
demonstrates the relationship between the clinicopathological
variables and disease-free survival following hepatic resection for
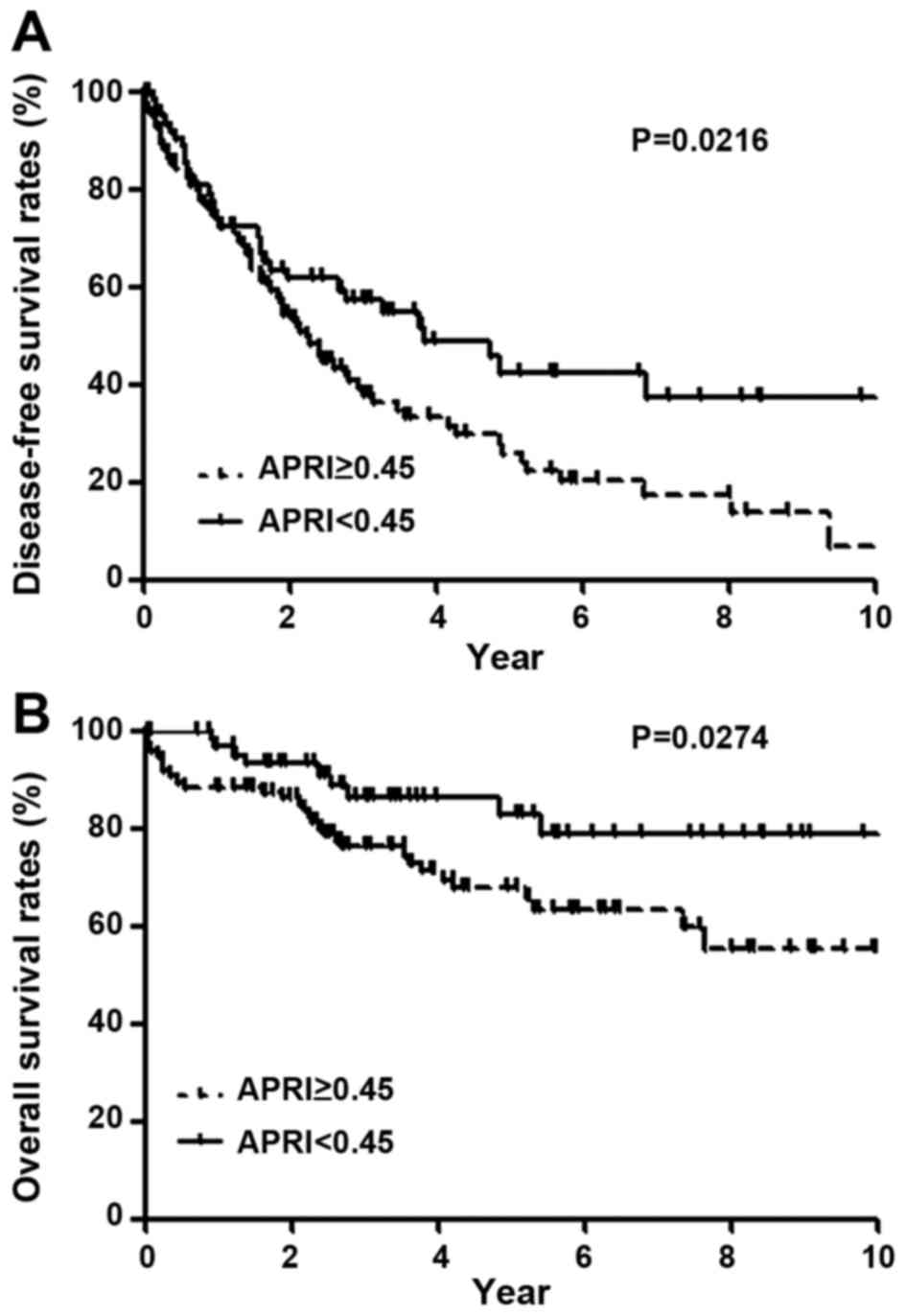
HCC. In univariate analysis, disease-free survival was
significantly poor in patients with age ≥65 years (P=0.0244),
ICG-R15 ≥15% (P=0.0043), APRI ≥0.45 (P=0.0216; Fig. 2A), perioperative blood transfusion of
RCC (P=0.0008), and TNM stage II, III or IV (P=0.0076). In
multivariate analysis, ICG-R15 ≥15% (P=0.0306), APRI ≥0.45
(P=0.0184), perioperative blood transfusion of RCC (P=0.0034), and
TNM stage II, III or IV (P=0.0184) were independent and significant
predictors of poor disease-free survival.
| Table II.Univariate and multivariate analysis
of disease-free survival following hepatic resection. |
Table II.
Univariate and multivariate analysis
of disease-free survival following hepatic resection.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Factor | Patient no. | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| Age, years |
|
|
|
|
|
|
≥65 | 73 | 1.606
(1.063–2.427) | 0.0244 | 1.37
(0.915–2.050) | 0.1263 |
|
<65 | 89 |
|
|
|
|
| Sex |
|
|
|
|
|
|
Male | 138 | 1.096
(0.5981–2.007) | 0.7671 | – | – |
|
Female | 24 |
|
|
|
|
| Hepatitis
virus |
|
|
|
|
|
| HCV
infection | 66 | 1.256
(0.8377–1.883) | 0.27 | – | – |
| Non-HCV
infection | 96 |
|
|
|
|
| Total bilirubin,
mg/dl |
|
|
|
|
|
|
≥1.4 | 9 | 2.008
(0.7999–5.039) | 0.1377 | – | – |
|
<1.4 | 153 |
|
|
|
|
| Albumin, g/dl |
|
|
|
|
|
|
≤3.5 | 33 | 1.437
(0.8660–2.386) | 0.1605 | – | – |
|
>3.5 | 129 |
|
|
|
|
| Prothrombin time,
% |
|
|
|
|
|
|
>80 | 129 | 1.522
(0.8694–2.665) | 0.1415 | – | – |
|
≤80 | 33 |
|
|
|
|
| Retention rate of
indocyanine green at 15 min, % |
|
|
|
|
|
|
≥15 | 67 | 1.876
(1.219–2.889) | 0.0043 | 1.586
(1.044–2.410) | 0.0306 |
|
<15 | 95 |
|
|
|
|
| Child-Pugh |
|
|
|
|
|
| B | 12 | 2.124
(0.9176–4.917) | 0.0785 | – | – |
| A | 150 |
|
|
|
|
| Aspartate
aminotransferase to platelet ratio index |
|
|
|
|
|
|
≥0.45 | 97 | 1.598
(1.071–2.382) | 0.0216 | 1.692
(1.093–2.620) | 0.0184 |
|
<0.45 | 65 |
|
|
|
|
| Surgical
procedure |
|
|
|
|
|
|
Anatomical | 93 | 1.003
(0.6753–1.491) | 0.9868 | – | – |
|
Non-anatomical | 69 |
|
|
|
|
| Surgery time,
min |
|
|
|
|
|
|
≥360 | 82 | 1.274
(0.8522–1.903) | 0.238 | – | – |
|
<360 | 80 |
|
|
|
|
| Estimated blood
loss, g |
|
|
|
|
|
|
≥745 | 81 | 1.417
(0.9524–2.109) | 0.0856 | – | – |
|
<745 | 81 |
|
|
|
|
| Perioperative blood
transfusion of red cell concentrates |
|
|
|
|
|
|
Present | 47 | 2.257
(1.404–3.628) | 0.0008 | 1.875
(1.231–2.857) | 0.0034 |
|
Absent | 115 |
|
|
|
|
|
Differentiation |
|
|
|
|
|
| Well or
moderate | 147 | 1.062
(0.5238–2.154) | 0.8669 | – | – |
|
Poor | 15 |
|
|
|
|
| Union for
International Cancer Control Stage |
|
|
|
|
|
| I | 99 | 1.783
(1.166–2.727) | 0.0076 | 1.637
(1.087–2.465) | 0.0184 |
| II, III
or IV | 63 |
|
|
|
|
Table III
demonstrates the relationship between the clinicopathological
variables and overall survival following hepatic resection for HCC.
In univariate analysis, overall survival was poor in patients with
ICG-R15 ≥15% (P=0.0084), APRI ≥0.45 (P=0.0274; Fig. 2B), perioperative blood transfusion of
RCC (P=0.0002), and TNM stage II, III or IV (P=0.0003). In
multivariate analysis, ICG-R15 ≥15% (P=0.0454), APRI ≥0.45
(P=0.0417), perioperative blood transfusion of RCC (P=0.0036), and
TNM stage II, III or IV (P=0.0033) were independent and significant
negative predictors.
| Table III.Univariate and multivariate analysis
of overall survival following hepatic resection. |
Table III.
Univariate and multivariate analysis
of overall survival following hepatic resection.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Factor | Patient no. | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| Age, years |
|
|
|
|
|
|
≥65 | 73 | 1.520
(0.8026–2.880) | 0.1987 | – | – |
|
<65 | 89 |
|
|
|
|
| Sex |
|
|
|
|
|
|
Male | 138 | 2.007
(0.7824–5.148) | 0.1472 | – | – |
|
Female | 24 |
|
|
|
|
| Hepatitis
virus |
|
|
|
|
|
| HCV
infection | 66 | 1.317
(0.6969–2.492) | 0.7155 | – | – |
| Non-HCV
infection | 96 |
|
|
|
|
| Total bilirubin,
mg/dl |
|
|
|
|
|
|
≥1.4 | 9 | 1.381
(0.3641–5.2236) | 0.6353 | – | – |
|
<1.4 | 153 |
|
|
|
|
| Albumin, g/dl |
|
|
|
|
|
|
≤3.5 | 33 | 1.561
(0.6987–3.488) | 0.2776 | – | – |
|
>3.5 | 129 |
|
|
|
|
| Prothrombin time,
% |
|
|
|
|
|
|
>80 | 129 | 2.078
(0.8750–4.936) | 0.0974 | – | – |
|
≤80 | 33 |
|
|
|
|
| Retention rate of
indocyanine green at 15 min, % |
|
|
|
|
|
|
≥15 | 67 | 2.460
(1.260–4.804) | 0.0084 | 1.966
(1.014–3.813) | 0.0454 |
|
<15 | 95 |
|
|
|
|
| Child-Pugh |
|
|
|
|
|
| B | 12 | 3.252
(0.8717–12.13) | 0.0792 | – | – |
| A | 150 |
|
|
|
|
| Aspartate
aminotransferase to platelet ratio index |
|
|
|
|
|
|
≥0.45 | 97 | 2.054
(1.083–3.896) | 0.0274 | 2.239
(1.031–4.862) | 0.0417 |
|
<0.45 | 65 |
|
|
|
|
| Surgical
procedure |
|
|
|
|
|
|
Anatomical | 93 | 1.859
(0.9857–3.505) | 0.0554 | – | – |
|
Non-anatomical | 69 |
|
|
|
|
| Surgery time,
min |
|
|
|
|
|
|
≥360 | 82 | 1.000
(0.5297–1.889) | 0.9994 | – | – |
|
<360 | 80 |
|
|
|
|
| Estimated blood
loss, g |
|
|
|
|
|
|
≥745 | 81 | 1.764
(0.9402–3.309) | 0.0771 | – | – |
|
<745 | 81 |
|
|
|
|
| Perioperative blood
transfusion of red cell concentrates |
|
|
|
|
|
|
Present | 47 | 3.679
(1.801–7.519) | 0.0002 | 2.607
(1.366–4.974) | 0.0036 |
|
Absent | 115 |
|
|
|
|
|
Differentiation |
|
|
|
|
|
| Well or
moderate | 147 | 2.237
(0.7414–6.752) | 0.153 | – | – |
|
Poor | 15 |
|
|
|
|
| Union for
International Cancer Control stage |
|
|
|
|
|
| I | 99 | 3.366
(1.732–6.542) | 0.0003 | 2.738
(1.399–5.358) | 0.0033 |
| II, III
or IV | 63 |
|
|
|
|
Univariate analysis of patient
characteristics in relation to APRI
Table IV
demonstrates the relationship between clinicopathological variables
and APRI. In univariate analysis, type of hepatitis virus (HCV
infection, P=0.002), liver function tests (serum total bilirubin,
P=0.0044; albumin, P=0.0002; PT%, P<0.0001; ICG-R15, P=0.0005),
and pathology-proven liver cirrhosis (P<0.0001) were positively
associated with APRI. Age (P=0.0524), type of resection (P=0.0653),
and Child Pugh classification (P=0.0849) demonstrated a trend
toward a positive association with APRI; however, these were not
significant.
| Table IV.Univariate analysis of patient
characteristics in relation to APRI. |
Table IV.
Univariate analysis of patient
characteristics in relation to APRI.
|
| APRI |
|
|---|
|
|
|
|
|---|
| Factor | ≥0.45 (n=97) | <0.45
(n=65) | Univariate
P-value |
|---|
| Sex
(male:female) | 82:15 | 56:9 | 0.7763 |
| Age, years | 63±9 | 60±13 | 0.0524 |
| Virus type |
|
(NBNC:HBV:HCV:HBV+HCV) | 21:27:48:1 | 32:16:16:1 | 0.0015 |
|
HCV:non-HCV | 49:48 | 17:48 | 0.0020 |
| Total bilirubin,
mg/dl | 0.9±0.4 | 0.8±0.3 | 0.0044 |
| Albumin, g/dl | 3.8±0.4 | 4.0±0.4 | 0.0002 |
| Prothrombin time,
% | 87±10 | 93±8 | <0.0001 |
| Retention rate of
indocyanine green at 15 min, % | 16±9 | 12±7 | 0.0005 |
| Child-Pugh
(A:B) | 87:10 | 63:2 | 0.0849 |
| Type of resection
(anatomical:non-anatomical) | 50:47 | 43:22 | 0.0653 |
| Estimated blood
loss, ml | 1,478±2,853 | 1,409±2,280 | 0.8707 |
| Surgery time,
min | 358±144 | 398±174 | 0.1558 |
| Perioperative blood
transfusion of red cell concentrates (present:absent) | 27:70 | 20:45 | 0.6867 |
| Differentiation
(well or moderate:poor) | 88:9 | 59:6 | 0.9918 |
| Liver cirrhosis
(present:absent) | 58:39 | 12:53 | <0.0001 |
| Union for
International Cancer Control stage (I:II, III or IV) | 60:37 | 39:26 | 0.8123 |
Discussion
Histological examination by biopsy remains an
important diagnostic modality to estimate the degree of liver
fibrosis (24). Although
percutaneous liver biopsy is, in general, a safe procedure, it is
costly and does carry a small risk of complication (25). Therefore, it is difficult to perform
liver biopsy for all preoperative patients with liver diseases. In
addition, sampling error may occur as only 1/50,000 of the whole
liver is sampled. Furthermore, inter- and intra-observer
discrepancies of 10–20% in assessing hepatic fibrosis have been
reported, which may lead to the misunderstanding of cirrhosis
(26–28). Therefore, the development of
noninvasive markers of liver fibrosis is a clinical and research
priority.
Some noninvasive indices, such as the amino-terminal
propeptide of collagen III, hyaluronic acid, Fibrotest, Fibrometer
test, Hepascore and FibroScan (transient elastography or liver
stiffness), have been introduced to assess the degree of fibrosis
(29). However, these tests usually
require special and costly equipment for daily practice. On the
other hand, APRI is a simple, noninvasive index derived from
routine blood tests, and correlates significantly with the stage of
fibrosis, with a higher correlation coefficient than platelet
count, or aspartate aminotransferase level alone, because it
amplifies the opposing effects of liver fibrosis on aspartate
aminotransferase and platelet count (15). Although APRI is a promising index
with limited expense and widespread availability, it has never been
reported as a prognostic factor of patients with HCC following
hepatic resection except in one report, in which APRI was advocated
to predict postoperative outcome in patients with solitary small
hepatitis B-related HCC (18). The
cut-off value of APRI in their report was 0.47, which was very
similar to the value in the present study of 0.45. On the other
hand, a difference was the patient criteria: The present study was
applied to operable patients with HCC regardless of type of
hepatitis virus, but the previous report was limited to solitary
and small hepatitis B-related HCC (18).
In patients with HCC, the incidence of concomitant
liver cirrhosis is much higher than chronic hepatitis, regardless
of type of hepatitis virus (30–32).
Depending on the etiology of liver cirrhosis, the lifetime risk for
the development of HCC is as high as 80% in patients with liver
cirrhosis (3). Therefore,
noninvasive fibrosis markers may be an important predictor of HCC
occurrence. In the present study, the difference in disease-free
survival is clearer later than 2 years after hepatic resection.
Then, this difference is due to multicentric occurrence of HCC
because intrahepatic recurrence via vascular invasion generally
occurs in the early period compared with multicentric recurrence
(9). The present study suggested
that APRI is a predictor of multicentric recurrence. Other
significant factors associated with overall or disease-free
survival on multivariate analysis were ICG-R15, TNM stage and
perioperative blood transfusion of RCC, which were consistent with
other reports (10,20,33–35).
In the present study, higher APRI values had a
positive association with the ratio of HCV infection. A
meta-analysis of patients undergoing hepatic resection for HCC
demonstrated that preoperative liver function, such as AST,
platelet count and Child-Pugh classification was worse in the
HCV-HCC group than in either the HBV-HCC or negative for both
markers of HBV and HCV infection [non-B, non-C (NBNC)]-HCC group
(36). The prevalence of liver
cirrhosis was the highest in the HCV-HCC group, followed by the
HBV-HCC group and the NBNC-HCC group (36). Therefore, the ratio of HCV infection
may be higher in the group of APRI ≥0.45 than APRI <0.45.
There are several limitations in the present study.
First, this is a retrospective study. It was not possible to
compare the APRI to other noninvasive indices, including the
amino-terminal propeptide of collagen III, hyaluronic acid,
FibroTest, FibroMeter test, Hepascore and Fibroscan (transient
elastography for liver stiffness). Second, the number of patients
who underwent hepatic resection was small, and so validation for
the survival rate following hepatic resection by using the value of
APRI could not be performed. To confirm the influence of APRI on
survival following hepatic resection, more case numbers or
prospective studies are required.
In conclusion, the present study suggests that APRI
derived from routine blood tests appears to be a significant
predictive factor of overall and disease-free survival following
hepatic resection for HCC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
The all authors conducted surgery and perioperative
management for patients, MM, SW, KH and HS contributed to the
clinical data analysis. MM and KY wrote the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Appropriate ethical approval was obtained from the
Institutional Review Board of The Jikei University School of
Medicine (Tokyo, Japan). Patient consent was not required for the
present study as it was conducted retrospectively.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Reig M, Darnell A, Forner A, Rimola J,
Ayuso C and Bruix J: Systemic therapy for hepatocellular carcinoma:
The issue of treatment stage migration and registration of
progression using the BCLC-refined RECIST. Semin Liver Dis.
34:444–455. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Forner A, Llovet JM and Bruix J:
Hepatocellular carcinoma. Lancet. 379:1245–1255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mazzaferro V, Regalia E, Doci R, Andreola
S, Pulvirenti A, Bozzetti F, Montalto F, Ammatuna M, Morabito A and
Gennari L: Liver transplantation for the treatment of small
hepatocellular carcinomas in patients with cirrhosis. N Engl J Med.
334:693–699. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Clinical Practice Guidelines for
Hepatocellular Carcinoma-The Japan Society of Hepatology 2009
update. Hepatol Res. 40 Suppl 1:S2–S144. 2010.
|
|
6
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S,
Kim JS, Luo R, Feng J, Ye S, Yang TS, et al: Efficacy and safety of
sorafenib in patients in the Asia-Pacific region with advanced
hepatocellular carcinoma: A phase III randomised, double-blind,
placebo-controlled trial. Lancet Oncol. 10:25–34. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Takayama T, Makuuchi M, Hirohashi S,
Sakamoto M, Yamamoto J, Shimada K, Kosuge T, Okada S, Takayasu K
and Yamasaki S: Early hepatocellular carcinoma as an entity with a
high rate of surgical cure. Hepatology. 28:1241–1246. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Imamura H, Matsuyama Y, Tanaka E, Ohkubo
T, Hasegawa K, Miyagawa S, Sugawara Y, Minagawa M, Takayama T,
Kawasaki S and Makuuchi M: Risk factors contributing to early and
late phase intrahepatic recurrence of hepatocellular carcinoma
after hepatectomy. J Hepatol. 38:200–207. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Poon RT, Ng IO, Fan ST, Lai EC, Lo CM, Liu
CL and Wong J: Clinicopathologic features of long-term survivors
and disease-free survivors after resection of hepatocellular
carcinoma: A study of a prospective cohort. J Clin Oncol.
19:3037–3044. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Poon RT, Fan ST, Lo CM, Liu CL and Wong J:
Intrahepatic recurrence after curative resection of hepatocellular
carcinoma: Long-term results of treatment and prognostic factors.
Ann Surg. 229:216–222. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yamamoto J, Kosuge T, Takayama T, Shimada
K, Yamasaki S, Ozaki H, Yamaguchi N and Makuuchi M: Recurrence of
hepatocellular carcinoma after surgery. Br J Surg. 83:1219–1222.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kusaka K, Harihara Y, Torzilli G, Kubota
K, Takayama T, Makuuchi M, Mori M and Omata S: Objective evaluation
of liver consistency to estimate hepatic fibrosis and functional
reserve for hepatectomy. J Am Coll Surg. 191:47–53. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kumazawa K, Edamoto Y, Yanase M and
Nakayama T: Liver analysis using
gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic
acid-enhanced magnetic resonance imaging: Correlation with
histological grading and quantitative liver evaluation prior to
hepatectomy. Hepatol Res. 42:1081–1088. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wai CT, Greenson JK, Fontana RJ,
Kalbfleisch JD, Marrero JA, Conjeevaram HS and Lok AS: A simple
noninvasive index can predict both significant fibrosis and
cirrhosis in patients with chronic hepatitis C. Hepatology.
38:518–526. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lin ZH, Xin YN, Dong QJ, Wang Q, Jiang XJ,
Zhan SH, Sun Y and Xuan SY: Performance of the aspartate
aminotransferase-to-platelet ratio index for the staging of
hepatitis C-related fibrosis: An updated meta-analysis. Hepatology.
53:726–736. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shaheen AA and Myers RP: Diagnostic
accuracy of the aspartate aminotransferase-to-platelet ratio index
for the prediction of hepatitis C-related fibrosis: A systematic
review. Hepatology. 46:912–921. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hung HH, Su CW, Lai CR, Chau GY, Chan CC,
Huang YH, Huo TI, Lee PC, Kao WY, Lee SD and Wu JC: Fibrosis and
AST to platelet ratio index predict post-operative prognosis for
solitary small hepatitis B-related hepatocellular carcinoma.
Hepatol Int. 4:691–699. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miyagawa S, Makuuchi M, Kawasaki S and
Kakazu T: Criteria for safe hepatic resection. Am J Surg.
169:589–594. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shiba H, Ishida Y, Wakiyama S, Iida T,
Matsumoto M, Sakamoto T, Ito R, Gocho T, Furukawa K, Fujiwara Y, et
al: Negative impact of blood transfusion on recurrence and
prognosis of hepatocellular carcinoma after hepatic resection. J
Gastrointest Surg. 13:1636–1642. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pugh RN, Murray-Lyon IM, Dawson JL,
Pietroni MC and Williams R: Transection of the oesophagus for
bleeding oesophageal varices. Br J Surg. 60:646–649. 1973.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Minagawa M, Ikai I, Matsuyama Y, Yamaoka Y
and Makuuchi M: Staging of hepatocellular carcinoma: Assessment of
the Japanese TNM and AJCC/UICC TNM systems in a cohort of 13,772
patients in Japan. Ann Surg. 245:909–922. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chevallier M, Guerret S, Chossegros P,
Gerard F and Grimaud JA: A histological semiquantitative scoring
system for evaluation of hepatic fibrosis in needle liver biopsy
specimens: Comparison with morphometric studies. Hepatology.
20:349–355. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cadranel JF, Rufat P and Degos F:
Practices of liver biopsy in France: Results of a prospective
nationwide survey. For the group of epidemiology of the French
association for the study of the liver (AFEF). Hepatology.
32:477–481. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Regev A, Berho M, Jeffers LJ, Milikowski
C, Molina EG, Pyrsopoulos NT, Feng ZZ, Reddy KR and Schiff ER:
Sampling error and intraobserver variation in liver biopsy in
patients with chronic HCV infection. Am J Gastroenterol.
97:2614–2618. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Westin J, Lagging LM, Wejstål R, Norkrans
G and Dhillon AP: Interobserver study of liver histopathology using
the Ishak score in patients with chronic hepatitis C virus
infection. Liver. 19:183–187. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Intraobserver and interobserver variations
in liver biopsy interpretation in patients with chronic hepatitis
C. The French METAVIR cooperative study group. Hepatology.
20:15–20. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shiha G, Sarin SK, Ibrahim AE, Omata M,
Kumar A, Lesmana LA, Leung N, Tozun N, Hamid S, Jafri W, et al:
Liver fibrosis: Consensus recommendations of the Asian pacific
association for the study of the liver (APASL). Hepatol Int.
3:323–333. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nishiguchi S, Kuroki T, Nakatani S,
Morimoto H, Takeda T, Nakajima S, Shiomi S, Seki S, Kobayashi K and
Otani S: Randomised trial of effects of interferon-alpha on
incidence of hepatocellular carcinoma in chronic active hepatitis C
with cirrhosis. Lancet. 346:1051–1055. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Liaw YF and Chu CM: Hepatitis B virus
infection. Lancet. 373:582–592. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kawaguchi T, Kakuma T, Yatsuhashi H,
Watanabe H, Saitsu H, Nakao K, Taketomi A, Ohta S, Tabaru A,
Takenaka K, et al: Data mining reveals complex interactions of risk
factors and clinical feature profiling associated with the staging
of non-hepatitis B virus/non-hepatitis C virus-related
hepatocellular carcinoma. Hepatol Res. 41:564–571. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yamamoto J, Kosuge T, Takayama T, Shimada
K, Yamasaki S, Ozaki H, Yamaguchi N, Mizuno S and Makuuchi M:
Perioperative blood transfusion promotes recurrence of
hepatocellular carcinoma after hepatectomy. Surgery. 115:303–309.
1994.PubMed/NCBI
|
|
34
|
Fujimoto J, Okamoto E, Yamanaka N, Tanaka
T and Tanaka W: Adverse effect of perioperative blood transfusions
on survival after hepatic resection for hepatocellular carcinoma.
Hepatogastroenterology. 44:1390–1396. 1997.PubMed/NCBI
|
|
35
|
Poon RT, Fan ST, Lo CM, Liu CL, Lam CM,
Yuen WK, Yeung C and Wong J: Improving perioperative outcome
expands the role of hepatectomy in management of benign and
malignant hepatobiliary diseases: Analysis of 1222 consecutive
patients from a prospective database. Ann Surg. 240:698–710.
2004.PubMed/NCBI
|
|
36
|
Zhou Y, Si X, Wu L, Su X, Li B and Zhang
Z: Influence of viral hepatitis status on prognosis in patients
undergoing hepatic resection for hepatocellular carcinoma: A
meta-analysis of observational studies. World J Surg Oncol.
9:1082011. View Article : Google Scholar : PubMed/NCBI
|