Introduction
Synovial osteochondroma (SO) is a relatively
uncommon disorder characterized by the development of hyaline
cartilage tissue from the synovium (1). It typically presents as knee
arthropathy, and is thought to arise from a metaplastic process on
the synovial membrane (2). This
cartilaginous tissue may form loose bodies in the joint and become
symptomatic (3). Malignant
transformation to chondrosarcoma is uncommon but has been described
(4). SO usually involves the joints,
such as the knee, hip, ankle, elbow, wrist, and shoulder joints
(5). Extra-articular lesions are
relatively uncommon and mainly observed in a synovial sheath or the
bursa of the foot or hand (6). Large
extra-articular lesions of the Hoffa's fat pad are rare. The
present study presents a case of extra-articular SO of the right
knee in a 56-year-old woman. This is the first case of large
extra-articular SO involving the patellar tendon with restriction
of range of motion in the knee.
Case report
A 56-year-old woman presented at Kindai University
Hospital (Osaka, Japan) with a 2-year history of knee pain
associated with an enlarging mass on the anterior of the right
knee. She had only a past medical history of a benign breast
tumor.
Examination of the right knee joint revealed an
8x9-cm elastic hard mass lesion on the anterolateral right knee.
The patient had restricted range of motion (0-130 degrees) of the
knee, and deep flexion aggravated the pain. Her inflammatory
markers were normal. Radiography showed enhancement of soft part
shadows and calcification at the Hoffa's fat pad (data not shown).
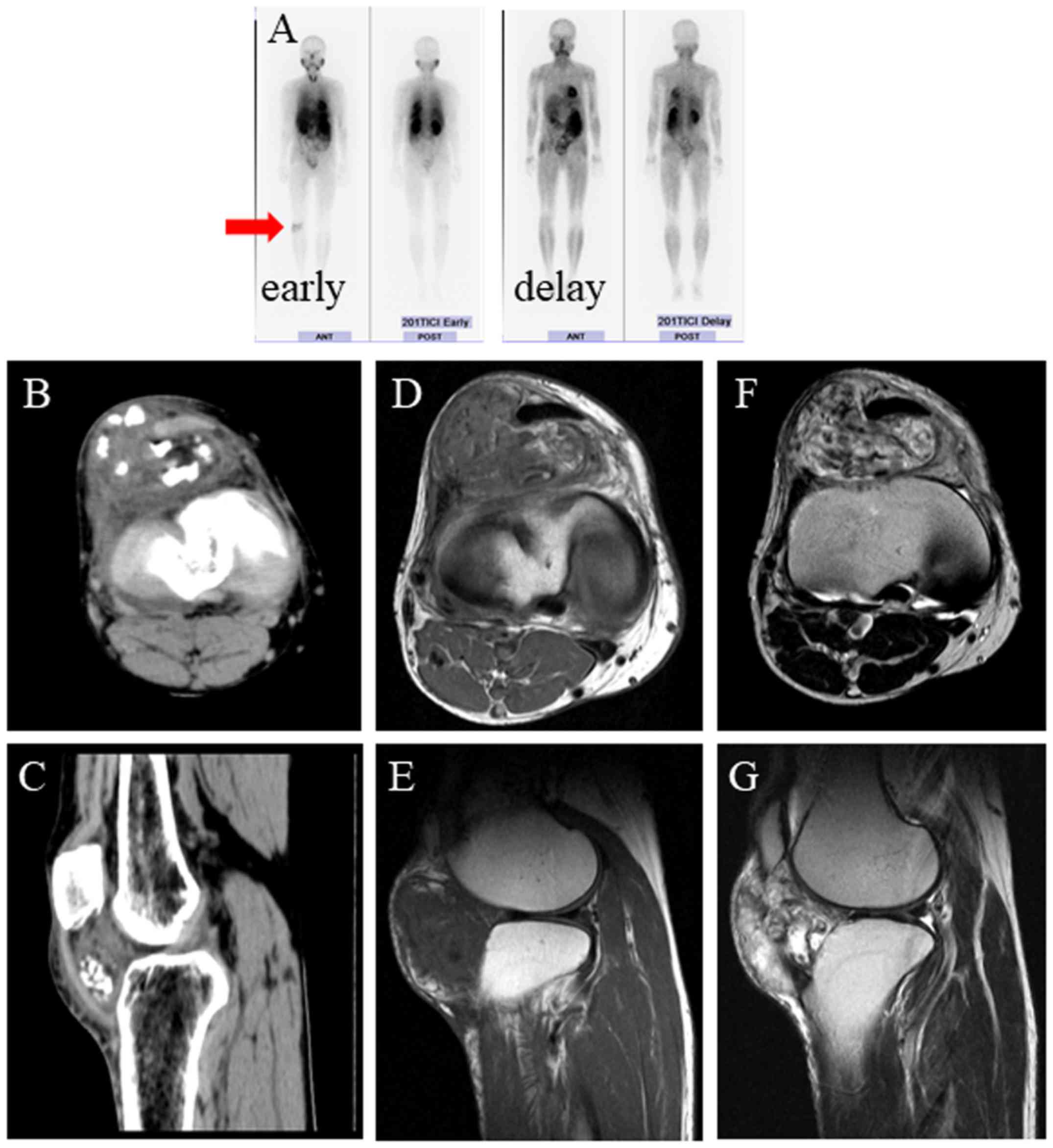
Bone scintigraphy showed abnormal accumulation in the front of the
right knee in the early phase that decreased in the delay phase
(Fig. 1A). Computed tomography
showed an iso- to low-intensity mass involving the patellar tendon
at the Hoffa's fat pad lesion with calcification (Fig. 1B and C). T1-weighted magnetic resonance imaging
(MRI) showed an iso-intensity mass (Fig.
1D and E), and T2-weighted MRI
showed a high-intensity mass (Fig.
1F and G). We conducted needle
biopsy. The histology showed synovial tissue and chondrocyte tissue
fragments (data not shown). No malignancy was detected. The patient
underwent marginal resection. Adhesion to the tissue surrounding
the tumor mass was confirmed. The tumor mass also adhered to the
patellar tendon, and we released the adhesion of the tumor mass and
patellar tendon. It was easy to release the tendon from the
tumor.
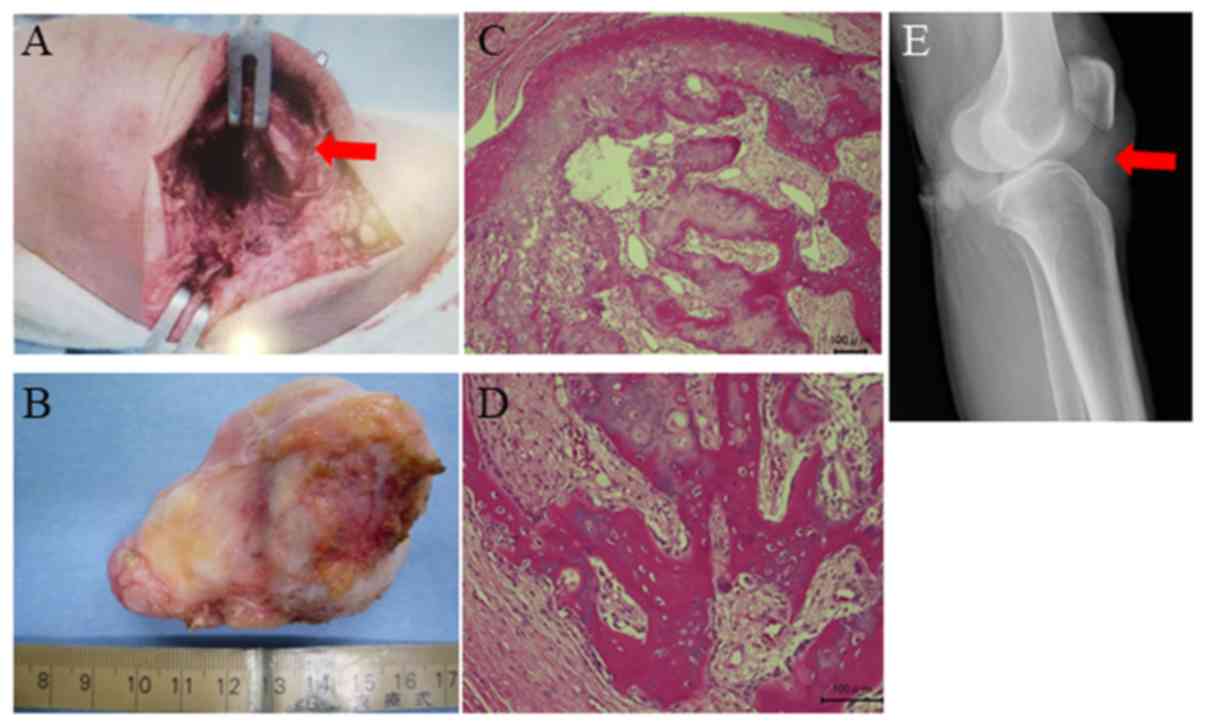
After the surgery, the patellar tendon was not
damaged (Fig. 2A). The excised
specimen showed an elastic, hard, white-yellow covering (Fig. 2B). Hematoxylin and eosin staining
showed hyaline cartilage and trabecular bone formation (Fig. 2C and D). Osteoblasts lined the trabecular bone,
and scattered osteoclasts were observed (Fig. 2C and D). Spindle-like cell proliferation was
observed between the trabeculae (Fig.
2C and D). We diagnosed SO by
the histological findings. Radiography after surgery confirmed that
there was no damage to the patellar tendon (Fig. 2E). The range of motion had improved
(0-145 degrees), and the knee pain during deep flexion
disappeared.
Discussion
Extra-articular SO often occurs at the site of the
Hoffa's fat pad (7). However,
extra-articular SO involving the patellar tendon has not been
previously reported. To the best of our knowledge, this is the
first case of extra-articular SO involving the patellar tendon.
The etiology of para-articular osteochondroma has
not been clarified (8). Metaplasia
from extra-synovial mesenchymal cells can be the origin of
osteochondroma (8). Repeated trauma
can also cause metaplasia (9,10).
Moreover, SO of the Hoffa's fat pad is considered the final stage
of inflammation after injury (11).
The possibility of existence of occult injury history of the
Hoffa's fat pad was also considered in the present case. The
differential diagnosis of SO in this location includes
para-articular osteochondroma, Hoffa's disease, and primary
chondrosarcoma (12).
Extra-articular synovial osteochondroma should be differentiated
from para-articular osteochondroma of the infrapatellar fat pad
(13). On histologic examination,
hypercellular hyaline cartilage arising from the synovium is
detected, and nuclear atypia is common. Benign synovial
chondromatosis can be difficult to differentiate histologically
from low-grade chondrosarcoma; some features more suggestive of
malignancy include cartilaginous cells in sheets rather than
clusters, myxoid changes, and the presence of necrosis (1-3).
However, no definitive criteria for the diagnosis of malignancy
exist. In the present case, no clear malignant findings were
detected.
We observed calcification by radiography, which is
common in such cases (14-16).
Computed tomography or MRI more commonly lead to characterization
of the lesion and can be diagnostic. Non-calcified and calcified
lesions may be differentiated on MRI because non-mineralized
chondromata are isointense on T1-but hyperintense on T2-weighted
images (17), as observed in the
present study.
With regard to the treatment of SO, marginal
resection is preferable when possible (4,5).
Over-wide surgical treatment should be avoided (18). Our patient underwent marginal
resection and has a good prognosis without functional disorder. If
restriction of knee range of motion is observed, as in the present
case, resection should be performed as early as possible. Long-term
follow-up is crucial because of the high rate of recurrence and
risk of malignant transformation (19).
Similar tumors have been reported in recent years
(15,16). Both cases originated from the Hoffa's
fat pad and caused knee pain. One patient demonstrated an
impingement of the knee joint (15).
However, unlike our case, the tumors in both cases did not show
involvement of the patellar tendon. Based on these findings, the
present case was more advanced than those limited to the Hoffa's
fat pad. Therefore, the present case is unique in that it
demonstrates that advanced cases with patellar tendon involvement
may be cured by marginal resection.
Acknowledgements
We thank Editage for the English editing.
Funding
Not applicable.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SN, SI, KN, SA, IT, KY, RK, KH and MA analyzed and
interpreted the patient data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The procedures followed were in accordance with the
Ethical standards of the responsible committee on human
experimentation (institutional and national) and with the Helsinki
Declaration of 1975, as revised in 2013. The patients also provided
written informed consent for this retrospective study.
Patient consent for publication
We obtained written informed consent for publication
from the patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Trevino M, Laks S, Kafchinski L,
Sundarakumar DK and Smith CM: Intermetatarsal bursa primary
synovial chondromatosis: Case report and review of the literature.
Skeletal Radiol. 46:1769–1773. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Temponi EF, Mortati RB, Mortati GMH,
Mortati LB, Sonnery-Cottet B and de Carvalho Júnior LH: Synovial
chondromatosis of the knee in a 2-year-old Child: A case report and
review of the literature. JBJS Case Connect. 6(e71)2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Raval P, Vijayan A and Jariwala A:
Arthroscopic retrieval of over 100 loose bodies in shoulder
synovial chondromatosis: A case report and review of literature.
Orthop Surg. 8:511–515. 2016.PubMed/NCBI View
Article : Google Scholar
|
|
4
|
Ng VY, Louie P, Punt S and Conrad EU:
Malignant transformation of synovial chondromatosis: A systematic
review. Open Orthop J. 11:517–524. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Lohmann CH, Köster G, Klinger HM and Kunze
E: Giant synovial osteochondromatosis of the acromio-clavicular
joint in a child. A case report and review of the literature. J
Pediatr Orthop B. 14:126–128. 2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Doral MN, Uzumcugil A, Bozkurt M, Atay OA,
Cil A, Leblebicioglu G and Tetik O: Arthroscopic treatment of
synovial chondromatosis of the ankle. J Foot Ankle Surg.
46:192–195. 2007.PubMed/NCBI View Article : Google Scholar
|
|
7
|
O'Connell L, Memon AR, Foran P, Leen E and
Kenny PJ: Synovial chondroma in Hoffa's fat pad: Case report and
literature review of a rare disorder. Int J Surg Case Rep.
32:80–82. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Li C, Arger PH and Dalinka MK: Soft tissue
osteochondroma. A report of three cases. Skeletal Radiol.
18:435–437. 1989.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kautz FG: Capsular osteoma of the knee
joint. Report of four cases. Radiology. 45:162–167. 1945.
View Article : Google Scholar
|
|
10
|
Krebs VE and Parker RD: Arthroscopic
resection of an extrasynovial ossifying chondroma of the
infrapatellar fat pad: End-stage Hoffa's disease? Arthroscopy.
10:301–304. 1994.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Turhan E, Doral MN, Atay AO and Demirel M:
A giant extrasynovial osteochondroma in the infrapatellar fat pad:
End stage Hoffa's disease. Arch Orthop Trauma Surg. 128:515–519.
2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ogura K, Goto T, Nemoto T and Imanishi J:
Para-articular osteochondroma of the infrapatellar fat pad. J Knee
Surg. 24:209–213. 2011.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Sakai H, Tamai K, Iwamoto A and Saotome K:
Para-articular chondroma and osteochondroma of the infrapatellar
fat pad: A report of three cases. Int Orthop. 23:114–117.
1999.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Osti L, Papalia R, Del Buono A, Denaro V
and Maffulli N: Recurrence of synovial chondromatosis of the
Hoffa's body. Knee Surg Sports Traumatol Arthrosc. 17:1421–1424.
2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Maljanovič M, Ristič V, Rasovič P,
Matijevič R and Milankov V: Solitary synovial chondromatosis as a
cause of Hoffa's fat pad impingement. Med Pregl. 68:49–52.
2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Lee DH and Jeong TW: Uncommon primary
synovial chondromatosis involving only the infrapatellar fat pad in
an elderly patient. Knee Surg Relat Res. 28:79–82. 2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Sheldon PJ, Forreste DM and Learch TJ:
Imaging of intraarticular masses. Radiographics. 25:105–119.
2005.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Maheshwari AV, Muro-Cacho CA and Pitcher
JD Jr: Extraskeletal para-articular osteochondroma of the posterior
knee. J Knee Surg. 22:30–33. 2009.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Bashaireh KM: Patellar subluxation with
early-phase synovial chondromatosis of the knee. Orthopedics.
39:e176–e179. 2016.PubMed/NCBI View Article : Google Scholar
|