Introduction
Invasive Paget's disease of the vulva (IP) is a rare
entity among patients with vulvar cancer, accounting for <1% of
all vulvar malignancies (1).
Radiation therapy and chemotherapy are not considered to be
radical, whereas surgical resection of the tumor with abdominal
lymphadenectomy is highly invasive (2,3). Paget's
disease of the vulva is classified into primary and secondary,
which may be distinguished using immunohistochemistry (3–5). Primary
Paget's disease is subdivided into three categories, namely
intraepithelial Paget's disease (IEP), IP, and Paget's disease as a
manifestation of an underlying adenocarcinoma of a skin appendage
or a vulvar gland (4–6). While IEP is usually treated with
surgery and its prognosis is relatively good, IP is associated with
a poor prognosis (1,3) and a treatment strategy for advanced IP
has not yet been standardized (2,6). Thus,
more effective and less invasive treatments for IP are
required.
We encountered a case of IP with metastases to the
pelvic lymph nodes, which was effectively treated with a
combination of wide local excision, inguinal lymph node resection
and laparoscopic pelvic lymphadenectomy, followed by concurrent
chemoradiotherapy (CCRT).
Case report
A 64-year-old woman visited Kyoto University
Hospital with a rapidly growing mass in the vulva accompanied by
pruritus. The patient had first experienced pruritus in the vulva 7
years prior and visited a local hospital. A topical cream was
prescribed, but the pruritus persisted. Finally, the patient found
a growing mass in the vulva and visited the hospital again. A wide
erythematous rash and a hemorrhagic red mass were observed in the
vulva and the patient was diagnosed with vaginal cancer and was
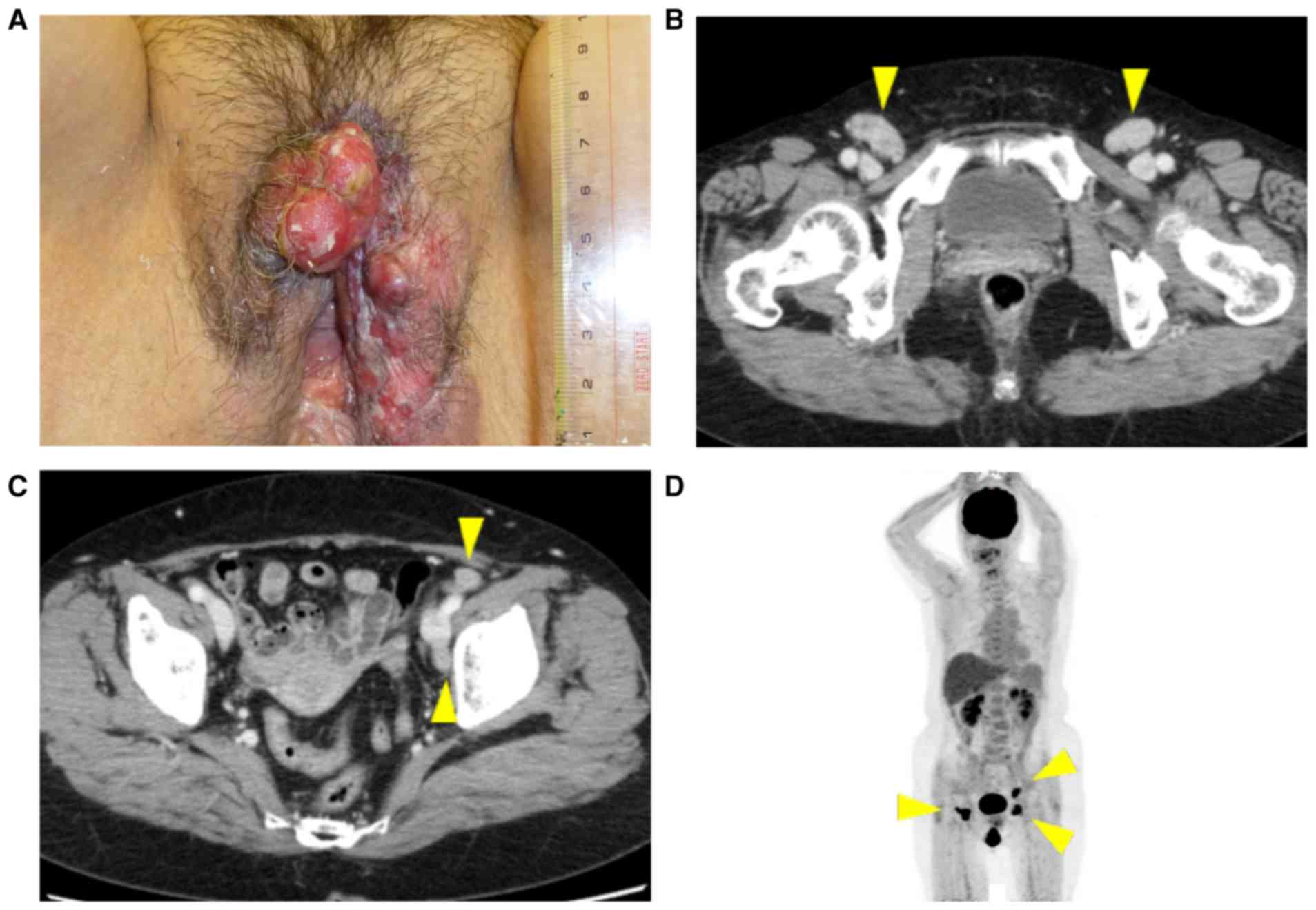
referred to our hospital for further evaluation. At presentation, a
solid mass measuring 4.3 cm was observed in the right vulva, with
bilateral inguinal lymphadenopathy (Fig.
1A). A biopsy of the mass revealed invasive cancer cells. The
results of the immunohistochemical examination revealed that the
tumor cells were positive for cytokeratin (CK)7 and negative for
p63 and CK20. Biopsies from the erythematous rash surrounding the
mass revealed Paget's cells in the epithelium, indicating that the
invasive tumor cells originated from primary vulvar Paget's cells,
and the case was diagnosed as IP. Bilateral superficial inguinal
lymphadenopathy and left obturator and lateral suprainguinal
lymphadenopathy were observed on computed tomography, magnetic
resonance imaging and positron emission tomography examination
(Fig. 1B-D). After mapping biopsy,
local tumor resection, bilateral inguinal lymph node resection and
laparoscopic pelvic lymphadenectomy were performed, followed by
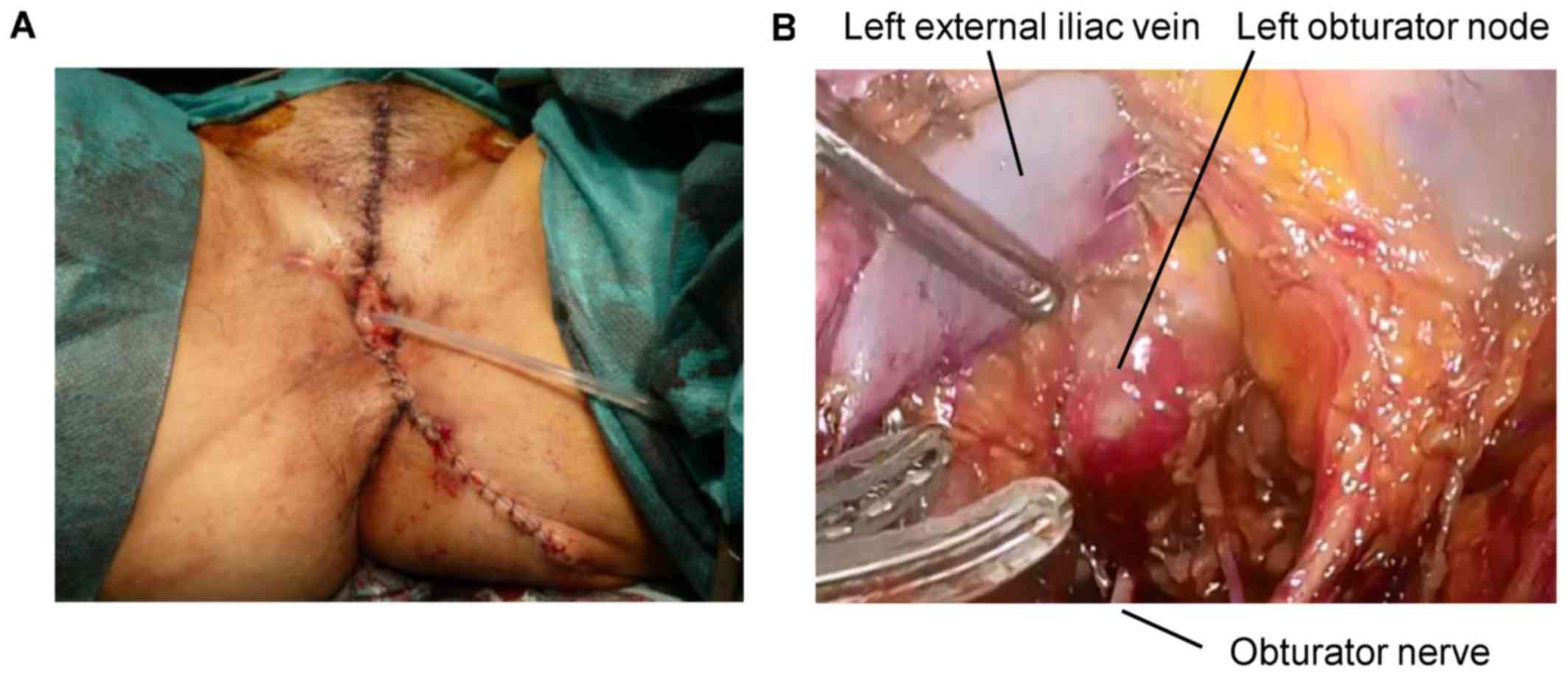
adjuvant CCRT. The vulva was reconstructed using a local fat flap
(Fig. 2A), and laparoscopic pelvic
lymphadenectomy was performed to determine the irradiation field
for CCRT (Fig. 2B). The operative
time was 8 h and 17 min and the total intraoperative blood loss was
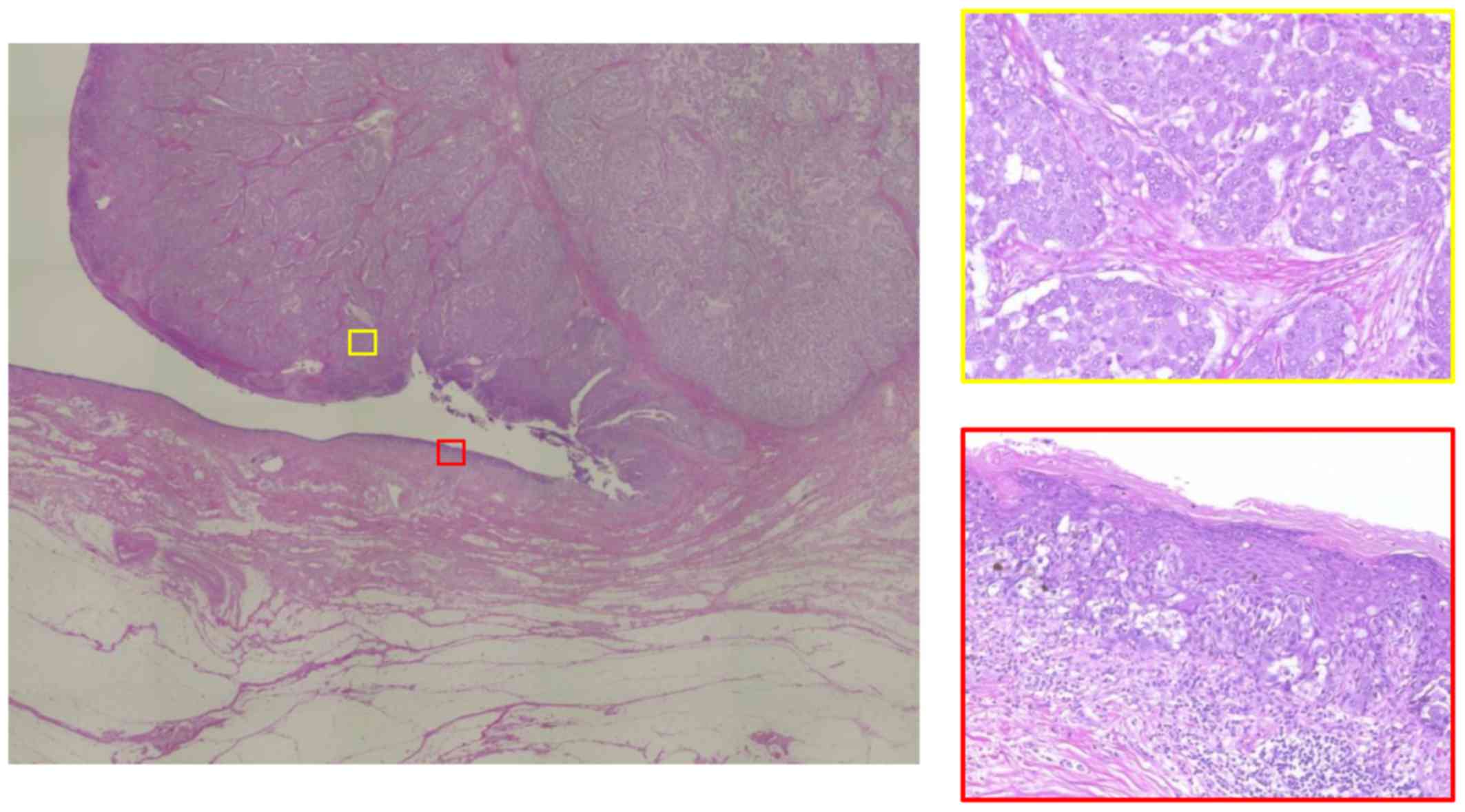
66 g. Postoperative pathological examination revealed invasive
adenocarcinoma arising from non-invasive Paget's disease (Fig. 3). Metastases to the bilateral
superficial inguinal nodes and left obturator and lateral
suprainguinal nodes were identified. CCRT (whole pelvic
irradiation, 50.4 Gy/28 fractions with weekly cisplatin 7 cycles,
40 mg/m2) was completed without notable complications.
The patient experienced an incomplete fracture of the left femoral
head, which was possibly treatment-related, 12 months after the
treatment and was treated conservatively with the administration of
non-steroidal anti-inflammatory drugs and rest. The patient
remained alive without recurrence 15 months after the
treatment.
Discussion
Paget's disease of the vulva is classified into
primary and secondary Paget's disease; the former is of cutaneous
origin, whereas the latter originates from other malignancies, such
as those from the urogenital or gastrointestinal tracts (3–5). Primary
Paget's disease is subdivided into three categories:
Intraepithelial Paget's disease (IEP), IP, and Paget's disease as a
manifestation of an underlying adenocarcinoma of a skin appendage
or vulvar gland (4–6). Immunohistochemistry is useful for the
differential diagnosis of primary and secondary Paget's disease;
Paget's cells of vulvar origin express CK7 and carcinoembryonic
antigen, whereas those secondary to urothelial cancer are positive
for CK20, p63, uroplakin-III and GATA-3, and those secondary to
anorectal adenocarcinoma are positive for CK20, CDX2 and MUC2, but
negative for CK7 (3,7). The tumor cells in the present case were
positive for CK7 and negative for p63 and CK20, suggesting a vulvar
origin.
While IEP is usually treated with surgery and its
prognosis is relatively good, the prognosis of IP is poor (1,3) and
treatment strategies for advanced IP have not yet been standardized
(2,6). IP is usually treated as squamous cell
carcinoma (SCC) of the vulva (3).
Stage IV SCC of the vulva is usually treated with chemotherapy or
CCRT (8–10). When Paget's disease is treated with
radiotherapy, a radiation dose of 40–50 Gy is recommended for IEP
and 55–65 Gy for IP (3,11,12). A
previous case report described the efficacy of CCRT in advanced IP;
good disease control was obtained within the irradiation field,
although the metastatic lesions outside the irradiation field
progressed (2). In the present case,
metastases were limited to inguinal and pelvic lymph nodes, both of
which were within the field of whole pelvic irradiation. Thus, it
was suggested that the disease may be controlled with CCRT.
Historically, radical vulvectomy was previously
performed for vulvar SCC, but this procedure is extremely invasive
and severe complications, such as postoperative wound dehiscence,
infection, lymphedema and psychosexual impairment, are common
(8,13). Moreover, recurrence following radical
vulvectomy is not rare in Paget's disease (6). Wide local resection, which is a less
invasive approach, is currently becoming the standard treatment
modality for early-stage SCC of the vulva and primary IEP (6,14). Our
patient did not experience wound dehiscence or infection following
wide local resection, and underwent adjuvant CCRT immediately after
the surgery. However, it is difficult to obtain clear surgical
margins in Paget's disease, as Paget's cells spread through the
epidermis (15,16). Intraoperative evaluation of the
surgical margins is conducted in some cases, but it is associated
with ~10% false negative outcomes, since Paget's cells are
difficult to evaluate on frozen sections (3,17).
Therefore, in the present case, mapping biopsy was conducted prior
to surgery, as it has been reported to be useful for determining
the surgical margins in extramammary Paget's disease (16).
Although surgery alone does not appear to be
sufficient for the treatment of IP (15), surgery as a staging procedure may be
useful, as accurate staging is key to determining treatment
strategy for IP. It has been reported that over one-third of
patients with Paget's disease with metastases to the lymph nodes
succumb to the disease (1), which
suggests that treating lymph node metastases is crucial.
Laparoscopic pelvic lymphadenectomy is widely performed in
gynecological malignancies, such as cancers of the uterine corpus
and cervix; this procedure is safe and less invasive, with a
shorter hospital stay compared with laparotomy (18). Laparoscopic lymphadenectomy is
conducted to determine the irradiation field in cervical cancer and
in some cases of vulvar SCC (18,19);
hence, it may also be useful for IP with suspected lymph node
metastases. Bilateral inguinal lymphadenectomy was avoided, as
lymphadenectomy combined with radiotherapy may cause severe
lymphedema (14). Instead, resection
of the enlarged lymph nodes was performed, and the patient did not
develop lymphedema after CCRT.
In conclusion, we herein present a case of invasive
Paget's disease treated successfully without severe complications
using a combination of local excision and laparoscopic pelvic
lymphadenectomy as a staging surgery followed by adjuvant CCRT.
Laparoscopic pelvic lymphadenectomy may be useful for determining
the irradiation field for adjuvant CCRT in cases with advanced IP.
However, further studies are required to establish an optimized
treatment strategy for IP.
Acknowledgements
Not applicable.
Funding
No specific grant was received.
Availability of data and materials
Not applicable.
Authors' contributions
YI and KA treated the patient and wrote the paper.
TM, AH, KY, TB and NM treated the patient and edited the
manuscript. SM made the pathological diagnosis and edited the
manuscript. MM approved the final version of the manuscript for
publication. All authors agree with the content of the manuscript
submitted for publication.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of the case details and associated
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CCRT
|
concurrent chemoradiotherapy
|
|
IEP
|
intraepithelial Paget's disease
|
|
IP
|
invasive Paget's disease of the
vulva
|
References
|
1
|
Parker LP, Parker JR, Bodurka-Bevers D,
Deavers M, Bevers MW, Shen-Gunther J and Gershenson DM: Paget's
disease of the vulva: Pathology, pattern of involvement, and
prognosis. Gynecol Oncol. 77:183–189. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yamamoto R, Sakuragi N, Shirato H, Shimizu
M and Fujimoto S: Radiotherapy with concurrent chemotherapy for
vulvar adenocarcinoma associated with extramammary Paget's disease.
Gynecol Oncol. 80:267–271. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
van der Linden M, Meeuwis KA, Bulten J,
Bosse T, van Poelgeest MI and de Hullu JA: Paget disease of the
vulva. Crit Rev Oncol Hematol. 101:60–74. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wilkinson EJ and Brown HM: Vulvar Paget
disease of urothelial origin: A report of three cases and a
proposed classification of vulvar Paget disease. Hum Pathol.
33:549–554. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kurman RJ, Ellenson LH and Ronnett BM:
Blaustein's Pathology of the Female Genital Tract. 6th.
Springer+Business Media; New York: pp. 81–86. 2011
|
|
6
|
Delport ES: Extramammary Paget's disease
of the vulva: An annotated review of the current literature.
Australas J Dermatol. 54:9–21. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kurman RJ, Carcangiu ML, Herrington CS and
Young RH: World Health Organization Classification of Tumours. Int
Agency Res Cancer; Lyon Cedex 08: pp. 236–237. 2014
|
|
8
|
Deppe G, Mert I and Winer IS: Management
of squamous cell vulvar cancer: A review. J Obstet Gynaecol Res.
40:1217–1225. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mak RH, Halasz LM, Tanaka CK, Ancukiewicz
M, Schultz DJ, Russell AH and Viswanathan AN: Outcomes after
radiation therapy with concurrent weekly platinum-based
chemotherapy or every-3-4-week 5-fluorouracil-containing regimens
for squamous cell carcinoma of the vulva. Gynecol Oncol.
120:101–107. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moore DH, Ali S, Koh WJ, Michael H, Barnes
MN, McCourt CK, Homesley HD and Walker JL: A phase II trial of
radiation therapy and weekly cisplatin chemotherapy for the
treatment of locally-advanced squamous cell carcinoma of the vulva:
A gynecologic oncology group study. Gynecol Oncol. 124:529–533.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Besa P, Rich TA, Delclos L, Edwards CL,
Ota DM and Wharton JT: Extramammary Paget's disease of the perineal
skin: Role of radiotherapy. Int J Radiat Oncol Biol Phys. 24:73–78.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hata M, Omura M, Koike I, Wada H, Miyagi
E, Tayama Y, Odagiri K, Minagawa Y, Ogino I and Inoue T: Role of
radiotherapy as curative treatment of extramammary Paget's disease.
Int J Radiat Oncol Biol Phys. 80:47–54. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
De Hullu JA, Hollema H, Lolkema S, Boezen
M, Boonstra H, Burger MP, Aalders JG, Mourits MJ and Van Der Zee
AG: Vulvar carcinoma. The price of less radical surgery. Cancer.
95:2331–2338. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hacker NF, Eifel PJ and van der Velden J:
Cancer of the vulva. Int J Gynecol Obstet. 119 Suppl 2:S90–S96.
2012. View Article : Google Scholar
|
|
15
|
Kodama S, Kaneko T, Saito M, Yoshiya N,
Honma S and Tanaka K: A clinicopathologic study of 30 patients with
Paget's disease of the vulva. Gynecol Oncol. 56:63–70. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kato T, Fujimoto N, Fujii N and Tanaka T:
Mapping biopsy with punch biopsies to determine surgical margin in
extramammary Paget's disease. J Dermatol. 40:968–972. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhu Y, Ye DW, Chen ZW, Zhang SL and Qin
XJ: Frozen section-guided wide local excision in the treatment of
penoscrotal extramammary Paget's disease. BJU Int. 100:1282–1287.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Walker JL, Piedmonte MR, Spirtos NM,
Eisenkop SM, Schlaerth JB, Mannel RS, Spiegel G, Barakat R, Pearl
ML and Sharma SK: Laparoscopy compared with laparotomy for
comprehensive surgical staging of uterine cancer: Gynecologic
Oncology Group Study LAP2. J Clin Oncol. 27:5331–5336. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Klemm P, Marnitz S, Köhler C, Braig U and
Schneider A: Clinical implication of laparoscopic pelvic
lymphadenectomy in patients with vulvar cancer and positive groin
nodes. Gynecol Oncol. 99:101–105. 2005. View Article : Google Scholar : PubMed/NCBI
|