Introduction
Non-small cell lung cancer (NSCLC) represents the
most common type of malignancy and the leading cause of
cancer-associated mortality worldwide (1,2).
Platinum doublet chemotherapy, alone or in combination with
radiation therapy, is the standard frontline treatment for patients
with advanced disease (stages IIIB-IV), with a good performance
status [Eastern Cooperative Oncology Group (ECOG) 0–1], no
actionable mutations/rearrangements/translocations in epidermal
growth factor receptor (EGFR; 8–10% of cases), anaplastic lymphoma
kinase [ALK]/echinoderm microtubule-associated protein-like [EML]
(3–4%) requiring specific drugs or over-expression (>50%) of the
programmed cell death receptor ligand-1 (PDL-1; 15–20%), which
allows the use of specific programmed cell death-receptor-1 (PD-1)
blockade with Pembrolizumab (3–6).
Furthermore, the addition of Bevacizumab, a monoclonal antibody
(mAb) to the vascular endothelial growth factor (VEGF), to the
platinum doublet is also recommended in patients with non-squamous
histology and a low risk of bleeding (7). Taken together, these treatments are
associated to a median progression-free survival (PFS) and overall
survival (OS) of 7–8 and 12–13 months, respectively (3–7).
Immune-checkpoint blockade with mAbs to PD-1 (Nivolumab and
Pembrolizumab) or PDL-1 (Atezolizumab) have been approved for the
salvage treatment of these patients with promising results in terms
of the benefits and survival, and is progressing towards successful
approval as a first line treatment in selected cases (8–10).
Nivolumab, in particular, is a fully human
immunoglobulin-G4 mAb to PD-1 and is presently recommended for the
treatment of malignant melanoma, kidney cancer, urothelial cancer,
head and neck cancer, and metastatic NSCLC (mNSCLC) (8–11).
Although its use may yield a significant benefit and a prolonged
survival in ~20% of patients with mNSCLC, this treatment may be
hampered by severe autoimmune adverse events, such as
immune-related adverse events (irAEs), and high economic costs
(12). At present, patients are
administered PD-1/PDL-1 blockade treatment on an empirical basis,
as no reliable response biomarkers that are able to guide the
patients' selection have been identified, with the exception of the
immune-histochemical expression of PDL-1 being >50% for first
line Pembrolizumab (15–25% of cases) or a high tumor mutation
burden for Nivolumab that occurs in <5% of the cases and
requires advanced technological approaches that cannot be utilized
worldwide yet (12–14).
In order to identify reliable biomarkers for patient
response to Nivolumab, the present study took into consideration
the hypothesis that the PD-1/PDL-1axis is a peripheral mechanism of
T cell inhibition and that its blockade triggers a fast cytolytic
effect in the tumor tissue, throughout the rescue of immune-check
point deactivated tumor infiltrating cytotoxic T cells (CTLs). The
presence of these immune-effectors represents an immunological
response to the tumor associated antigens (TAAs) and tumor specific
antigens (TSAs) produced by transformed cells as a natural
consequence of their carcinogenetic process, which pre-exists the
use of the immune-checkpoint blocker mAbs (15,16). In
this context, the PD-1/PDL-1 blockade and the consequent CTL rescue
give rise to a fast T cell-mediated cytolytic response in tumor
sites that will be rapidly terminated if there is not a continuous
self-sustained and prolonged supply of new active tumor-specific
immune-effectors from central lymphoid organs (17). Experimental evidence has suggested
that the latter process defined as immune-priming, may be critical
for patient survival as it is required to avoid the exhaustion of
the most specific and active CTL clones in the tumor, and to
prevent an adaptive response by the tumor targets (17). On the other hand, the generation of
new immune-effectors does not occur in the tumor, but rather in
central lymphoid organs for the cross-presentation (immune-priming)
of antigenic material released in the blood stream and lymphatic
vessels by tumor tissues. Tumor-derived antigens are then taken up
and processed by professional antigen presenting cells such as,
dendritic cells (DCs) and activated B cells, and cleaved in small
major histocompatibility complex (MHC) haplotype specific epitope
peptides that are subsequently exposed on their membrane for T cell
precursor recognition and activation (18).
A number of studies have shown that the efficacy of
immune-effectors and antigen cross-priming may be supported by
specific anticancer treatments (including radiotherapy,
chemotherapy, steroid hormones, and immune-adjuvant agents), the
hypoxic response and/or tumor associated inflammation (19–27).
Tumor irradiation, several anticancer drugs, as well as specific
anti-angiogenic treatments (metronomic chemotherapy, bevacizumab
and multi-kinase inhibitors) may, in fact, induce immunogenic cell
death, antigen modulation and release in the tumor tissues, and may
also interfere with the activity of many different
immunosuppressive cell lineages, such as myeloid derivative
suppressor cells and regulatory T cells (Treg) (19–27). In
this regard, several immunotherapy studies in mouse models and
cancer patients have demonstrated that host survival upon treatment
with cancer vaccines, immunologic treatments as well as
radiotherapy (abscopal effect) was correlated with the ability of
the experimental treatment to trigger an immunological antigen
cascade and promote immune-priming to TAAs and TSAs (19–26) with
amplified multi-antigen specific immune-responses. This effect has
been recognized as a direct consequence of the treatment that was
able to trigger the release of neo-antigens, producing powerful
immunological danger signals (such as Calreticuline, Heath-shock
proteins and damage-associated molecular patterns) that are able to
alert the immune-surveillance system to a prompt an adequate
response (19–26). The activation of an antigen cascade
is therefore responsible for the appearance of multiple and more
active tumor specific CTL precursors, TAA-specific antibodies and
autoimmunity, and in turn, auto-antibodies (AAbs) such as those
detected in patients with common autoimmune diseases (28–37).
Thus the present study performed retrospective analysis to
investigate the ability of several clinical, immune-biological
parameters that reflect the aforementioned considerations, in order
to predict the survival of patients with mNSCLC who received
salvage treatment with Nivolumab.
Materials and methods
Patient sample, treatment and
monitoring
The present multi-institutional retrospective
analysis included a database of 120 mNSCLC patients who were
sequentially enrolled to receive salvage biweekly therapy with
Nivolumab at the Medical Oncology Unit, Grand Metropolitan Hospital
in Reggio Calabria, at the Radiation Oncology Unit, Siena
University Hospital, and at the Medical and Translational Oncology
Units, at AOU ‘Mater Domini-Magna Graecia’ University Hospital of
Catanzaro, Italy, between September 2015 and June 2018. The present
study was performed using a representative group of 92 cases
(76.7%), who had been screened for AAb detection and
immune-biological analysis as well as treatment. Due to the
retrospective nature of the study, the AAb assays could not be
evaluated in 28 patients, as their serum was not available at
baseline. These patients were consequently excluded from the
statistical analysis; this did not influence the results of the
statistical analysis, as it was completely casual. All of the
enrolled patients received intravenous Nivolumab at a dosage of 3
mg/kg in 60 min on a biweekly basis. The treatment was continued
until clear progression, unacceptable toxicity or mortality. These
patients, prior to PD-1 blockade, had received at least 1 previous
line of platinum-based doublet +/− bevacizumab, presented a
performance status <2, complete physical examination reports,
histological samplings, and hematological, biochemical,
immune-biological, imaging and instrumental monitoring.
Clinical history and physical examinations with
recordings of adverse events were assessed every 2 weeks according
to the best clinical practice. A computed tomography-scan was
performed every 3 months or in any case showing clinical signs of
Progressive Disease or an increase in any specific tumor marker,
and evaluated according to the iRECIST Criteria (37).
Patients were monitored for blood cell counts,
biochemistry, inflammatory markers [including C Reactive Protein
(CRP), Erythrocyte-Sedimentation Ratio (ESR) and Lactate
Dehydrogenase (LDH)] at baseline and prior to each treatment
course. Detection assays for serum AAbs such as, anti-nuclear
antigens (ANAs), extractable nuclear antigens (ENAs), anti-smooth
cell antigens (ASMAs), anti-neutrophil cell antigen (c-ANCA and
p-ANCA), anti-thyreoglobulin and anti-thyreo-peroxidases
antibodies, were performed at baseline and every 4 weeks since the
beginning of the treatment as described previously (38,39).
Patients were also monitored for FT3, FT4, thyroid stimulating
hormone, adreno-corticotropic hormone (ACTH) and aldosterone blood
levels on a monthly basis from the start of Nivolumab
treatment.
An immuno-cytofluorometric analysis was also
performed using the peripheral blood mononuclear cells of 40
patients enrolled in the Units of Siena and Catanzaro with the aim
to evaluate the possible treatment-associated changes in the
percentage of Treg
(CD3+CD4+CD25+FoxP3+),
central memory T cells (TCM;
CD3+CD8+CD45RA−CCR7+),
effector memory T cells (TEM;
CD3+CD8+CD45RA−CCR7−),
and natural killer (NK) subsets
(CD3−CD16+CD56Dim) as described in
our previous works (38–40).
Ethical consideration
All patients gave written consent for the anonymous
use of their examinations for research. The retrospective analysis
of the data was approved by the University Hospital of Siena
Institutional Review Board. All procedures were undertaken in
compliance with the ethical statements of the Helsinki Declaration
(1964, amended most recently in 2008) of the World Medical
Association. The Patients' Database is available on request, in
accordance with Italian Law on the protection of personal data.
Statistical analysis
Data were expressed as the mean ± standard deviation
(normally distributed data), median and inter-quartile range (IQR;
non-normally distributed data) or as per cent frequency
(categorical data). Comparisons among groups were conducted using
U-Mann Whitney test. Survival analyses were performed using
Kaplan-Meier curves and univariate Cox regression analyses. The
study outcomes were PFS and OS. The Cox analyses data were
expressed as the hazard ratio (HR), 95% Confidence interval (CI)
and P-value. Statistical analysis was performed using SPSS for
Windows software (Version 24; IBM, Corp., Armonk, NY, USA) and
STATA for Windows software (Version 13; StataCorp LP, College
Station, TX, USA).
Results
Patient features
The present cohort of 92 patients included 75 males
and 17 females, with an average age of 66 years and a median follow
up of 9 months. Squamous cell carcinoma was diagnosed in 31 cases,
adenocarcinoma in 55 and undefined histology (NOS) in 6 patients.
Prior to Nivolumab treatment, 51 patients had received a standard
doublet chemotherapy line (either carboplatin + paclitaxel or
carboplatin/cisplatin + gemcitabine or cisplatin + pemetrexed); and
41 received fractioned cisplatin (30 mg/m2 days 1-3q21)
and metronomic oral etoposide (50 mg days 1-15q21) according to the
mPE regimen alone (17 patients), or in combination (24 patients)
with bevacizumab (5 mg/kg day 3q21; mPEBev) (39–43).
Overall, the latter 41 patients, treated in the Siena and
Reggio-Calabria Units, received frontline treatment with a
non-canonic, innovative metronomic chemotherapy, which has
previously shown powerful antitumor activity and a significant
immunomodulating effect (39–43).
Patients receiving the frontline mPE/mPEBev regimen
(41 patients) and those who received more canonic frontline
platinum doublet (51 patients) presented similar features in terms
of the following: Performance status (ECOG 0 vs. ECOG
<2=mPE/mPEBev regimen: 21 vs. 20 patients; platinum doublets: 38
vs. 13 patients), sex (males vs. female=mPE/mPEBev regimen: 32 vs.
9 patients; platinum doublets: 43 vs. 8 patients) and histology
(Squamous vs. adenocarcinoma + NOS= mPE/mPEBev regimen 15 vs. 26
patients; platinum doublets: 22 vs. 29 patients).
Overall, 40 patients received >1 treatment line
and 22 additional treatments of TKI (Erlotinib) even in the absence
of driving EGFR mutation. Finally, palliative radiotherapy (25–30
Gy either hypo-fractionated in 1 day or fractionated in 5 days) on
symptomatic single lesions (parenchymal, lymph-nodes, soft tissue,
bone or brain) was administered in 48 patients prior to
nivolumab.
Predictive values of clinical
parameters
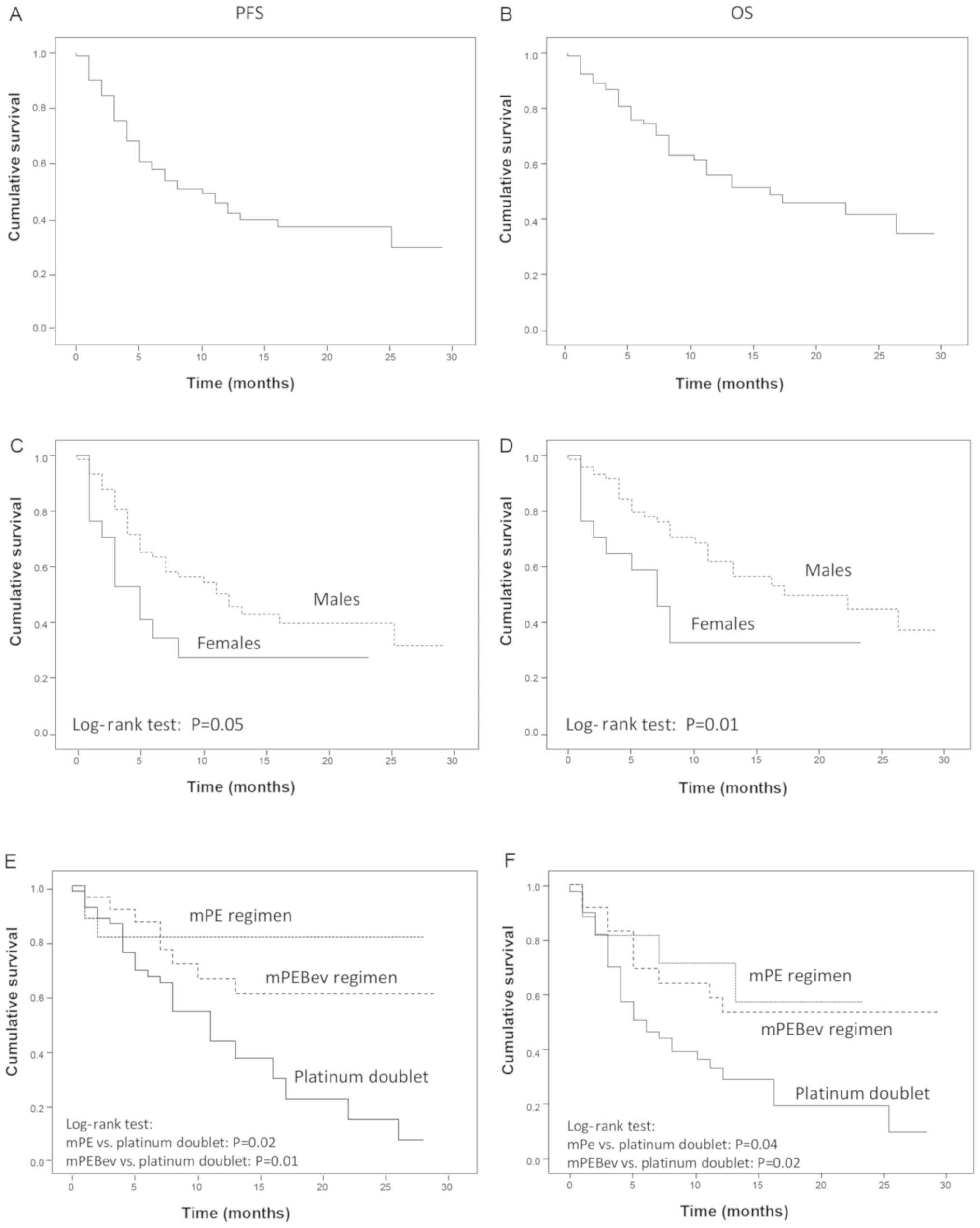
The median PFS and OS were 10.0 [IQR: 5.8–14.2] and
16.0 [IQR: 6.2–25.8] months, respectively (Fig. 1A and B). As previously reported in
the literature, the mortality rate was higher in females than in
males [HR: 2.29 (95%CI: 1.13–4.62), P=0.01], and a similar trend
was observed for PFS [HR: 1.87 (95%CI: 0.97–3.60), P=0.05]
(Fig. 1C and D). These results were
not correlated with smoking habits, as 14 out of 17 were smokers.
Nivolumab administration was well tolerated and the occurrence of
grade 1–2 irAEs was recorded in 43 out of 92 (47.8%) patients.
These mainly consisted of cutaneous rush, poly-arthritis and
thyroiditis, generally occurring concomitantly following 6–8
treatment courses. A more severe autoimmune pneumonitis was
recorded in 3 cases following 6–7 treatment courses, and uveitis
was recorded in 2 patients following 5 and 6 treatment courses.
Hypophysitis and adrenal gland damage were not demonstrated even
though asymptomatic concomitant decline in ACTH and aldosterone
serum levels were recorded in 4 patients following 6–8 treatment
courses.
Treatment response and
autoimmunity
The present study was unable to identify a
correlation among PFS and OS, and age, smoking habitude, histology,
number of previous chemotherapy lines, TKI or radiotherapy (data
not shown). On the other hand, the results revealed a significant
advantage in PFS and OS in the group of patients who had received
metronomic chemotherapy according to the mPE regimen [PFS: HR=0.40
(95% CI: 0.16–1.03) P=0.02; OS: HR=0.29 (95% CI: 0.09–0.95),
P=0.04] or metronomic chemotherapy and bevacizumab [mPEBev regimen;
PFS: HR=0.44 (95% CI: 0.22–0.91), P=0.01; OS: HR=0.40 (95% CI:
0.18–0.88), P=0.02] (Fig. 1E and F);
compared with the group of patients who received a standard
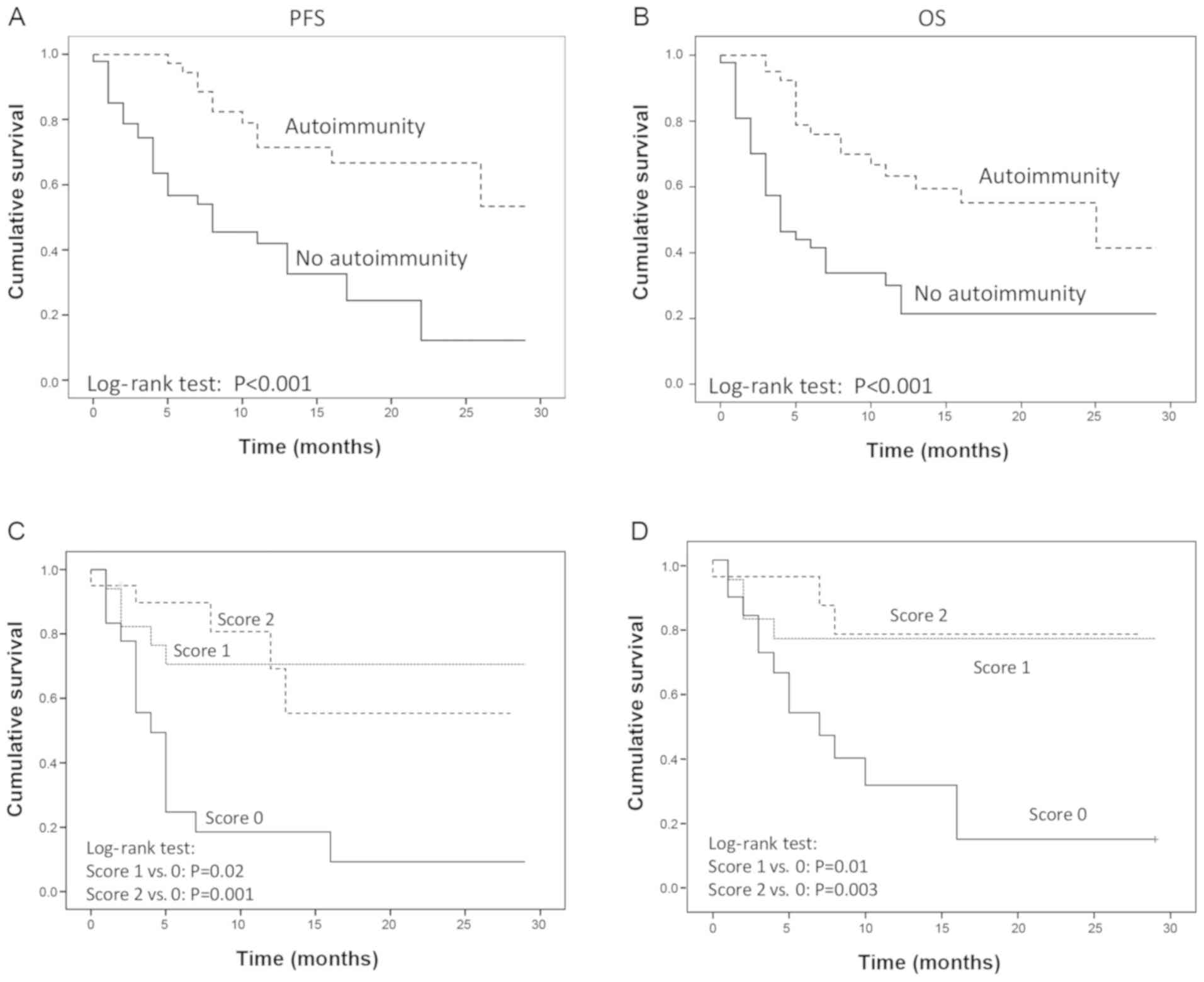
platinum doublet. A prolonged PFS and OS was finally recorded in
patients who manifested irAEs [PFS: HR=0.31 (95% CI, 0.17–0.58)
P<0.001; OS: HR=0.26 (95% CI: 0.13–0.53), P<0.001; (Fig. 2A and B).
Immune-biological markers
Monitoring Nivolumab treatment did not reveal
significant changes in the blood cell counts of neutrophils,
monocytes, lymphocytes, or the neutrophil to lymphocyte ratio
(NLR). Similarly, no statistically significant treatment-associated
changes were detected for inflammatory markers such as CRP, ESR or
LDH. In addition, the peripheral lymphocyte subsets
CD3+CD8+ [23.1% (+/−9.5) vs. 26.7% (+/−14.8),
P=0.58)], CD3+CD4+PD-1+ [5.77%
(+/−2.72) vs. 8.25% (+/−6.88), P=0.169], Tcm [2%
(+/−1.85) vs. 3.41% (+/−4.03), P=0.32], Tem [4.03%
(+/−2.39) vs. 5.01% (+/−3.25), P=0.39],
CD3+CD4+ [50.7% (+/−11.09) vs. 42% (+/−14.9),
P=0.0163], Treg [2.8% (+/−1.93) vs. 1.87% (+/−1.11);
P=0.088] or NKs [7.66 (+/−3.62) vs. 7.19 (+/−4.99), P=0.75] did not
show any significant treatment-associated changes following 3
treatment courses. However, a significant increase in the
eosinophil cell counts was recorded, exhibiting a rapid and
significant increase with treatment [baseline value vs. value after
3 treatment courses: 0.095 (+/−0.013) vs. 0.140 (+/− 0.018)
103 cells/mm3, P=0.0014].
The present study then evaluated the patients'
serum-conversion of AAbs (ANA, ENA, ANCA, p-ANCA and c-ANCA), which
are commonly associated with frequently occurring auto-immune
diseases. Within 30 days since the beginning of the treatment 18
patients (25.7%) became positive (Serum titration >1/160) for
the expression of 1 of these (15 ANA and 3 ENA; scored as 1), while
a further 22 (31.4%) became contemporary positive for the
expression of 2 or 3 of these (ANA, ENA and ASMA; scored as 2).
Overall, there was a statistically significant increase in serum
ANA (baseline vs. third treatment course: 0.37 vs. 1.13 title
score; P=0.00028) and ASMA (baseline vs. third treatment course:
0.076 vs. 0.41 title score; P=0.0094). Only 3 patients exhibited a
significant increase in c-ANCA and p-ANCA levels following 12
months of treatment, and were not clustered with ANA, ENA and ASMA
nor were they associated with clinical evidence of more severe
irAEs (grade 3).
Statistical correlation
The present analysis demonstrated that either PFS or
OS were directly correlated with the early (within 30 days)
serum-conversion for one (score 1) or more (score 2) AAbs among
ANA, ENA, ASMA [PFS: score 1 vs. score 0: HR=0.23 (95% CI:
0.08–0.65), P=0.006; score 2 vs. score 0: HR=0.23 (95% CI:
0.08–0.62), P=0.004; OS: score 1 vs. score 0: HR=0.28 (95% CI:
0.09–0.88), P=0.03; score 2 vs. score 0: HR=0.19 (95% CI:
0.05–0.68), P=0.01]; (Fig. 2C and
D).
Cox regression analysis revealed a direct
association between the risk of progression and death with the
baseline values of neutrophil and lymphocyte cell counts, ESR and
LDH (Table I). Both the risk of
progression and death were correlated with treatment-associated
changes (Delta value) in neutrophil counts and NLR (where the Delta
value=value detected following 3 treatment courses-the value
detected at baseline). Conversely, PFS and OS were not correlated
with changes in CRP, ESR and LDH, or changes in the aforementioned
lymphocyte subsets (data not shown). Taken together, these results
suggest that a chronic inflammation status may negatively affect
the treatment response to Nivolumab. Conversely, the present
analysis also revealed an inverse correlation between the risk of
progression and death and treatment-associated changes (Delta
value) with eosinophil and lymphocyte cell count changes (Table II).
 | Table I.Cox regression analysis indicated a
direct association between the risk of progression and fatality
with baseline values of neutrophil and lymphocyte counts, ESR and
LDH. |
Table I.
Cox regression analysis indicated a
direct association between the risk of progression and fatality
with baseline values of neutrophil and lymphocyte counts, ESR and
LDH.
|
| PFS | OS |
|---|
|
|
|
|
|---|
| Variables at
baseline (units) | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Neutrophil cell
counts (103/mm3) | 1.13
(1.01–1.26) | 0.04 | 1.14
(1.003–1.29) | 0.04 |
| Lymphocytes cell
count (103/mm3) | 1.14
(0.98–1.31) | 0.08 | 1.19
(1.02–1.40) | 0.03 |
| ESR (mm/h) | 1.03
(1.01–1.04) | 0.002 | 1.04
(1.02–1.06) | 0.001 |
| LDH (20 U/l) | 1.04
(1.02–1.06) | <0.001 | 1.04
(1.01–1.06) | 0.001 |
| Table II.Cox regression analysis indicated a
direct association between the risk of progression and fatality
with changes (Delta of values at three treatment courses vs.
baseline) in neutrophil counts and NLR, and an inverse correlation
of the risk of both outcomes with changes in eosinophil and
lymphocyte counts. |
Table II.
Cox regression analysis indicated a
direct association between the risk of progression and fatality
with changes (Delta of values at three treatment courses vs.
baseline) in neutrophil counts and NLR, and an inverse correlation
of the risk of both outcomes with changes in eosinophil and
lymphocyte counts.
|
| PFS | OS |
|---|
|
|
|
|
|---|
| Variables at the
third treatment course (units) | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Neutrophil cell
counts (103/mm3) | 1.13
(1.03–1.24) | 0.009 | 1.16
(1.04–1.29) | 0.007 |
| Lymphocytes cell
count (103/mm3) | 0.79
(0.63–1.00) | 0.05 | 0.71
(0.55–0.91) | 0.007 |
| Eosinophil cell
counts (103/mm3) | 0.008
(0.00–0.23) | 0.005 | 0.03
(0.001–0.771) | 0.04 |
| NLR | 1.19
(1.06–1.34) | 0.005 | 1.27
(1.10–1.46) | 0.001 |
Comparative analyses
Patients who exhibited irAEs, when compared with the
other patients, had lower baseline levels of monocyte cell counts
[0.57 103/mm3 (IQR 0.41–0.68 vs. 0.73
103/mm3 (IQR 0.57–0.87), P=0.006], CRP [3.07
mg/dl (IQR 1.64–10.44 vs. 11.49 mg/dl (IQR 3.15–36.25), P=0.007]
and LDH [376 U/l (IQR 232–431 vs. 472 U/l (IQR 288–704), P=0.024].
Patients who exhibited irAEs also had a significant
treatment-associated increase in the number of lymphocytes [Δ: 0.19
103/mm3 (IQR −0.14–0.50) vs. −0.12
103/mm3 (IQR −0.42–0.16), P=0.037] and
monocytes [Δ: 0.07 103/mm3 (IQR −0.10 - 0.19)
vs. −0.11 103/mm3 (IQR −0.29–0.08), P=0.031]
in comparison with the other patients. By contrast, higher baseline
NLRs were correlated with a lower frequency of irAEs [Δ: −0.36 (IQR
−1.59–0.68) vs. 0.20 (IQR −0.86–2.32), P=0.009], and a rise in
AAbs.
A Chi square test finally revealed that the
frequency of irAEs was correlated with both AAbs' serum conversion
(P=0.002) and the type of therapy received prior to Nivolumab
administration. Finally, the present analysis also revealed a
greater frequency of irAEs in patients who had received metronomic
+/− bevacizumab when compared with those who had received standard
chemotherapy doublet prior nivolumab [69.04% vs. 34.6%;
P=0.007].
Discussion
The recent development of the PD-1/PDL-1 blockade
with the newest mAbs represents an extraordinary challenge in term
of costs, adverse events and patient monitoring. In this context,
the identification of biomarkers that can predict the response of
the patients' treatment selection appears to be of critical value
and is urgently required. In the present retrospective study, we
evaluated multiple clinical and immune-biological markers, that
were directly or indirectly correlated with both immune-priming and
effector phases of immune-response. The results revealed that the
male gender, the occurrence of irAEs, as well as the use of the
immune-modulating chemotherapy regimen, known as mPE +/−
bevacizumab, prior to nivolumab administration, were strongly
predictive of a positive outcome in terms of both PFS and OS. In
addition, patients who had received the mPE regimen +/− bevacizumab
prior to Nivolumab presented a greater risk of irAEs with the
immuno-oncological treatment. These results were not surprising,
considering that the mPE/mPEBev regimen had been designed on a
translational basis (BEVA2007 trial), in order to achieve a higher
dose intensity of both cisplatin and etoposide to induce
anti-angiogenetic effects and to the trigger immune-modulating
effects associated with VEGF and angiopoietin-2 decline (21,39–43). At
the end of the treatment, the BEVA2007 phase I–II trials, which
enrolled a cohort of 112 mNSCLC patients [39 of whom received the
mPE regimen and 73 were administered mPE in combination with
bevacizumab (mPEBev)] reported a median PFS and OS of 7 (95% CI:
6.17–7.82) and 15 (95% CI: 13.23–16.77) months, respectively
(39–43).
The immune-biological monitoring of these patients
demonstrated a treatment-associated induction of the cytotoxic
TH1 cytokine phenotype and with a treatment-associated
increase in activated myeloid derivative DCs, TCMs,
TEMs, activated CTLs
(CD3+CD8+CD62L+
andCD3+CD8+CD27+), and tumor
specific T cell precursors' frequency (39–43).
Further ancillary analysis of the BEVA2007 trial
revealed that the patients who had received palliative radiotherapy
in the course of the mPE/mPEBev treatment, presented the longest
survival and that this event was strictly correlated with the
treatment-associated rise in activated DC and Tcm
(39,44). The results of this study supported
the hypothesis of the immune-mediated effect of radiotherapy, which
was able to trigger efficient immune-priming coupled with the
production of immune-danger signals, becoming a powerful source of
new available antigens for an efficient immune-response, which was
subsequently supported by the immune-biological effects of the
cytotoxic regimen (19,32).
In line with the literature, the present study
reported that the PD-1/PDL-1 immune-checkpoint blockade, similarly
to other anti-cancer immunological treatments, was associated with
the occurrence of more or less severe irAEs and that this event in
turn, was predictive of prolonged survival (29–31,45–47).
This phenomenon, consequential to the occurrence of an
immune-primed antigen cascade and antigen migration, has been
recorded in other immunotherapy-(Gvax, Ipilimumab +/− gp100, TSPP
vaccine) (48,49) and chemo-immunotherapy models (mPEBev,
GOLFIG1 and 2 trials) (31,39,40,50–52) and
represents the basic concept of the radiotherapy-induced abscopal
effects and is strongly predictive of positive outcome (33). The occurrence of irAEs (such as
thyroiditis, polyarthritis and hypophysitis) in patients treated
with Nivolumab is an unpredictable event in terms of sites and
timing. It may be very difficult to identify at its early stage,
and is often complicated by confounding co-morbidities and
symptoms. Thus, it cannot be considered as a predictive biomarker
of response; however, in an attempt to target autoimmunity as a
potential biomarker of response, the present study evaluated the
serum of these patients, the levels of multiple AAbs currently
associated with the most common systemic auto-immune-diseases (ENA,
ANA and ASMA) and vasculitis (c-ANCA and p-ANCA), and monitored the
trend of inflammatory markers (CRP, ESR and LDH); the rise in these
markers has been detected in previous immunotherapy studies
performed by our group (31,39,49–53). An
early (15–30 days) serum-conversion of at least 1 of the 3AAbs
among ENA, ANA and ASMA, was recorded in 57% of the patients, an
event that was highly predictive of a better outcome and occurrence
of subsequent autoimmunity. It was also demonstrated that the rise
in AAbs was clustered with previous mPE/mPEBev treatment, a lower
NLR value at baseline and a low inflammatory level at the baseline,
while it was directly correlated with treatment-associated
increases in eosinophil and lymphocyte counts. While the present
study was unable to demonstrate a significant correlation between
eosinophil cell count increase with both a higher frequency of
irAEs or rise in AAbs, a significant inverse correlation was
detected among increased NLR, irAEs and increased AAbs. The latter
of which, in particular, was in line with the results of Bagley
et al (54) who revealed that
a baseline NLR ≥5 was strongly predictive of poor outcomes in term
of PFS and OS in patients with NSCLC under treatment with PD-1
inhibitors.
The fast occurrence of AAbs in these patients upon
Nivolumab treatment supports the hypothesis that
nivolumab-reactivated CTLs may also trigger both the immune-priming
of new antigens (antigen migration) and a clear antigen cascade
process resulting in the occurrence of AAbs including ANA, ENA, and
ASMA. The immune-mediated damage of the tumor tissue, in fact may
give rise to the immune-priming of sequestered material recognized
as non-self that in turn gives rise to a humoral, as well as a cell
mediated response. This phenomenon explains the rapid occurrence of
Abs to nuclear antigens (ANA and ENA), smooth cells (ASMA) and the
thyroid (microsomal antigens), which in the long term have provided
clinical evidence of autoimmunity and are indirect signs of an
efficient immune-reaction. Similar results have also been achieved
in other immunotherapy trials that aimed to test Gvax in
gastro-enteric malignancies; ipilimumab +/− gp100 in malignant
melanoma, and the TSPP vaccine in colorectal cancer, whose
administration was associated to a treatment-associated
serum-conversion for anti-thyroid AAbs, NY-ESO-1 Abs, and
anti-neutrophil AAbs (c/p-ANCA) respectively, which was in turn
predictive of treatment response and longer survival (39,48,49,52,53).
To date, no clear biomarker has been able to select
patients who may benefit from treatment with Nivolumab in NSCLC.
PDL-1 expression in the tumor sites is not reliable for several
reasons including the dynamic expression on tumor-associated
inflammatory cells and the presence of other PD-1 ligands (54). Similarly, a predictive value has been
identified in DNA mismatch repair deficiency (MSI-high status) and
in a high tumor mutation burden (TMB), which is suggestive of a
greater number of potential neo-antigens and eventually, an
expanded multi-antigenic CTL response to the tumor. TMB in
particular, has been associated with a favorable response to
Nivolumab in NSCLC patients receiving this treatment as frontline
therapy. Nevertheless, next generation sequencing, which allows for
TMB analysis, cannot be considered as a common practice (14,55).
At the present, research on biomarkers has also
focused on the expression of MHC molecules on tumor cells and the
role of multiple immunosuppressive tumor infiltrating cell lineages
(such as macrophages, Tregs, MDSCs and
IDO+DCs) with controversial results in terms of their
validation as predictive biomarkers (56,57).
Concomitant use of Nivolumab or Pembrolizumab with platinum
doublets has also been investigated reporting a better outcome in
patients who had received the chemo-immuno-oncologic treatment as a
frontline therapy compared with those who received the same
chemotherapy alone and PD-1/PDL-1 blockade at the sign of
progression. The concomitant and or sequential use of these mAbs
with specific anticancer drugs, radiotherapy to induce immunogenic
cell death, as well as tumor specific active specific immunotherapy
(cancer vaccines), and other immune-checkpoint inhibitors is still
an argument to debate.
In conclusion, the present results indicate that the
early treatment-associated rise of serum AAbs ANA, ENA and ASMA,
may be a surrogate marker of autoimmunity and is strongly
predictive of patient response to Nivolumab in terms of PFS and
long term survival. Additionally, the present study suggested the
potential mechanisms that are able to trigger an antigen cascade
and enhance the cross-priming of neo-antigens, which may improve
the survival of these patients, thereby offering the rationale to
design perspective trials aiming to evaluate the predictive value
of these AAbs to select patients that may not require the addition
of other checkpoint inhibitor treatment or chemotherapy following a
course of Nivolumab alone. The present results also support the
additional investigation of the ability of the mPE/mPEBev regimen
to improve the therapeutic effects of the PD-1/PDL-1 blockade.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
RG, GDA, CB, RA and PC made substantial
contributions to conception and design. PDM, ACF, VB, NS and TDG
made substantial contributions in the acquisition of data. PP, VN,
MM, GC, GT, LP, PTas, PTag and PC made substantial contributions in
the analysis and interpretation of data. All authors contributed in
drafting the manuscript and gave final approval of the version to
be published.
Ethics approval and consent to
participate
All patients gave written consent for the anonymous
use of their data. The retrospective analysis of the data was
approved by the University Hospital of Siena Institutional Review
Board. All procedures were undertaken in compliance with the
ethical statements of the Helsinki Declaration (1964, amended most
recently in 2008) of the World Medical Association.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cetin K, Ettinger DS, Hei YJ and O'Malley
CD: Survival by histologic subtype in stage IV nonsmall cell lung
cancer based on data from the Surveillance, epidemiology and end
results program. Clin Epidemiol. 3:139–148. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pilkington G, Boland A, Brown T, Oyee J,
Bagust A and Dickson R: A systematic review of the clinical
effectiveness of first-line chemotherapy for adult patients with
locally advanced or metastatic non-small cell lung cancer. Thorax.
70:359–367. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Noh JM, Kim JM, Ahn YC, Pyo H, Kim B, Oh
D, Ju SG, Kim JS, Shin JS, Hong CS, et al: Effect of radiation
therapy techniques on outcome in N3-positive IIIB non-small cell
lung cancer treated with concurrent chemoradiotherapy. Cancer Res
Treat. 48:106–114. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bearz A, Berretta M and Tirelli U:
Clinical effectiveness and cost-effectiveness of target therapies
for adult patients with locally advanced or metastatic non-small
cell lung cancer: A systematic review. Curr Cancer Drug Targets.
18:405–409. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Horn L, Spigel DR, Vokes EE, Holgado E,
Ready N, Steins M, Poddubskaya E, Borghaei H, Felip E, Paz-Ares L,
et al: Nivolumab versus docetaxel in previously treated patients
with advanced non-small-cell lung cancer: Two-year outcomes from
two randomized, open-label, phase III trials (CheckMate 017 and
CheckMate 057). J Clin Oncol. 35:3924–3933. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Di Costanzo F, Mazzoni F, Micol Mela M,
Antonuzzo L, Checcacci D, Saggese M and Di Costanzo F: Bevacizumab
in non-small cell lung cancer. Drugs. 68:737–746. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Meyers DE, Bryan PM, Banerji S and Morris
DG: Targeting the PD-1/PD-L1 axis for the treatment of
non-small-cell lung cancer. Curr Oncol. 25:e324–e334. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Herzberg B, Campo MJ and Gainor JF: Immune
checkpoint inhibitors in non-small cell lung cancer. Oncologist.
22:81–88. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Alsaab HO, Sau S, Alzhrani R, Tatiparti K,
Bhise K, Kashaw SK and Iyer AK: PD-1 and PD-L1 checkpoint signaling
inhibition for cancer immunotherapy: Mechanism, combinations, and
clinical outcome. Front Pharmacol. 8:5612017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Brahmer JR, Govindan R, Anders RA, Antonia
SJ, Sagorsky S, Davies MJ, Dubinett SM, Ferris A, Gandhi L, Garon
EB, et al: The society for immunotherapy of cancer consensus
statement on immunotherapy for the treatment of non-small cell lung
cancer (NSCLC). J Immunother Cancer. 6:752018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Arriola E, Wheater M, Galea I, Cross N,
Maishman T, Hamid D, Stanton L, Cave J, Geldart T, Mulatero C, et
al: Outcome and biomarker analysis from a multicenter phase 2 study
of ipilimumab in combination with carboplatin and etoposide as
first-line therapy for extensive-stage SCLC. J Thorac Oncol.
11:1511–1521. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hellmann MD, Callahan MK, Awad MM, Calvo
E, Ascierto PA, Atmaca A, Rizvi NA, Hirsch FR, Selvaggi G,
Szustakowski JD, et al: Tumor mutational burden and efficacy of
nivolumab monotherapy and in combination with ipilimumab in
small-cell lung cancer. Cancer Cell. 33:853–861 e854. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang RF and Rosenberg SA: Human tumor
antigens for cancer vaccine development. Immunol Rev. 170:85–100.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cohen CJ, Gartner JJ, Horovitz-Fried M,
Shamalov K, Trebska-McGowan K, Bliskovsky VV, Parkhurst MR, Ankri
C, Prickett TD, Crystal JS, et al: Isolation of neoantigen-specific
T cells from tumor and peripheral lymphocytes. J Clin Invest.
125:3981–3991. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sanchez-Paulete AR, Teijeira A, Cueto FJ,
Garasa S, Pérez-Gracia JL, Sánchez-Arráez A, Sancho D and Melero I:
Antigen cross-presentation and T-cell cross-priming in cancer
immunology and immunotherapy. Ann Oncol. 28 (Suppl 12):xii44–xii55.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
McDonnell AM, Robinson BW and Currie AJ:
Tumor antigen cross-presentation and the dendritic cell: Where it
all begins? Clin Dev Immunol. 2010:5395192010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gebremeskel S and Johnston B: Concepts and
mechanisms underlying chemotherapy induced immunogenic cell death:
Impact on clinical studies and considerations for combined
therapies. Oncotarget. 6:41600–41619. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Patel RB, Baniel CC, Sriramaneni RN,
Bradley K, Markovina S and Morris ZS: Combining brachytherapy and
immunotherapy to achieve in situ tumor vaccination: A review of
cooperative mechanisms and clinical opportunities. Brachytherapy.
17:995–1003. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Botta C, Misso G, Martino EC, Pirtoli L,
Cusi MG, Tassone P, Tagliaferri P, Caraglia M and Correale P: The
route to solve the interplay between inflammation, angiogenesis and
anti-cancer immune response. Cell Death Dis. 7:e22992016.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang D and DuBois RN: Immunosuppression
associated with chronic inflammation in the tumor microenvironment.
Carcinogenesis. 36:1085–1093. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kanterman J, Sade-Feldman M and Baniyash
M: New insights into chronic inflammation-induced
immunosuppression. Semin Cancer Biol. 22:307–318. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wu J and Waxman DJ: Immunogenic
chemotherapy: Dose and schedule dependence and combination with
immunotherapy. Cancer Lett. 419:210–221. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shahabi V, Postow MA, Tuck D and Wolchok
JD: Immune-priming of the tumor microenvironment by radiotherapy:
Rationale for combination with immunotherapy to improve anticancer
efficacy. Am J Clin Oncol. 38:90–97. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Apetoh L, Ladoire S, Coukos G and
Ghiringhelli F: Combining immunotherapy and anticancer agents: The
right path to achieve cancer cure? Ann Oncol. 26:1813–1823. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nardone V, Pastina P, Giannicola R,
Agostino R, Croci S, Tini P, Pirtoli L, Giordano A, Tagliaferri P
and Correale P: How to increase the efficacy of immunotherapy in
NSCLC and HNSCC: Role of radiation therapy, chemotherapy, and other
strategies. Front Immunol. 9:29412018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Attia P, Phan GQ, Maker AV, Robinson MR,
Quezado MM, Yang JC, Sherry RM, Topalian SL, Kammula US, Royal RE,
et al: Autoimmunity correlates with tumor regression in patients
with metastatic melanoma treated with anti-cytotoxic T-lymphocyte
antigen-4. J Clin Oncol. 23:6043–6053. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Maker AV, Phan GQ, Attia P, Yang JC,
Sherry RM, Topalian SL, Kammula US, Royal RE, Haworth LR, Levy C,
et al: Tumor regression and autoimmunity in patients treated with
cytotoxic T lymphocyte-associated antigen 4 blockade and
interleukin 2: A phase I/II study. Ann Surg Oncol. 12:1005–1016.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Correale P, Botta C, Ciliberto D, Pastina
P, Ingargiola R, Zappavigna S, Tassone P, Pirtoli L, Caraglia M and
Tagliaferri P: Immunotherapy of colorectal cancer: New perspectives
after a long path. Immunotherapy. 8:1281–1292. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Correale P, Tagliaferri P, Fioravanti A,
Del Vecchio MT, Remondo C, Montagnani F, Rotundo MS, Ginanneschi C,
Martellucci I, Francini E, et al: Immunity feedback and clinical
outcome in colon cancer patients undergoing chemoimmunotherapy with
gemcitabine + FOLFOX followed by subcutaneous granulocyte
macrophage colony-stimulating factor and aldesleukin (GOLFIG-1
Trial). Clin Cancer Res. 14:4192–4199. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kudo-Saito C, Schlom J and Hodge JW:
Induction of an antigen cascade by diversified
subcutaneous/intratumoral vaccination is associated with antitumor
responses. Clin Cancer Res. 11:2416–2426. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hodge JW, Sharp HJ and Gameiro SR:
Abscopal regression of antigen disparate tumors by antigen cascade
after systemic tumor vaccination in combination with local tumor
radiation. Cancer Biother Radiopharm. 27:12–22. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Diem S, Keller F, Ruesch R, Maillard SA,
Speiser DE, Dummer R, Siano M, Urner-Bloch U, Goldinger SM and
Flatz L: Pembrolizumab-triggered uveitis: An additional surrogate
marker for responders in melanoma immunotherapy? J Immunother.
39:379–382. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wargo JA, Reuben A, Cooper ZA, Oh KS and
Sullivan RJ: Immune effects of chemotherapy, radiation, and
targeted therapy and opportunities for combination with
immunotherapy. Semin Oncol. 42:601–616. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gibney GT, Weiner LM and Atkins MB:
Predictive biomarkers for checkpoint inhibitor-based immunotherapy.
Lancet Oncol. 17:e542–e551. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Seymour L, Bogaerts J, Perrone A, Ford R,
Schwartz LH, Mandrekar S, Lin NU, Litière S, Dancey J, Chen A, et
al: iRECIST: Guidelines for response criteria for use in trials
testing immunotherapeutics. Lancet Oncol. 18:e143–e152. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Correale P, Botta C, Martino EC, Ulivieri
C, Battaglia G, Carfagno T, Rossetti MG, Fioravanti A, Guidelli GM,
Cheleschi S, et al: Phase Ib study of poly-epitope peptide
vaccination to thymidylate synthase (TSPP) and GOLFIG
chemo-immunotherapy for treatment of metastatic colorectal cancer
patients. Oncoimmunology. 5:e11012052015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Martino EC, Misso G, Pastina P, Costantini
S, Vanni F, Gandolfo C, Botta C, Capone F, Lombardi A, Pirtoli L,
et al: Immune-modulating effects of bevacizumab in metastatic
non-small-cell lung cancer patients. Cell Death Discov.
2:160252016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Correale P, Cerretani D, Remondo C,
Martellucci I, Marsili S, La Placa M, Sciandivasci A, Paolelli L,
Pascucci A, Rossi M, et al: A novel metronomic chemotherapy regimen
of weekly platinum and daily oral etoposide in high-risk non-small
cell lung cancer patients. Oncol Rep. 16:133–140. 2006.PubMed/NCBI
|
|
41
|
Pastina P, Nardone V, Croci S, Battaglia
G, Vanni F, Bellan C, Barbarino M, Ricci V, Costantini S, Capone F,
et al: Anti-cancer activity of dose-fractioned mPE +/− bevacizumab
regimen is paralleled by immune-modulation in advanced squamous
NSLC patients. J Thoracic Dis. 9:3123–3131. 2017. View Article : Google Scholar
|
|
42
|
Correale P, Botta C, Basile A, Pagliuchi
M, Licchetta A, Martellucci I, Bestoso E, Apollinari S, Addeo R,
Misso G, et al: Phase II trial of bevacizumab and dose/dense
chemotherapy with cisplatin and metronomic daily oral etoposide in
advanced non-small-cell-lung cancer patients. Cancer Biol Ther.
12:112–118. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Correale P, Remondo C, Carbone SF, Ricci
V, Migali C, Martellucci I, Licchetta A, Addeo R, Volterrani L,
Gotti G, et al: Dose/dense metronomic chemotherapy with fractioned
cisplatin and oral daily etoposide enhances the anti-angiogenic
effects of bevacizumab and has strong antitumor activity in
advanced non-small-cell-lung cancer patients. Cancer Biol Ther.
9:685–693. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Pastina P, Nardone V, Botta C, Croci S,
Tini P, Battaglia G, Ricci V, Cusi MG, Gandolfo C, Misso G, et al:
Radiotherapy prolongs the survival of advanced non-small-cell lung
cancer patients undergone to an immune-modulating treatment with
dose-fractioned cisplatin and metronomic etoposide and bevacizumab
(mPEBev). Oncotarget. 8:75904–75913. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Day D and Hansen AR: Immune-related
adverse events associated with immune checkpoint inhibitors.
BioDrugs. 30:571–584. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Weber JS, Yang JC, Atkins MB and Disis ML:
Toxicities of immunotherapy for the practitioner. J Clin Oncol.
33:2092–2099. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
De Remigis A, de Gruijl TD, Uram JN, Tzou
SC, Iwama S, Talor MV, Armstrong TD, Santegoets SJ, Slovin SF,
Zheng L, et al: Development of thyroglobulin antibodies after GVAX
immunotherapy is associated with prolonged survival. Int J Cancer.
136:127–137. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Yuan J, Adamow M, Ginsberg BA, Rasalan TS,
Ritter E, Gallardo HF, Xu Y, Pogoriler E, Terzulli SL, Kuk D, et
al: Integrated NY-ESO-1 antibody and CD8+ T-cell responses
correlate with clinical benefit in advanced melanoma patients
treated with ipilimumab. Proc Natl Acad Sci USA. 108:16723–16728.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Cusi MG, Botta C, Pastina P, Rossetti MG,
Dreassi E, Guidelli GM, Fioravanti A, Martino EC, Gandolfo C,
Pagliuchi M, et al: Phase I trial of thymidylate synthase
poly-epitope peptide (TSPP) vaccine in advanced cancer patients.
Cancer Immunol Immunother. 64:1159–1173. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Correale P, Botta C, Rotundo MS, Guglielmo
A, Conca R, Licchetta A, Pastina P, Bestoso E, Ciliberto D, Cusi
MG, et al: Gemcitabine, oxaliplatin, levofolinate, 5-fluorouracil,
granulocyte-macrophage colony-stimulating factor, and interleukin-2
(GOLFIG) versus FOLFOX chemotherapy in metastatic colorectal cancer
patients: The GOLFIG-2 multicentric open-label randomized phase III
trial. J Immunother. 37:26–35. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Correale P, Botta C, Staropoli N, Nardone
V, Pastina P, Ulivieri C, Gandolfo C, Baldari TC, Lazzi S,
Ciliberto D, et al: Systemic inflammatory status predict the
outcome of k-RAS WT metastatic colorectal cancer patients receiving
the thymidylate synthase poly-epitope-peptide anticancer vaccine.
Oncotarget. 9:20539–20554. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Guirgis HM: The impact of PD-L1 on
survival and value of the immune check point inhibitors in
non-small-cell lung cancer; proposal, policies and perspective. J
Immunother Cancer. 6:152018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Correale P, Cusi MG, Tsang KY, Del Vecchio
MT, Marsili S, Placa ML, Intrivici C, Aquino A, Micheli L, Nencini
C, et al: Chemo-immunotherapy of metastatic colorectal carcinoma
with gemcitabine plus FOLFOX 4 followed by subcutaneous granulocyte
macrophage colony-stimulating factor and interleukin-2 induces
strong immunologic and antitumor activity in metastatic colon
cancer patients. J Clin Oncol. 23:8950–8958. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Bagley SJ, Kothari S, Aggarwal C, Bauml
JM, Alley EW, Evans TL, Kosteva JA, Ciunci CA, Gabriel PE, Thompson
JC, et al: Pretreatment neutrophil-to-lymphocyte ratio as a marker
of outcomes in nivolumab-treated patients with advanced
non-small-cell lung cancer. Lung Cancer. 106:1–7. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Banna GL, Passiglia F, Colonese F, Canova
S, Menis J, Addeo A, Russo A and Cortinovis DL: Immune-checkpoint
inhibitors in non-small cell lung cancer: A tool to improve
patients' selection. Crit Rev Oncol Hematol. 129:27–39. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Dudley JC, Lin MT, Le DT and Eshleman JR:
Microsatellite instability as a biomarker for PD-1 blockade. Clin
Cancer Res. 22:813–820. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Zhu Y, Zhao F, Li Z and Yu J: Current
landscape and future directions of biomarkers for predicting
responses to immune checkpoint inhibitors. Cancer Manag Res.
10:2475–2488. 2018. View Article : Google Scholar : PubMed/NCBI
|