Introduction
Colorectal cancer (CRC) is a frequent cause of
cancer-related mortality (1) and is
estimated to be the second leading cause of cancer-related death
for both males and females (2).
Lately, the incidence rate of CRC has been increasing in developing
countries as well (3,4). Although cancer stage is the major
prognostic factor for CRC, the actual risks of recurrence are
variable in individuals, even if they are at the same stage.
Reportedly, there is a subset of patients with stage II colon
cancer who have a high likelihood of recurrence and have attained a
clinically significant benefit from chemotherapy (5). However, few studies have examined to
define the subset of patients with stage II colon cancer who are at
high risk of recurrence. While the American Society of Clinical
Oncology guidelines do not recommend routine adjuvant chemotherapy
for stage II patients (6), the
European Society of Medical Oncology (ESMO) guidelines recommended
that adjuvant chemotherapy be used for selected patients with stage
II CRC. Hence, the necessity of adjuvant treatment at stage II is
controversial.
Various studies have reported that factors such as
T4 disease, poorly differentiated histology, tumor perforation,
vascular invasion, lymphatic invasion, neuroinvasion, perineural
invasion, bowel obstruction, surgical margin positivity, and
inadequate lymph node sampling are related with poor prognosis in
stage II CRC (3,5).
According to data from the Surveillance,
Epidemiology, and End Results (SEER) program in the United States,
some reports have suggested that the prognosis of stage IIB (T4,
N0) patients is worse than that of stage IIIA (T1-2, N1) patients
(7). In recent years, these
predictive factors for high-risk colon cancer have been
retrospectively evaluated, and it is challenging to determine the
benefits after curative resection and predict the prognosis in
patients with stage II CRC (8,9).
In this study, we report a prediction model that can
predict recurrence of stage II colon cancer in patients after
curative resection. Furthermore, it provides a prediction
probability for individual outcomes that will benefit patients in
selecting adjuvant treatment after curative resection.
Patients and methods
Patients and dataset
In this study, 436 patients at Osaka International
Cancer Institute and Yao Municipal Hospital were identified as
having a diagnosis of stage II colorectal cancer from July 2004 to
September 2012. All patients were histologically diagnosed with
colorectal cancer and underwent curative surgical resection. A
total of 84 patients with tumors located in the upper and lower
rectum and/or who underwent adjuvant chemotherapy and neoadjuvant
chemotherapy were excluded, and the remaining 352 patients were
included. This study was approved by the Institutional Review
Boards of our institutes. Patient records were anonymized before
the analysis.
These 352 patients were included in the learning
set, and the Cox proportional hazards regression model was used to
develop the prediction model for the 5-year disease-free survival
(DFS). An independent group of 213 patients who underwent curative
resection for stage II colon cancer at Osaka University Hospital
from January 2001 to December 2012 was used to validate the
prediction model.
Clinicopathological evaluation and
follow-up
Data on the age, sex, body mass index (BMI),
preoperative serum level of the tumor marker carcinoembryonic
antigen (CEA), pre-perforation, pre-obstruction, post-anastomotic
leakage, surgery, dissection for lymph node, number of lymph nodes
sampled, colorectal tumor location, and pathological findings
(e.g., histology, histological grade, tumor invasion, lymph node
sampling, lymphatic invasion, and venous invasion) were retrieved
from patients' medical records for evaluation. Preoperative
determination of the extent of tumor spread was performed using
X-ray, CT, MRI, and/or positron emission tomography. Preoperative
obstruction was defined as intestinal stenosis diagnosed by
endoscopy and the starvation was necessary for over a week until
colorectomy. Intraoperative findings contributed to the
determination of metastatic tumor involvement. Surgical specimens
were fixed in formalin, processed through a graded ethanol series,
and embedded in paraffin. The sections were stained with
hematoxylin and eosin and Elastica van Gieson stain, and the
histological grade, degree of lymphatic invasion, and degree of
venous invasion were examined. The clinicopathological factors were
assessed according to the TNM classification of the UICC (10). After surgery, all patients underwent
follow-up blood examinations to evaluate the serum levels of the
tumor markers CEA and carbohydrate antigen 19-9, and further
imaging with abdominal ultrasonography, CT, chest X-ray, and/or
positron emission tomography every 3–6 months and colonoscopy every
year following the Japanese guidelines (11).
Statistical analysis
Univariate analysis was performed using a
proportional hazards model for DFS after primary curative resection
to identify the independent factors. The two-sided P<0.05 were
considered statistically significant. A classification and
regression tree (CART) was structured as a prediction model for DFS
by variables, with the limit to enter a variable in the analysis
set at P<0.05. The Kaplan-Meier survival curves were plotted and
compared with the generalized log-rank test. All statistical
analyses were performed using the JMP 13.0 statistical software
program (SAS Institute, Cary, NC, USA). The CART was structured
using R 3. 1. 3 (CRAN; R Foundation for Statistical Computing,
Vienna, Austria).
Results
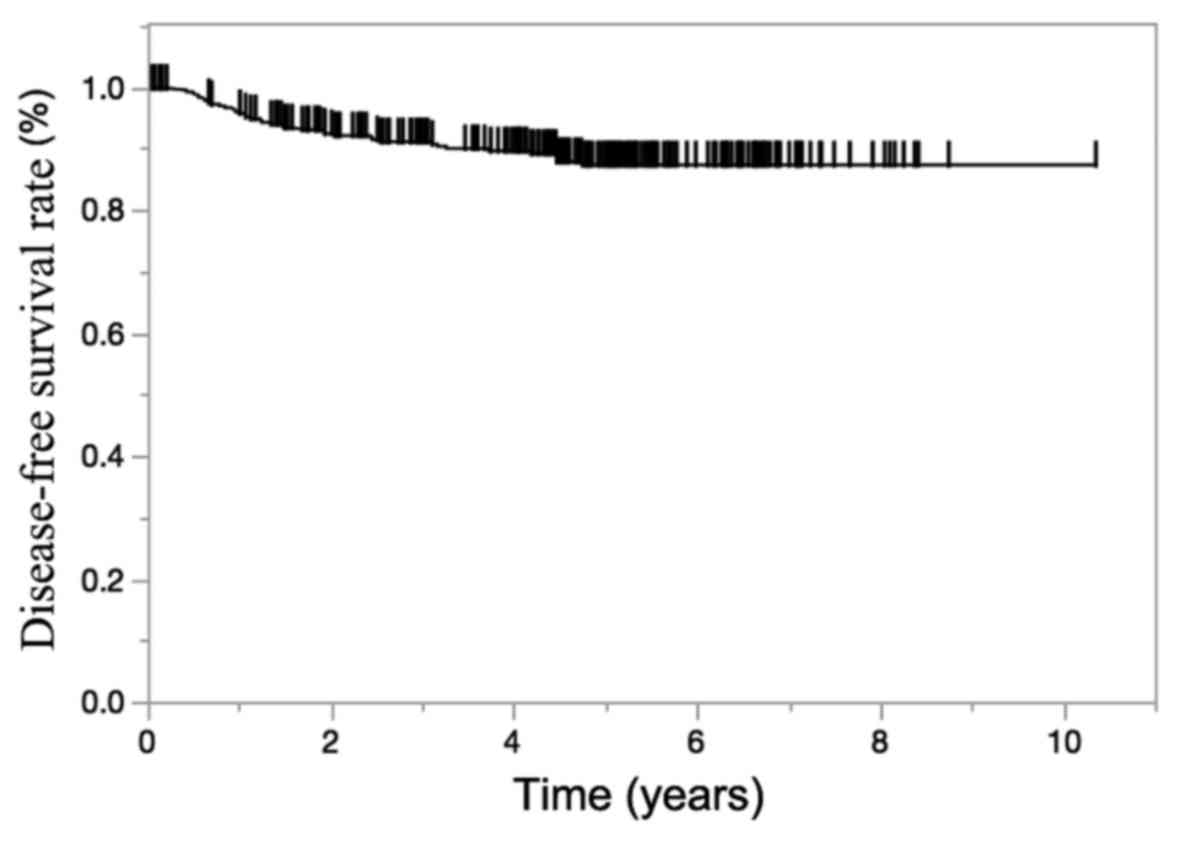
The characteristics of all 352 patients in the
learning set are listed in Table I.
All patients' ages ranged from 34 to 96 years, and 196 patients
(55.7%) were male. The median follow-up time was 4.67 years, and
the 5-year DFS rate was 89.2% (Fig.
1). After curative surgical resection, 314 patients (89.2%) had
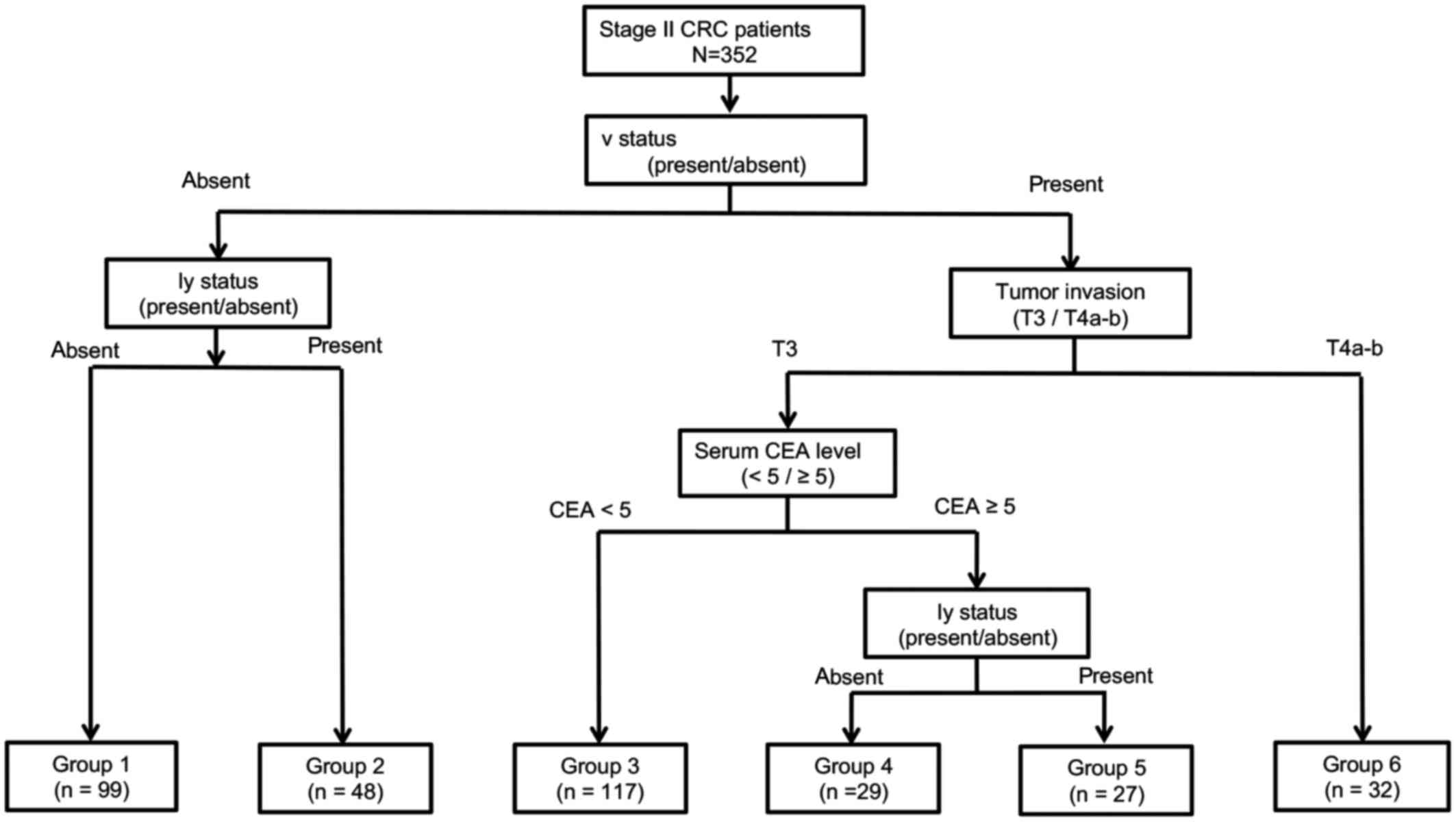
no recurrence. The univariate analysis of the clinicopathological
factors for recurrence (Table II)
revealed that high preoperative serum CEA level (P=0.038),
pre-obstruction (P=0.005), tumor invasion (P=0.034), lymphatic
invasion (P=0.029), and venous invasion (P=0.011) were significant
factors for recurrence. These factors were introduced to create the
prediction model as the CART. Finally, patients were segregated
into six groups based on the following four factors: CEA level,
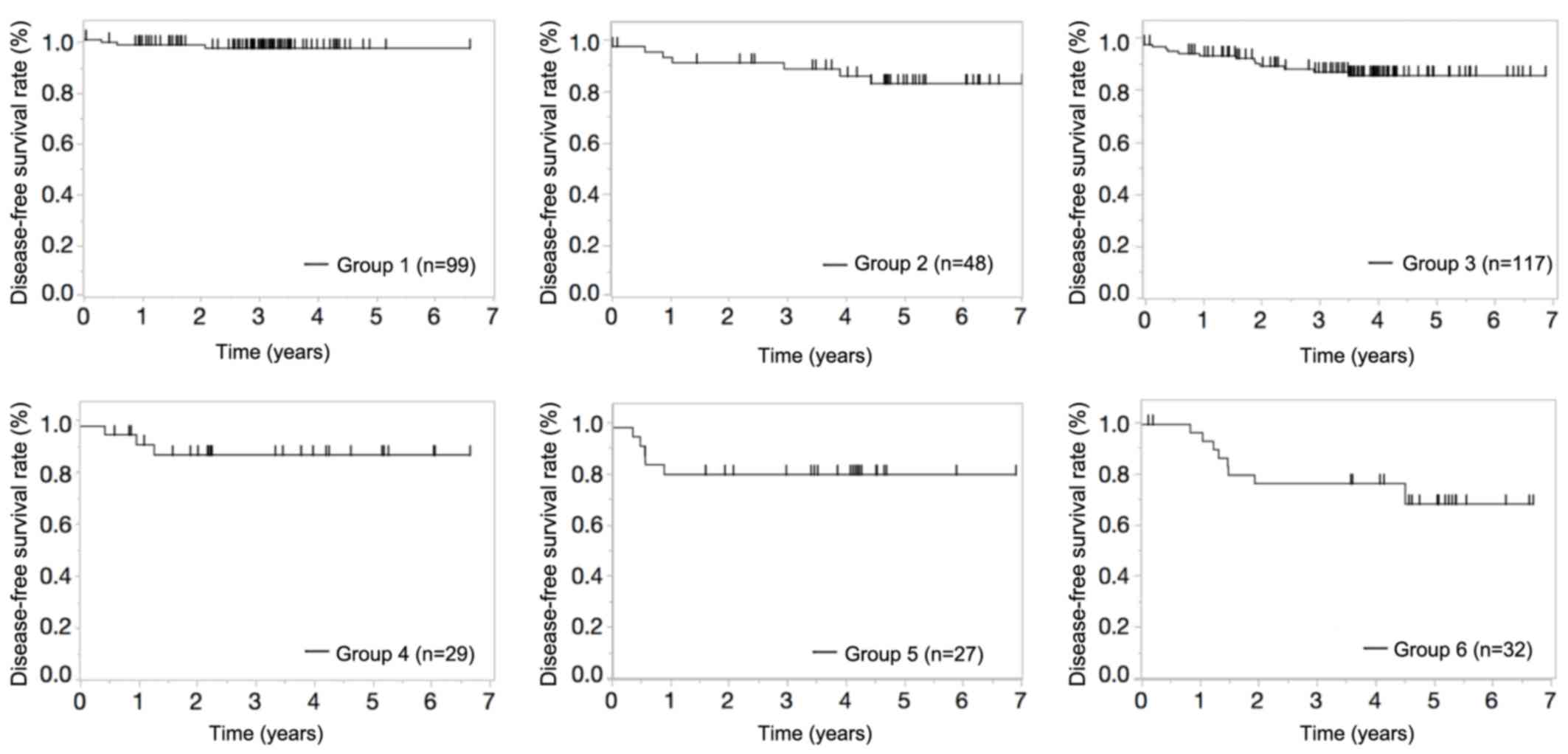
tumor invasion, lymphatic invasion, and venous invasion. The DFS
rates for each subgroup are shown in Figs. 2 and 3. The concordance indices for DFS after
current surgical resection were 0.675 in the learning set and 0.552
in the validation set.
 | Table I.Clinicopathological factors in 352
patients with stage II colorectal cancer. |
Table I.
Clinicopathological factors in 352
patients with stage II colorectal cancer.
| Clinicopathological
factors | N=352 |
|---|
| Age (years) | 69
(34–96)a |
| Sex
(male/female) | 196/156 |
| BMI | 22.7
(12.1–49.9)a |
| CEA (ng/ml) | 2.5
(0.1–296.1)a |
| Pre-obstruction
(present/absent) | 12/340 |
| Pre-perforation
(present/absent) | 4/348 |
| Post-anastomosis
leakage (present/absent) | 8/344 |
| Surgery
(open/laparoscopy) | 290/62 |
| Lymph node
dissectionb
(D1,2/D3) | 63/289 |
| Number of lymph nodes
sampling (<12/≥12) | 80/272 |
| Tumor location
(Caecum/ascending/transverse/descending/sigmoid/rectosigmoid) |
32/77/45/30/120/48 |
| Tumor
invasionc
(T3/T4b/T4d) | 295/44/13 |
| Histological grade
(Well-modd/otherse) | 332/20 |
| Lymphatic invasion
(present/absent) | 132/220 |
| Venous invasion
(present/absent) | 205/147 |
| Recurrence
(present/absent) | 38/314 |
| Table II.Univariate analysis for disease-free
survival. |
Table II.
Univariate analysis for disease-free
survival.
| Factors | HR | 95% CI | P-value |
|---|
| Age, years
(<69/≥69) | 1.472 | 0.775–2.882 | 0.239 |
| Sex
(male/female) | 1.381 | 0.724–2.738 | 0.331 |
| BMI
(≥22.7/<22.7) | 1.374 | 0.725–2.660 | 0.331 |
| CEA
(≥5.0/<5.0) | 2.014 | 1.040–3.816 | 0.038a |
| Pre-obstruction
(present/absent) | 5.211 | 1.782–12.220 | 0.005a |
| Surgery
(open/laparoscopy) | 1.031 | 0.463–2.742 | 0.945 |
| Lymph nodes
dissectionb
(D3/D1-2) | 1.142 | 0.463–2.742 | 1.142 |
| Number of lymph node
sampling (<12/≥12) | 1.286 | 0.600–3.179 | 0.538 |
| Histological grade
(well-modc/othersd) | 2.415 | 0.524–42.861 | 0.314 |
| Tumor
invasione
(T4a-b/T3) | 2.485 | 1.076–5.305 | 0.034a |
| Lymphatic invasion
(present/absent) | 2.036 | 1.076–3.910 | 0.029a |
| Venous invasion
(present/absent) | 2.483 | 1.223–5.567 | 0.011a |
| Tumor location
(left/right) | 1.123 | 0.889–3.540 | 0.109 |
The CART divided the six groups based on the
following four factors. Group 6 was the group with the highest risk
of recurrence, and 5-year DFS was low at 68.6%. Patients in group 6
gains more benefit from adjuvant chemotherapy than other
groups.
Discussion
Although curative surgical resection is an effective
treatment for CRC, some patients experience recurrence, which
results in poor prognosis. In stage III, about 30% of patients
experienced recurrence after curative resection (8,9). The
current guidelines recommend adjuvant chemotherapy for stage III
CRC. Although recent chemotherapeutic development has improved the
overall outcomes of advanced metastatic CRC, metastasis influences
the prognosis. In stage II, about 13% of patients experience
recurrence after curative resection, and the administration of
adjuvant chemotherapy for patients with stage II CRC is
controversial (12). The explorative
CART analysis was used to define the relevant prognostic groups
concerning survival probability. CARTs are machine-learning methods
for constructing prediction models. Models are obtained by a
recursive partitioning method using data, fitting a simple
prediction model for each partition. Regression trees are for
dependent variables taking continuous or discrete values, with
prediction error measured by the squared difference between the
observed and predicted values. During the CART analysis, first, the
entire sample, and, after that, all newly defined subgroups were
investigated at every stage of the analysis to determine which
variable yielded the most significant division into the prognostic
groups regarding the estimates of DFS probabilities according to
Kaplan-Meier analysis and compared with log-rank test statistics
(13).
Because clinical trials have not demonstrated a
significant improvement in DFS, inclusion of a surgery-alone
control arm in randomized trials for average-risk stage II patients
remains justifiable. Meanwhile, the oncology research community has
recently emphasized conducting trials to establish the role of
molecular prognostic and predictive factors better. The motivation
behind these trials is the identification of those patients who are
most likely to benefit from treatment by their high risk of
recurrence and/or high probability of response to treatment. As
such, models to predict the prognosis after curative surgical
resection would be useful in determining the necessity of an
intensive follow-up to select adjuvant therapy. In our study, the
clinicopathological analysis revealed that high preoperative serum
CEA level, pre-obstruction, pathologically defined tumor invasion,
lymphatic invasion, and venous invasion were associated with a poor
prognosis for DFS.
Patients were divided into six groups by the CART
based on the following four factors. Group 6 had the highest risk
group of recurrence, with a 5-year DFS of 68.6%. This recurrence
rate is roughly the same as that in stage III patients after
curative resection. We also analyzed patients who underwent
adjuvant chemotherapy and were excluded from this study because
there are influence of chemotherapy in DFS. As there was also
concern that high risk groups of recurrence were excluded, we
examined about the patients who underwent adjuvant chemotherapy in
the DFS. The patients who underwent adjuvant chemotherapy
classified in group 6 had no recurrence. This indicates that there
are some patients who can benefit from adjuvant chemotherapy in
stage II, and adjuvant chemotherapy might improve postoperative
prognosis in the highest risk group.
We developed a prediction model for recurrence in
patients with stage II colon cancer. High preoperative serum CEA
level, pre-obstruction, tumor invasion, lymphatic invasion, and
venous invasion were significant factors of recurrence in the
univariate analysis for DFS and they constructed the branches of
the CART. However, there are some limitations. Although
preoperative obstruction was a significant factor in the univariate
analysis, it was not included in the CART. We found there was a
positive correlation between venous invasion and preoperative
obstruction. Venous invasion appeared as the first branch of CART,
and it might be a confounding factor for preoperative obstruction
in our present retrospective analysis. We created the prediction
model as a CART using five factors that were introduced by
univariate analysis. We also performed the multivariate analysis to
examine the predictive factors. There were only two significant
factors, venous invasion (P=0.038) and pre-obstruction (P=0.029),
in the multivariate analysis. Other factors that high preoperative
serum CEA level (P=0.135), tumor invasion (P=0.172), and lymphatic
invasion (P=0.097) were not significant for recurrence in the
multivariate analysis. Two factors are too few to create the
prediction model. Therefore, more patients and multi-institutional
studies are necessary to create a universal CART from the results
of multivariate analysis. Finally, some reported risk factors, such
as poorly differentiated histology and bowel obstruction, were not
significant, and tumor perforation, neuroinvasion, and perineural
invasion were not examined in this study. Hence, a
multiple-institutional study that enrolls many patients should be
conducted.
However, the prediction model we have generated will
help in selecting high-risk patients with stage II colon cancer who
have significantly benefited from adjuvant chemotherapy. In
addition, it will enable the selection of appropriate treatment for
patients, resulting in effective outcomes.
In conclusion, a new prediction model was developed
that indicates the risk of recurrence and prognosis in patients
with stage II colon cancer, which will facilitate the appropriate
introduction of adjuvant chemotherapy in high-risk stage II
patients.
Acknowledgements
The authors would like to thank Ms. Aya Ito for
special technical assistance regarding sample preparation
(Department of surgery, Osaka International Cancer Institute,
Osaka, Japan) for special technical assistance regarding sample
preparation.
Funding
The present work was supported by a grant-in-aid for
scientific research (grant no. 17K10572).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
KS and NM conceptualized the project, designed and
performed the experiments and interpreted the results. KS also
wrote the manuscript. NM, YT, YT, JN, MY, MO, MT, YI, HT, NH, TH,
TH and CM performed the surgery and analyzed the clinical data. SF,
NM, TM, YD and MM analyzed the data or participated in the
discussions of the results.
Ethics approval and consent to
participate
This study was approved by the Institutional Review
Boards of our institutes. Patient records were anonymized before
the analysis.
Patient consent for publication
Patients provided written, informed consent.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel R, Desantis C and Jemal A:
Colorectal cancer statistics, 2014. CA Cancer J Clin. 64:104–117.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
National Comprehensive Cancer Network:
NCCN Clinical Practice Guidelines in Oncology. Colon Cancer.
Version 2. 2017.
|
|
4
|
Colvin H, Mizushima T, Eguchi H, Takiguchi
S, Doki Y and Mori M: Gastroenterological surgery in Japan: The
past, the present and the future. Ann Gastroenterol Surg. 1:5–10.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Labianca R, Nordlinger B, Beretta GD,
Mosconi S, Mandala M, Cervantes A and Arnold D; ESMO Guidelines
Working Group, . Early colon cancer: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol. 24
Suppl 6:vi64–vi72. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Benson AB III, Schrag D, Somerfield MR,
Cohen AM, Figueredo AT, Flynn PJ, Krzyzanowska MK, Maroun J,
McAllister P, Van Cutsem E, et al: American Society of Clinical
Oncology recommendations on adjuvant chemotherapy for stage II
colon cancer. J Clin Oncol. 22:3408–3419. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
O'Connell JB, Maggard MA and Ko CY: Colon
cancer survival rates with the new American Joint Committee on
Cancer sixth edition staging. J Natl Cancer Inst. 96:1420–1425.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Benson AB III, Venook AP, Cederquist L,
Chan E, Chen YJ, Cooper HS, Deming D, Engstrom PF, Enzinger PC,
Fichera A, et al: Colon Cancer, Version 1.2017, NCCN Clinical
Practice Guidelines in Oncology. J Natl Compr Canc Netw.
15:370–398. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kucukzeybek Y, Dirican A, Demir L,
Yildirim S, Akyol M, Yildiz Y, Bayoglu IV, Alacacioglu A, Varol U,
Salman T, et al: Adjuvant chemotherapy and prognostic factors in
stage II colon cancer-Izmir Oncology Group Study. Asian Pac J
Cancer Prev. 16:2413–2418. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Patriarca S, Ferretti S and Zanetti R: TNM
Classification of malignant tumours-Eighth edition: Which news?
Epidemiol Prev. 41:140–143. 2017.(In Italian). PubMed/NCBI
|
|
11
|
Watanabe T, Muro K, Ajioka Y, Hashiguchi
Y, Ito Y, Saito Y, Hamaguchi T, Ishida H, Ishiguro M, Ishihara S,
et al: Japanese Society for Cancer of the Colon and Rectum (JSCCR)
guidelines 2016 for the treatment of colorectal cancer. Int J Clin
Oncol. 23:1–34. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wong AC, Stock S, Schrag D, Kahn KL, Salz
T, Charlton ME, Rogers SO Jr, Goodman KA and Keating NL:
Physicians' beliefs about the benefits and risks of adjuvant
therapies for stage II and stage III colorectal cancer. J Oncol
Pract. 10:e360–e367. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Leiter U, Buettner PG, Eigentler TK and
Garbe C: Prognostic factors of thin cutaneous melanoma: An analysis
of the central malignant melanoma registry of the german
dermatological society. J Clin Oncol. 22:3660–3667. 2004.
View Article : Google Scholar : PubMed/NCBI
|