Introduction
Malignant gliomas (MGs) are the most common primary
malignant brain tumours in adults (~60% of the total) (1). According to WHO classification of brain
tumours, MGs include grade III gliomas (or anaplastic gliomas-AGs)
and glioblastoma multiforme (GBM) (2,3), which
is the most frequent and aggressive MG, characterised by a high
recurrence and mortality rate. Standard first-line therapy of GBM
includes maximal-safe surgical resection followed by radiotherapy
plus concomitant and adjuvant temozolomide (TMZ), as defined in the
EORTC Phase III trial (4). Despite
the optimal standard treatment, recurrence rates are high (~90%)
with median survival ranges from 15–18 months for GBM (5) and from 2–5 years for AGs (6).
On the contrary, there are no standard therapies for
recurrent MGs. Different options are under investigation, including
resurgery, reirradiation and chemotherapy, and their combinations
(7).
Fotemustine (FTM) is a third-generation nitrosourea,
an alkylating agent, which is a widely used and studied therapeutic
option for MGs recurring after TMZ treatment, especially in Europe
(8–11).
There are two types of FTM schedule. The standard
schedule includes an induction phase dose of 100 mg/mq weekly for 3
consecutive weeks followed by a 5-week rest period and a
maintenance phase dose of 100 mg/mq every 3 weeks (12–15).
Haematological toxicity is observed in >30% of patients
(9,16), mainly at the end of the induction
phase, with grade 3–4 thrombocytopenia and neutropenia occurring in
~14% of patients (11).
In 2011 Addeo et al proposed a fractionated
FTM schedule which includes an induction phase dose of 80 mg/mq
every 2 weeks for 5 consecutive weeks followed by a 4-week rest
period and a maintenance phase dose of 80 mg/mq every 4 weeks
(16). This treatment is associated
with a lower rate of myelotoxicities, with grade 3 thrombocytopenia
and leukopenia occurring in only 7 and 3% of patients respectively
(10,16).
Resurgery and reirradiation are two controversial
therapeutic options due to the lack of prospective randomized
trials but multiple trials have studied their survival and clinical
benefit especially in combination with subsequent chemotherapy
(7,17,18).
We retrospectively analysed recurrent MGs patients
receiving fractionated FTM schedule proposed by Addeo et al
(16) in order to evaluate the
efficacy and safety of this second-line option according to disease
and treatment subgroup analysis and compared to the literature.
Patients and methods
Study population
From the database of the Department of Oncology Unit
A of Policlinico Umberto I, Sapienza University of Rome, we
performed a retrospective analysis of consecutive recurrent MGs
patients treated with Addeo FTM schedule after a first-line therapy
with maximum safe resection and adjuvant TMZ-based therapy. We
excluded those patients with evidence of cerebral haemorrhage on
baseline MRI, treated with FTM standard schedule or FTM combined
with other therapies or affected by clinically significant medical
conditions that would make the treatment unsafe.
For all patients, the initial diagnosis was
established by magnetic resonance imaging (MRI) and histologically
using WHO criteria.
O6-methylguanine-DNA methyltransferase
(MGMT) promoter methylation and IDH mutation analyses were
performed (3) using a digital
polymerase chain reaction (PCR) method. The recurrence after
first-line therapy was established by MRI and histological
examination when surgery was performed.
Clinical data at recurrence included patients
characteristics (sex, age and Karnofsky performance status (KPS) at
recurrence) tumour characteristics (laterality and lobe interested,
histotype at recurrence, MGMT methylation and IDH mutation status
at diagnosis) and treatment information (surgery and radiotherapy
at recurrence, line of treatment and median cycles of FTM,
first-line therapy, interval between completion of RT/TMZ and
recurrence, next lines of chemotherapy and completion of induction
phase).
Treatment plan
All patients included in the analysis underwent
second-line treatment with FTM alone, according to the new Addeo
schedule (16): induction phase dose
of 80 mg/mq every 2 weeks for 5 consecutive weeks followed by a
4-weeks rest period and a maintenance phase dose of 80 mg/mq every
4 weeks.
Response and toxicity evaluation
All patients were followed clinically by a
multidisciplinary team and radiologically by MRI scans. The
evaluations were made after the induction phase (5 cycles of
chemotherapy) and then every 2 cycles during the maintenance phase
or whenever progression disease was clinically suspected.
Evaluation response was assessed according to RANO criteria
(19) as complete (CR) and partial
(PR) response, stable (SD) and progression (PD) disease. Disease
control (DC) was defined as the sum of CR, PR and SD. Diagnosis of
recurrence was determined by MRI in all patients and by
histological examination when a second surgical resection was
made.
All adverse events, as worsening of previous
symptoms or development of new symptoms during treatment, were
graded according to the Common Terminology Criteria for Adverse
Events (CTCAE) of the National Cancer Institute, version 4.03
(20). Toxicity was evaluated at
2-weekly intervals or, if clinically indicated, at weekly
intervals.
Statistical analysis
Survival analysis was conducted on the efficacy of
FTM in recurrent MGs in terms of 6 and 12 months progression-free
survival (PFS) and overall survival (OS), median PFS (mPFS) and OS
(mOS) from FTM treatment. Safety analysis evaluated the toxicity
profile of FTM Addeo schedule compared to the standard
schedule.
PFS was measured from the start of FTM therapy to
diagnosis of PD evidenced by MRI or to death from any cause or to
last follow-up assessment. OS was measured from the start of
treatment with FTM to death from any cause or last follow-up.
Median PFS and OS were estimated with their 95%
confidence interval. Survival curves of PFS and OS were generated
using the Kaplan-Meier method (21).
Differences in PFS and OS were evaluated using the log-rank test
(Mantel-Cox) for statistical significance, which was defined at the
p<0.05 level (21).
Results
Patients' characteristics
Between August 2010 and October 2017, 40 patients
with recurrent MGs receiving FTM schedule proposed by Addeo et
al as second-line treatment were included in the analysis.
Patient, tumour and treatment characteristics at recurrence are
summarised in Table I.
 | Table I.Patient (n=40) and tumor
characteristics at recurrence. |
Table I.
Patient (n=40) and tumor
characteristics at recurrence.
|
Characteristics | n (%) |
|---|
| Sex |
|
|
Male | 27 (68) |
|
Female | 13 (32) |
| Median age, years
(range) | 54 (25–75) |
| Karnofsky
performance status |
|
| Median
(range) | 80 (60–90) |
|
90–100 | 7 (17) |
|
70–80 | 28 (70) |
| 60 | 5 (13) |
| Laterality |
|
|
Right | 22 (55) |
|
Left | 18 (45) |
| Histotype |
|
|
Glioblastoma multiforme | 34 (85) |
|
Anaplastic glioma | 6 (15) |
| MGMT promoter
methylation status at diagnosis |
|
|
Methylated | 20 (50) |
|
Unmethylated | 16 (40) |
|
Unknown | 4 (10) |
| IDH mutation status
at diagnosis |
|
|
Mutated | 11 (28) |
| Non
mutated | 16 (40) |
|
Unknown | 13 (32) |
| Surgery at
recurrence |
|
|
Yes | 25 (63) |
| No | 15 (37) |
| RT at
recurrence |
|
|
Yes | 17 (42) |
| No | 23 (58) |
| Interval between
completion of RT/TMZ and recurrence |
|
| ≤3
months | 7 (17) |
| >3
months | 33 (83) |
| No. of lines of
chemotherapy after FTM |
|
|
None | 24 (60) |
|
One | 11 (28) |
|
Two | 3 (7) |
| In
progress with FTM | 2 (5) |
| Median cycles
received, no. (range) | 5 (2–50) |
| Induction phase
completed |
|
|
Yes | 27 (68) |
| No | 13 (32) |
Most patients were male (68%), the median age was 54
years (range 25–75 years) and median KPS was 80 (range, 60–90). All
patients had a histological diagnosis of MGs: GBM was the
predominant histotype (85%), while grade III gliomas represented
the 15% of the total. At first relapse all grade-III grade gliomas
evolved in GBM (secondary GBM), whose diagnosis was made
radiologically in 5 patients and histologically after resurgery in
1 patient.
The assessment of the MGMT promoter methylation
status was conducted in 36 patients (90%). MGMT promoter was
methylated in 20 patients (50%) and unmethylated in 16 patients
(40%). The assessment of the IDH mutation status was conducted in
25 patients (68%). IDH gene was mutated in 5 patients (13%) and non
mutated in 22 patients (55%).
All patients underwent surgery at diagnosis and were
treated as first-line treatment with radiotherapy plus concomitant
and adjuvant TMZ as Stupp protocol (4). At first recurrence, 63% of patients
underwent resurgery and 42% of patients were treated with
radiotherapy.
All patients received FTM as second-line treatment
according to Addeo schedule. Most patients (83%) started FTM after
3 months from TMZ last administration, in order to reduce the
influence of pseudoprogression effect on the occurrence
evaluation.
All patients received at least two doses of FTM. The
median number of cycles administered was 5 (range, 2–50) with a
completion of the induction phase in the 68% of patients. The main
reason for not beginning maintenance phase was disease progression.
Fourteen patients (35%) with progressive disease after FTM
underwent further lines of chemotherapy: 11 patients (28%)
underwent a third line chemotherapy and 3 patients (7%) up to a
fourth line.
Activity evaluation
All patients included in the study were assessable
for response analysis (Table II).
Among the 40 patients, 5 patients achieved PR (13%) and 19 patients
SD (47%) with a DCR of 60%.
| Table II.Results of FTM as second-line therapy
in malignant gliomas. |
Table II.
Results of FTM as second-line therapy
in malignant gliomas.
| A, Objective
responses, n (%) |
|---|
|
|---|
|
| GBM | AG | Total patients |
|---|
| Response |
|
Complete responses | 0 (0) | 0 (0) | 0 (0) |
| Partial
response | 3 (9) | 2 (33) | 5 (13) |
| Stable
disease | 17 (50) | 2 (33) | 19 (47) |
|
Progressive disease | 14 (41) | 2 (33) | 16 (40) |
| Disease
control | 20 (59) | 4 (67) | 24 (60) |
|
|
| B, Survival
data |
|
|
Survival |
|
| Values |
|
| 6
months-PFS, % |
|
| 33 |
| 12
months-PFS, % |
|
| 13 |
| Median PFS, months
(range) |
|
| 4 (2–49)
(3.02–5) |
| (95%
CI) |
|
|
|
| 6
months-OS, % |
|
| 55 |
| 12
months-OS, % |
|
| 30 |
| Median
OS, months (range) |
|
| 9 (2.5–50.5)
(7.36–10.64) |
| (95% CI) |
|
|
|
| Complete responses,
% |
|
| 33 |
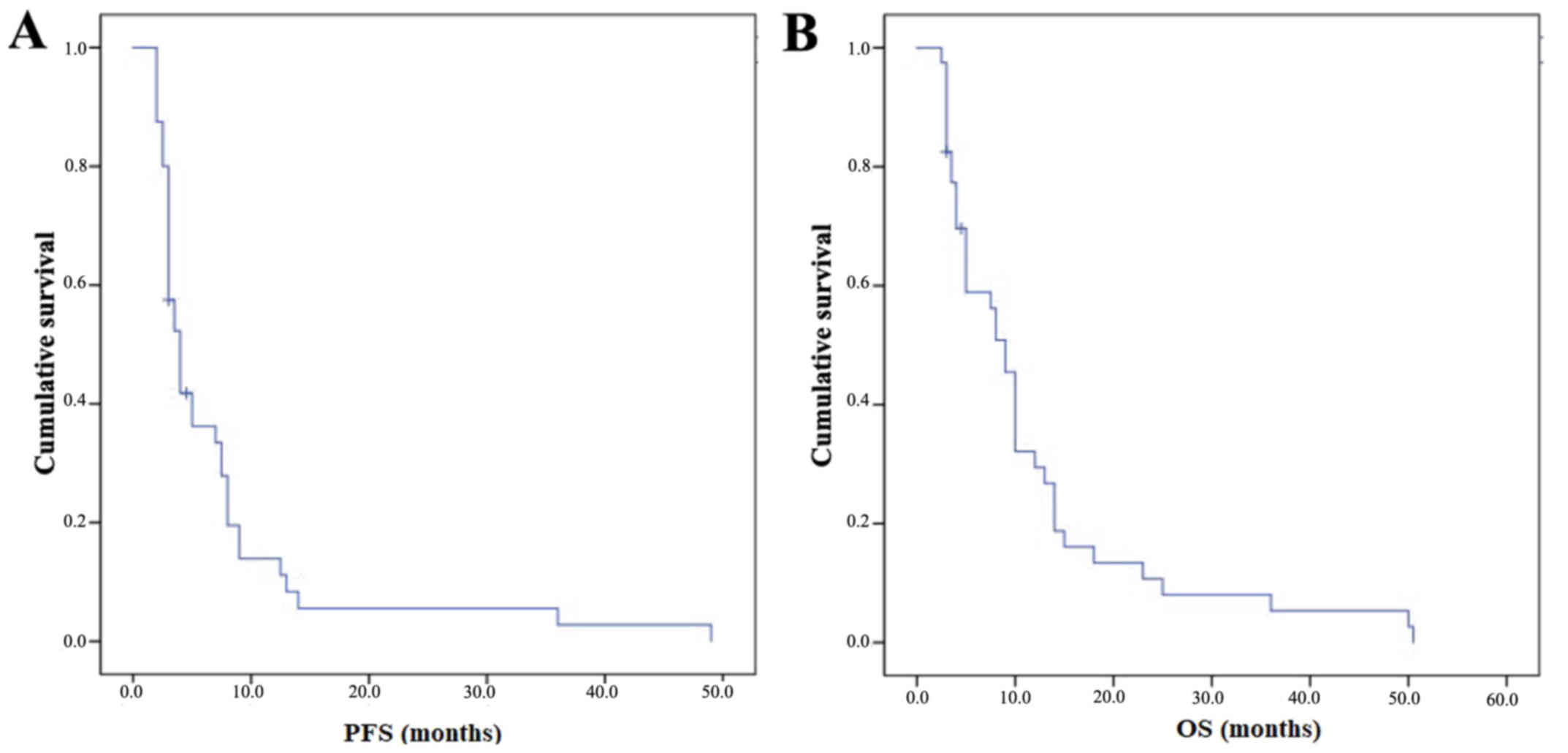
The mPFS was 4 months (95% CI 3.02–5) with a PFS-6
of 33% and a PFS at 1 year (PFS-1y) of 13% (Fig. 1A). The mOS from the start of FTM was
9 months (95% CI 7.36–10.64) with an OS at 6 months of 55% and an
OS at 1 year of 30% (Fig. 1B).
Subgroup analyses were performed and are summarised in Table III.
| Table III.Subgroup analyses. |
Table III.
Subgroup analyses.
|
| No. of
patients | mPFS | 95% CI | P-value | mOS | 95% CI | p-value |
|---|
| KPS, % |
|
>70 | 28 | 5.0 | 3.8–6.2 | 0.72 | 10 | 5.3–14.7 | 0.22 |
|
<70 | 12 | 4.0 | 0–10.8 |
| 8 | 3.8–12.2 |
|
| MGMT
methylation |
|
Yes | 20 | 6.0 | 3.0–8.9 | 0.004 | 10 | 6.5–13.5 | <0.0001 |
| No | 16 | 3.0 | 2.5–3.5 |
| 4 | 2.2–5.8 |
|
| IDH mutation |
|
Yes | 11 | 4.0 | 2.4–5.6 | 0.94 | 10 | 6.4–13.6 | 0.91 |
| No | 16 | 3.0 | 1.3–4.7 |
| 10 | 4.4–15.6 |
|
| Induction phase
completed |
|
Yes | 27 | 6.0 | 4.1–7.9 | 0.02 | 10 | 8.8–11.2 | 0.004 |
| No | 13 | 3.0 | 1.7–4.3 |
| 4 | 2.2–5.8 |
|
| RT ar
recurrence |
|
Yes | 17 | 5.0 | 2.9–7.1 | 0.48 | 10 | 3.7–6.3 | 0.11 |
| No | 23 | 3.5 | 2.5–4.5 |
| 5 | 0.11 |
|
| Surgery at
recurrence |
|
Yes | 25 | 6.0 | 0.1–11.9 | 0.18 | 9 | 5.6 12.4 | 0.95 |
| No | 15 | 5.0 | 3.9–6.1 |
| 9 | 2–16 |
|
Patients who completed the induction phase (n=27)
experienced longer survival outcomes with a mPFS of 6 vs. 3 months
(p=0.02) and a mOS of 10 vs. 4 months (p=0.004). Patients with a
KPS >70% (70%) were associated with a higher OS (10 vs. 8
months) and a similar PFS (5 vs. 4 months) compared to patients
with a lower KPS.
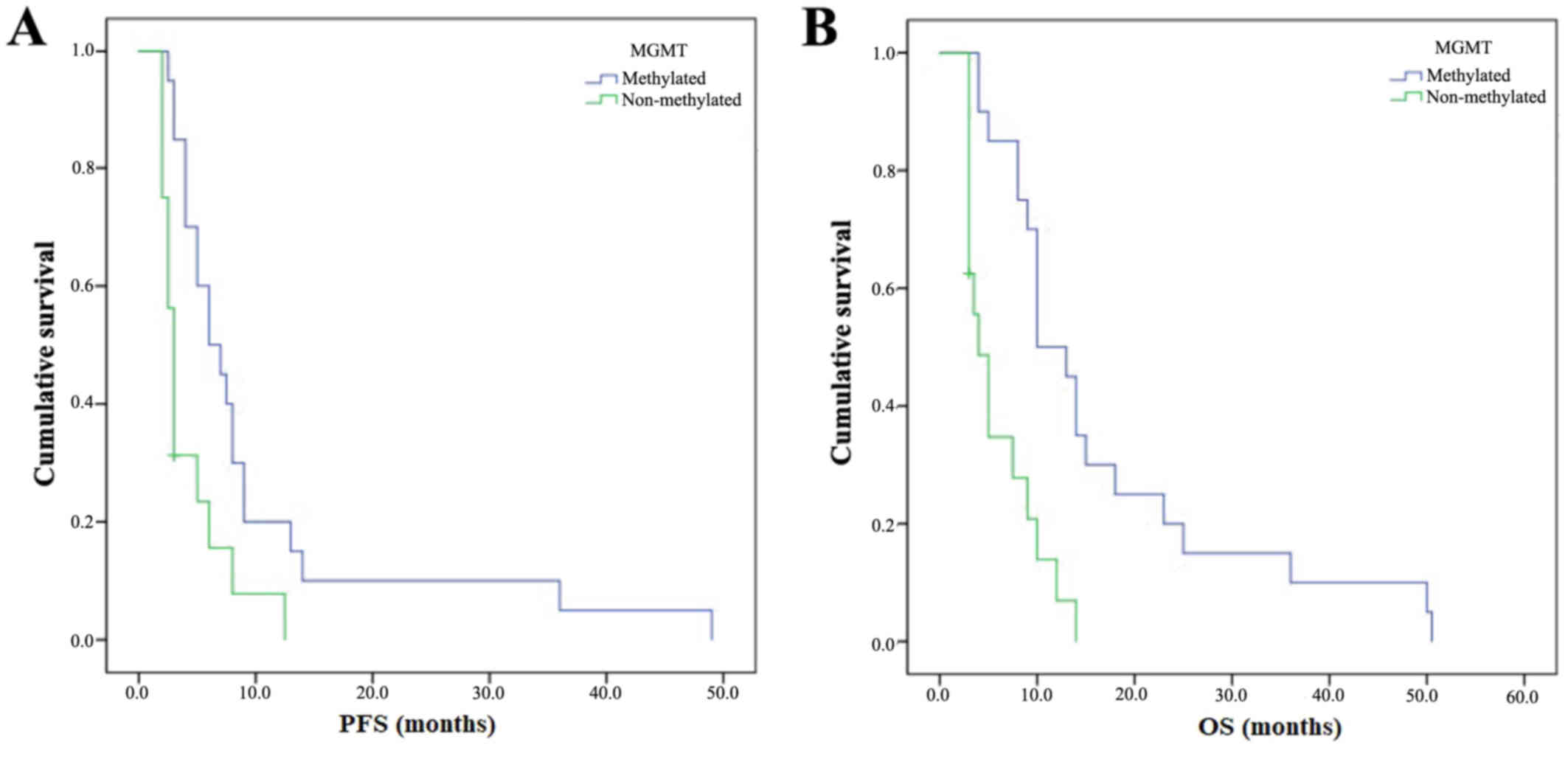
Activity according to MGMT
methylation
Methylated patients (n=20) experienced longer mPFS
(6 vs. 3 months) (Fig. 2A) and mOS
(10 vs. 4 months) compared to unmethylated patients (n=16) with
statistical significance (p=0.004 and p<0.0001 respectively)
(Fig. 2B). Subgroup analyses
according to IDH mutation were not performed due to the low number
of patients.
Activity according to resurgery and
reirradiation
Patients treated with radiotherapy at recurrence
(n=17) before FTM therapy experienced longer mPFS (5 vs. 3.5
months) and longer mOS (10 vs. 5 months) without statistical
significance (p=0.48 and p=0.11 respectively).
Patients who underwent surgery at recurrent (n=25)
before FTM therapy had similar mPFS (6 vs. 5 months) and mOS (both
9 months) compared to patients who did not undergo resurgery.
Toxicity evaluation
All 43 patients were evaluated for safety (Table IV). Grade 3–4 haematological
toxicities were developed in 15% of patients. Grade 3–4
thrombocytopenia and leukopenia occurred respectively in 6% of
patients each. Grade 3 neutropenia was observed in 3% of patients.
None of the patients developed grade 3–4 anaemia. No grade 3–4
non-haematological toxicities were recorded. The haematological
toxicity incidence has a peak in correspondence of the induction
completion, while during maintenance phase a higher incidence of
hepatic, renal and general toxicity was observed. FTM was generally
well tolerated and treatment interruption or death related to
chemotherapy toxicity were not documented.
| Table IV.Toxicities by grade of severity,
according to the CTCAE (version 4.03). |
Table IV.
Toxicities by grade of severity,
according to the CTCAE (version 4.03).
|
Chemotherapy-related toxicity | Grade 1, n (%) | Grade 2, n (%) | Grade 3, n (%) | Grade 4, n (%) |
|---|
| Haematological |
|
Thrombocytopenia | 14 (38) | 5 (14) | 1 (3) | 1 (3) |
|
Leukopenia | 11 (30) | 6 (16) | 1 (3) | 1 (3) |
|
Neutropenia | 5 (14) | 4 (11) | 1 (3) | – |
|
Lymphopenia | 3 (8) | 4 (11) | 3 (8) | 1 (3) |
|
Anemia | 14 (38) | 3 (8) | – | – |
|
Hypertransaminasemia |
|
ALT | 9 (24) | 1 (3) | – | – |
|
AST | 1 (3) | – | – | – |
|
γGT | 4 (11) | 2 (5) | – | – |
| Renal |
|
Creatinine increase | 7 (19) | – | 1 (3) | – |
|
Gastrointestinal |
|
Nausea | 5 (14) | 2 (5) | – | – |
|
Diarrhea | – | 1 (3) | 1 (3) | – |
|
Mucositis | 1 (3) | – | 1 (3) | – |
| General |
|
Astenia | 6 (16) | 6 (16) | 1 (3) | – |
|
Anorexia | – | 2 (5) | 6 (16) | – |
Discussion
Radiotherapy plus concomitant and adjuvant TMZ has
become the standard treatment for newly diagnosed MGs with an
improvement in OS and PFS compared to radiotherapy alone (4). However, recurrence probability is high
(~90%) and there is no consensus on second-line therapy, with
treatment recommendations based on non-controlled phase II
trials.
Nitrosoureas are the most widely studied therapeutic
option, particularly FTM, a third generation nitrosourea. The use
and efficacy of FTM as second-line treatment in recurrent MGs are
known especially in the conventional schedule proposed by Frenay
et al (tree weekly FTM cycles at 100 mg/mq followed by a
5-week rest and a maintenance phase with 100 mg/mq of FTM every
three weeks) (12).
Several Italian phase II trials (6,13–15,22)
have investigated the use of FTM conventional schedule in MGs
patients recurring after Stupp standard treatment with a wide range
of survival data (Table V).
| Table V.Clinical trial on fotemustine as
second-line chemotherapy in recurrence MGs after temozolomide
failure. |
Table V.
Clinical trial on fotemustine as
second-line chemotherapy in recurrence MGs after temozolomide
failure.
| Authors, year | No of patients | Histotype | Recurrence | Schedule | mPFS, months | PFS6, % | mOS, months | DCR, % | Grade 3–4
toxicity | (Refs.) |
|---|
| Scoccianti et
al, 2008 | 27 | GBM | II | Standard | 5.7 | 48.15 | 9.1 | 48.1 | 14.8% | (13) |
| Fabrini et
al, 2009 | 50 | MGs | II | Standard | 6.1 | 51.5 | 8.1 | 62.0 | 14% | (14) |
| Brandes et
al, 2009 | 43 | GBM | II | Standard | 1.7 | 20.9 | 6.0 | 42.5 | 50% | (15) |
| Fabi et al,
2009 | 40 | MGs | II and III | Range of doses | 4.0 | 27.0 | 30.0 | 47.5 | 40% higher dose
(standard schedule) | (22) |
| Fabi et al,
2010 | 40 | MGs | II and III | Low dose | 3.0 | 21.0 | 6.0 | 52.5 | 27.5% | (6) |
| Addeo et al,
2011 | 40 | GBM | II | Fractionated | 6.7 | 61.0 | 11.1 | 65.0 | 12.5% induction
phase 17.7% maintenance phase | (16) |
| Gaviani et
al, 2013 | 20 | MGs | II and III | Fractionated | 3.7 | 38.2 | 6.9 | NA | 19.2% | (15) |
| Present study | 40 | MGs | II | Fractionated | 4.0 | 33.0 | 9.0 | 60.0 | 24.3% |
|
Scoccianti et al (13) and Fabrini et al (14) reported similar survival results in
terms of PFS-6 rates (~50%), mPFS (nearly 6 months), mOS (nearly
8.6 months), DCR (~55%) and grade 3–4 haematological toxicities
(~14%) in 27 GBM and 50 MGs patients respectively.
Brandes et al (15) reported a mPFS and OS of 1.7 and 6
months respectively with a 6-PFS of 20,9% and a DRC of 42,5%.
Haematological toxicity was high with grade 3–4 adverse events in
nearly 50% of patients. This was the first study that showed a
higher DCR in methylated MGMT patients (75%) than in unmethylated
MGMT patients (34,6%) without statistical difference in terms of
PFS-6 and OS between the two groups. Moreover, Brandes et al
reported a significantly higher PFS-6 in patients who started FTM
≥3 months after TMZ completion than in those who started FTM within
3 months.
FTM standard regimen showed to be efficacy in
recurrent MGs but was limited by considerable myelotoxicity,
especially thrombocytopenia and leukopenia, with grade 3–4 adverse
events in nearly 40% of patients. For this reason, subsequent phase
II trials studied alternative FTM schedules in order to improve the
safety profile of FTM second-line therapy.
In 2009 Fabi et al (22) analysed the activity of different
doses of FTM, ranging from 65 to 100 mg/mq, as second- or
third-line therapy in 40 MGs patients. The survival data were
comparable to those of the conventional schedule, but with grade
3–4 haematological toxicities (40% of patients) occurred only in
the group with the highest FTM dosage. Fabi et al. confirmed that
methylated MGMT patients went better than unmethylated MGMT
patients in terms of PFS, OS and DCR, although this did not reach
statistical significance.
In another prospective study (6), the same authors confirmed that lower
doses of FTM (60 mg/mq for the induction phase and 75 mg/mq for the
maintenance phase) had the same activity of the full dose regimen
but with a significantly lower rate of severe myelotoxicity
(27.5%).
To explain the wide range of PFS-6 reported by these
phase II trials (Table V), in 2012
Paccapelo et al (23)
investigated different response pattern to FTM in correlation to
the end of radiotherapy or predictive risk factors. They confirm
that a longer time to progression after radiotherapy and surgery at
recurrence are associated with a higher PFS-6 and DCR.
In 2011 Addeo et al (16) planned a new FTM schedule that
maintains the global dosage but with different fractionation. Forty
recurrent GBM patients received 80 mg/mq every 2 weeks for five
consecutive administrations (induction phase) and then every 4
weeks at 80 mg/mq as maintenance, after a 4-week rest period.
Efficacy data were similar to those of the conventional FTM
schedule (mPFS of 6.7 months, PFS-6 of 61% and mOS of 11.1 months),
but with a better DCR (65%) and a lower rate of grade 3–4
myelotoxicity in the induction and maintenance phase (12,50% and
17,70% respectively). They found also a trend toward prolonged
PFS-6, without statistical relevance, and a higher DCR in
methylated MGMT patients.
Only one prospective trial, performed by Gaviani
et al (24), studied the
Addeo FTM schedule at first or second recurrence. Survival data
were quite comparable to other studies on standard FTM schedule
(mPFS of 16 weeks with a 6-PFS of 38.2 % and mOS of 30 weeks). The
myelotoxicity profile was similar to that one of Addeo et al
with a low rate of grade 3–4 thrombocytopenia and leukopenia (0.3 %
each), but with a higher rate of grade 3–4 lymphopenia (18.5
%).
In the present retrospective study, we analysed the
efficacy and safety profile of fractionated FTM schedule proposed
by Addeo et al as second-line therapy in 40 recurrent MGs
patients. Survival analysis showed DCR of 60%, mPFS of 4 months
with PFS-6 of 33% and mOS of 9 months with OS-6 of 55%. These
results are comparable to those reported by all the other trials on
FTM, as reported in Table V. As
concern Scoccianti, Fabrini and Addeo results, the favourable
survival data, especially PFS, could be, in part, due to the
inclusion in the study of patients with pseudoprogression rather
than disease recurrence, with an overestimate of the results
(6,9,16).
Pseudoprogression, a treatment-related reaction which mimics tumour
progression, occurs mainly within 3 months after concurrent
radio-chemotherapy with TMZ and correlates with favourable
prognosis and higher response rate to FTM (25,26).
Differently from Brandes et al (15), Fabi et al (6,22) and
Addeo et al (16) we observed
a statistical significance in terms of survival outcomes between
methylated and unmethylated MGMT patients. The MGMT methylation
status is prognostic at the time of diagnosis (27) but also in recurrent GBM as reported
by the DIRECTOR and the BELOB trials (28,29). The
AVAREG trial (30) demonstrated also
that MGMT methylation status was predictive of efficacy of FTM in
the recurrence setting.
Subgroup analysis according to resurgery and
reirradiation before FTM second-line treatment were performed since
the evaluation of different treatment options and of their
combinations is of high interest (31,32) in
order to improve local control of the disease and survival
outcomes. Unfortunately, we didn't observe a survival benefit with
resurgery probably due to the low number of patients, while data on
reirradiation were more promising. Recent literature reviews and
several retrospective studies showed a survival benefit with
resurgery and reirradiation at the time of recurrence, with higher
survival in selected patients with favourable clinical and
radiological characteristics (17,18).
Our results on grade 3–4 myelotoxicity (15%) are
comparable to those reported by Addeo et al and Gaviani
et al (16,24). Lower toxicity permits to preserve
quality of life (QoL), which is an essential aim for MGs patients
who can only be palliated (16). In
fact, it is important to notice the high percentage of patients
still fit for third (28%) and fourth (7%) line therapy after FTM
failure (Table I).
Even if this is a retrospective analysis with a
limited number of patients, a heterogeneous population (including
primary and secondary GBM), our survival data are comparable to
those presented by Addeo et al (16) and other phase II trials on standard
schedule, with results which confirms that the fractionated FTM
schedule has a better safety profile than standard regimen
(Table V).
From our experience, despite it remains unclear if
the alternative schedule proposed by Addeo et al could be
more effective than the standard one, we registered a low toxicity
profile.
Considering these data, this fractionated FTM
schedule can be an efficient second-line therapy in the treatment
of such poor prognosis disease as it is MG, associated with less
myelotoxicity compared to the literature.
Future phase III randomised trial with a larger
number of patients and an adequate assessment of MGMT status at
diagnosis and recurrence are needed to define the role of MGMT
status in second-line therapy in MGs patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AP and SER contributed equally to this work and were
the major contributors in writing the manuscript, analysing and
interpreting the patient data. MG, MS, ADE, FB and CF were involved
in acquisition, analysis and interpretation of patient data. ST and
VB were involved in designing the study, writing the manuscript and
revising it critically for important intellectual content. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ostrom Q, Gittleman H, Farah P, Ondracek
A, Chen Y, Wolinsky Y, et al: CBTRUS statistical report: primary
brain and central nervous system tumors diagnosed in the United
States in 2006–2010. Neuro-Οncol. 15:ii1–ii56. 2013.
|
|
2
|
Stupp R, Brada M, van den Bent MJ, Tonn JC
and Pentheroudakis G: ESMO Guidelines Working Group: High-grade
glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment
and follow-up. Ann Oncol. 25 Suppl 3:iii93–iii101. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Louis DN, Ohgaki H, Wiestler OD, Cavenee
WK, Burger PC, Jouvet A, Scheithauer BW and Kleihues P: The 2007
WHO classification of tumours of the central nervous system. Acta
Neuropathol. 114:97–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stupp R, Mason WP, van den Bent MJ, Weller
M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn
U, et al: European Organisation for Research and Treatment of
Cancer Brain Tumor and Radiotherapy Groups; National Cancer
Institute of Canada Clinical Trials Group: Radiotherapy plus
concomitant and adjuvant temozolomide for glioblastoma. N Engl J
Med. 352:987–996. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Weller M, Cloughesy T, Perry JR and Wick
W: Standards of care for treatment of recurrent glioblastoma-are we
there yet? Neuro-oncol. 15:4–27. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fabi A, Metro G, Vidiri A, Lanzetta G,
Carosi M, Telera S, Maschio M, Russillo M, Sperduti I, Carapella
CM, et al: Low-dose fotemustine for recurrent malignant glioma: A
multicenter phase II study. J Neurooncol. 100:209–215. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tosoni A, Franceschi E, Poggi R and
Brandes AA: Relapsed Glioblastoma: Treatment Strategies for Initial
and Subsequent Recurrences. Curr Treat Options Oncol. 17:492016.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Beauchesne P: Fotemustine: A
third-generation nitrosourea for the treatment of recurrent
malignant gliomas. Cancers (Basel). 4:77–87. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Silvani A, Gaviani P, Lamperti E, Botturi
A, Ferrari D, Simonetti G and Salmaggi A: Lecture: Fotemustine in
brain tumors. Neurol Sci. 32 Suppl 2:S255–S257. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lombardi G, Farina P, Della Puppa A,
Cecchin D, Pambuku A, Bellu L and Zagonel V: An overview of
fotemustine in high-grade gliomas: From single agent to association
with bevacizumab. BioMed Res Int. 2014:6985422014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kyritsis AP and Levin VA: An algorithm for
chemotherapy treatment of recurrent glioma patients after
temozolomide failure in the general oncology setting. Cancer
Chemother Pharmacol. 67:971–983. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Frenay M, Giroux B, Khoury S, Derlon JM
and Namer M: Phase II study of fotemustine in recurrent
supratentorial malignant gliomas. Eur J Cancer. 27:852–856. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Scoccianti S, Detti B, Sardaro A, Iannalfi
A, Meattini I, Leonulli BG, Borghesi S, Martinelli F, Bordi L,
Ammannati F, et al: Second-line chemotherapy with fotemustine in
temozolomide-pretreated patients with relapsing glioblastoma: A
single institution experience. Anticancer Drugs. 19:613–620. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fabrini MG, Silvano G, Lolli I, Perrone F,
Marsella A, Scotti V and Cionini L: A multi-institutional phase II
study on second-line Fotemustine chemotherapy in recurrent
glioblastoma. J Neurooncol. 92:79–86. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Brandes AA, Tosoni A, Franceschi E, Blatt
V, Santoro A, Faedi M, Amistà P, Gardiman M, Labianca R, Bianchini
C, et al: Fotemustine as second-line treatment for recurrent or
progressive glioblastoma after concomitant and/or adjuvant
temozolomide: A phase II trial of Gruppo Italiano Cooperativo di
Neuro-Oncologia (GICNO). Cancer Chemother Pharmacol. 64:769–775.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Addeo R, Caraglia M, De Santi MS, Montella
L, Abbruzzese A, Parlato C, Vincenzi B, Carraturo M, Faiola V,
Genovese M, et al: A new schedule of fotemustine in
temozolomide-pretreated patients with relapsing glioblastoma. J
Neurooncol. 102:417–424. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Montemurro N, Perrini P, Blanco MO and
Vannozzi R: Second surgery for recurrent glioblastoma: A concise
overview of the current literature. Clin Neurol Neurosurg.
142:60–64. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sulman EP, Ismaila N, Armstrong TS, Tsien
C, Batchelor TT, Cloughesy T, Galanis E, Gilbert M, Gondi V, Lovely
M, et al: Radiation Therapy for Glioblastoma: American Society of
Clinical Oncology Clinical Practice Guideline Endorsement of the
American Society for Radiation Oncology Guideline. J Clin Oncol.
35:361–369. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wen PY, Macdonald DR, Reardon DA,
Cloughesy TF, Sorensen AG, Galanis E, Degroot J, Wick W, Gilbert
MR, Lassman AB, et al: Updated response assessment criteria for
high-grade gliomas: Response assessment in neuro-oncology working
group. J Clin Oncol. 28:1963–1972. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Common Terminology Criteria for Adverse
Events v4.03 (CTCAE). http://ctep.cancer.govAugust 10–2017
|
|
21
|
Kaplan E and Meier P: Nonparametric
estimation from incomplete observations. J Am Stat Assoc.
53:457–481. 1958. View Article : Google Scholar
|
|
22
|
Fabi A, Metro G, Russillo M, Vidiri A,
Carapella CM, Maschio M, Cognetti F, Jandolo B, Mirri MA, Sperduti
I, et al: Treatment of recurrent malignant gliomas with fotemustine
monotherapy: Impact of dose and correlation with MGMT promoter
methylation. BMC Cancer. 9:1012009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Paccapelo A, Lolli I, Fabrini MG, Silvano
G, Detti B, Perrone F, Savio G, Santoni M, Bonizzoni E, Perrone T,
et al: A retrospective pooled analysis of response patterns and
risk factors in recurrent malignant glioma patients receiving a
nitrosourea-based chemotherapy. J Transl Med. 10:902012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gaviani P, Simonetti G, Salmaggi A,
Lamperti E and Silvani A: Safety of second-line chemotherapy with
non-conventional fotemustine schedule in recurrent high grade
gliomas: A single institution experience. J Neurooncol.
113:527–529. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Brandes AA, Franceschi E, Tosoni A, Blatt
V, Pession A, Tallini G, Bertorelle R, Bartolini S, Calbucci F,
Andreoli A, et al: MGMT promoter methylation status can predict the
incidence and outcome of pseudoprogression after concomitant
radiochemotherapy in newly diagnosed glioblastoma patients. J Clin
Oncol. 26:2192–2197. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Taal W, Brandsma D, de Bruin HG, Bromberg
JE, Swaak-Kragten AT, Smitt PA, van Es CA and van den Bent MJ:
Incidence of early pseudo-progression in a cohort of malignant
glioma patients treated with chemoirradiation with temozolomide.
Cancer. 113:405–410. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hegi ME, Diserens AC, Gorlia T, Hamou MF,
de Tribolet N, Weller M, Kros JM, Hainfellner JA, Mason W, Mariani
L, et al: MGMT gene silencing and benefit from temozolomide in
glioblastoma. N Engl J Med. 352:997–1003. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Weller M, Tabatabai G, Kästner B, Felsberg
J, Steinbach JP, Wick A, Schnell O, Hau P, Herrlinger U, Sabel MC,
et al: DIRECTOR Study Group: MGMT promoter methylation is a strong
prognostic biomarker for benefit from dose-intensified temozolomide
rechallenge in progressive glioblastoma: The DIRECTOR Trial. Clin
Cancer Res. 21:2057–2064. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Taal W, Oosterkamp HM, Walenkamp AM,
Dubbink HJ, Beerepoot LV, Hanse MC, Buter J, Honkoop AH, Boerman D,
de Vos FY, et al: Single-agent bevacizumab or lomustine versus a
combination of bevacizumab plus lomustine in patients with
recurrent glioblastoma (BELOB trial): A randomised controlled phase
2 trial. Lancet Oncol. 15:943–953. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Brandes AA, Finocchiaro G, Zagonel V, Reni
M, Caserta C, Fabi A, Clavarezza M, Maiello E, Eoli M, Lombardi G,
et al: AVAREG: A phase II, randomized, noncomparative study of
fotemustine or bevacizumab for patients with recurrent
glioblastoma. Neuro-oncol. 18:1304–1312. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Azoulay M, Santos F, Shenouda G, Petrecca
K, Oweida A, Guiot MC, Owen S, Panet-Raymond V, Souhami L and
Abdulkarim BS: Benefit of re-operation and salvage therapies for
recurrent glioblastoma multiforme: Results from a single
institution. J Neurooncol. 132:419–426. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Seystahl K, Wick W and Weller M:
Therapeutic options in recurrent glioblastoma-An update. Crit Rev
Oncol Hematol. 99:389–408. 2016. View Article : Google Scholar : PubMed/NCBI
|