Introduction
The use of epidermal growth factor receptor-tyrosine
kinase inhibitors (EGFR-TKIs) has been approved for the treatment
of advanced non-small-cell lung carcinoma (NSCLC) with
EGFR-activating mutations. Although their efficacy is
well-established, almost all patients treated with EGFR-TKIs
eventually develop resistance to these agents. Of those patients,
60% carry the missense mutation T790M in EGFR (1), which may occur concurrently with human
epidermal growth factor receptor 2 (HER2) mutation,
MET amplification, or small-cell transformation. Hence, the
T790M mutation plays an important role in acquired resistance to
treatment with EGFR-TKIs. In 2015, the third-generation EGFR-TKI
osimertinib was approved for the treatment of NSCLC harboring the
T790M mutation in patients with disease progression following
therapy with first- or second-generation EGFR-TKIs. Therefore,
re-biopsy may be used to detect the mutation responsible for the
development of resistance in such patients.
The present case report details the occurrence of
squamous cell transformation in combination with the T790M mutation
and the efficacy of osimertinib in a patient with lung
adenocarcinoma.
Case report
A 73-year-old male Japanese patient, with a smoking
history of 75 pack-years, was referred to the Department of
Respiratory Medicine of Showa University Fujigaoka Hospital
(Yokohama, Japan) with dyspnea on effort. A chest X-ray revealed
severe pleural effusion in the left lung and a chest computed
tomography scan revealed a primary tumor (77 mm in greatest
diameter) in the left upper lobe. In addition, positron emission
tomography detected a mass in the left adrenal gland. There was no
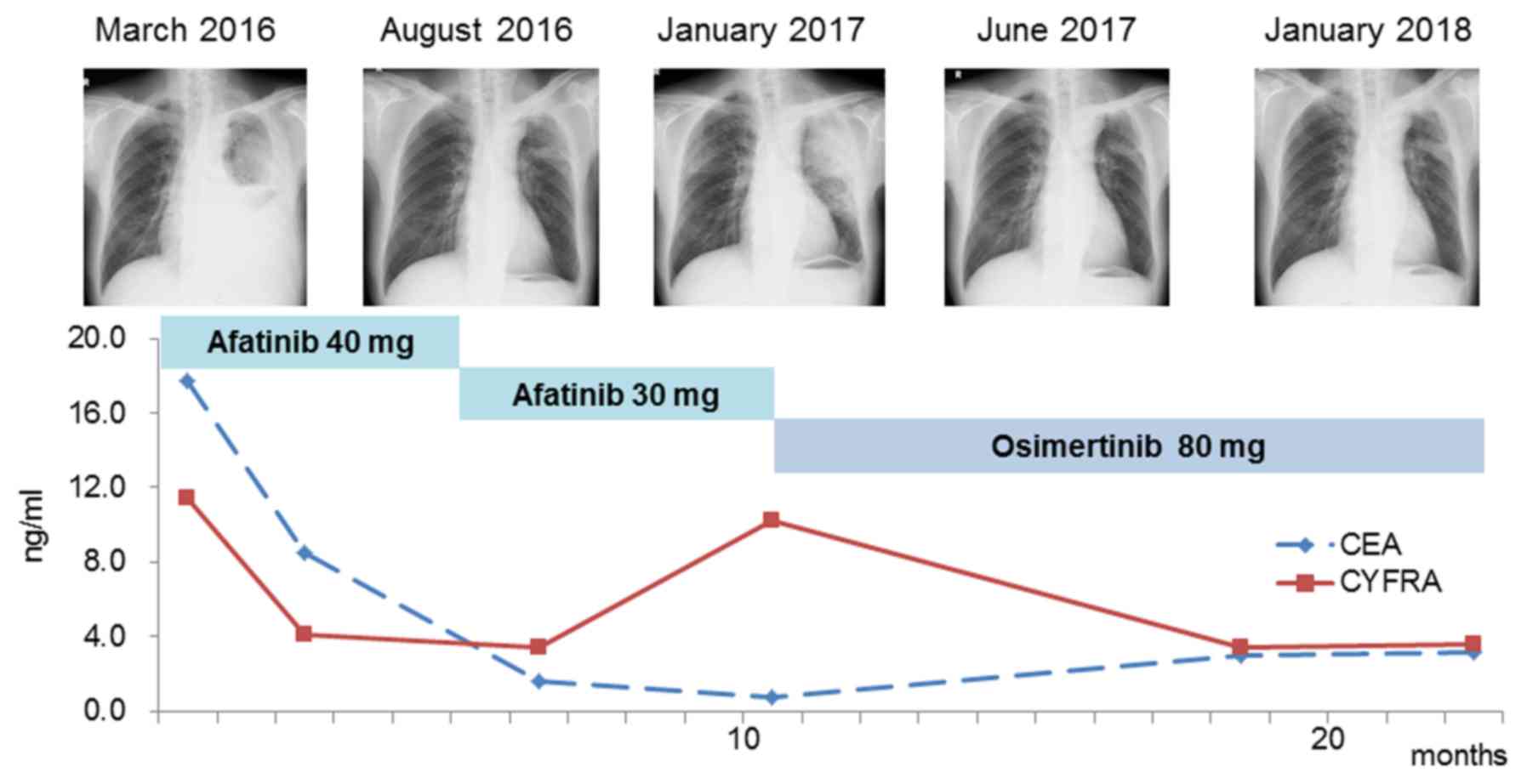
evidence of brain or bone metastasis. The levels of the tumor
markers carcinoembryonic antigen (CEA) and cytokeratin 19 fragment
(CYFRA) were increased; (CEA: 17.7 ng/ml; normal range: 0–5.0
ng/ml, CYFRA: 11.4 ng/ml; normal range: 0–3.5 ng/ml; Fig. 1). Adenocarcinoma cells were detected
in the pleural effusion. Immunohistochemical analysis was not
possible due to the limited number of cancer cells. Transbronchial
lung biopsy from the left upper lobe did not demonstrate malignant
findings. The patient was diagnosed with stage IVA lung
adenocarcinoma, and cytology examination using a specimen from the
pleural effusion revealed the presence of an EGFR-activating
mutation (deletion E746-A750 in exon 19). Hence, treatment with the
second-generation EGFR-TKI afatinib (40 mg) was initiated as
first-line therapy.
Gene alterations in lung carcinoma were analyzed by
collecting and examining pleural effusion at the time of diagnosis.
DNA was extracted from cell pellets using the QIAmp DNA Mini kit
(Qiagen, Valencia, CA, USA). The PCR-Invader (BML Inc., Tokyo,
Japan) method was performed to detect EGFR mutations.
Re-biopsy specimens were also analyzed in a similar manner.
Official approval for gene analysis was obtained in advance from
the Ethics Committee for Genomic Research at Showa University
(approval no. 113) and the patient provided written informed
consent.
At 5 months after initiation of afatinib treatment,
the primary tumor site had almost disappeared, without observed
recurrence. In addition, the levels of CEA and CYFRA returned to
normal. The treatment course exacerbated the skin lesions at grade
3 according to the Common Terminology Criteria for Adverse Events
version 4.0 (2), and the dosage of
afatinib was adjusted to 30 mg. Ten months after administration of
afatinib, recurrence of the tumor on the primary site was reported.
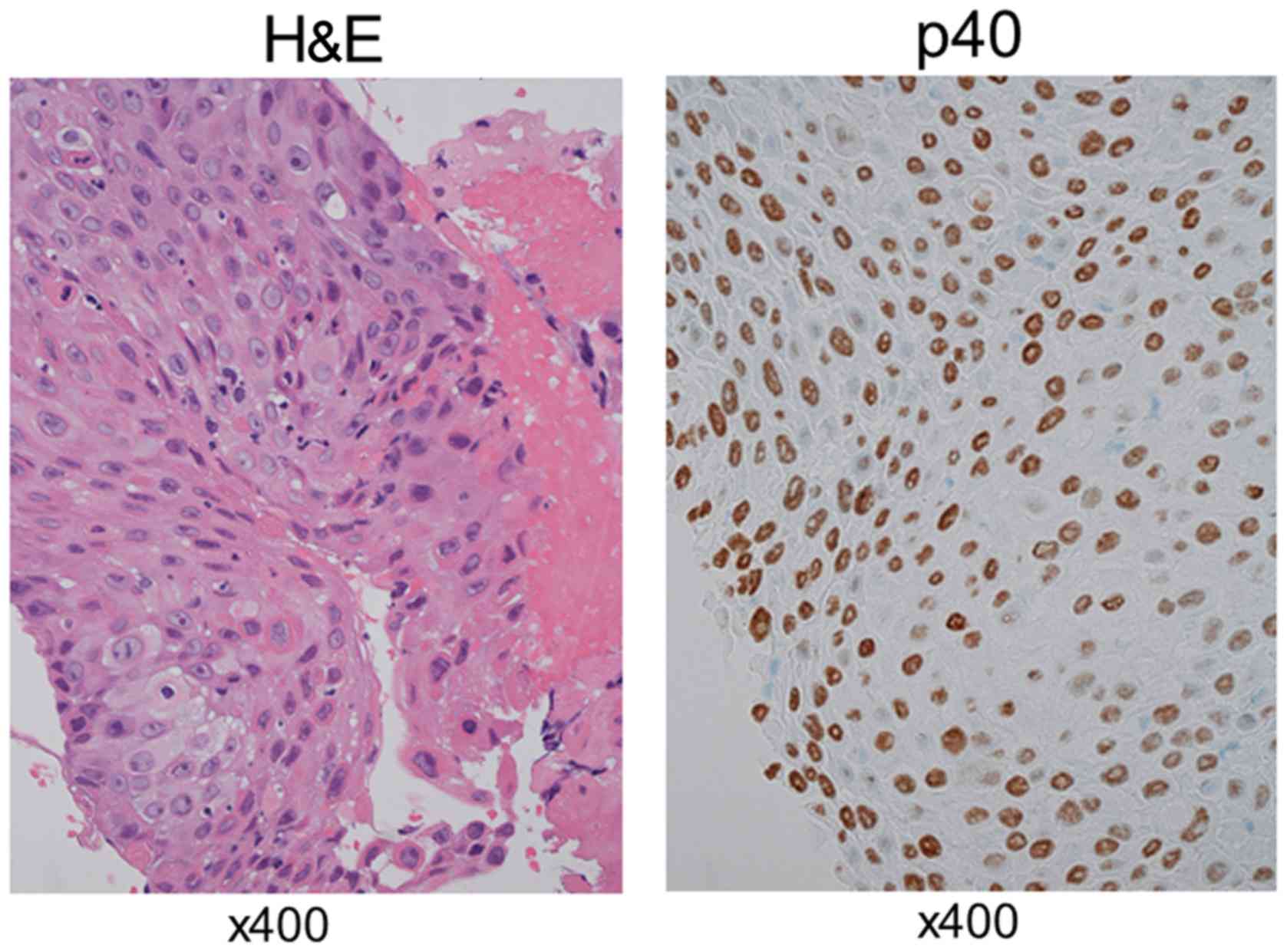
Bronchoscopic re-biopsy of the tissue was performed;
pathologically, the tumor was a typical squamous cell carcinoma
with alveolar structures. On immunohistochemical examination, the
tumor was positive for p40 (Fig. 2)
and negative for thyroid transcription factor (TTF)-1 and Napsin A.
Although the levels of CYFRA were increased (10.2 ng/ml) at this
point, the levels of CEA remained within normal limits. Paraffin
sections were analyzed to determine the presence of an acquired
resistance mutation. In addition to the exon 19 deletion originally
harbored by the tumor at the time of diagnosis, this analysis
detected the T790M mutation. The patient received treatment with
the third-generation EGFR-TKI osimertinib (80 mg), and a partial
response was observed in the recurrent site. The levels of CYFRA
returned to normal, and the patient was relapse-free 1 year after
treatment initiation. At the last follow up in April 2018, the
patient was symptom free.
Discussion
Numerous studies have reported the use of re-biopsy
in NSCLC patients with disease progression following first- or
second-generation EGFR-TKI therapy (3,4).
Moreover, recent studies have reported squamous cell transformation
in patients with NSCLC during the course of treatment (5–18),
described as a mechanism of acquired resistance to these
agents.
In the present case, the T790M mutation was detected
in combination with squamous cell transformation in a patient with
lung adenocarcinoma who was treated with afatinib. The tumor
maintained the original exon 19 deletion, suggesting a monoclonal
origin and clonal progression. Administration of osimertinib
resulted in a partial response and was well-tolerated, without
severe adverse events. Third-generation EGFR-TKIs, such as
osimertinib and rociletinib, selectively block T790M mutant clones.
The efficacy of osimertinib in the treatment of T790M-positive
NSCLC has been demonstrated (19).
As shown in Table I, a total of 18
cases of squamous cell transformation in lung adenocarcinoma
harboring an EGFR-activating mutation after treatment with
cytotoxic chemotherapy or EGFR-TKIs have been reported (5–18); in 8
of those, the T790M mutation was also detected. These patients were
treated with EGFR-TKIs as first-line therapy. There was no
significant association of the T790M mutation with age, gender,
clinical stage, smoking history or activating mutation status (data
not shown). Five of the patients with the T790M mutation received
treatment with third-generation EGFR-TKIs, and the recurrence site
improved in all cases. EGFR-TKIs have been reported to be less
effective in the treatment of non-adenocarcinoma tumors compared
with adenocarcinoma (20). However,
third-generation EGFR-TKIs may be beneficial in the treatment of
squamous cell carcinoma harboring the T790M mutation.
 | Table I.Clinical characteristics of lung
cancer patients. |
Table I.
Clinical characteristics of lung
cancer patients.
| No. | Age, years | Sex | Stage | EGFR
mutation | T790M | TTF-1 | Napsin A | p40 | p63 | Smoking history | Pre-TKI
treatment | 3rd generation
TKI | (Refs.) |
|---|
| 1 | 58 | Female | IIIA | Exon19 del | − | − |
|
| + | Evera | Erlotinib | − | (5) |
| 2 | 63 | Female | IVA | L858R | + | − |
| + |
| Never | Erlotinib | − | (6) |
| 3 | 43 | Male | IIIA | Exon19 del | − | + |
|
|
| Evera | − | − | (7) |
| 4 | 51 | Female | IVB | Exon19 del | − | − | − | + |
| Evera | Gefitinib | − | (8) |
| 5 | 61 | Female | IVB | L858R | − |
|
| + |
| Never | Gefitinib | − | (8) |
| 6 | 63 | Female | IV | L858R | − | − |
|
| + | Never | Erlotinib | − | (9) |
| 7 | 66 | Female | IVA | Exon19 del | − | − | − |
| + | Never | Erlotinib | − | (10) |
| 8 | 74 | Female | IVA | L858R | + | − |
| + |
| Evera | Gefitinib | − | (11) |
| 9 | 79 | Female | IVB | Exon19 del | + | − |
| + |
| Never | Gefitinib | − | (11) |
| 10 | 48 | Female | IIIA | Exon19 del | − | − |
| + |
| Never | Gefitinib | − | (12) |
| 11 | 64 | Female | IV | L858R | + | − |
| + |
| Never | Gefitinib | Rociletinib | (12) |
| 12 | 44 | Female | IV | Exon19 del | + | − |
| + |
| Evera | Afatinib | Osimertinib | (13) |
| 13 | 43 | Female | IVB | L858R | − | − |
| + |
| Evera | Gefitinib | − | (14) |
| 14 | 79 | Female | IIB | Exon19 del | − | − |
|
| + | Never | − | − | (15) |
| 15 | 69 | Male | IVB | Exon19 del | + | − |
| + |
| Evera | Erlotinib | Osimertinib | (16) |
| 16 | 67 | Female | IVA | Exon19 del | − | − |
|
| + | Unknown | Afatinib | − | (17) |
| 17 | 68 | Male | IB | L858R | + | − |
| + |
| Evera | Erlotinib | Osimertinib | (18) |
| 18 | 73 | Male | IVB | Exon19 del | + | − | − | + |
| Evera | Afatinib | Osimertinib | Present case |
The pathogenesis of squamous cell transformation in
lung adenocarcinoma remains elusive. In NSCLC, the presence of
adenocarcinoma and squamous cell carcinoma is associated with
distinct clinical characteristics, gene expression, and specific
biomarkers. Adenocarcinoma usually arises in the distal airway,
whereas squamous cell carcinoma is more frequently reported in the
proximal airway. EGFR mutations are more frequent in
adenocarcinoma compared with squamous cell carcinoma.
Immunohistochemical analysis in adenocarcinoma demonstrated
diffusely positive staining for TTF-1 and Napsin A, and negative
staining for p40 and p63 expression, whereas the opposite was
observed in squamous cell carcinoma. In the present study,
detection of an EGFR exon19 deletion in the re-biopsy
specimen decreased the possibility of de novo squamous cell
carcinoma development. There are two possible mechanisms of
transformation: The first hypothesis is that adenocarcinoma may
develop squamous metaplasia, an authentic transformation during
therapy. In a mouse model, liver kinase B1 inactivation resulted in
accumulation of reactive oxygen species (ROS), eventually causing
progressive transdifferentiation of the adenocarcinoma to squamous
cell carcinoma through an intermediate mixed status (21). Although excessive levels of ROS
induce apoptosis and decrease cell proliferation in adenocarcinoma,
squamous cell carcinoma is strongly resistant to ROS. The second
hypothesis is that the initial tumor contains squamous cell
carcinoma components in varying proportions, clinically termed
adenosquamous carcinoma. This is a rare subtype of NSCLC (≤4% of
all lung carcinomas), defined by mixed adenocarcinomatous and
squamous cell carcinomatous components >10% (22). In some cases, clinically defined
adenocarcinoma or squamous cell carcinoma, diagnosed through biopsy
or cytology specimens, may in fact be adenosquamous carcinoma.
Therefore, it is important to diagnose adenosquamous carcinoma
using surgical specimens rather than biopsy samples. The
clinicopathological characteristics of adenosquamous carcinoma
remain unclear. It has been reported that adenosquamous carcinoma
is more aggressive and has a worse prognosis compared with either
adenocarcinoma or squamous cell carcinoma (23,24). By
contrast, several studies revealed similar frequencies of
EGFR mutations between adenosquamous carcinoma and
adenocarcinoma (25,26), an association between adenosquamous
carcinoma with EGFR-activating mutations, and good response
to EGFR-TKIs (27).
The aforementioned hypotheses suggest that resistant
clones, which consist of squamous cell carcinoma, are increased
through EGFR-TKI therapy. As shown in Fig. 1, the CEA and CYFRA tumor markers were
elevated at the time of diagnosis and returned within normal limits
simultaneously during therapy with afatinib. The levels of CEA,
which is particularly associated with adenocarcinoma, remained
within the normal range, whereas the level of CYFRA, a tumor marker
for follow-up of squamous cell carcinoma, increased to 10.2 ng/ml
during disease progression. This suggests that the initial
adenocarcinoma was diminished, and the squamous cell carcinoma
component was limited by treatment with afatinib, a finding
consistent with the latter hypothesis. However, it is possible that
adenocarcinoma progressively transdifferentiates into squamous cell
carcinoma during therapy, even if the original tumor contains both
adenocarcinoma and squamous cell carcinoma.
In the present case, the T790M mutation was
identified in a patient with lung adenocarcinoma and presence of
squamous cell carcinoma, as shown by re-biopsy. The patient
received osimertinib treatment, with an evident beneficial effect
on the recurrence site. These findings suggest that this
third-generation EGFR-TKI is a viable treatment option for patients
with lung adenocarcinoma exhibiting squamous cell transformation
harboring the T790M mutation. Re-sequencing is warranted,
regardless of the detection of morphological transition of primary
adenocarcinoma. The use of re-biopsy may also be important for
investigating the progression of lung cancer and overcoming
resistance to therapeutic agents.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets generated and/or analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
FY, EK, AW and YS examined and cared for the
patient. FY wrote the manuscript. EK, AW and YS contributed to the
writing of the manuscript and commented at all stages. FY had full
access to all the data in the study and has final responsibility
for the decision to submit for publication. All the authors have
read and approved the final version of this manuscript.
Ethics approval and consent to
participate
Official approval for gene analysis was obtained in
advance from the Ethics Committee for Genomic Research at Showa
University (approval no. 113). The patient provided written
informed consent for gene analysis.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of the case details and any associated
images.
Competing interests
All the authors declare that they have no conflict
of interest in connection with this study. The authors received no
payment or services from a third party in relation to this
study.
Glossary
Abbreviations
Abbreviations:
|
EGFR
|
epidermal growth factor receptor
|
|
TKI
|
tyrosine kinase inhibitor
|
|
NSCLC
|
non-small-cell lung carcinoma
|
|
CEA
|
carcinoembryonic antigen
|
|
CYFRA
|
cytokeratin 19 fragment
|
|
ROS
|
reactive oxygen species
|
References
|
1
|
Yu HA, Arcila ME, Rekhtman N, Sima CS,
Zakowski MF, Pao W, Kris MG, Miller VA, Ladanyi M and Riely GJ:
Analysis of tumor specimens at the time of acquired resistance to
EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers.
Clin Cancer Res. 19:2240–2247. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cancer Therapy Evaluation Program (CTEP)
Common Terminology Criteria for Adverse Events (CTCAE). Version
4.0. National Cancer Institute, . 2010.
|
|
3
|
Chouaid C, Dujon C, Do P, Monnet I,
Madroszyk A, Le Caer H, Auliac JB, Berard H, Thomas P, Lena H, et
al: Feasibility and clinical impact of re-biopsy in advanced non
small-cell lung cancer: A prospective multicenter study in a
real-world setting. Lung Cancer. 86:170–173. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nosaki K, Satouchi M, Kurata T, Yoshida T,
Okamoto I, Katakami N, Imamura F, Tanaka K, Yamane Y, Yamamoto N,
et al: Re-biopsy status among non-small cell lung cancer patients
in Japan: A retrospective study. Lung Cancer. 101:1–8. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Scher KS, Saldivar JS, Fishbein M,
Marchevsky A and Reckamp KL: EGFR-mutated lung cancer with
T790M-acquired resistance in the brain and histologic
transformation in the lung. J Natl Compr Canc Netw. 11:1040–1044.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bugano DDG, Kalhor N, Zhang J, Neskey M
and William WN: Squamous-cell transformation in a patient with lung
adenocarcinoma receiving erlotinib: Co-occurrence with T790M
mutation. Cancer Treat Commun. 4:34–36. 2015. View Article : Google Scholar
|
|
7
|
Burkart J, Shilo K, Zhao W, Ozkan E, Ajam
A and Otterson GA: Metastatic squamous cell carcinoma component
from an adenosquamous carcinoma of the lung with identical
epidermal growth factor receptor mutations. Case Rep Pulmonol.
2015:2838752015.PubMed/NCBI
|
|
8
|
Hsieh MS, Jhuang JY, Hua SF and Chou YH:
Histologic evolution from adenocarcinoma to squamous cell carcinoma
after gefitinib treatment. Ann Thorac Surg. 99:316–319. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kuiper JL, Ronden MI, Becker A, Heideman
DA, van Hengel P, Ylstra B, Thunnissen E and Smit EF:
Transformation to a squamous cell carcinoma phenotype of an
EGFR-mutated NSCLC patient after treatment with an EGFR-tyrosine
kinase inhibitor. J Clin Pathol. 68:320–321. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Levin PA, Mayer M, Hoskin S, Sailors J,
Oliver DH and Gerber DE: Histologic transformation from
adenocarcinoma to squamous cell carcinoma as a mechanism of
resistance to EGFR inhibition. J Thorac Oncol. 10:e86–e88. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jukna A, Montanari G, Mengoli MC, Cavazza
A, Covi M, Barbieri F, Bertolini F and Rossi G: Squamous cell
carcinoma ‘transformation’ concurrent with secondary T790M mutation
in resistant EGFR-mutated adenocarcinomas. J Thorac Oncol.
11:e49–e51. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Haratani K, Hayashi H, Watanabe S, Kaneda
H, Yoshida T, Takeda M, Shimizu T and Nakagawa K: Two cases of EGFR
mutation-positive lung adenocarcinoma that transformed into
squamous cell carcinoma: Successful treatment of one case with
rociletinib. Ann Oncol. 27:200–202. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bruno R, Proietti A, Alì G, Puppo G,
Ribechini A, Chella A and Fontanini G: Squamous cell transformation
and EGFR T790M mutation as acquired resistance mechanisms in a
patient with lung adenocarcinoma treated with a tyrosine kinase
inhibitor: A case report. Oncol Lett. 14:5947–5951. 2017.PubMed/NCBI
|
|
14
|
Longo L, Mengoli MC, Bertolini F, Bettelli
S, Manfredini S and Rossi G: Synchronous occurrence of
squamous-cell carcinoma ‘transformation’ and EGFR exon 20 S768I
mutation as a novel mechanism of resistance in EGFR-mutated lung
adenocarcinoma. Lung Cancer. 103:24–26. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Le T, Sailors J, Oliver DH, Mayer M,
Hoskin S and Gerber DE: Histologic transformation of EGFR mutant
lung adenocarcinoma without exposure to EGFR inhibition. Lung
Cancer. 105:14–16. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Okabe N, Takagi H, Mine H, Fukai S,
Minemura H and Suzuki H: Osimertinib for epidermal growth factor
receptor mutation-positive lung adenocarcinoma that transformed to
T790M-positive squamous cell carcinoma. J Thorac Oncol.
12:e167–e169. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Clery E, Pisapia P, Feliciano S, Vigliar
E, Marano A, De Luca C, Malapelle U, Troncone G and Bellevicine C:
There is still a role for cytology in the ‘liquid biopsy’ era. A
lesson from a TKI-treated patient showing adenocarcinoma to
squamous cell carcinoma transition during disease progression. J
Clin Pathol. 70:798–802. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Izumi H, Yamasaki A, Ueda Y, Sumikawa T,
Maeta H, Nakamoto S and Shimizu E: Squamous cell carcinoma
transformation from EGFR-mutated lung adenocarcinoma: A case report
and literature review. Clin Lung Cancer. 19:e63–e66. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jänne PA, Yang JC, Kim DW, Planchard D,
Ohe Y, Ramalingam SS, Ahn MJ, Kim SW, Su WC, Horn L, et al: AZD9291
in EGFR inhibitor-resistant non-small-cell lung cancer. N Engl J
Med. 372:1689–1699. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shukuya T, Takahashi T, Kaira R, Ono A,
Nakamura Y, Tsuya A, Kenmotsu H, Naito T, Kaira K, Murakami H, et
al: Efficacy of gefitinib for non-adenocarcinoma non-small-cell
lung cancer patients harboring epidermal growth factor receptor
mutations: A pooled analysis of published reports. Cancer Sci.
102:1032–1037. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hou S, Zhou S, Qin Z, Yang L, Han X, Yao S
and Ji H: Evidence, mechanism, and clinical relevance of the
transdifferentiation from lung adenocarcinoma to squamous cell
carcinoma. Am J Pathol. 187:954–962. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Travis WD, Brambilla E, Nicholson AG,
Yatabe Y, Austin JHM, Beasley MB, Chirieac LR, Dacic S, Duhig E,
Flieder DB, et al: The 2015 world health organization
classification of lung tumors: Impact of genetic, clinical and
radiologic advances since the 2004 classification. J Thorac Oncol.
10:1243–1260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shimizu J, Oda M, Hayashi Y, Nonomura A
and Watanabe Y: A clinicopathologic study of resected cases of
adenosquamous carcinoma of the lung. Chest. 109:989–994. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gawrychowski J, Bruliński K, Malinowski E
and Papla B: Prognosis and survival after radical resection of
primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg.
27:686–692. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jia XL and Chen G: EGFR and KRAS mutations
in Chinese patients with adenosquamous carcinoma of the lung. Lung
Cancer. 74:396–400. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wang R, Pan Y, Li C, Zhang H, Garfield D,
Li Y, Ye T, Hu H, Luo X, Li H, et al: Analysis of major known
driver mutations and prognosis in resected adenosquamous lung
carcinomas. J Thorac Oncol. 9:760–768. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Fan L, Yang H, Yao F, Zhao Y, Gu H, Han K
and Zhao H: Clinical outcomes of epidermal growth factor receptor
tyrosine kinase inhibitors in recurrent adenosquamous carcinoma of
the lung after resection. Onco Targets Ther. 10:239–245. 2017.
View Article : Google Scholar : PubMed/NCBI
|