Introduction
Postoperative chylothorax after esophagectomy is a
relatively rare complication with a reported incidence rate ranging
from 1.1 to 3.9% (1). However, once
it occurs, chylothorax can lead to serious complications such as
significant impairment of the cardiovascular and respiratory
systems, nutritional status, and immune system unless appropriately
treated (2,3). Treatment of chylothorax includes
conservative treatment and surgical treatment. Conservative
treatment including total parenteral nutrition, no enteral intake,
and octreotide is initially chosen, but if the chylothorax is not
improved, surgical treatment is often required (4). However surgical treatment may be highly
invasive for patients with postope-rative chylothorax who are
frequently in a poor nutritional and immunosuppressive condition,
and lymphangiography must be considered before surgical treatment.
Although the traditional lymphangiography procedure uses a
bilateral pedal approach (5), recent
studies have suggested the use of ultrasound-guided intranodal
lymphangiography because of its simplicity and safety (6,7).
Intranodal lymphangiography involving inguinal lymph node puncture
is a feasible and useful treatment in terms of not only the way in
which it helps determine the site of chyle leakage but also as an
effective therapeutic modality for treating chylothorax.
The purpose of this study is to clarify the efficacy
of lymphangiography for chyle leakage. We herein report three cases
of esophagectomy complicated by chyle leakage. In two of them,
lymphangiography visualized the movement of the thoracic duct and
clearly depicted its positional relationship with other organs
which lead to appropriate surgical treatment. In one case, chyle
leakage was successfully treated by lymphangiography as
embolization of micro-injury in thoracic duct.
Case report
Case 1
A 67-year-old man was diagnosed as having middle
thoracic esophageal squamous cell carcinoma of cT3N1M0 cStage IIIA
(UICC 8th edition). He underwent radical esophagectomy by
video-assisted thoracic surgery (VATS) following 2 cycles of
neoadjuvant biweekly-DCF chemotherapy (docetaxel 35
mg/m2 on days 1 and 15; cisplatin 40 mg/m2 on
days 1 and 15; and 5-FU 400 mg/m2/day on days 1-5 and
15-19; Bi-DCF). Operation time was 515 min, blood loss was 145 g,
and the thoracic duct was preserved. After enteral feeding was
started on postoperative day (POD) 2, right pleural effusion
drainage increased to 1,360 ml daily and changed to a milky white
color. The patient then was diagnosed as having postoperative
chylothorax. After conservative treatment including fat restriction
was started on the same day, the chylothorax improved for a few
days. However, he complained of breathing difficulties after
enteral nutrition that included added fat. Re-exacerbation of the
chylothorax up to 1,500 ml daily was observed on POD 15, and
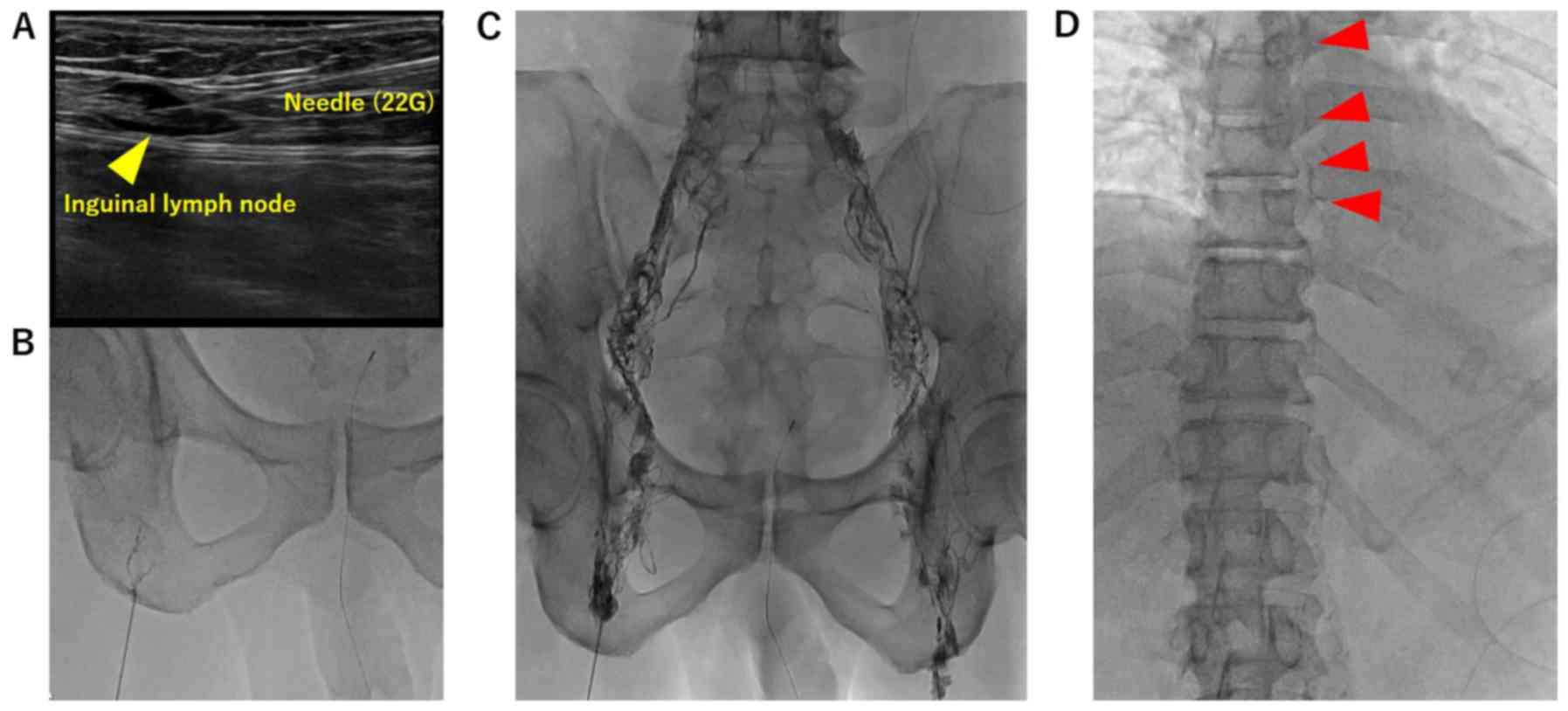
conservative treatment was started once again. On POD 50,
ultrasound-guided intranodal Lipiodol lymphangiography involving
inguinal lymph node puncture (Fig.
1) was performed that revealed Lipiodol leakage 4 cm on the
caudal side of the tracheal bifurcation along the thoracic duct
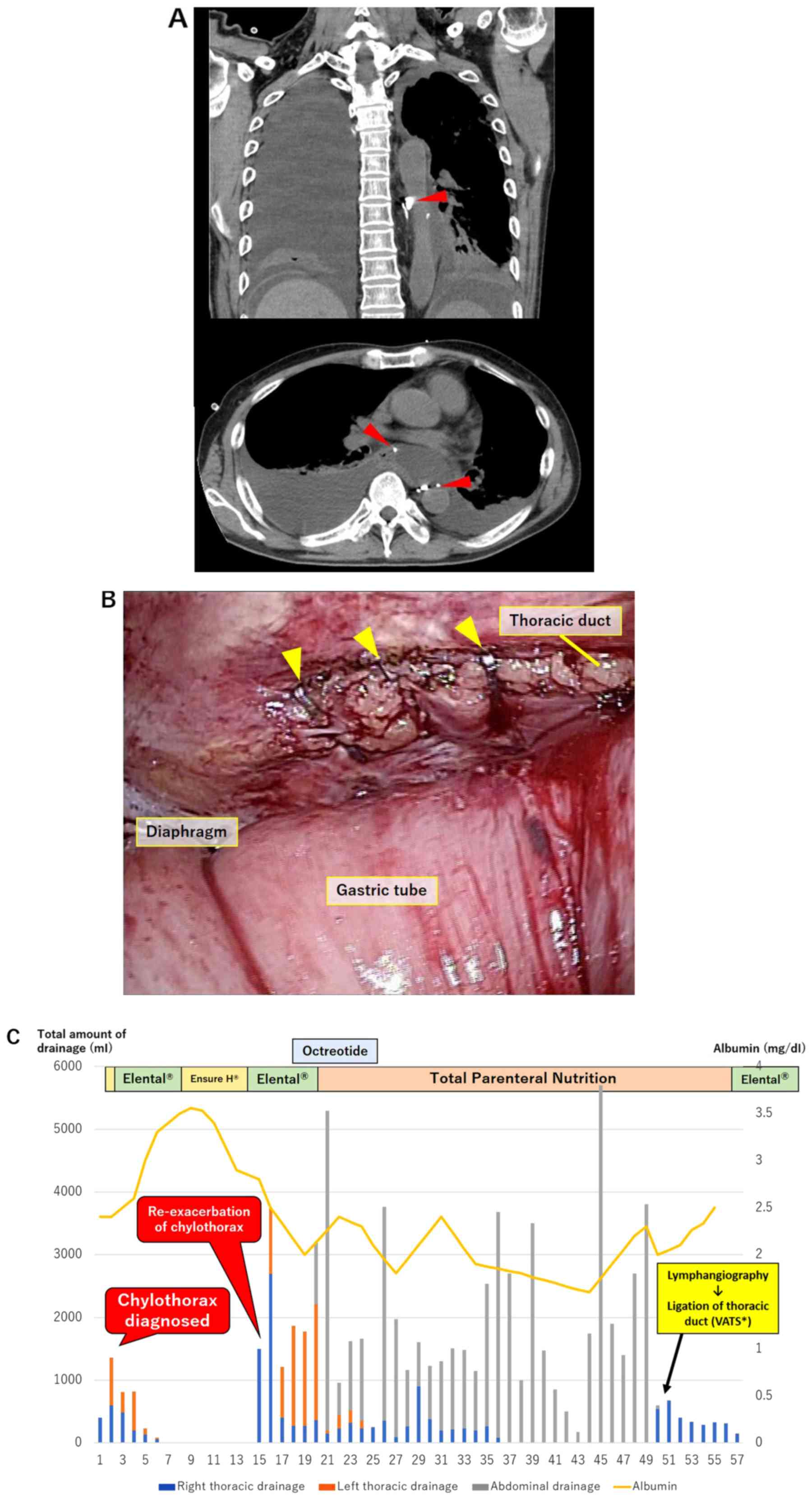
(Fig. 2A). Ligation of the thoracic
duct by VATS was performed following the lymphangiography. Thoracic
duct was identified in the lower mediastinum, and clipping was
performed on the caudal side of the injured part (Fig. 2A). The patient's chylothorax improved
completely by the next day, and the right thoracic drain was
removed 7 days after the operation (Fig.
2C).
Case 2
A 69-year-old man was diagnosed as having lower
esophageal squamous cell carcinoma of cT3N3M0 cStage IIIC (UICC 8th
edition). He was initially started on chemoradiotherapy (radiation
2 Gy for 30 days and 2 cycles of Bi-DCF). Although remarkable tumor
shrinkage was obtained initially, the tumor relapsed 5 months
later. Therefore, esophagectomy was performed as a salvage
operation. Operation time was 367 min, blood loss was 260 g, and
the thoracic duct was preserved. After enteral feeding was started
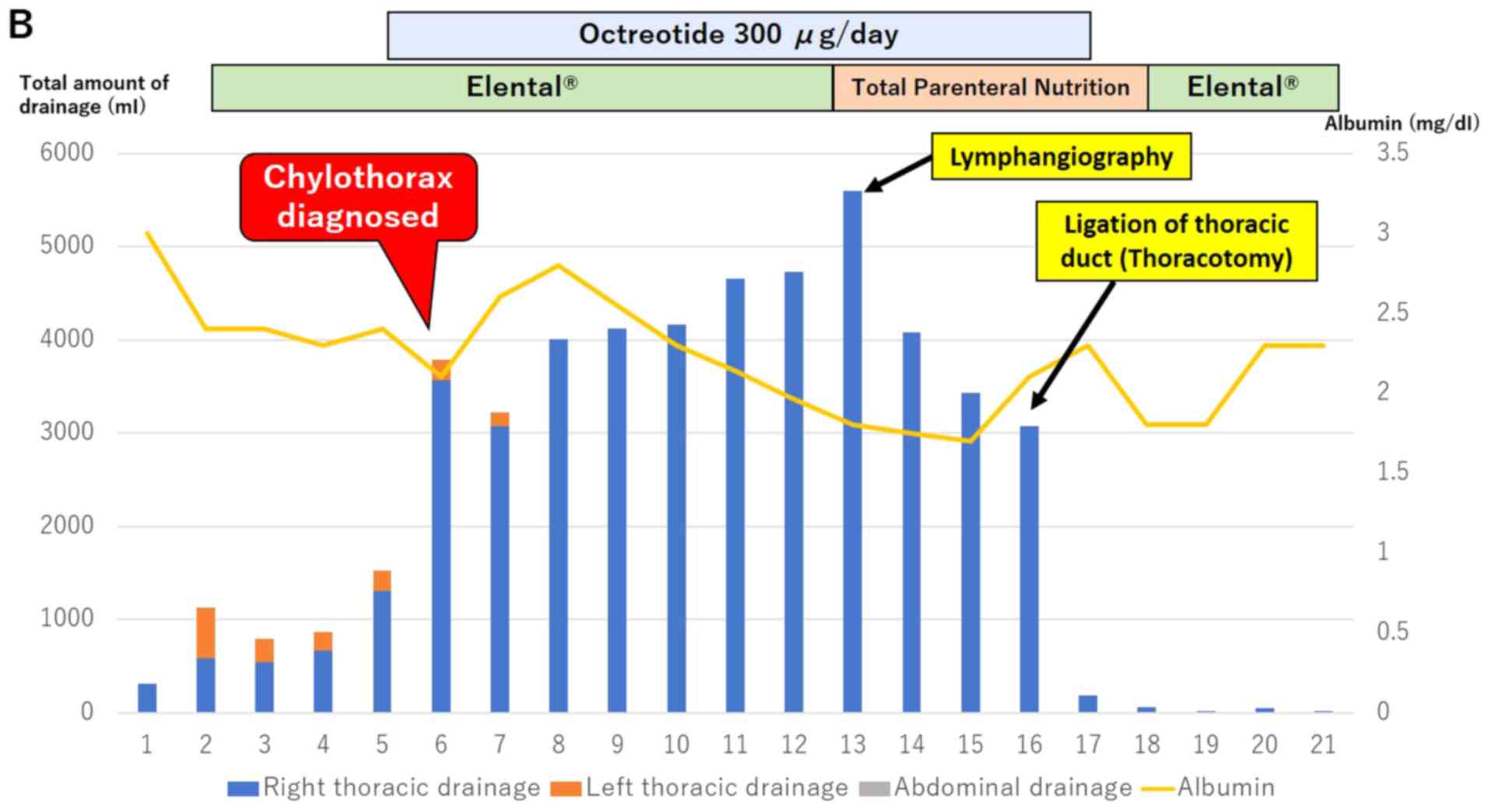
on POD 3, right pleural effusion drainage increased to 3,790 ml on
POD 6 and chylothorax was diagnosed. The patient was started on
conservative treatment, but the volume of pleural fluid did not
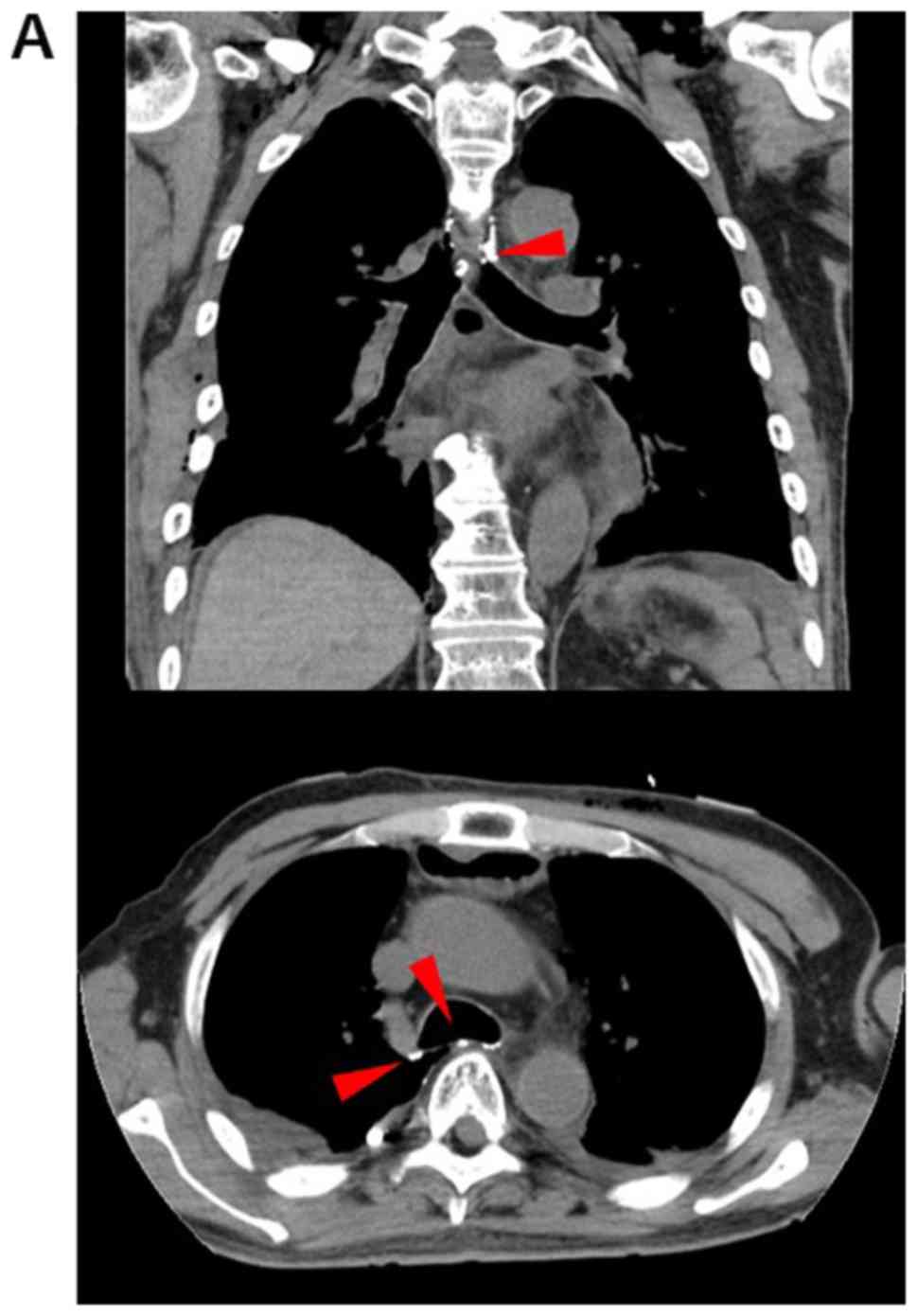
decrease. Intranodal Lipiodol lymphangiography was performed on POD
13, and contrast medium was observed draining from the thoracic
duct near the tracheal bifurcation (Fig.
3A). We performed a thoracotomy on POD 15 for ligation of the
thoracic duct. Thereafter, the volume of drainage from the thoracic
drain decreased significantly, and the right thoracic drain was
removed 5 days after the operation (Fig.
3B).
Case 3
A 65-year-old man was diagnosed as having
hypopharyngeal squamous cell carcinoma of cT4aN0M0 cStage IVA (AJCC
Cancer Staging Manual 8th edition) and upper thoracic esophageal
squamous cell carcinoma of cT3N1M0 cStage IIIA (UICC 8th edition).
He underwent total pharyngopharyngeal esophagectomy by VATS
following 1 cycle of neoadjuvant chemotherapy (NAC) (cisplatin 80
mg/m2 on days 1 and 5-FU 800 mg/m2 on days
1-5). Operation time was 755 min, blood loss was 620 g, and the
thoracic duct was preserved. Enteral feeding was started on POD 4,
but ascites fluid appeared from the upper wound edge on POD 5.
Besides, the pleural fluid increased to 3,140 ml and turned white
color on POD7. He was diagnosed as having postoperative chylothorax
on the same day. Although he was started on conservative treatment,
the volume of pleural fluid did not decrease. After cessation of
enteral nutrition on POD 13, pleural effusion gradually decreased,
but due to concerns about re-enhancing pleural effusion following
resumption of nutrition, intranodal lymphangiography was performed
on POD 19. The thoracic duct was completely visualized and showed
small outflow of Lipiodol contrast into the mediastinum from the
thoracic duct (Fig. 4A). The volume
of pleural fluid decreased and there was no re-progression after
lymphangiography. All drainage tubes were removed 8 days after the
procedure (Fig. 4B).
Discussion
The cause of chylothorax as a postoperative
complication after surgery for esophageal cancer appears to be
thoracic duct injury associated with the surgical intervention.
Furthermore, an increased incidence of postoperative chylothorax
has recently been reported most notably following increasingly
radical procedures that are performed after neoadjuvant
chemoradiotherapy (8).
Although the thoracic duct can have a variable
course, it is usually detected at the level of the diaphragm where
it passes through the aortic hiatus with the aorta and azygous vein
in the posterior mediastinum. The thoracic duct then continues its
course between the aorta and azygos vein and crosses to the left
side of the body at either the fifth or sixth thoracic vertebra. The
thoracic duct runs posterior to the aortic arch and next to the
esophagus until it drains into the junction of the left subclavian
and internal jugular veins, where lymph enters the systemic
circulation (9).
Two of our three patients received preoperative
chemo-therapy and one received preoperative chemoradiotherapy.
According to the esophageal cancer treatment guidelines in Japan,
combined therapy with cisplatin and 5-FU is standard preoperative
chemotherapy (10), but the
effectiveness of triplet regimens has also been reported (11-13).
At our institution, Bi-DCF therapy is used as a potent triple
regimen for preoperative chemotherapy, and a 90.3% response rate is
reported (14). There is a report of
increased postoperative chylothorax following chemoradiotherapy
(8), and we have also experienced
one case, but it is also possible that postoperative chylothorax is
likely to occur in cases in which a tumor located beside the
thoracic duct shrinks significantly due to effective NAC.
An early indication of chylothorax includes a daily
chest tube output of more than 400 ml. Besides, chylothorax is
readily diagnosed by the detection of milky white fluid draining
from the chest after the initiation of enteral nutrition. High
triglyceride levels and the demonstration of Sudan III-stained fat
droplets in the pleural effusion are also diagnostic factors.
Triglyceride values >110 mg/dl are highly suggestive of a
chylous effusion (15).
The thoracic duct transports between 1.5 and 4 l of
chyle per day back into the bloodstream in a normal adult.
Hypovolemia may be present due to intravascular volume depletion.
Electrolyte imbalance following chylothorax can also result in
metabolic acidosis, hyponatremia, or hypocalcemia. In addition, the
loss of proteins, fat-soluble vitamins, lipids, and electrolytes
leads to nutritional deficiency. A decrease in cellular and humoral
immunity (hypogammaglo-bulinemia) ultimately leaves the patient
immunosuppressed and susceptible to infection and sepsis (16). The greater the duration of chyle
leakage, the greater are the detrimental effects, and thus the need
for urgent treatment.
Initial treatment of chylothorax is usually
conservative and includes fat restriction, fasting, and total
parenteral nutrition to reduce the flow of lymph fluid. In
addition, albumin supplementation is also examined for malnutrition
due to the loss of lymph fluid.
The effectiveness of the administration of
octreotide, a long-acting somatostatin analogue, was also reported
in the treatment of chylothorax (17). If the patient does not show signs of
improvement, lymphangiography is considered before surgical
therapy.
Recently, several studies showed good outcomes
following interventional radiology embolization of the thoracic
duct using a vascular coil or lipid material (5). Itkin et al (5) reported that the cure rate was 71% in
109 patients who needed treatment for chylothorax due to thoracic
duct injuries while safety was maintained. Besides, to reduce
invasiveness and ensure safety, intranodal lymphangiography
involving inguinal lymph node puncture was reported to be a
feasible and useful treatment for patients (6,7).
If conservative treatment fails, surgical treatment
is often considered. Direct thoracic duct ligation via VATS and
open surgery are popular and successful means of resolving
postoperative chylothorax. However, indications and timing for
surgical treatment are controversial. Some authors recommend
ligation of the thoracic duct when the amount of chylous drainage
exceeds 1,000 ml for >7 days (18,19).
Miao et al (4) reported
medical management was more likely to fail in patients who had
chest tube drainage volume of more than 13.5 ml/kg on the third day
after initiation of conservative treatment.
In this study, though one patient showed improvement
of his chylothorax after lymphangiography, the other two patients
required surgical treatment. In case 1, the amount of pleural
effusion varied greatly, and even though it seemed to have improved
once, the course that the amount of drainage increased the next day
was repeated. The decision to perform lymphangiography was delayed.
There was also a gradual decrease in nutrition, and the contrast
medium did not stay in the damaged area when lymphangiography was
performed, and the contrast medium through thoracic duct flowed out
to the intrathoracic cavity. It was judged that lymphangiography
alone was inadequate. Besides, this patient was originally
performed esophagectomy by VATS, and thoracic duct ligation with
VATS was deemed appropriate. In case 2, due to radical
chemoradiotherapy and salvage operation, his capacity to receive
the treatment was declining when he diagnosed chylothorax.
Therefore, conservative treatment with simultaneous enteral
nutrition excluding fat was considered. However, there is no
improvement of chylothorax exceeding 3,000 ml daily for a week and
lymphangiography was performed. Lymphangiography showed that the
contrast medium though thoracic duct flowed out to the
intrathoracic cavity similar to case 1. He was performed thoracic
duct ligation in a few days. On the other hand, in case 3,
lymphangiography was performed when pleural effusion was decreasing
<1,000 ml daily. Contrast medium from the thoracic duct remained
in the mediastinum around the leak point. Considering these cases,
large amount of pleural effusion over 1,000 ml daily and the
flowing out of contrast medium to intrathoracic cavity seem to be
indications to required surgical treatment despite performing
lymphangiography.
Lymphangiography was performed without complications
in all cases. Improvement in nutritional status and serum albumin
level was observed after chylothorax treatment.
In conclusion, ultrasound-guided intranodal Lipiodol
lymphangiography involving inguinal lymph node puncture not only
helps to determine the site of chyle leakage but can also be
effective for curing chylothorax. Besides, poor improvement with
conservative treatment, including lymphangiography, are good
indications for surgical treatment. Safe and appropriate treatment
for postoperative chylothorax following esophagectomy needs to be
established.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
TS and YoT contributed to study conception and
design. TS, YoT, SB, MF, IY, YI, TI, ToT, SM, HI, NM, TaT, KYa,
YuT, HK and MM contributed to the acquisition of data. TS and YoT
contributed to the analysis and interpretation of data, and drafted
the manuscript. TS, YoT and KYo critically revised the manuscript.
KYo supervised the study.
Ethics approval and consent to
participate
Informed consent for participation in the study or
use of their tissue was obtained from the patients.
Patient consent for publication
Written informed consent was obtained from each
patient for publication of this case report and accompanying
images.
Competing interests
K. Yoshida has received grants, personal fees and
nonfinancial support from Chugai Pharmaceutical Co., Ltd. during
the conduction of the study; grants and personal fees from Taiho
Pharmaceutical Co., Ltd., Pfizer Inc., and Yakult Honsha Co., Ltd.;
grants from Bristol-Myers Squibb; grants from Kyowa Hakko Kirin
Co., Ltd. outside the submitted work; honoraria from Taiho
Pharmaceutical Co., Ltd., Pfizer Inc., Chugai Pharmaceutical Co.,
Ltd., Kyowa Hakko Kirin Co., Ltd., and Yakult Honsha Co., Ltd.; and
had a consultant or advisory relationship with Taiho Pharmaceutical
Co., Ltd. and La Roche, Ltd. T. Takahashi has received honoraria
for lectures from Takeda Pharmaceutical Co., Ltd. All remaining
authors declare that they have no competing interests.
References
|
1
|
Merigliano S, Molena D, Ruol A, Zaninotto
G, Cagol M, Scappin S and Ancona E: Chylothorax complicating
esophagectomy for cancer: A plea for early thoracic duct ligation.
J Thorac Cardiovasc Surg. 119:453–457. 2000.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Merrigan BA, Winter DC and O'Sullivan GC:
Chylothorax. Br J Surg. 84:15–20. 1997.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lagarde SM, Omloo JM, de Jong K, Busch OR,
Obertop H and van Lanschot JJ: Incidence and management of chyle
leakage after esophagectomy. Ann Thorac Surg. 80:449–454.
2005.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Miao L, Zhang Y, Hu H, Ma L, Shun Y, Xiang
J and Chen H: Incidence and management of chylothorax after
esophagectomy. Thorac Cancer. 6:354–358. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Itkin M, Kucharczuk JC, Kwak A, Trerotola
SO and Kaiser LR: Nonoperative thoracicductembolization for
traumatic thoracicduct leak: Experience in 109 patients. J Thorac
Cardiovasc Surg. 139:584–589. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nadolski GJ and Itkin M: Feasibility of
ultrasound-guided intranodal lymphangiogram for thoracic duct
embolization. J Vasc Interv Radiol. 23:613–616. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yamamoto M, Miyata H, Yamasaki M, Maeda N,
Miyazaki Y, Takahashi T, Kurokawa Y, Nakajima K, Takiguchi S, Mori
M and Doki Y: Chylothorax after esophagectomy cured by intranodal
lymphangiography: A case report. Anticancer Res. 35:891–895.
2015.PubMed/NCBI
|
|
8
|
Ohkura Y, Ueno M, Shindoh J, Iizuka T, Ka
H and Udagawa H: Risk factors for postoperative chylothorax after
radical subtotal esophagectomy. Ann Surg Oncol. 25:2739–2746.
2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Loukas M, Wartmann CT, Louis RG Jr, Tubbs
RS, Salter EG, Gupta AA and Curry B: Cisterna chyli: A detailed
anatomic investigation. Clin Anat. 20:683–688. 2007.PubMed/NCBI View
Article : Google Scholar
|
|
10
|
The Japan Esophageal Society: Guidelines
for Diagnosis and Treatment of Carcinoma of the Esophagus. Kanehara
Co Ltd., Tokyo, 2017.
|
|
11
|
Hara H, Tahara M, Daiko H, Kato K, Igaki
H, Kadowaki S, Tanaka Y, Hamamoto Y, Matsushita H, Nagase M and
Hosoya Y: Phase II feasibility study of preoperative chemotherapy
with docetaxel, cisplatin, and fluorouracil for esophageal squamous
cell carcinoma. Cancer Sci. 104:1455–1460. 2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Watanabe M, Baba Y, Yoshida N, Ishimoto T,
Nagai Y, Iwatsuki M, Iwagami S and Baba H: Outcomes of preoperative
chemotherapy with docetaxel, cisplatin, and 5-fluorouracil followed
by esophagectomy in patients with resectable node-positive
esophageal cancer. Ann Surg Oncol. 21:2838–2844. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yamashita K, Hosoda K, Moriya H, Katada C,
Sugawara M, Mieno H, Komori S, Katada N and Watanabe M: Prognostic
advantage of docetaxel/cisplatin/5-fluorouracil neoadjuvant
chemotherapy in clinical stage II/III esophageal squamous cell
carcinoma due to excellent control of preoperative disease and
postoperative lymph node recurrence. Oncology. 92:221–228.
2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tanaka Y, Yoshida K, Yamada A, Tanahashi
T, Okumura N, Matsuhashi N, Yamaguchi K and Miyazaki T: Phase II
trial of biweekly docetaxel, cisplatin, and 5-fluorouracil
chemotherapy for advanced esophageal squamous cell carcinoma.
Cancer Chemother Pharmacol. 77:1143–1152. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Staats BA, Ellefson RD, Budahn LL, Dines
DE, Prakash UB and Offord K: The lipoprotein profile of chylous and
nonchylous pleural effusions. Mayo Clin Proc. 55:700–704.
1980.PubMed/NCBI
|
|
16
|
Lai FC, Chen L, Tu YR, Lin M and Li X:
Prevention of chylothorax complicating extensive esophageal
resection by mass ligation of thoracic duct: A random control
study. Ann Thorac Surg. 91:1770–1774. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Fujita T and Daiko H: Efficacy and
predictor of octreotide treatment for postoperative chylothorax
after thoracic esophagectomy. World J Surg. 38:2039–2045.
2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Cerfolio RJ, Allen MS, Deschamps C,
Trastek VF and Pairolero PC: Postoperative chylothorax. J Thorac
Cardiovasc Surg. 112:1361–1365. 1996.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kranzfelder M, Gertler R, Hapfelmeier A,
Friess H and Feith M: Chylothorax after esophagectomy for cancer:
Impact of the surgical approach and neoadjuvant treatment:
Systematic review and institutional analysis. Surg Endosc.
27:3530–3538. 2013.PubMed/NCBI View Article : Google Scholar
|