Introduction
‘Juvenile’ nasopharyngeal angiofibroma (NA) occurs
almost exclusively in males, but has also been documented in
females, albeit infrequently (1–5). When a
diagnosis of NA is made in a female patient, caution is necessary
to exclude the possibility of a conventional nasal or antrochoanal
polyp with fibrosis. The presentation age ranges from 10 to 25
years (2), whereas a few cases of NA
patients aged >30 years have been reported in the literature
(6).
NA is a vascular tumor that accounts for <1% of
all head and neck neoplasms, with a higher reported incidence in
India (2,7); it originates from the sphenopalatine
foramen and involves both the pterygopalatine fossa and the
posterior nasal cavity (8,9). Despite being histologically benign, NA
is locally invasive and is associated with a high rate of
persistence and recurrence mainly due to incomplete resection
during surgery (10).
The aim of the present study was to report a
particularly rare case of a 68-year-old female patient who was
diagnosed with NA and describe the diagnostic and therapeutic
workup.
Case report
A 68-year-old woman was admitted to the ENT Clinic
of Sapienza University Hospital (Rome, Italy) in May 2015 with an
18-month history of nasal obstruction, episodes of left-sided
hearing loss, discharge of mucus in the nasopharynx, occasional
headaches and snoring. The patient was otherwise healthy, with no
reported comorbidities. She had gone into menopause 11 years
earlier and, up to that point, she had had regular menstrual cycles
and two pregnancies.
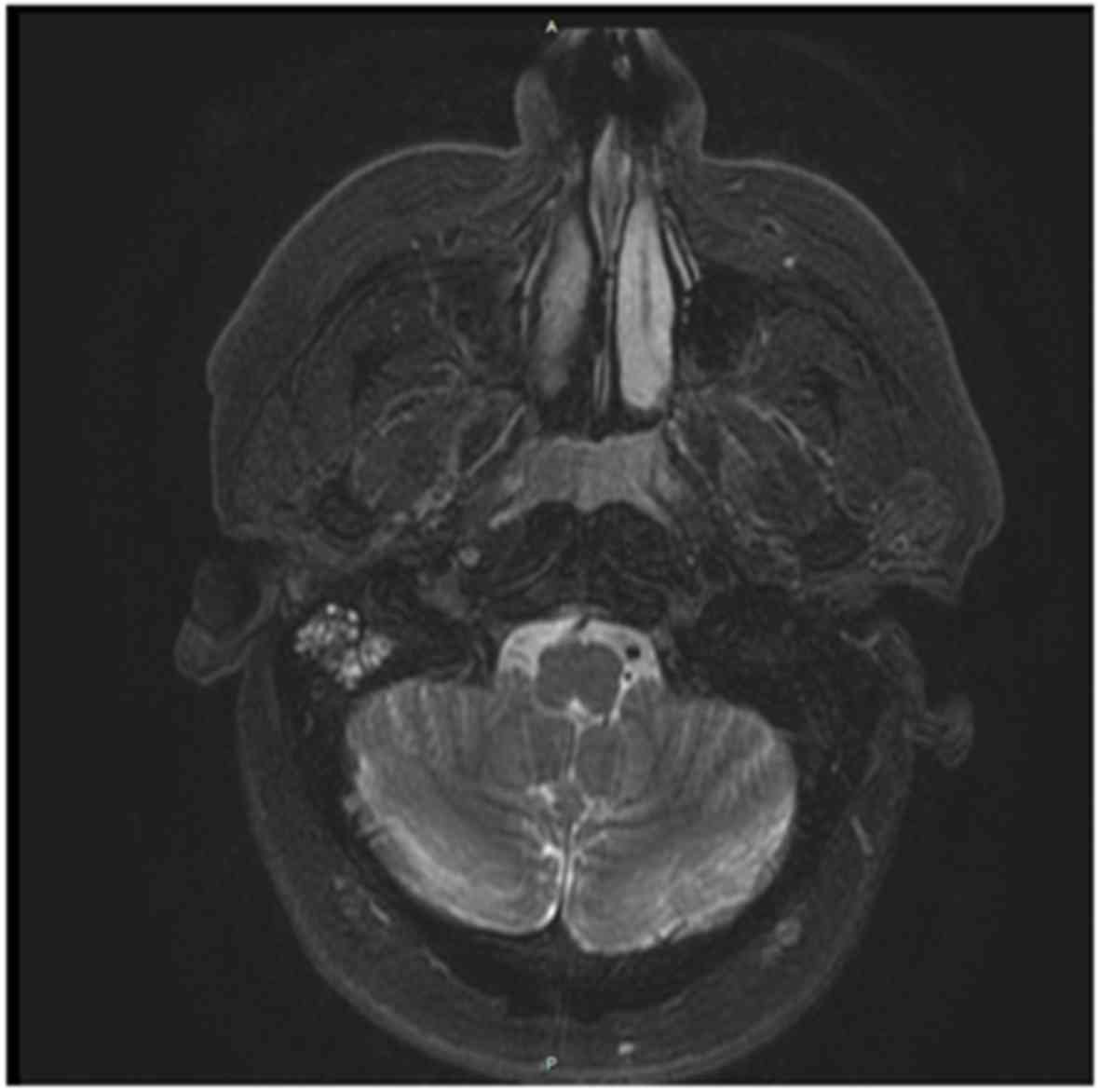
The patient underwent endoscopic examination of the
upper airways that revealed a whitish, non-ulcerated, non-bleeding
large mass in the posterior nasal cavity extending to the
nasopharynx. Endoscopy was followed by magnetic resonance imaging
(MRI) examination of the head and neck with gadolinium contrast,
which confirmed the presence of a polypoid lesion sized 3.2×2.6 cm
in the posterior nasal cavity, without invasion of the roof or
posterior wall of the nasopharynx. There were no enlarged lymph
nodes in the upper part of the neck (Fig. 1).
The patient underwent functional transnasal
endoscopic removal of the mass under general anesthesia; consistent
bleeding occurred during surgery. The mass was entirely removed and
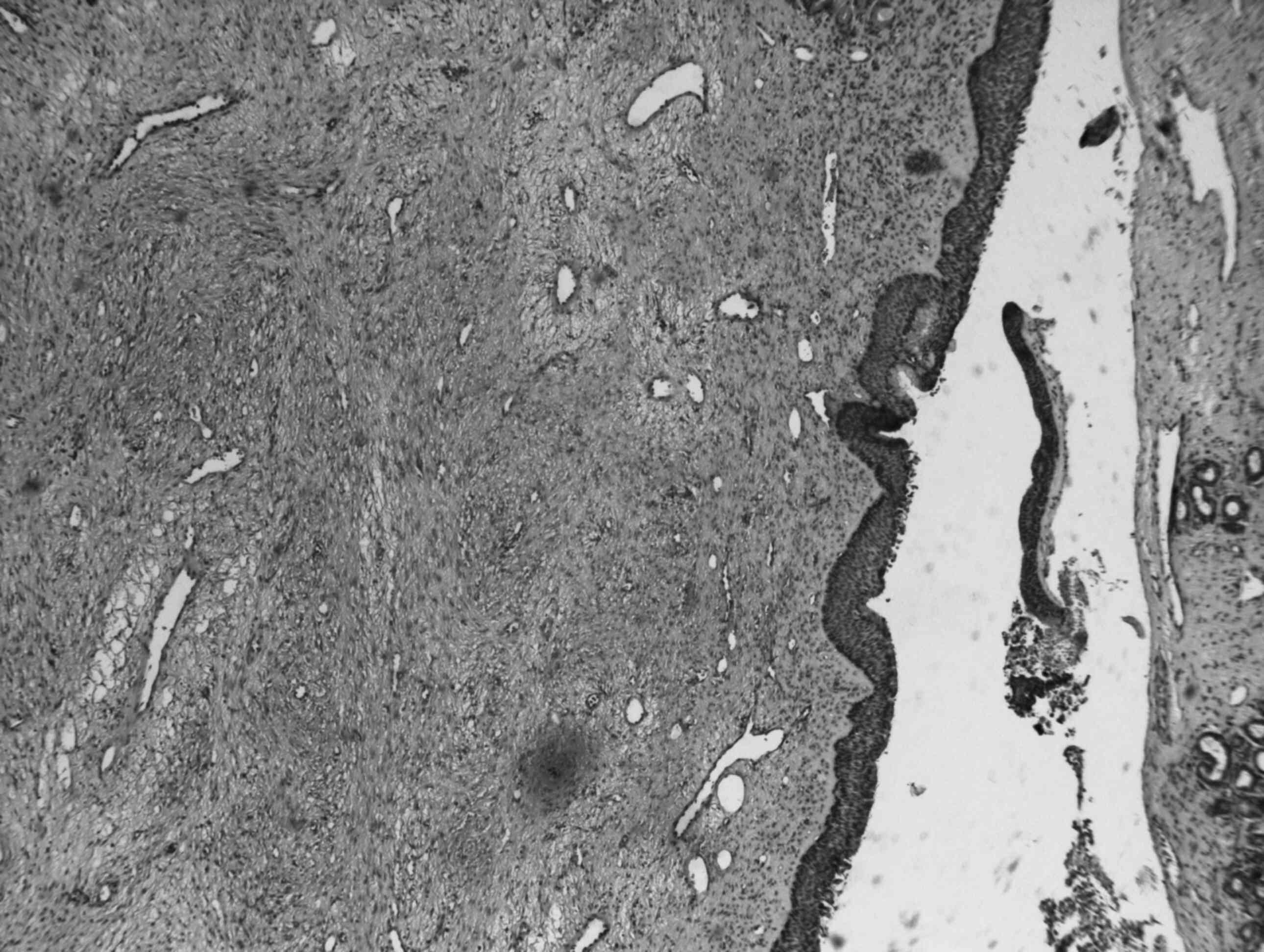
was found to be of firm, elastic consistency. The specimen was sent
for histological examination; hematoxylin and eosin staining
demonstrated that the mass was composed of proliferating blood
vessels of variable shape and size, intermixed with a connective
tissue stroma. The wall of the vessels was formed only by
endothelial cells (CD34+). The connective tissue was
fibrocellular, with an irregular pattern and plump fibroblasts
(Fig. 2). Immunohistochemical
analysis was performed with actin staining for smooth muscle; the
perimeter of the mass appeared as a thin rim of smooth muscle cells
topped by endothelium (vimentin+ and CD68+).
Ki-67 immunostaining demonstrated only a few positive cells,
confirming low cell proliferation rate and excluding the
possibility of a conventional nasal or antrochoanal polyp with
fibrosis (11).
The postoperative course was uneventful, and no
disease recurrence was observed during the last follow-up visit in
March 2018, nearly 3 years after surgery.
Discussion
NA is a rare benign tumor affecting almost
exclusively adolescents and young adults who have been symptomatic
for 15 to 24 months prior to seeking medical treatment (2,11–13).
Only a few studies have reported NA in women (3–5). Neel
et al (10) and Conley et
al (14) in two case series
including 150 and 38 cases, respectively, reported no female
patients. In a systematic review of the literature, Gruber et
al (15) found only 28 female
cases.
NAs are mainly diagnosed in patients aged between 14
and 25 years, with a mean age of 15 years (2,16,17). The
small number of patients aged >30 years confirms that a
presentation after this age is quite rare (6,18,19).
Isolated cases of angiofibroma arising outside the nasopharynx have
been reported, most commonly in the maxillary (32%) and ethmoid
(10%) sinuses (20). These tumors
are clinically distinct from NA, they develop at a slightly older
age and occur more commonly in women. Based on these facts, the
case of a 68-year-old woman with NA is considered as particularly
rare due to both the sex and the age of patient; to the authors'
best knowledge, this is the oldest patient with NA reported in the
literature.
The etiology of NA is debated; it has been
hypothesized that NA i) arises from the periosteum (21), ii) is a distinct type of hemangioma
(22), iii) is a connective tissue
response of the nasopharyngeal periosteum to an ectopic nidus of
vascular tissue, possibly of the inferior turbinate type (23), and iv) is a specific type of
fibromatosis (24).
The occurrence of NA in women has been seldom
reported; to explain the male predominance in NA it has been
hypothesized that NA may be a testosterone-dependent tumor that
arises from a fibrovascular nidus in the nasopharynx that lies
dormant until the onset of puberty (25). At this time, coincident with the
increase in testosterone levels, the tumor grows and becomes
symptomatic. Estrogens, acting in an antagonistic manner, inhibit
the release of trophic hormones from the pituitary gland, causing a
decline in testosterone production and, therefore, a decrease in
the size of the tumor (26). The
hormonal theory suggests that high estrogen levels act protectively
in women; Johns et al observed a reduction of the mass with
estrogenic therapy in 6 patients (27), while Johnsen et al reported
that testosterone therapy was associated with tumor enlargement
(28).
In the present case, the occurrence of NA after
menopause may also support the idea of this hormonal impact. It may
be hypothesized that the patient's NA had undergone natural
regression during the years of increased estrogen production and
then started proliferating after menopause due to the decreased
hormonal levels. The fact that the patient had regular menstrual
cycles suggests the absence of abnormal variations in her hormonal
levels throughout her fertile life. The high levels of estrogen and
progesterone during her two pregnancies may have also delayed the
appearance of the tumor. However, the case of NA in a pregnant
woman reported by Péloquin et al in 1997 favors the
likelihood of other congenital or inflammatory factors contributing
to the pathogenesis of NA (29).
The preoperative diagnosis of NA is mainly based on
a careful history and nasal endoscopic examination and is
supplemented by imaging using computed tomography or MRI scans;
however, final diagnosis must be based on histological and
immunohistochemical examination. Biopsies to establish histological
diagnosis are contraindicated due to the risk of substantial
bleeding; however, with the advancements in angiography, diagnosis
and embolization of the tumor-feeding vessels may be performed at
the same time. In older patients, the tumor becomes fibrotic and
bleeding is usually not a major concern although consistent
bleeding may occur during surgery, as in the present case.
The surgical approach to NA resection depends on the
stage of the tumor based on the Fisch classification (30).
In conclusion, NA is a rare, vascular, benign tumor
that typically affects adolescent boys. The etiopathogenesis
remains unknown; the most important theories are genetic and
hormonal, although the latter may not apply to all cases, since NA
has been reported in a pregnant woman. In the present case, the sex
and age of the patient are particularly rare for this condition and
warrant suspicion of NA in any patient presenting with a
nasopharyngeal mass and recommendation of an angiographic
examination to prevent dangerous intra- and postoperative
bleeding.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of any associated data and accompanying images.
Authors' contributions
MR and MF wrote the paper, IV and SM provided
clinical assistance and contributed to paper writing, MV and AG
performed the surgery and provided critical review of the paper.
All the authors have read and approved the final version of this
manuscript.
Competing interests
The authors declare that they have no competing
interests to disclose.
References
|
1
|
Salimov A and Ozer S: A rare location of
angiofibroma in the inferior turbinate in young woman. Int Arch
Otorhinolaryngol. 19:187–190. 2015.PubMed/NCBI
|
|
2
|
López F, Triantafyllou A, Snyderman CH,
Hunt JL, Suárez C, Lund VJ, Strojan P, Saba NF, Nixon IJ, Devaney
KO, et al: Nasal juvenile angiofibroma: Current perspectives with
emphasis on management. Head Neck. 39:1033–1045. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Osborn DA and Sokolovski A: Juvenile
nasopharyngeal angiofibroma in a female. Report of a case. Arch
Otolaryngol. 82:629–632. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Patrocínio JA, Patrocínio LG, Borba BH,
Bonatti BS and Guimarães AH: Nasopharyngeal angiofibroma in an
elderly woman. Am J Otolaryngol. 26:198–200. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Szymańska A, Korobowicz E and Gołabek W: A
rare case of nasopharyngeal angiofibroma in an elderly female. Eur
Arch Otorhinolaryngol. 263:657–660. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Windfuhr JP and Remmert S:
Extranasopharyngeal angiofibroma: Etiology, incidence and
management. Acta Otolaryngol. 124:880–889. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tiwari PK, Teron P, Saikia N, Saikia HP,
Bhuyan UT and Das D: Juvenile nasopharyngeal angiofibroma: A rise
in incidence. Indian J Otolaryngol Head Neck Surg. 68:141–148.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kania RE, Sauvaget E, Guichard JP, Chapot
R, Huy PT and Herman P: Early postoperative CT scanning for
juvenile nasopharyngeal angiofibroma: Detection of residual
disease. AJNR Am J Neuroradiol. 26:82–88. 2005.PubMed/NCBI
|
|
9
|
Lloyd G, Howard D, Phelps P and Cheesman
A: Juvenile angiofibroma: The lessons of 20 years of modern
imaging. J Laryngol Otol. 113:127–134. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Neel HB III, Whicker JH, Devine KD and
Weiland LH: Juvenile angiofibroma. Review of 120 cases. Am J Surg.
126:547–556. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liang J, Yi Z and Lianq P: The nature of
juvenile nasopharyngeal angiofibroma. Otolaryngol Head Neck Surg.
123:475–481. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gupta R and Agarwal SP: Juvenile
Nasopharyngeal Angiofibroma: Combined approach for excision,
transpalatal and endoscopic; a new perspective. Indian J
Otolaryngol Head Neck Surg. 70:125–129. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Patrocínio JA, Patrocínio LG, Martins LP
and da Cunha AR: Vision recovery following nasopharyngeal
angiofibroma excision. Auris Nasus Larynx. 29:309–311. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Conley J, Healey WV, Blaugrund SM and
Erzin KH: Nasopharyngeal angiofibroma in the juvenile. Surg Gynecol
Obstet. 126:825–837. 1968.PubMed/NCBI
|
|
15
|
Gruber B, Kron TK, Goldman ME and Matz GJ:
Nasopharyngeal angiofibroma in two young children. Otolaryngol Head
Neck Surg. 93:803–806. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Briant TD, Fitzpatrick PJ and Berman J:
Nasopharyngeal angiofibroma: A twenty year study. Laryngoscope.
88:1247–1251. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rupa V, Mani SE, Backianathan S and
Rajshekhar V: Management and outcome in patients with advanced
juvenile nasopharyngeal angiofibroma. J Neurol Surg B Skull Base.
79:353–360. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Economou TS, Abemayor E and Ward PH:
Juvenile nasopharyngeal angiofibroma: An update of the UCLA
experience, 1960-1985. Laryngoscope. 98:170–175. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jacobsson M, Petruson B, Svendsen P and
Berthelsen B: Juvenile nasopharyngeal angiofibroma. A report of
eighteen cases. Acta Otolaryngol. 105:132–139. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Huang RY, Damrose EJ, Blackwell KE, Cohen
AN and Calcaterra TC: Extranasopharyngeal angiofibroma. Int J
Pediatr Otorhinolaryngol. 56:59–64. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Szymańska A, Szymański M, Czekajska-Chehab
E and Szczerbo-Trojanowska M: Invasive growth patterns of juvenile
nasopharyngeal angiofibroma: Radiological imaging and clinical
implications. Acta Radiol. 55:725–731. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sternberg SS: Pathology of juvenile
nasopharyngeal angiofibroma; a lesion of adolescent males. Cancer.
7:15–28. 1954. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schiff M: Juvenile nasopharyngeal
angiofibroma. A theory of pathogenesis. Laryngoscope. 69:981–1016.
1959. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Allen PW: The fibromatoses: A
clinicopathologic classification based on 140 cases. Am J Surg
Pathol. 1:255–270. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Montag AG, Tretiakova M and Richardson M:
Steroid hormone receptor expression in nasopharyngeal
angiofibromas. Consistent expression of estrogen receptor beta. Am
J Clin Pathol. 125:832–837. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kruk-Zagajewska A, Piatkowski K and
Thielemann A: Value of free testosterone and estrogen-progesterone
receptor concentration in juvenile patients with angiofibroma.
Otolaryngol Pol. 56:561–565. 2002.PubMed/NCBI
|
|
27
|
Johns ME, MacLeod RM and Cantrell RW:
Estrogen receptors in nasopharyngeal angiofibromas. Laryngoscope.
90:628–634. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Johnsen S, Kloster JH and Schiff M: The
action of hormones on juvenile nasopharyngeal angiofibroma. A case
report. Acta Otolaryngol. 61:153–160. 1966. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Péloquin L, Klossek JM, Basso-Brusa F,
Gougeon JM, Toffel PH and Fontanel JP: A rare case of
nasopharyngeal angiofibroma in a pregnant woman. Otolaryngol Head
Neck Surg. 117:S111–S114. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tang IP, Shashinder S, Gopala Krishnan G
and Narayanan P: Juvenile nasopharyngeal angiofibroma in a tertiary
centre: Ten-year experience. Singapore Med J. 50:261–264.
2009.PubMed/NCBI
|