Introduction
The phosphatase and tensin homolog (PTEN) gene is
one of the tumor suppressor genes (1) located in chromosome 10q23.31, encoding
403 amino acids of 47166 Da protein. Loss of heterozygosity and
deletion of this gene was first reported in glioblastomas, and
later in several malignant tumors (2). PTEN germline mutations cause a
wide variety of phenotypic diseases, such as macrocephaly/autism
syndrome (OMIM #605309) usually noticed in infants and PTEN
hamartoma tumor syndrome (PHTS, OMIM #601728). PHTS includes Cowden
syndrome (CS, OMIM#158350) and Bannayan-Riley-Ruvalcaba syndrome
(BRRS, OMIM#153480) (3).
Macrocephaly/autism syndrome is an autosomal
dominant disorder characterized by increased head circumference,
abnormal facial features, and delayed psychomotor development
resulting in autistic behavior or mental retardation (4). Varga et al (5) reported that PTEN mutations were
detected in 5 of 60 (8.3%) patients with autism spectrum disorder
(ASD) and 6 of 49 (12.2%) patients with developmental delay and
macrocephaly without ASD.
CS is a multiple hamartoma syndrome with a high risk
for benign and malignant tumors of the thyroid, breast, and
endometrium in young adults and adults. Arteriovenous malformation,
multiple lipomas, and other soft-tissue tumors are also reported
(3,6). Affected individuals usually develop
macrocephaly, trichilemmomas, and papillomatous papules by late
20s. On the other hand, BRRS is a congenital disorder characterized
by macrocephaly, intestinal hamartomatous polyposis, lipomas, and
pigmented macules of the glans penis (3). For PHTS patients, 2019.2 NCCN guideline
(7) recommends that tumor follow-up
involves annual physical examination and thyroid ultrasound, with
colonoscopy every 5 years beginning at age 35 or earlier based on
family colon cancer history and kidney ultrasound every 1-2 years
starting at age 40.
We found a de novo PTEN germline mutation in
a male infant with macrocephaly and lipomas by using NGS analysis.
A rapidly growing lipoma was resected and examined for PTEN
by immunostaining, since there have been few reports on PTEN
inactivation, two hits or one hit, in tumors in PHTS patients.
Case report
Patient
Male infant was born after 37 weeks gestation with
4,078 g (+2.7 SD) in weight, 52 cm (+1.4 SD) in height and 36 cm
(+1.9 SD) in head circumference.
Family history: No physical abnormalities are
apparent with the father, 37 years old, the mother, 33 years old
and a sister, 3 years old.
Pregnancy history: Pregnancy progressed
uneventfully. The delivery was through the vagina after
induction.
Postnatal progress: No special findings in one- and
four-month postnatal examinations. The infant showed roll-over at 6
months old, neck stabilization at 7 months old, and independent
gait at 1 year and 5 months. He exhibited obsession and temper
tantrum frequently after 2 years of age. Macrocephaly was pointed
out when he was taken to a hospital for treatment of bronchitis at
the age of 8 months. His height was then 70 cm (+2.8 SD), weight
8,845 g (+0.2 SD) and head circumference 48.5 cm (+2.8 SD). Brain
MRI showed no abnormal signals in cerebral parenchyma (data not
shown), indicating that his macrocephaly was a simple one. To
elucidate the cause of macrocephaly, genetic testing was performed
at the age of 1 year and 9 months under the informed consents of
the parents.
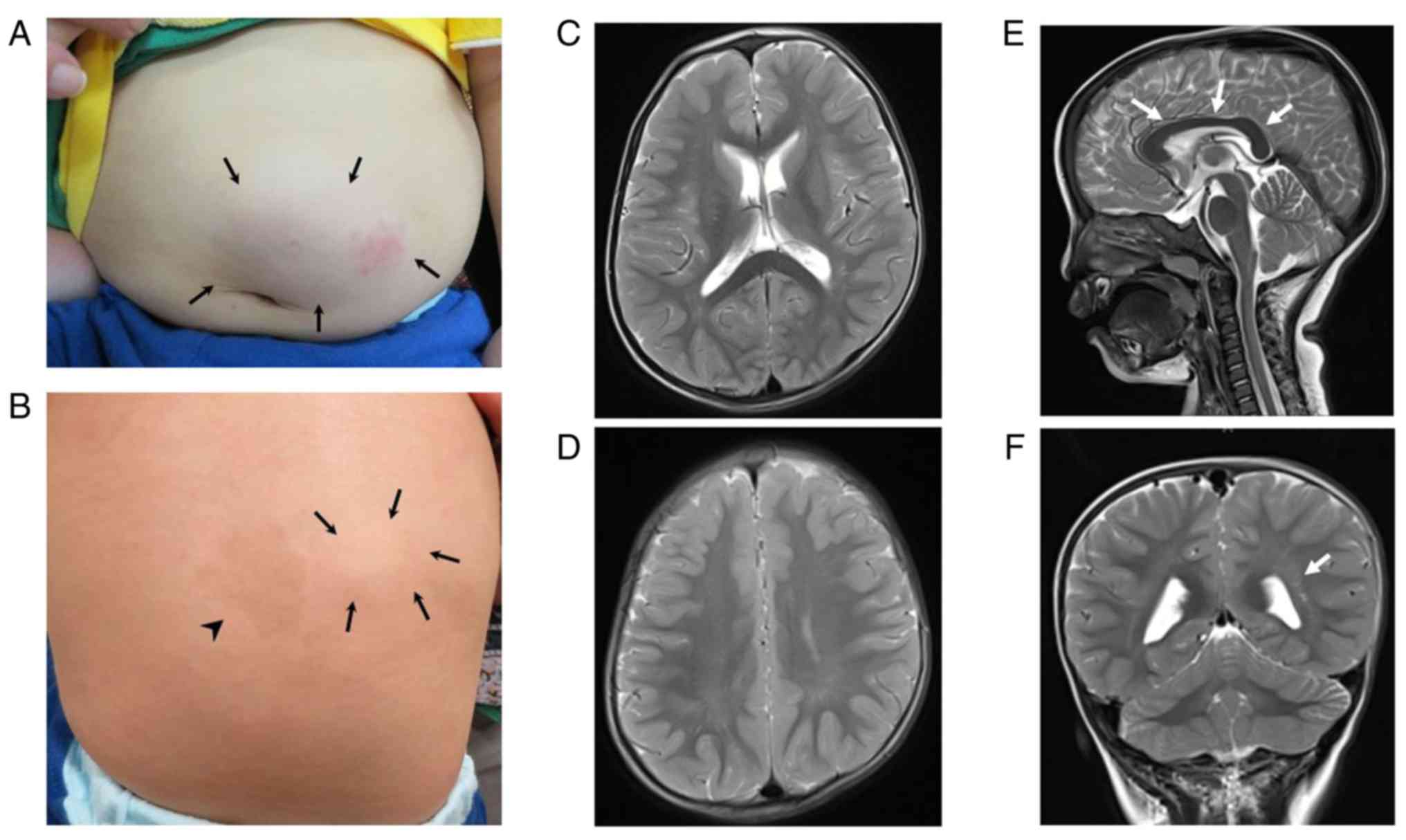
At the age of one-year, two elastic soft
subcutaneous tumors of 1-2 cm in diameter appeared in the abdomen
and in the right side of the back. A café-au-lait spot of 2 cm in
diameter was also found on the left side of the back. At the age of
1 year and 9 months, one tumor in the abdomen rapidly enlarged to
6x5 cm (Fig. 1A) and was surgically
removed. The removed tumor was soft and yellowish and
macroscopically diagnosed as a lipoma.
At the age of 2 years and 9 months, the results of
genetic testing were reported, and genetic counseling was
performed. At this time, his height was 92 cm (+0.2 SD), weight 16
kg (+2.1 SD), and head circumference 55 cm (+3.7 SD). He showed a
broad and projected forehead, a flat nasal root and low-set
deformed auricles. A café-au-lait spot of 2x2.5 cm in size was
present on the left back and subcutaneous tumors of 2x2 cm in the
right back (Fig. 1B) and in the sole
(not shown). Developmental test by Kyoto Scale of Psychological
Development 2001(8) showed 64 scores
in total developmental quotient (100 as an average), indicating
that he had moderate developmental delay.
At the age of 3 years, follow-up brain MRI showed no
abnormality in the cerebral white matter (Fig. 1C and D), except for the hypertrophied corpus
callosum (Fig. 1E) and enlargement
of the perivascular space (Fig. 1F),
of which findings were consistent with simple macrocephaly.
At the age of 5 years, subcutaneous tumors in the
back and the sole remained the same in size, and no newly developed
tumors and café-au-lait spots were detected. He could not
communicate normally and was diagnosed as ASD with moderate
developmental delay.
Chromosomal analysis
Using peripheral blood, G-banding was performed.
Whole-exome sequencing and Sanger
sequencing
DNA was extracted from peripheral blood of the
patient and the parents and Whole exome sequencing was performed as
previously described (9). Regions
suspected of containing pathological mutations were amplified by
PCR and subjected to Sanger analysis (HGMDR Professional
2016.1).
Pathologic examination
The surgical specimen was fixed in formalin and
embedded in a paraffin block. Sections cut from the block were
stained with hematoxylin-eosin and with an immunoperoxidase method
using anti-PTEN antibody (Dako/Agilent Technologies, Santa Clara,
CA). Stained sections were examined under a light microscope. As a
control, a subcutaneous fat containing skin sample obtained from a
one-year-old male infant without CS were used anonymously.
Chromosomal analysis
Chromosomal analysis showed a normal karyotype.
Mutation of the PTEN gene
In exon 3 of the PTEN (NM_000314.7),
c.195C>A, p.Y65* was found as a heterozygous germline
variant in the patient. This mutation is considered as pathogenic,
since the same mutation has been reported in one young adult female
with macrocephaly/autism syndrome and one adult female with CS
(10,11) (referred HGMDR Professional
2019.1). The predicting truncated PTEN protein with deletion of
most of the C-terminal region is likely unstable leading to
haploinsufficiency. This mutation is sporadic, since his parents
did not carry the mutation. Based on these results, we diagnosed
this patient with PTEN hamartoma tumor syndrome (PHTS). As
this mutation was reported in a CS case, we performed ultrasound
analysis of the thyroid and visual and palpitation inspection of
breasts of the patient at 2 years and 10 months. No abnormalities
were found in both tissues. Endoscopic examination of
gastrointestinal tract was not performed because of his young
age.
Pathologic findings of the
subcutaneous tumor
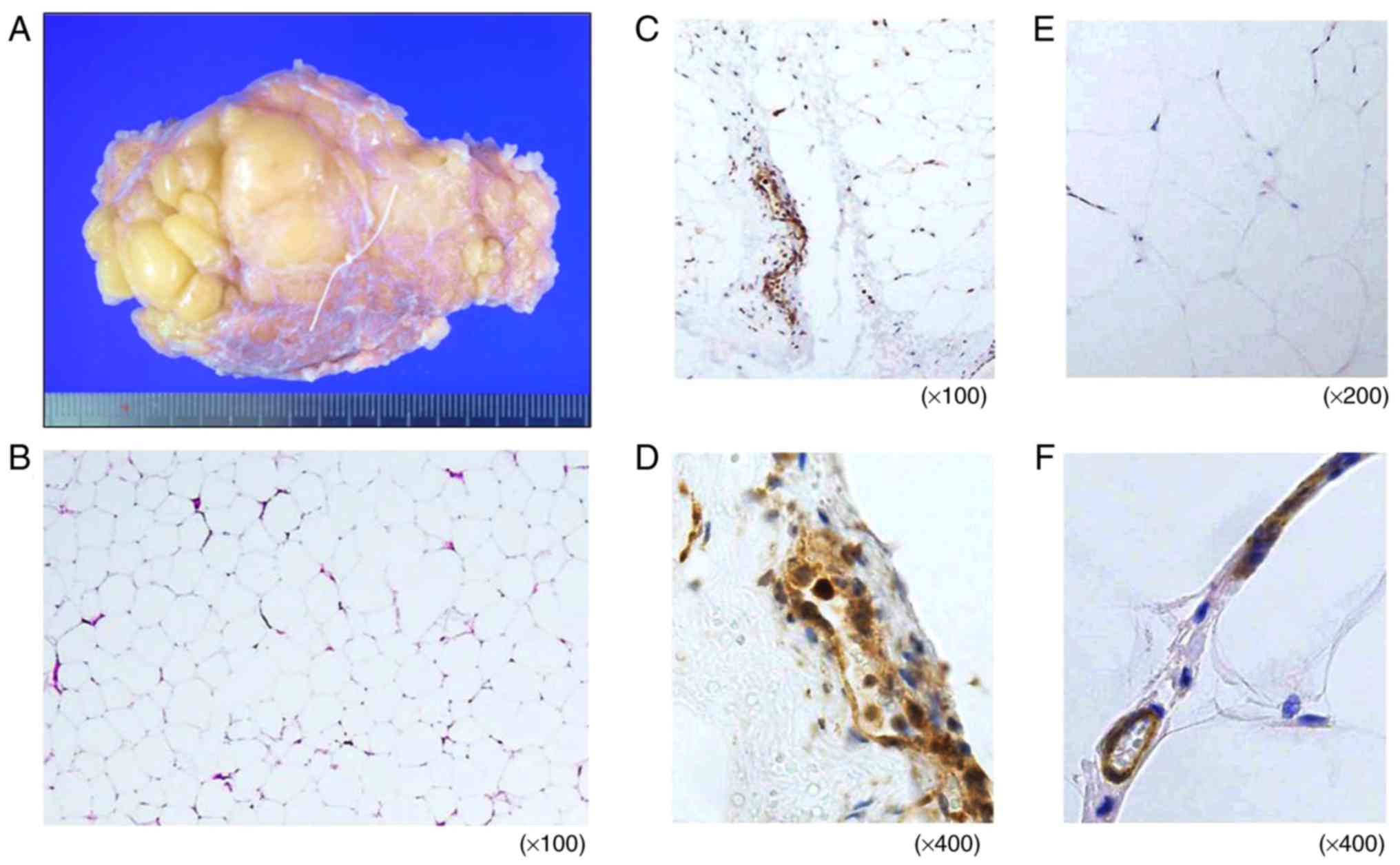
The surgical specimen had a lobulated macroscopic
appearance and was encapsulated with delicate fibrous veil
(Fig. 2A). Histologically, it
consisted of mature adipocytes, sparse blood vessels and thin
collagen bundles (Fig. 2B), and the
diagnosis of lipoma was confirmed. Immunohistochemically, PTEN
expression was observed in vessels in the control sample, as was
expected (Fig. 2C and D). A few subcutaneous adipocytes were also
stained. Similarly, in the lipoma tissue, vessels and a small
number of neoplastic adipocytes were PTEN-positive (Fig. 2E and F). No obvious differences in PTEN
expression, its distribution pattern and intensity, were detected
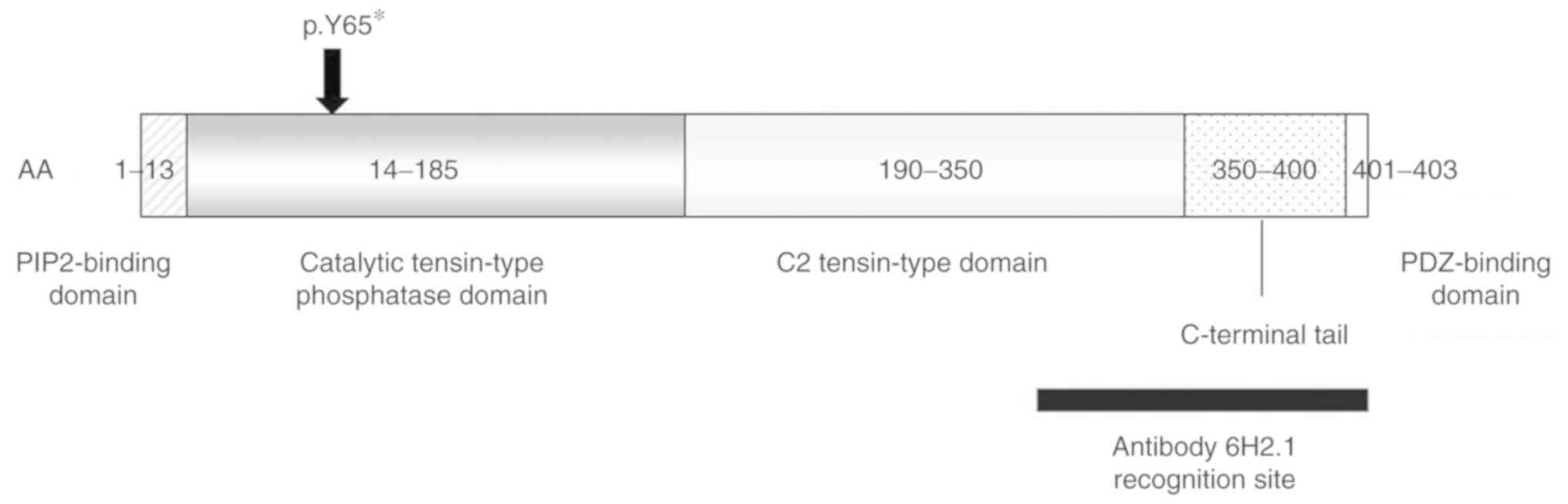
between the lipoma tissue and the control tissue. Fig. 3 shows the position of the mutation in
the PTEN protein (12). Anti-PTEN
antibody binds to a C-terminal region (13). It is not possible to bind to the
truncated protein due to the nonsense mutation in this patient
(Fig. 3).
Discussion
We found a PTEN mutation by NGS analysis in a
male infant with macrocephaly. Brain MRI examination showed simple
macrocephaly consistent with PTEN macrocephaly/autism
syndrome reported by Vanderver et al (14) and Bhargava et al (15).
Table I shows 30
patients of <3 years of age with macrocephaly or autism spectrum
in whom PTEN mutations were detected (4,11,14-20).
Clinical manifestations of these patients are presented in Table II. All cases showed developmental
delay with 8 cases diagnosed as autism spectrum and 10 hypotonia.
Ten of 30 cases showed frontal bossing with 8 exhibiting
café-au-lait spots and skin features, and 5 diagnosed with tumors
and hamartomas, such as gastrointestinal polyps and cutaneous
lipomas. Our case, an only in infant patient with
macrocephaly/autism syndrome reported, suggests that the
PTEN mutation detected is responsible for the syndrome.
 | Table IReported 30 patients diagnosed as
having PTEN mutation at <3 years. |
Table I
Reported 30 patients diagnosed as
having PTEN mutation at <3 years.
| Author, year | Case no. | Age | PTEN
mutation | Inheritance | (Refs.) |
|---|
| Vanderver et
al, 2014 | 1 | 0d | partial deletion of
exon 6, identified on array-CGH; arr10q23.31
(89.683.610-89.702.204) *1 | de novo | (14) |
| Vanderver et
al, 2014 | 2 | 3m | c.1120_1121dup :
p.D375* | de novo | (14) |
| Vanderver et
al, 2014 | 3 | 5m | c.A17T : p.K6I | ND | (14) |
| Tan et al,
2011 and Vanderver et al, 2014 | 4 | 7m | c.253+5G>T | de novo | (11,14) |
| Vanderver et
al, 2014 | 5 | 7m | Yes | ND | (14) |
| Tan et al,
2011 and Vanderver et al, 2014 | 6 | 8m | c.T149C : p.I50T | de novo | (11,14) |
| Present study | 7 | 8m | c.C195A :
p.Y65* | de novo | - |
| Varga et al,
2009 | 8 | 9m | p.R173H | Maternal | (5) |
| Varga et al,
2009 | 9 | 9m | c.IVS8-2A>G | Paternal | (5) |
| Vanderver et
al, 2014 | 10 | 10m | c.A80G :
p.Y27C | de novo | (14) |
| Vanderver et
al, 2014, Bhargava et al, 2014 and Rodríguez-Escudero
et al, 2011 | 11 | 10m | c.G131A :
p.G44D | ND | (14,15,16) |
| Vanderver et
al, 2014 and Nelen et al, 1997 | 12 | 10m | c.C388T :
p.R130* | ND | (14,17) |
| Vanderver et
al, 2014 | 13 | 10m | c.C511G :
p.Q171E | Familial | (14) |
| Vanderver et
al, 2014 and Eng, 2003 | 14 | 10m | c.C633G :
p.C211W | Familial | (14,18) |
| Herman et
al, 2007 and Vanderver et al, 2014 | 15 | 10m | c.C1003T :
p.R335* | de novo | (4,14) |
| Vanderver et
al, 2014 | 16 | 11m | c.A16G : p.K6E | ND | (14) |
| Vanderver et
al, 2014 | 17 | 11m | c.G853T :
p.G285* | de novo | (14) |
| Vanderver et
al, 2014 | 18 | 12m | c. A320G :
p.D107G | ND | (14) |
| Vanderver et
al, 2014 | 19 | 1y3m | c.C138G :
p.Y46* | ND | (14) |
| Herman et
al, 2007 and Varga et al, 2009 | 20 | 1y4m | c.520insT | de novo | (4,5) |
| Tan et al,
2011 and Vanderver et al, 2014 | 21 | 1y6m | c.A45T :
p.R15S | de novo | (11,14) |
| Hansen-Kiss et
al, 2017 | 22 | 1y6m | c.G1004A :
p.R335Q | Paternal | (19) |
| Varga et al,
2009 | 23 | 1y8m | p.T202I | de novo | (5) |
| Vanderver et
al, 2014 and Eng, 2003 | 24 | 2y | c.T959G :
p.L320* | ND | (14,18) |
| Hansen-Kiss et
al, 2017 | 25 | 2y | c.607_608delAT :
p.L230* | Maternal | (19) |
| Hansen-Kiss et
al, 2017 | 26 | 2y | c.A667T :
p.K223* | ND | (19) |
| Varga et al,
2009 | 27 | 2y3m | p.G44D | ND | (5) |
| Butler et
al, 2005 | 28 | 2y6m | p.F241S | ND | (20) |
| Bhargava et
al, 2014 | 29 | 2y7m | No protein | ND | (15) |
| Bhargava et
al, 2014 | 30 | 2y8m | No protein | ND | (15) |
| Table IIClinical characteristics of 30
patients diagnosed as having PTEN mutation at <3 years old. |
Table II
Clinical characteristics of 30
patients diagnosed as having PTEN mutation at <3 years old.
| | | | Growth | Neurological
findings | Physical
features |
|---|
| Case no. | Age | Sex | MC | MS | MR | AS | Hypo-tonia | Facial
features | Nevus and
hamartoma/tumor | Others |
|---|
| 1 | 0d | M | + | + | +a | | | +i | | Postaxial
polydactyly |
| 2 | 3m | F | + | | +b | | + | | | |
| 3 | 5m | M | + | | + | +e | + | +i | Pigmented speckled
macules of the glans penis | |
| 4 | 7m | F | + | | + | | + | +i | | |
| 5 | 7m | M | + | | + | | | | Café-au-lait spot,
thyroid, nodules testicular hamartomas, rectal and gastric
polyps | |
| 6 | 8m | M | + | + | + | | | | | |
| 7 | 8m | M | + (2.8 SD) | + | + | +f | | | Café-au-lait spot,
subcutaneous lipomas | |
| 8 | 9m | M | + (4.4 SD) | | + | | | | | |
| 9 | 9m | M | + (3.5 SD) | | + | | | +j | | |
| 10 | 10m | F | + | | + | | + | | | Abnormal EEG but no
seizures |
| 11 | 10m | M | + | | +c | | | +i | | |
| 12 | 10m | F | + | | + | | + | +k | | |
| 13 | 10m | F | + | | + | + | + | +i | | Left cataract |
| 14 | 10m | M | + | | + | +g | | | | |
| 15 | 10m | F | + | | + | | | +i | Abdomen and axillar
trichilemmomas, subcutaneous lipomas | Split uvula |
| 16 | 11m | F | + | | + | | + | | | |
| 17 | 11m | F | + | | + | | + | +i | Mucosal
neuroma | |
| 18 | 1 m | M | + | | + | | + | +k | | |
| 19 | 1y3m | F | + | | + | | | | | |
| 20 | 1y4m | F | + (5.8 SD) | | + | +h | | | | |
| 21 | 1y6m | M | + | | + | | | | | |
| 22 | 1y6m | F | + (2.6 SD) | | + | | | | Dermalogical
features, BRRS |
| 23 | 1y8m | M | + (6.5 SD) | | + | | | | | |
| 24 | 2y | M | + | | + | + | + | +l | | |
| 25 | 2y | F | + (6.5 SD) | | + | | | | BRRS | |
| 26 | 2y | F | + (4.7 SD) | | + | | | | | |
| 27 | 2y3m | F | + (5.0 SD) | | + | | | | Large café-au-lait
spots on chest and abdomen | Bilateral
hernia |
| 28 | 2y6m | M | + (4.5 SD) | | + | + | | | Freckles on the
glans penis moles, thyroid nodules, intestinal polyps | |
| 29 | 2y7m | M | + | | + | | | | | |
| 30 | 2y8m | M | + | | +d | + | | | | |
All the 30 patients with macrocephaly in Table I showed no apparent
genotype-phenotype correlation nor malignant tumors that are
frequently observed in patients with CS. The risk of developing
malignant tumors in later years is not clear, without follow-up
data.
Tan et al (21) reported lifetime cancer risks of
individuals with PTEN germline mutation listing a variety of
cancers (breast, thyroid, endometrial, colorectal, renal cell, and
melanoma) found in a cohort of 368 children and adults aged 0.4-83
years (median age; 39 years). The earliest age of cancer onset
reported was 3 years for melanoma. In this paper, no follow-up
analysis from childhood to adulthood was reported. Consequently, it
is not clear as to how many infant macrocephaly cases with
PTEN mutation developed to CS in adulthood. Smpokou et
al (22) reported that, in the
case of a 7-year-old patient with a thyroid cancer, clinical
description would allow better formulation of clinical guidelines
in children with PHTS. For infant patients with PTEN
mutation, pediatricians have tendency to focus attention on
macrocephaly, developmental delay or autism. It is therefore
important to conduct follow-up assessment for both developmental
problem and cancer incidence, and carry out lifelong and total
medical management.
On this basis, we conducted thyroid ultrasonography
of our patient at the age of 2 years and 10 months, 4 years and 5
years of age and found no abnormality. Regarding gastrointestinal
tract hamartomas, we did not perform endoscopic examination, since
there have been no reports on the onset in childhood. We examined
breasts only by inspection and palpation since the possibility of
breast cancer was considered to be lower for male infant patients
than female (23).
Lipomas and a café-au-lait spot on the skin were
also found in our case. Our immunohistochemical examination
revealed that lipoma tissue and the skin tissue obtained from a
control subject showed very similar PTEN expression. No obvious
differences in PTEN expression were detected among them, suggesting
that two-hit in the PTEN gene by loss of heterozygosity was
unlikely even in the rapidly growing lipoma. A previous report
shows that loss of heterozygosity of markers in endometrial cancer,
glioblastoma, and breast cancer (13). In our lipoma case, we are unable to
do the immunohistochemical evaluation clearly.
To relieve psychosocial anxiety for PHTS patients
and their parents with respect to cancer predisposition and
developmental problems, genetic counseling is of need. Genetic
counseling is also of use for family members who may feel at risk.
Taken together, long-term follow-up plans for soft-tissue tumors,
thyroid cancer, breast cancer and GI-hamartomas, as well as
psychosocial problems are indispensable.
Acknowledgements
The authors would like to thank Dr Ai Takada
(Department of Human Genetics, Yokohama City University Graduate
School of Medicine, Yokohama, Japan) and Ms Yasuko Takahata
(Department of Genetic Medicine, Takatsuki General Hospital, Osaka,
Japan) for their help in this study and ethical board tasks.
Funding
The present study was supported grants by AMED
(grant nos. JP18ek0109280, JP18dm0107090, JP18ek0109301,
JP18ek0109348 and JP18kk020500), JSPS KAKENHI (grant nos.
JP17H01539 and JP17K10080; to NM) and Kawano Masanori Memorial
Public Interest Incorporated Foundation for Promotion of Pediatrics
(to SM).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YY wrote the manuscript. YY, AH and JT acquired the
patient data and contributed clinical advice. YI pathologically
diagnosed the patient and wrote the manuscript. HU evaluated the
images. SM, NM and YK performed genetic analysis. THT performed
genetic counseling and revised the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Gene analysis was conducted with approval of Ethical
Review Board of Takatsuki General Hospital (IRB no. 2012-8).
Histological analysis was conducted after obtaining approval of
Ethical Review Board of Takatsuki General Hospital (IRB No.
2017-25).
Patient consent for publication
Informed consent was obtained from a parent of the
patient for the publication of the case details and any associated
images since the patient was a child.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Li J, Yen C, Liaw D, Podsypanina K, Bose
S, Wang SI, Puc J, Miliaresis C, Rodgers L, McCombie R, et al:
PTEN, a putative protein tyrosine phosphatase gene mutated in human
brain, breast, and prostate cancer. Science. 275:1943–1947.
1997.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Teng DH, Hu R, Lin H, Davis T, Iliev D,
Frye C, Swedlund B, Hansen KL, Vinson VL, Gumpper KL, et al:
MMAC1/PTEN mutations in primary tumor specimens and tumor cell
lines. Cancer Res. 57:5221–5225. 1997.PubMed/NCBI
|
|
3
|
Eng C: PTEN hamartoma tumor syndrome. Gene
reviews https://www.ncbi.nlm.nih.gov/books/NBK1488/
Accessed 1 March 2017.
|
|
4
|
Herman GE, Butter E, Enrile B, Pastore M,
Prior TW and Sommer A: Increasing knowledge of PTEN germline
mutations: Two additional patients with autism and macrocephaly. Am
J Med Genet A = 143A. 589–593. 2007.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Varga EA, Pastore M, Prior T, Herman GE
and McBride KL: The prevalence of PTEN mutations in a clinical
pediatric cohort with autism spectrum disorders, developmental
delay, and macrocephaly. Genet Med. 11:111–117. 2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kurek KC, Howard E, Tennant LB, Upton J,
Alomari AI, Burrows PE, Chalache K, Harris DJ, Trenor CC III, Eng
C, et al: PTEN hamartoma of soft tissue: A distinctive lesion in
PTEN syndromes. Am J Surg Pathol. 36:671–87. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
NCCN Clinical Practice Guidelines in
OncologyVersion 3. 2019 Cowden syndrome/PHTS. NCCN Guidelines®:
https://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf.
Accessed 8 May 2019.
|
|
8
|
Society for the Kyoto scale of
psychological development test. Shinpan K Shiki Hattatsu Kensahou
2001 Nenban (The Kyoto Scale of Psychological Development Test
2001). Kyoto, Japan: Nakanishiya Shuppan, 2008.
|
|
9
|
Iwama K, Osaka H, Ikeda T, Mitsuhashi S,
Miyatake S, Takata A, Miyake N, Ito S, Mizuguchi T and Matsumoto N:
A novel SLC9A1 mutation causes cerebellar ataxia. J Hum Genet.
63:1049–1054. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
D'Gama AM, Pochareddy S, Li M, Jamuar SS,
Reiff RE, Lam AN, Sestan N and Walsh CA: Targeted DNA sequencing
from autism spectrum disorder brains implicates multiple genetic
mechanisms. Neuron. 88:910–917. 2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tan MH, Mester J, Peterson C, Yang Y, Chen
JL, Rybicki LA, Milas K, Pederson H, Remzi B, Orloff MS and Eng C:
A clinical scoring system for selection of patients for PTEN
mutation testing is proposed on the basis of a prospective study of
3042 probands. Am J Hum Genet. 88:42–56. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bermúdez Brito M, Goulielmaki E and
Papakonstanti EA: Focus on PTEN regulation. Front Oncol.
5(166)2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Perren A, Weng LP, Boag AH, Ziebold U,
Thakore K, Dahia PL, Komminoth P, Lees JA, Mulligan LM, Mutter GL
and Eng C: Immunohistochemical evidence of loss of PTEN expression
in primary ductal adenocarcinomas of the breast. Am J Pathol.
155:1253–1260. 1999.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Vanderver A, Tonduti D, Kahn I, Schmidt J,
Medne L, Vento J, Chapman KA, Lanpher B, Pearl P, Gropman A, et al:
Characteristic brain magnetic resonance imaging pattern in patients
with macrocephaly and PTEN mutations. Am J Med Genet A.
164A:627–633. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Bhargava R, Au Yong KJ and Leonard N:
Bannayan-Riley-Ruvalcaba syndrome: MRI neuroimaging features in a
series of 7 patients. Am J Neuroradiol. 35:402–406. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Rodríguez-Escudero I, Oliver MD,
Andrés-Pons A, Molina M, Cid VJ and Pulido R: A comprehensive
functional analysis of PTEN mutations: Implications in tumor- and
autism-related syndromes. Hum Mol Genet. 20:4132–4142.
2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Nelen MR, van Staveren WC, Peeters EA,
Hassel MB, Gorlin RJ, Hamm H, Lindboe CF, Fryns JP, Sijmons RH,
Woods DG, et al: Germline mutations in the PTEN/MMAC1 gene in
patients with Cowden disease. Hum Mol Genet. 6:1383–1387.
1997.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Eng C: PTEN: One gene, many syndromes. Hum
Mutat. 22:183–198. 2003.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hansen-Kiss E, Beikampen S, Adler B,
Frazier T, Prior T, Erdman S, Eng C and Herman G: A retrospective
chart review of the features of PTEN hamartoma tumour syndrome in
children. J Med Genet. 54:471–478. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Butler MG, Dasouki MJ, Zhou XP,
Talebizadeh Z, Brown M, Takahashi TN, Miles JH, Wang CH, Stratton
R, Pilarski R and Eng C: Subset of individuals with autism spectrum
disorders and extreme macrocephaly associated with germline PTEN
tumour suppressor gene mutations. J Med Genet. 42:318–321.
2005.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Tan MH, Mester JL, Ngeow J, Rybicki LA,
Orloff MS and Eng C: Lifetime cancer risks in individuals with
germline PTEN mutations. Clin Cancer Res. 18:400–407.
2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Smpokou P, Fox VL and Tan WH: PTEN
hamartoma tumour syndrome: Early tumour development in children.
Arch Dis Child. 100:34–37. 2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Pilarski R: PTEN hamartoma tumor syndrome:
A clinical overview. Cancers (Basel). 11(E844)2019.PubMed/NCBI View Article : Google Scholar
|