Introduction
Primary cardiac tumours are very uncommon, and
approximately 75% of primary cardiac tumours are benign. In adults,
myxoma is the most common type of primary benign cardiac tumours,
followed by lipoma, fibroma, and teratoma (1,2). The
incidence of primary cardiac lipomas is only 0.17–0.19% based on
autopsy reports (3). Cardiac lipomas
account for 8.4% of all primary cardiac tumours; they have no
gender or age predominance (4) and
they vary significantly in size (3).
Most cardiac lipomas arise from the endocardium or the epicardium,
while very few develop in the myocardial layer. Although there have
been reports of cardiac lipomas developing in both the atria and
the ventricles, they generally tend to develop in the right atrium
(4).
A cardiac lipoma should be distinguished from
cardiac liposarcoma. Liposarcoma was first reported by Virchow in
1857. Despite liposarcoma being the most common cancer of
mesenchymal origin in adults, 75% of liposarcoma cases occur in
deep muscle tissue of the limbs, 20% occur in the retroperitoneum,
and the remainder occur in other sites. Mediastinal liposarcoma is
extremely rare (5,6); primary mediastinal liposarcoma accounts
for only 0.13–0.75% of mediastinal cancers, and most occur in the
posterior mediastinum (6). Cardiac
liposarcoma is even rarer and account for approximately 1% of all
primary cardiac malignant tumours (2,7,8). Similar to cardiac lipomas, cardiac
liposarcoma has no gender predominance (9), and most also occur in the right atrium
(7).
The symptoms of cardiac lipoma and liposarcoma are
not obvious in the vast majority of cases, making them easy to be
missed in diagnosis. Moreover, cardiac lipoma and cardiac
liposarcoma (especially well-differentiated liposarcoma) are
sometimes difficult to distinguish, and they are easily
misdiagnosed.
This paper presents a case of multiple
well-differentiated cardiac liposarcoma with a concomitant
myocardial lipoma. We describe the patient's presentation including
details regarding their ultrasound, computed tomography (CT), and
magnetic resonance imaging (MRI) findings, to help improve the
diagnosis and treatment of this condition. To our knowledge the
coexistence of these two conditions has never been reported in the
literature.
Case report
A 49-year-old Chinese male experienced idiopathic
chest and back pain for >20 days and thus sought treatment at
the local hospital. Echocardiography indicated space-occupying
masses in the right atrium and pericardium. The patient was
recommended to seek further diagnosis and treatment at our
hospital. The patient had a history of an ischemic stroke that
occurred 2 years prior, but otherwise he had no past medical or
family history. After admission, a physical examination revealed
murmurs that changed with position at the left edge of the sternum,
between ribs 4 and 5. Laboratory examination did not reveal any
obvious abnormalities.
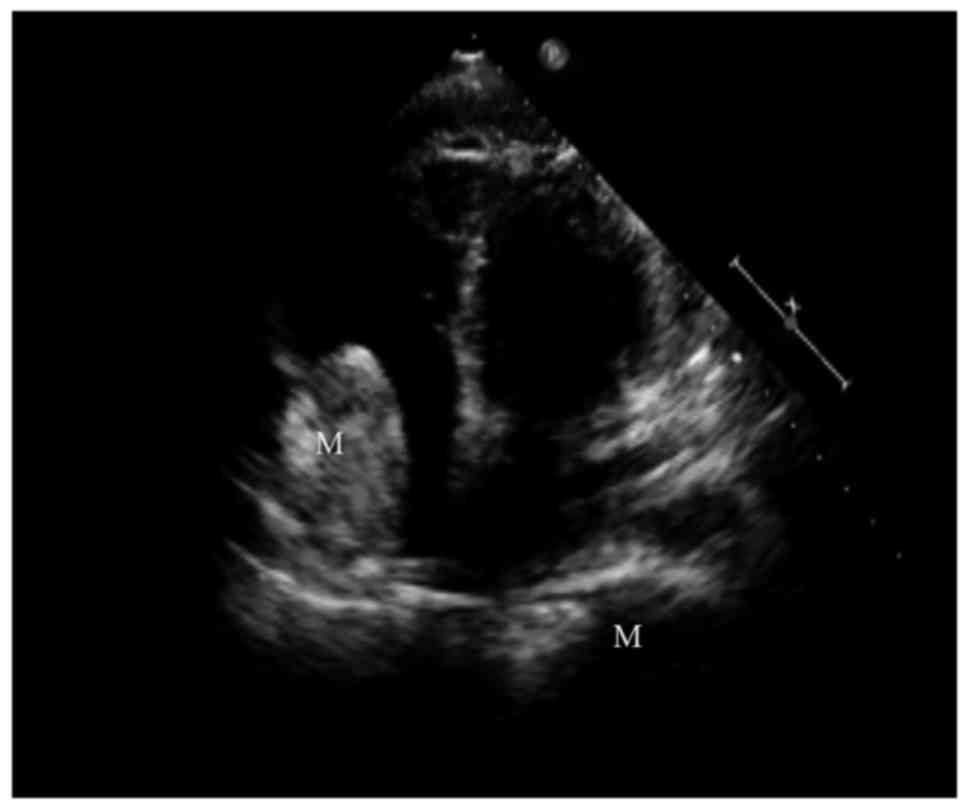
At our hospital, transthoracic echocardiography
indicated a very large solid mass (162×105 mm) in the pericardium
located primarily in the posterior of the heart and surrounding it,
with an inhomogeneous hypoechoic interior accompanied with
hyperechoic bands. Deformation of the cardiac apex was accompanied
by a local protrusion (32×28 mm), inside which the blood flow
signal was visible. Moderately hyperechoic lumps (48×31 mm) were
visible in the right atrium (Fig.
1). The mass was connected to the lateral wall of the right
atrium near the atrioventricular ring by a stem like connection,
which moved with the cardiac cycle and with mild tricuspid valve
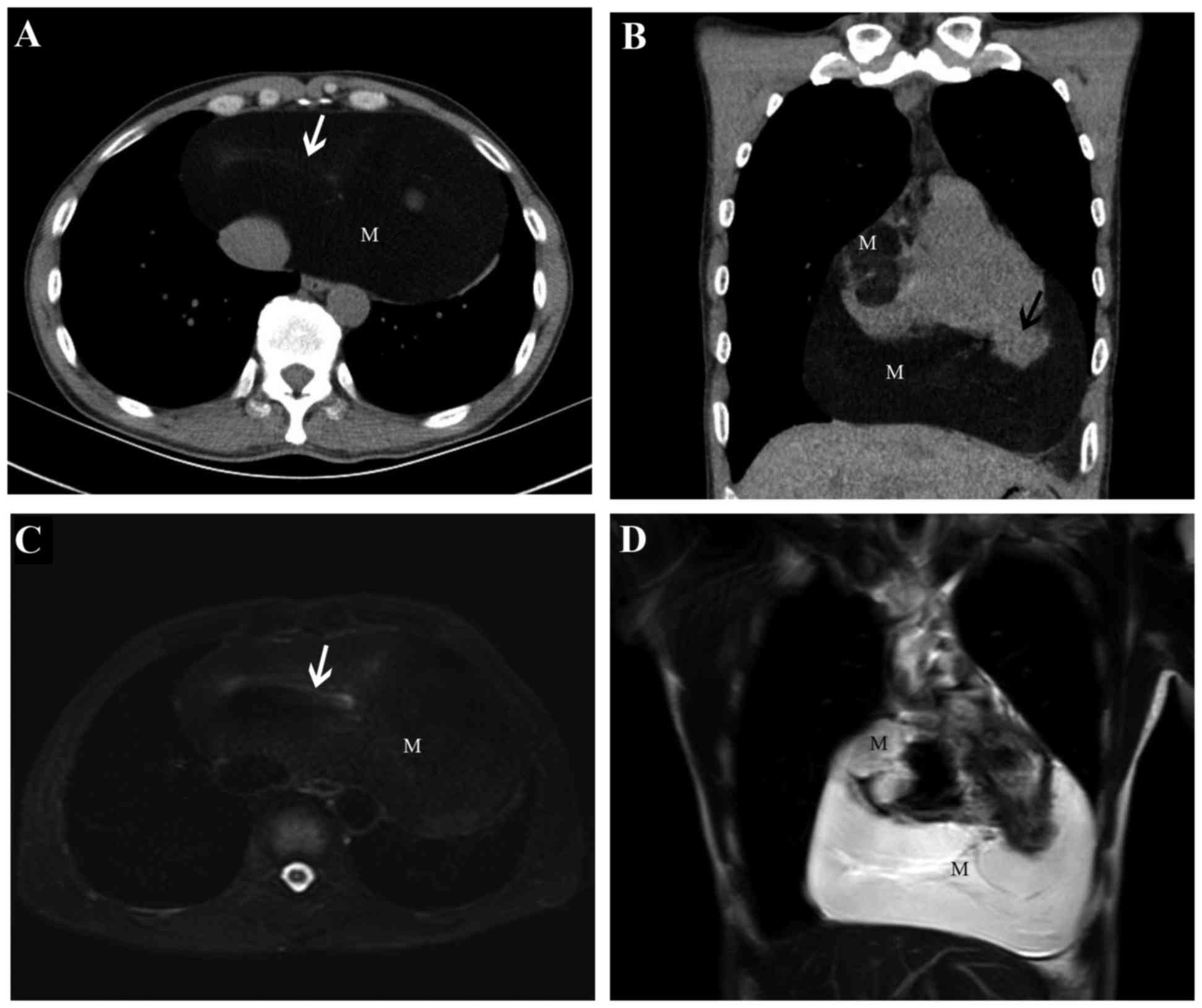
regurgitation. Further CT scanning showed a dense mass with highly
homogeneous fat inside the pericardium, inside which a few slightly
high-density slivers were visible. In the right atrium, a dense
fatty mass with lobulation was visible, and the boundary between
the mass and the right atrial wall was unclear (Fig. 2). After obtaining written informed
consent from the patient, a free contrast-enhanced cardiac MRI
examination was performed. The results showed that the pericardial
mass was composed of fat, and its interior was not enhanced. The
mass in the right atrium was also composed of fat, and an envelope
was visible in its periphery. The mass was continuous with the
lateral right atrial wall and it oscillated with blood flow. The
local protrusions in the cardiac apex had weaker movement, and a
narrow neck-like connection with the left ventricle was visible
(Fig. 2). Considering the medical
history of the patient, the various examinations performed, and
additional discussion, we made a diagnosis of right atrial and
pericardial lipomas and apical diverticula. The cardiac surgeon
decided to surgically remove the cardiac lipomas.
With the patient on extracorporeal circulation, a
median sternotomy was performed, and the pericardium was opened. A
very large fatty mass (20.4×13.5×5 cm3) was visible
between the bottom of the heart and the diaphragm and was
continuous with the cardiac apex. In addition, a fatty mass
(6×3.5×2 cm3) was visible in the right atrial wall
protruding into the atrium. The fatty masses in the pericardium and
right atrium were completely resected. After opening the right
atrial wall, multiple small fatty masses (the size of the larger of
these masses was 3×2×1.5 cm3) were visible in the right
atrial wall; these were also resected. The pericardial membrane
naturally repaired the right atrium, and indwelling drainage tubes
were placed in the pericardium and behind the sternum.
Postoperative pathological examination revealed
atypical lipomas (well-differentiated liposarcoma) in the
pericardium and the right atrial wall (Fig. 3), and a myocardial lipoma was
identified in the right atrium (Fig.
3). The patient had a large amount of postoperative pericardial
drainage, and an open chest surgery was performed the following
night. The wound exhibited slight blood seepage, and once
haemostasis was confirmed, the undiscovered active bleeding was
investigated. The patient was postoperatively given an infusion of
red blood cells and plasma to alleviate anaemia and coagulation.
The patient was discharged on postoperative day 9, the symptoms
disappeared, and follow-up after 1 year did not reveal
recurrence.
This study was conducted with written informed
consent from the patient.
Discussion
Pathologically, a cardiac lipoma can be categorized
into two types: Lipomatous hypertrophy of the interatrial septum
and a true lipoma (1,3). Lipomatous hypertrophy tends to develop
in the interatrial septum and usually develops continually with the
epicardial fat. A true lipoma, on the other hand, is a mass
composed of encapsulated adipose tissue, usually mature adipocytes
(3,4). When a lipoma invades the myocardium,
the tumour is known as a myocardial lipoma. If fibrous components
appear, then the tumour is known as a fibrolipoma. If the tumour
contains only adipocytes, it is known as a lipoma (1). In our patient, the mass in the right
atrium had invaded the myocardium, and proliferating adipose tissue
was observed in the myocardium by microscopy. Accordingly, the
pathological diagnosis was myocardial lipoma.
The criteria for liposarcoma diagnosis and
classification are based on the pathological criteria established
by the WHO (10). Liposarcomas can
be divided into four subtypes: Well-differentiated liposarcoma (or
atypical lipoma), myxoid/round cell liposarcoma, pleomorphic
liposarcoma, and dedifferentiated liposarcoma. Well-differentiated
liposarcoma accounts for 40–45% of liposarcoma cases and they
usually have a very low degree of malignancy (2). A lipomatous presentation is the most
common presentation among the various types of well-differentiated
liposarcoma (6). Local lesion cells
with slightly enlarged nuclei were visible in the masses in the
pericardium and right atrial wall of our patient, and the
pathological diagnosis was lipomatous well-differentiated
liposarcoma (or atypical lipoma).
Cardiac lipomas are usually asymptomatic due to
their slow rates of growth and softness (11,12), and
are usually serendipitously discovered in autopsies or examinations
for other reasons. Cardiac liposarcoma tends to invade neighbouring
organs, so they are more likely to cause symptoms than lipomas,
which only compress surrounding organs (6). The symptoms of cardiac lipoma and
liposarcoma are generally similar, and patients often present with
fatigue, dyspnoea, syncope, chest discomfort, chest pain,
palpitation, and even sudden death (3,11). The
appearance of symptoms is usually determined by the location and
size of the tumour. If the tumour is located under the pericardium,
it may grow to a large size but remain asymptomatic; such tumours
are often clinically discovered at a late stage. Many pericardial
lipomas can cause dyspnoea by occupying the air spaces of the lungs
or compressing the heart. Chest pain can be caused by compression
of the coronary arteries by the tumour. Tumours located near the
valves may lead to valve regurgitation. Finally, myocardial lipomas
that interfere with the conduction system can lead to arrhythmias
(12,13). Our patient had a myocardial lipoma in
the right atrium, and as a result, exhibited mild tricuspid valve
regurgitation and heart murmur on physical examination. The
patient's chest and back pain may have been caused by the atypical
lipoma compressing the coronary arteries.
Conventional X-ray examinations cannot usually
achieve an accurate diagnosis of cardiac tumours. Thus,
transthoracic echocardiography has become an extremely valuable
method for the initial discovery and diagnosis of cardiac tumours
due to its high accuracy and non-invasiveness. On transthoracic
echocardiography, pericardial lipomas usually present a relatively
anechoic structure. In contrast, lipomas in the heart cavity have
an echoic presentation (12).
However, CT and MRI, and especially contrast-enhanced examination,
are the most important and valuable methods for providing
information on tumour size, location, and composition. Lipomas are
often easily distinguishable by CT because they are composed of
low-density tissue. On MRI, lipomas present with high signal
intensity on T1- and T2-weightedimages, and the signal is
significantly decreased when fat suppression sequences are used
(14). Liposarcoma often presents
with disordered density on conventional CT scanning. In addition,
calcification is occasionally observed. On MRI, liposarcoma is
often presented as primarily lipid signals with irregular mixed
signal, and sometimes only present as a small number of soft tissue
bands within the lipid signals. On enhanced CT and MRI, they often
present as irregular enhancements (13). However, our patient presented with
homogeneous adipose density or signal, and the well-differentiated
liposarcoma in the pericardium only presented as a small number of
bands with no definite enhancement observed. This suggests that CT
and MRI are still insufficient for distinguishing between lipoma
and well-differentiated liposarcoma. Consistently, the results of a
study by Goto et al (7) also
suggest that CT and MRI cannot distinguish between benign and
malignant cardiac pathologies.
In addition to imaging examination, biopsy is often
insufficient for the accurate diagnosis of lipomatous masses,
especially for distinguishing between lipomas and
well-differentiated liposarcoma. This difficulty arises because
biopsy sample collection can only partially represent the degree of
differentiation, and immunohistochemical and ultrastructural
analysis cannot be completed with insufficient sample collection.
Thus, accurate diagnosis often requires open surgery or
pathological examination of resected tissue (6).
It is exactly because neither imaging nor biopsy can
accurately diagnose lipomatous masses, and because cases of sudden
death have been reported, that we advocate for proactive surgical
resection. This is also true for asymptomatic patients whose masses
are accidently found, followed by patient management and
determination of the prognosis based on postoperative pathological
classification. According to the literature, cardiac lipoma
patients that undergo surgical resection have good prognoses
(15), and to our knowledge there
are currently no case reports of recurrence. The prognosis for
cardiac liposarcoma is primarily determined by pathological subtype
and the range of safety of surgical resection. The recurrence rate
is approximately 40%, and the longest time to recurrence has been
reported as 14 years post-operation (6). The patient described in the present
report did not undergo chemotherapy after successful surgical
resection and exhibited no signs of recurrence when re-examined 1
year after surgery.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and material
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
FK performed the majority of the experiments. WZ
captured and assessed the images, and critically analysed the
manuscript for important intellectual content. QG conceived the
study and gave final approval of the version to be published. All
authors read and approved the contents of the final draft of the
manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient.
Patient consent for publication
Written informed consent was obtained from the
patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
H&E
|
haematoxylin and eosin
|
References
|
1
|
Habertheuer A, Andreas M, Wiedemann D,
Rath C and Kocher A: A rare case of obstructive right atrial
lipoma. Ann R Coll Surg Engl. 96:e39–e41. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Papavdi A and Agapitos E: Undiagnosed
primary cardiac liposarcoma in an adult: A case report and review
of the literature. Am J Forensic Med Pathol. 34:299–301. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wu S, Teng P, Zhou Y and Ni Y: A rare case
report of giant epicardial lipoma compressing the right atrium with
septal enhancement. J Cardiothorac Surg. 10:1502015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Khoueiry G, Abi Rafeh N, Waked A, Abdo A,
Azab B, Asgarian KT and Snyder ST: Left atrial appendage lipoma: An
unusual location of cardiac lipomas. Echocardiography. 28:E91–E93.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ortega P, Suster D, Falconieri G, Zambrano
E, Moran CA, Morrison C and Suster S: Liposarcomas of the posterior
mediastinum: Clinicopathologic study of 18 cases. Mod Pathol.
28:721–731. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Steger CM: Primary liposarcoma of the
heart. BMJ Case Rep. 2011(pii): bcr03201140132011.PubMed/NCBI
|
|
7
|
Goto T, Ohte N, Tani T, Suda H and Kimura
G: Malignant nature of cardiac liposarcoma revealed by fluorine-18
fluorodeoxyglucose positron emission tomographic imaging. Intern
Med. 51:1367–1370. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Grebenc ML, Rosado de Christenson ML,
Burke AP, Green CE and Galvin JR: Primary cardiac and pericardial
neoplasms: Radiologic-pathologic correlation. Radiographics.
20:1073–1103. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Araoz PA, Eklund HE, Welch TJ and Breen
JF: CT and MR imaging of primary cardiac malignancies.
Radiographics. 19:1421–1434. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fletcher CDM, Unni KK and Mertens F: World
Health Organization classification of tumors. Pathology and
genetics of tumors of soft tissue and bone. Kleihues P and Sobin
LH: IARC; Lyons: pp. pp35–46. 2002
|
|
11
|
Zwolinski R, Ammer A, Walczak A and
Jaszewski R: Intrapericardial lipoma: Diagnosed unexpectedly and
resected during coronary artery bypass surgery. Interact Cardiovasc
Thorac Surg. 11:211–212. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Vijay SK, Dwivedi SK, Chandra S and Saran
RK: Giant intrapericardial lipoma: An unusual cause of dyspnoea.
Indian Heart J. 65:104–106. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhu H, Wang M, Feng D, Feng Y, Ren Y, Chen
J, He Y and Yuan J: Ultrasonography, X-ray and CT imaging findings
of a giant pericardial lipoma: Imaging diagnosis and review of the
literature. Oncol Lett. 7:195–198. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
van Beek EJ, Stolpen AH, Khanna G and
Thompson BH: CT and MRI of pericardial and cardiac neoplastic
disease. Cancer Imaging. 7:19–26. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Girrbach F, Mohr FW and Misfeld M:
Epicardial lipoma-a rare differential diagnosis in cardiovascular
medicine. Eur J Cardiothorac Surg. 41:699–701. 2012. View Article : Google Scholar : PubMed/NCBI
|