Introduction
Bone and soft tissue sarcomas (BSTS) are connective
tissue malignancies arising from tissues of mesenchymal origin
(1). BSTS may occur in all age
groups. However, it is not common in adolescents and young adults
(AYAs) aged 15-39 years (2) with
these tumors comprising only 6-8% of all malignancies in AYAs
(3-5).
The mortality rates among AYAs with BSTS are high as these types of
cancer confer poorer prognoses than those of other types such as
Hodgkin's lymphoma, melanoma, or germ cell tumors (6). In AYA sarcomas also confer poorer
prognoses than in both, younger and older patients, irrespective of
the histological type (6-8).
However, data from clinical investigations of the outcomes of AYA
patients with BSTS are scarce (2,7-10).
In this study, we aimed to determine the survival
rates of AYAs with BSTS at the Kindai University Hospital and the
factors contributing to poorer prognosis in patients of this age
group.
Patients and methods
Patients
The records of 7 male patients and 6 female patients
aged 17-39 (mean: 34 years) with BSTS were reviewed retrospectively
between October 2009 and July 2017. Data on the size, histological
grade, location, stage, treatment modalities, local recurrence,
presence of metastasis, and final outcomes were recorded. The
resected specimens were stained with hematoxylin-eosin (H&E).
The histological grade was determined based on the four-point
grading system for bone tumors (11)
and the Federation Nationale des Centres de Lutte Contres le Cancer
grading system for soft tissue tumors (12).
This study was approved by the Ethics Committee of
Kindai University Hospital (approval no.: 31-153) (Osaka, Japan).
All patients also provided written informed consent for the
participation of this retrospective study.
Methods
The grading system for bone tumors, with the
exception of Ewing sarcoma, was based on a previously described
system (11). Tumors of grades 1-2
and 3-4 were considered as low- and high-grades, respectively.
Among soft tissue tumors, lesions of grades 1 and 2-3 were
classified as low- and high-grade, respectively. The clinical
staging was individually evaluated based on the American Joint
Committee on Cancer (AJCC) 7th edition for soft tissue tumors and
bone cancer (13,14). The mean follow-up period was 45
(range: 11-111 months). Surgery was aimed at achieving wide
surgical margins in all cases (Table
I: 11/13 cases). The surgical margins in resected specimens
were categorized as R0, R1, or R2, as previously classified
(15). The patients' 5-year survival
rates were calculated using the Kaplan-Meier method; and the 5-year
survival rates of younger (15-29 years) and older (≥30) patients,
as well as that of patients with bone vs. soft tissue sarcoma,
low-vs. high-grade tumors, and trunk-vs. extremity-located tumors
using log-rank tests.
 | Table IClinical features of patients with
sarcoma. |
Table I
Clinical features of patients with
sarcoma.
| Patient no. | Age (y)/Sex | Size (mm) | Bone or soft
tissue | Site | Histopathology | Grade | Stage | Treatment | Surgical margin | Local recurrence | Metastasis | Follow-up (Mo) | Outcome |
|---|
| 1 | 27/F | 85x36 | B | Sacrum | Osteosarcoma | High | III | CT, HPR | - | - | - | 11 | DOD |
| 2 | 32/M | 120x60 | S | Buttock | Ewing sarcoma | High | IV | WR, CT | R0 | - | + | 13 | DOD |
| 3 | 35/M | 21x8 | S | Knee | Synovial sarcoma | High | II | WR | R1 | - | - | 20 | CDF |
| 4 | 34/M | 94x62 | B | Pelvic | Ewing sarcoma | High | III | CT, HPR | - | - | + | 24 | DOD |
| 5 | 27/F | 45x36 | S | Side abdomen | Synovial
sarcoma | High | I | CT, WR | R0 | - | - | 36 | CDF |
| 6 | 17/M | 107x67 | B | Pelvic | Osteosarcoma | High | IVB | CT, WR | R1 | + | + | 43 | DOD |
| 7 | 35/F | 105x59 | S | Thigh | Leiomyosarcoma | High | II | CT, WR | R0 | - | | 45 | DOD |
| 8 | 36/F | 73x65 | B | Tibia | Osteosarcoma | Low | IIA | CT, MR | R2 | + | - | 54 | NED |
| 9 | 36/F | 13x13 | S | Upper arm | Myxoid
Liposarcoma | Low | II | WR | R0 | - | - | 54 | CDF |
| 10 | 39/M | 120x24 | B | Thigh | Chondrosarcoma | Low | I | WR | R0 | - | - | 63 | CDF |
| 11 | 26/F | 143x39 | S | Thigh | Myxoid
Liposarcoma | High | III | WR | R0 | - | - | 66 | CDF |
| 12 | 33/M | 44x21 | B | Femur | Chondrosarcoma | Low | I | MR | R0 | - | - | 72 | CDF |
| 13 | 34/F | 162x99 | S | Thigh | Myxoid
Liposarcoma | High | III | CT, WR | R1 | + | + | 111 | NED |
Statistical analysis
The Statmate 4.01 software package was used to
assess the 5-year survival rates. The patients' 5-year survival
rates were calculated using the Kaplan-Meier method and differences
were assessed using the log-rank test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patients and treatment
Seven and six patients had bone and soft tissue
sarcomas, respectively. Among those with bone sarcomas, four, two,
and one had osteosarcoma, chondrosarcoma, and Ewing sarcoma,
respectively; three had high-grade disease, while the tumors were
of low grades in the remainder. Among the six patients with soft
tissue sarcomas, three had myxoid liposarcoma, two had synovial
sarcoma, and one had Ewing sarcoma; six and one had high- and
low-grade disease, respectively (Table
I). Nine sarcomas were located in the lower limbs, three were
in the trunk, and one was in the upper limbs. Sarcomas in older
patients were staged according to the AJCC criteria: Stage I (n=3),
IIA (n=1), II (n=3), III (n=4), IV (n=1), and IVB (n=1). Lymph node
metastases were observed during the first examination in 1 case
(Table I; patient number 2). In
addition, lung metastasis had developed in 3 cases during treatment
(Table I; patient numbers 4, 6, and
13). A total of 11 patients underwent tumor resections (wide and
marginal in 9 and 2, respectively). The surgical margin status was
R0, R1, and R2 in 7, 3, and 1 cases, respectively (Table I). The remaining two patients did not
undergo surgery owing to difficulties in accessing the pelvic tumor
and extensive disease in 1 case each; these patients were treated
with 5-6 courses of chemotherapy according to the NECO-95J protocol
(16) and heavy-particle
radiotherapy (70 Gy) (n=2). Chemotherapy was selected for soft
tissue sarcomas that were exceptionally large or in close proximity
to vessels or nerves, precluding the achievement of wide margins;
chemotherapy was also administered in cases where the margin was
positive after surgery. We administered ifosfamide and doxorubicin
hydrochloride to all patients with myxoid liposarcoma, synovial
sarcoma, and leiomyosarcoma (17).
We also administered vincristine, doxorubicin, cyclophosphamide,
ifosfamide, and etoposide to patients with Ewing sarcoma (18). In cases of bone sarcoma, chemotherapy
was administered to patients with osteosarcoma according to the
NECO-95J protocol using the same dosage as that used for adults
(16). No lethal side-effects were
noted in any of the patients (Table
II).
| Table IIChemotherapy toxic effects, worst
grade per patient. |
Table II
Chemotherapy toxic effects, worst
grade per patient.
| Item | Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|
| Hematological | | | | | |
|
White blood
cells | 3 | 2 | 2 | 1 | 0 |
|
Neutrophils | 2 | 1 | 3 | 2 | 0 |
|
Platelets | 5 | 2 | 1 | 0 | 0 |
| Biochemical | | | | | |
|
Creatinine | 0 | 0 | 0 | 0 | 0 |
|
AST | 6 | 1 | 1 | 0 | 0 |
|
ALT | 6 | 1 | 1 | 0 | 0 |
| Clinical | | | | | |
|
Nausea | 2 | 2 | 2 | 0 | 0 |
|
Vomiting | 1 | 0 | 0 | 0 | 0 |
|
Diarrhoea | 1 | 0 | 0 | 0 | 0 |
|
Mucositis | 0 | 0 | 0 | 0 | 0 |
|
Alopecia | 1 | 3 | 1 | 0 | 0 |
|
Fever | 2 | 0 | 0 | 0 | 0 |
|
Infection | 0 | 0 | 0 | 1 | 0 |
|
Neurological | 0 | 0 | 0 | 0 | 0 |
|
Cardiac | 0 | 0 | 0 | 0 | 0 |
Recurrence
Two patients experienced local recurrence. No
evidence of disease (NED) status was maintained in 1 case after a
second resection of the osteosarcoma in the tibia 36 months after
the first marginal resection. This patient had undergone marginal
resection after being misdiagnosed with a giant cell tumor on
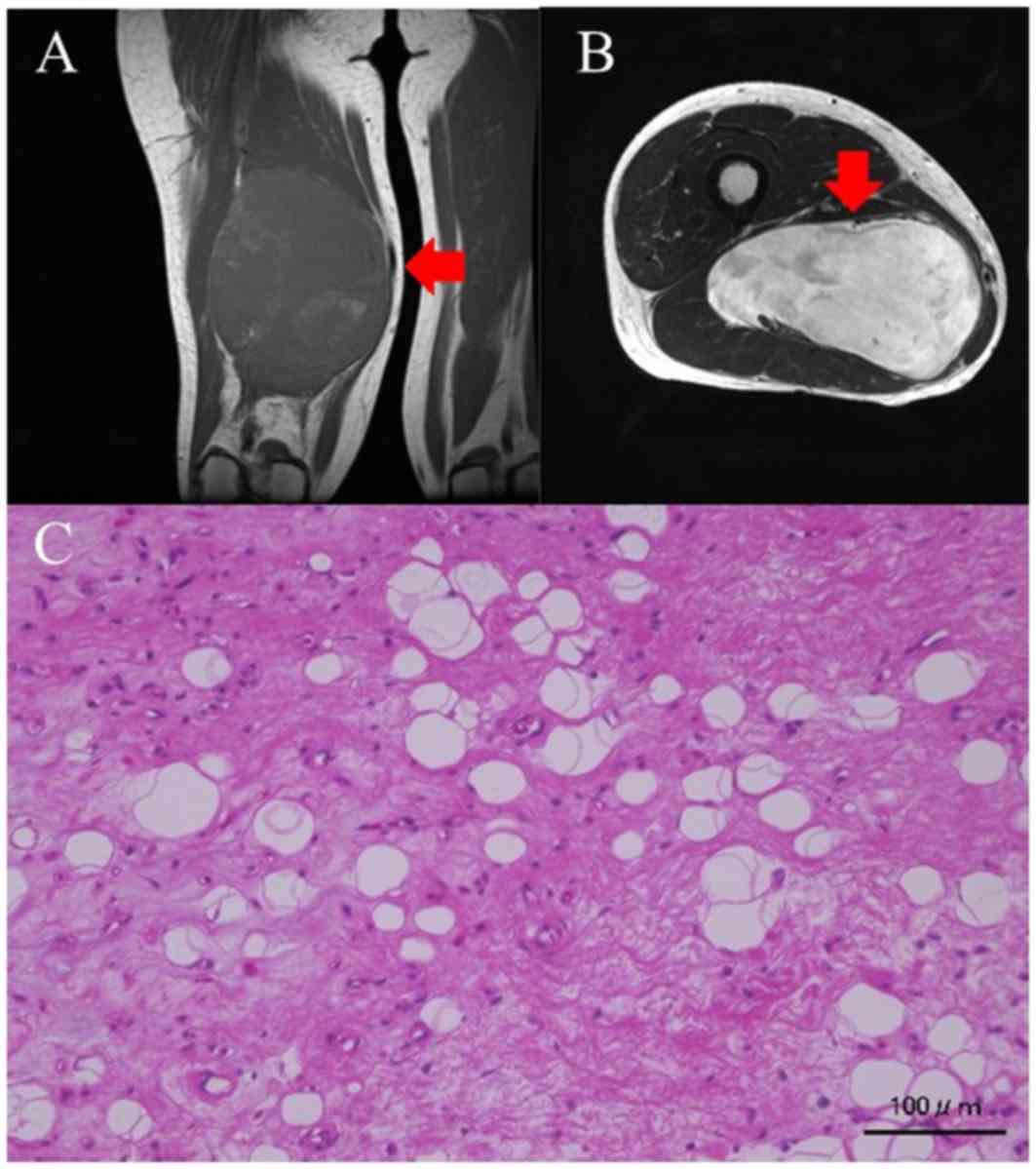
histological evaluation of the biopsy sample. The other patient had
a myxoid liposarcoma of the thigh that recurred 73 months after
wide- resection; this patient also achieved NED status after
undergoing a second resection. Images from her first MRI showed a
myxomatous tumor (Fig. 1A and
B). This was resected widely, and
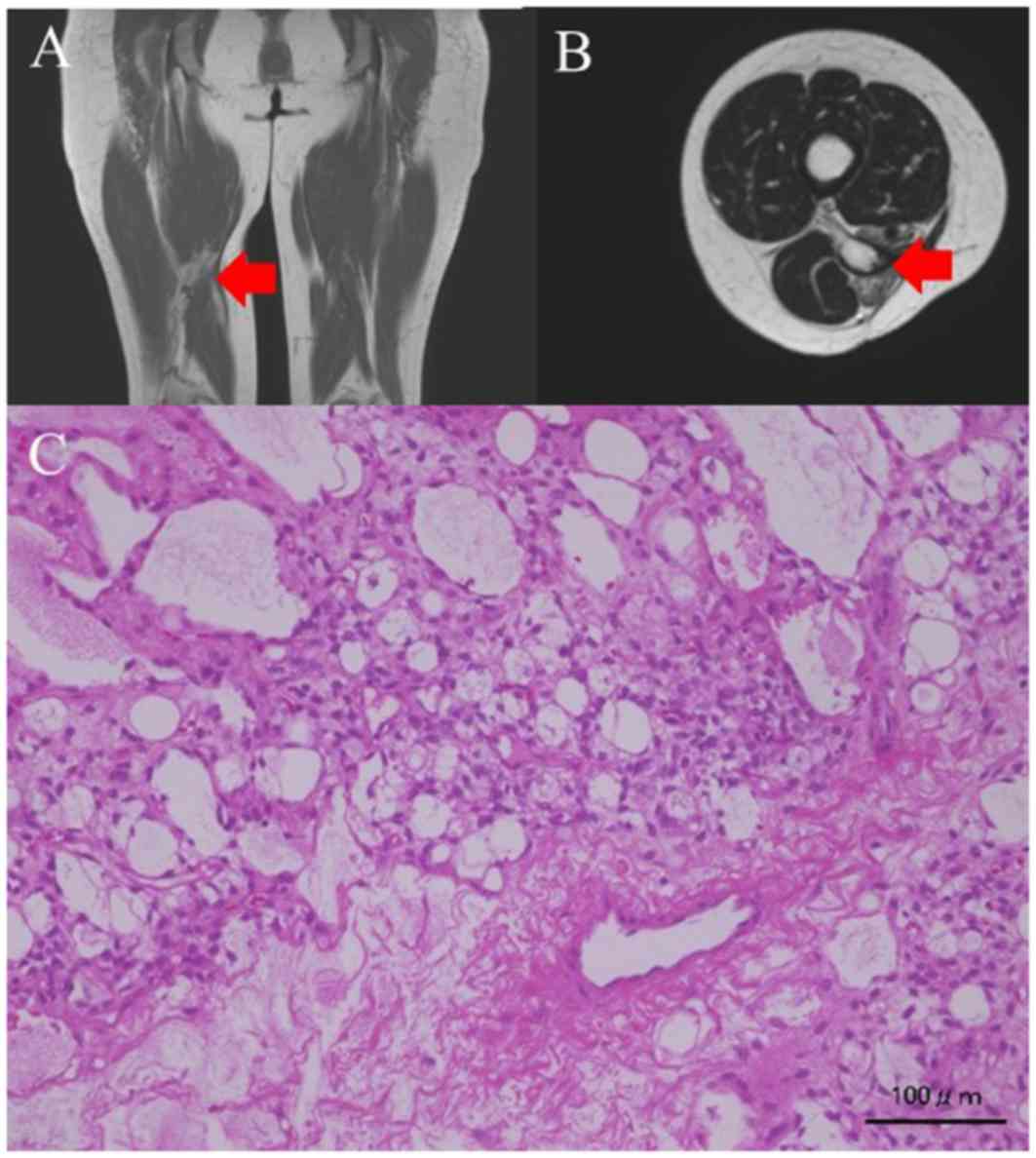
the histology was found to be myxoid liposarcoma (Fig. 1C). The surgical margins were
inadequate (R1), and a recurrence occurred in the nerve, 6 years
after the surgery (Fig. 2A and
B) leading to the tumor being
removed marginally. The histology revealed recurrent liposarcoma
(Fig. 2C).
The clinical results indicated a CDF, NED, and dead
of disease (DOD) status in 6, 2, and 5 cases, respectively. The
inadequate margins (R1 or R2) in 4 cases led to recurrence and DOD
status in 2 and 1 cases, respectively.
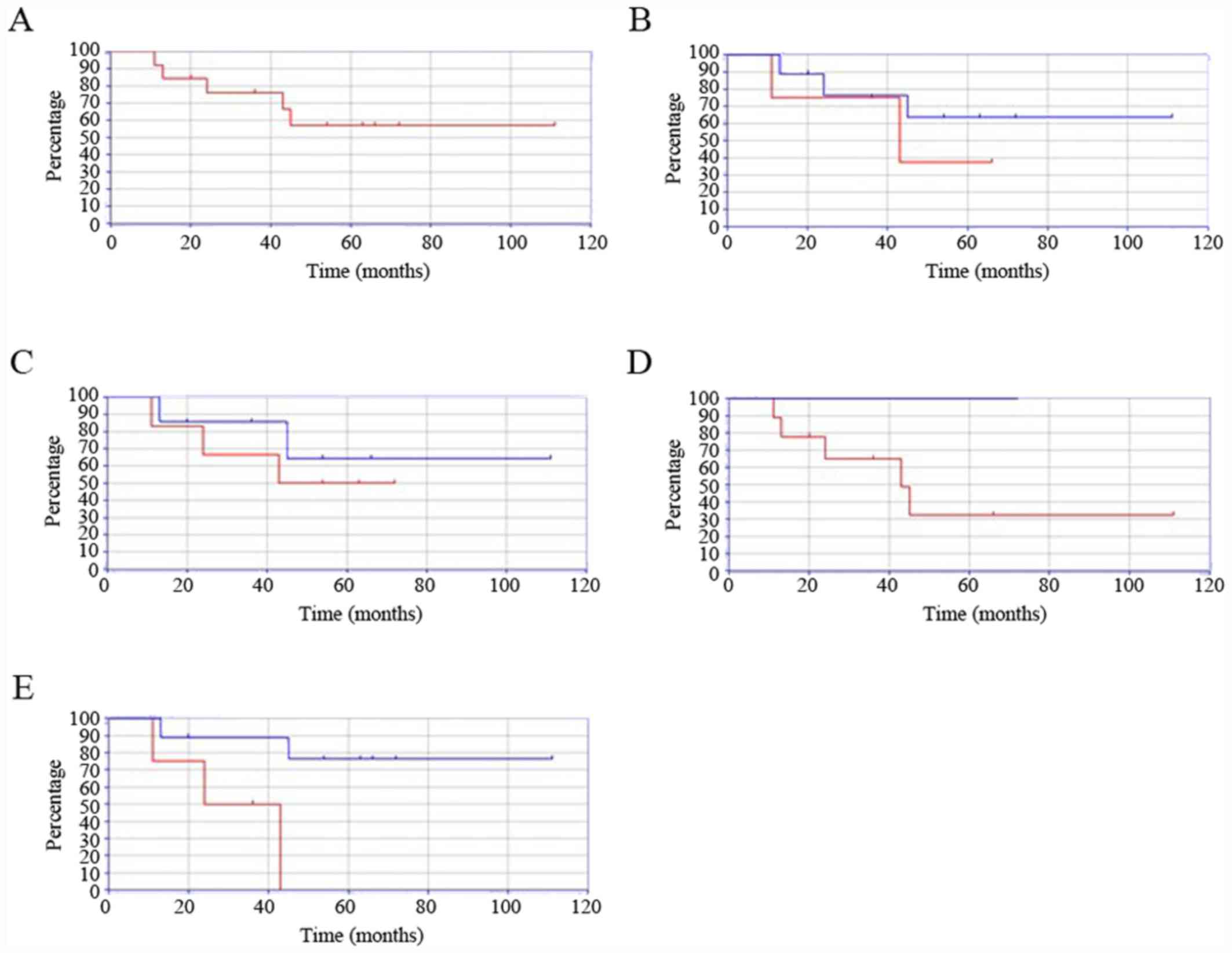
Survival
The 5-year survival rate for the entire cohort was
57.1% (Fig. 3A). The survival rate
of younger patients (15-29 years) was lower than that of their
older counterparts (≥30 years) (37.5 vs. 63.4%, P=0.43, Fig. 3B). The differences in survival were
similar between patients with bone and soft tissue tumors (72.0 vs.
64.2%, P=0.53, Fig. 3C). The 5-year
survival rate was decreased in patients with high-grade compared to
low-grade sarcomas (32.4 vs. 100%, P<0.001, Fig. 3D). The 5-year survival rate was also
decreased in patients with sarcomas located in the trunk compared
to in the extremities (0 vs. 76.2%, P=0.017, Fig. 3E).
Discussion
The clinical outcomes in AYAs with BSTS have not
improved owing to the lack of actionable data (10). In the present study, we determined
the clinical features and outcomes of AYA patients with BSTS.
Three of the major histological types of malignant
bone sarcomas among AYAs (based on incidence rates) are
osteosarcomas, Ewing sarcomas of the bone, and chondrosarcoma
(19). The major histological types
of soft tissue sarcomas found in AYAs include rhabdomyosarcomas,
synovial sarcomas, leiomyosarcomas, undifferentiated pleomorphic
sarcomas, and liposarcomas (5,19). In
the present study, almost all AYAs with BSTS had one of the major
histological types; however, Ewing sarcoma of the bone, which was
found in one patient, is relatively rare in the AYA age group.
Major sarcomas may metastasize to lymph nodes more
frequently in AYAs than in younger and older age groups (20,21);
lymph node metastatic status was previously found to be the most
important prognostic factor in patients with sarcomas (22,23). In
the present study, only one patient experienced sequential
metastases to the lymph nodes and lung, and subsequently succumbed
to the disease.
In general, surgical margins are associated with the
prognosis of malignant bone and soft tissue tumors (24,25).
Previous findings demonstrated that the surgical margin is
associated with the prognosis of malignant bone and soft tissue
tumors in AYA patients (26). In the
present study, inadequate surgical margins conferred poor
prognosis.
Previous findings have shown that 5-year survival
rates for AYA patients with BSTS range from 68.7 to 75.3% (10,27).
Being in the AYA age group is an independent negative prognostic
factor for patients with cancer (28). In addition, survival rates in AYA
patients with osteosarcoma were significantly poorer than those of
children (7,29). By contrast, in another study it was
shown that being in the AYA age group does not influence the
prognosis of patients with bone sarcoma (10). In the present study, the 5-year
survival rate was poorer than both the rates reported in previous
studies, and that of older patients with sarcoma (86.02%) included
in the present study (30). These
data support the hypothesis that being in the AYA age group is a
poor prognostic factor.
The prognostic factors for sarcoma in AYA patients
have been previously explored (5,10,31).
Previous findings have shown that older age, large tumor size, high
grade, lack of neoadjuvant chemotherapy, and positive surgical
margin adversely influence prognosis (32-35).
In the present study, younger patients with sarcomas had poorer
5-year survival rates than that of the older patients. Patients
with sarcomas of the trunk had poorer 5-year survival rates than
those with sarcomas in the extremities. Patients with high-grade
sarcomas also had poorer 5-year survival rates than those with
low-grade tumors. Thus, younger age, trunk location, and high-grade
status appear to be poor prognostic factors in AYA patients with
BSTS.
Our study had certain limitations. First, the number
of patients was small. Consequently, statistical analysis was not
feasible, and the report was therefore descriptive. Second, the
included tumors were considerably diverse. Third, we were unable to
compare the outcomes of these patients to those of younger patients
with sarcoma, and a future comparative study has been planned.
In conclusion, in the present study, we determined
the clinical features and outcomes of AYA patients with BSTS.
Younger age, trunk location, and high-grade tumors were associated
with poorer 5-year survival rates. Therefore, BSTS located in the
trunk or of high-grade should be treated more aggressively in
younger AYA patients.
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
KH, SN, and NO conceived and designed the study. KH,
SN, NO, and MA performed data acquisition. KH, SN, and MA performed
analysis and interpretation of data. KH, SN, NO, and MA were
involved in drafting the manuscript or revising it critically for
important intellectual content. KH, SN, NO, and MA gave final
approval of the version to be published and agreed to be
accountable for all aspects of the work. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Kindai University Hospital (approval no.: 31-153) (Osaka, Japan).
All patients also provided written informed consent for the
participation of this retrospective study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Burningham Z, Hashibe M, Spector L and
Schiffman JD: The epidemiology of sarcoma. Clin Sarcoma Res.
2(14)2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Herzog CE: Overview of sarcomas in the
adolescent and young adult population. J Pediatr Hematol Oncol.
27:215–218. 2005.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Barr RD, Ries LA, Lewis DR, Harlan LC,
Keegan TH, Pollock BH and Bleyer WA: US National Cancer Institute
Science of Adolescent and Young Adult Oncology Epidemiology Working
Grou: Incidence and incidence trends of the most frequent cancers
in adolescent and young adult Americans, including
‘nonmalignant/noninvasive’ tumors. Cancer. 122:1000–1008.
2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bleyer A, O'Leary M, Barr R and Ries LAG
(eds): Cancer epidemiology in older adolescents and young adults 15
to 29 years of age, including SEER incidence and survival:
1975-2000. Bethesda, MD: U.S. Dept. of Health and Human Services,
National Institutes of Health, National Cancer Institute, pp205,
2006.
|
|
5
|
Kasper B, Ouali M, van Glabbeke M, Blay
JY, Bramwell VH, Woll PJ, Hohenberger P and Schöffski P: Prognostic
factors in adolescents and young adults (AYA) with high risk soft
tissue sarcoma (STS) treated by adjuvant chemotherapy: A study
based on pooled European organisation for research and treatment of
cancer (EORTC) clinical trials 62771 and 62931. Eur J Cancer.
49:449–456. 2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Albritton KH: Sarcomas in adolescents and
young adults. Hematol Oncol Clin North Am. 19:527–546, vii.
2005.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Keegan TH, Ries LA, Barr RD, Geiger AM,
Dahlke DV, Pollock BH and Bleyer WA: National Cancer Institute Next
Steps for Adolescent and Young Adult Oncology Epidemiology Working:
Comparison of cancer survival trends in the United States of
adolescents and young adults with those in children and older
adults. Cancer. 122:1009–1016. 2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Haggar FA, Preen DB, Pereira G, Holman CD
and Einarsdottir K: Cancer incidence and mortality trends in
Australian adolescents and young adults, 1982-2007. BMC Cancer.
12(151)2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Eleutério SJ, Senerchia AA, Almeida MT, Da
Costa CM, Lustosa D, Calheiros LM, Barreto JH, Brunetto AL, Macedo
CR and Petrilli AS: Osteosarcoma in patients younger than 12 years
old without metastases have similar prognosis as adolescent and
young adults. Pediatr Blood Cancer. 62:1209–1213. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fukushima T, Ogura K, Akiyama T, Takeshita
K and Kawai A: Descriptive epidemiology and outcomes of bone
sarcomas in adolescent and young adult patients in Japan. BMC
Musculoskelet Disord. 19(297)2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Broders AC: Squamous cell epithelioma of
the lip. A study of 537 cases. JAMA. 74:656–664. 1920. View Article : Google Scholar
|
|
12
|
Trojani M, Contesso G, Coindre JM, Rouesse
J, Bui NB, de Mascarel A, Goussot JF, David M, Bonichon F and
Lagarde C: Soft-tissue sarcomas of adults; study of pathological
prognostic variables and definition of a histopathological grading
system. Int J Cancer. 33:37–42. 1984.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Edge SB, Byrd DR and Compton CC (eds):
Soft tissue sarcoma. American Joint Committee on Cancer cancer
staging manual. 7th edition. New York, Springer, New York, NY,
pp291-296, 2010.
|
|
14
|
Edge SB, Byrd DR and Compton CC (eds):
Bone. American Joint Committee on Cancer cancer staging manual. 7th
edition. New York, Springer, New York, NY, pp281-290, 2010.
|
|
15
|
Gundle KR, Kafchinski L, Gupta S, Griffin
AM, Dickson BC, Chung PW, Catton CN, O'Sullivan B, Wunder JS and
Ferguson PC: Analysis of margin classification systems for
assessing the risk of local recurrence after soft tissue sarcoma
resection. J Clin Oncol. 36:704–709. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Iwamoto Y, Tanaka K, Isu K, Kawai A,
Tatezaki S, Ishii T, Kushida K, Beppu Y, Usui M, Tateishi A, et al:
Multiinstitutional phase II study of neoadjuvant chemotherapy for
osteosarcoma (NECO study) in Japan: NECO-93J and NECO-95J. J Orthop
Sci. 14:397–404. 2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Tanaka K, Kawamoto H, Saito I, Yoshimura
K, Fukuda H and Iwamoto Y: Preoperative and postoperative
chemotherapy with ifosfamide and adriamycin for adult high-grade
soft-tissue sarcomas in the extremities: Japan clinical oncology
group study JCOG0304. Jpn J Clin Oncol. 39:271–273. 2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Pretz JL, Barysauskas CM, George S,
Hornick JL, Raut CP, Chen YE, Marcus KJ, Choy E, Hornicek F, Ready
JE, et al: Localized adult Ewing sarcoma: Favorable outcomes with
alternating vincristine, doxorubicin, cyclophosphamide, and
ifosfamide, etoposide (VDC/IE)-based multimodality therapy.
Oncologist. 22:1265–1270. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Katanoda K, Shibata A, Matsuda T, Hori M,
Nakata K, Narita Y, Ogawa C, Munakata W, Kawai A and Nishimoto H:
Childhood, adolescent and young adult cancer incidence in Japan in
2009-2011. Jpn J Clin Oncol. 47:762–771. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Mazeron JJ and Suit HD: Lymph nodes as
sites of metastases from sarcomas of soft tissue. Cancer.
60:1800–1808. 1987.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Al-Refaie WB, Andtbacka RH, Ensor J,
Pisters PW, Ellis TL, Shrout A, Hunt KK, Cormier JN, Pollock RE and
Feig BW: Lymphadenectomy for isolated lymph node metastasis from
extremity soft-tissue sarcomas. Cancer. 112:1821–1826.
2008.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Johannesmeyer D, Smith V, Cole DJ, Esnaola
NF and Camp ER: The impact of lymph node disease in extremity
soft-tissue sarcomas: A population-based analysis. Am J Surg.
206:289–295. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Riad S, Griffin AM, Liberman B, Blackstein
ME, Catton CN, Kandel RA, O'Sullivan B, White LM, Bell RS, Ferguson
PC and Wunder JS: Lymph node metastasis in soft tissue sarcoma in
an extremity. Clin Orthop Relat Res. 129–134. 2004.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Fujiwara T, Medellin MR, Sambri A, Tsuda
Y, Balko J, Sumathi V, Gregory J, Jeys L and Abudu A: Preoperative
surgical risk stratification in osteosarcoma based on the proximity
to the major vessels. Bone Joint J. 101-B:1024–1031.
2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Vodanovich DA, Spelman T, May D, Slavin J
and Choong PFM: Predicting the prognosis of undifferentiated
pleomorphic soft tissue sarcoma: A 20-year experience of 266 cases.
ANZ J Surg. 89:1045–1050. 2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Janeway KA, Barkauskas DA, Krailo MD,
Krailo MD, Meyers PA, Schwartz CL, Ebb DH, Seibel NL, Grier HE,
Gorlick R and Marina N: Outcome for adolescent and young adult
patients with osteosarcoma: A report from the children's oncology
group. Cancer. 118:4597–4605. 2012.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Avila JC, Livingston JA, Rodriguez AM,
Kirchhoff AC, Kuo YF and Kaul S: Disparities in adolescent and
young adult sarcoma survival: Analyses of the texas cancer registry
and the national SEER data. J Adolesc Young Adult Oncol. 6:681–687.
2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Tricoli JV, Seibel NL, Blair DG, Albritton
K and Hayes-Lattin B: Unique characteristics of adolescent and
young adult acute lymphoblastic leukemia, breast cancer, and colon
cancer. J Natl Cancer Inst. 103:628–635. 2011.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Khamly KK, Thursfield VJ, Fay M, Desai J,
Toner GC, Choong PF, Ngan SY, Powell GJ and Thomas DM:
Gender-specific activity of chemotherapy correlates with outcomes
in chemosensitive cancers of young adulthood. Int J Cancer.
125:426–431. 2009.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Hashimoto K, Nishimura S, Hara Y, Oka N,
Tanaka H, Iemura S and Akagi M: Clinical outcomes of patients with
primary malignant bone and soft tissue tumor aged 65 years or
older. Exp Ther Med. 17:888–894. 2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
White VM, Orme LM, Skaczkowski G,
Pinkerton R, Coory M, Osborn M, Bibby H, Nicholls W, Conyers R,
Phillips MB, et al: Management of sarcoma in adolescents and young
adults: An Australian population-based study. J Adolesc Young Adult
Oncol. 8:272–280. 2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Duchman KR, Gao Y and Miller BJ:
Prognostic factors for survival in patients with Ewing's sarcoma
using the surveillance, epidemiology, and end results (SEER)
program database. Cancer Epidemiol. 39:189–195. 2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bertrand TE, Cruz A, Binitie O, Cheong D
and Letson GD: Do surgical margins affect local recurrence and
survival in extremity, nonmetastatic, high-grade osteosarcoma? Clin
Orthop Relat Res. 474:677–683. 2016.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Buchner M, Bernd L, Zahlten-Hinguranage A
and Sabo D: Primary malignant tumours of bone and soft tissue in
the elderly. Eur J Surg Oncol. 30:877–883. 2004.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Duchman KR, Gao Y and Miller BJ:
Prognostic factors for survival in patients with high-grade
osteosarcoma using the surveillance, epidemiology, and end results
(SEER) program database. Cancer Epidemiol. 39:593–599.
2015.PubMed/NCBI View Article : Google Scholar
|