Introduction
Mediastinal atypical carcinoid is a type of
neuroendocrine tumor which is rare and aggressive mediastinal tumor
(1). Neuroendocrine carcinoma is
often divided into typical carcinoid, atypical carcinoid, small
cell carcinoma and large cell neuroendocrine carcinoma based on
morphology. Small cell carcinoma and large cell neuroendocrine
carcinoma are high-grade tumors. Typical and atypical carcinoid
tumors are low-medium grade tumors (2). Clinically, patients may be asymptomatic
or show local symptoms because of the compression or invasion of
mediastinal structures, or systemic symptoms secondary to the tumor
ability to produce hormones or cytokines (3). Neuroendocrine tumors (NETs) are
epithelial neoplasms with major neuroendocrine differentiation that
begin in most organs of the body. Primary NET of the mediastinum
are very occasional (2), they have
been the source of investigation and debatable in the literature
because of their origin.
Thymic carcinoids characterize by unusual neoplasms.
Their yearly over all age-adjusted occurrence has been described to
be estimated 1 of 10,000,000(4), and
roughly 200 cases have been stated in the literature (5). Thymic carcinoids occur mainly in men
with a ratio of 3:1 to that of women. It has a middling age of 43
years (range 39–60 years)(6).
Neuroendocrine carcinomas of the thymus and are reasonably
differentiated with a high rate of metastasis. These tumors reveal
a 5-year survival rate of 60% and their reappearance is
common.(7,8) Furthermore, the brutality of the illness
is frequently abandoned since the medical appearance is somewhat
benign. Hence, thymic carcinoids are usually revealed at a far
advanced stage, which may also account for the poor prognosis
(9)
Thymic carcinoids often act destructively. Thorough
surgical removal of the thymus is the first treatment of
high-quality for thymic carcinoids as chemotherapy and radiotherapy
are not active for lengthening survival (9,10). When
the tumor is destructive to the patient, surgery is still the best
way to eradicate the tumor for causing death. Different options
have been raised on the functions of chemotherapy and radiotherapy
in the postoperative management of thymic carcinoids. However,
adjuvant treatment may also assist in the disease control, it is
not active to eliminate tumors and to inhibit the growth of tumor
or metastases (11). On the other
hand, adjuvant radiotherapy has been described in avoidance of
local-regional reappearance (12).
Utilization of the following therapy only or in combination
chemotherapies with 5-fluorouracil, streptozocin, carmustine,
VP-16, and cisplatin have been administered earlier without any
significant influence on the reappearance rate or overall survival
(13). Herein we reported a very
special case of primary cutaneous NET (atypical carcinoid)
expressing CA125 and CRP with immunohistochemical markers (CD 56+,
CD 117+, Syn+, CgA+.and CK+).
Case report
A 56-year-old male was presented with intermittent
chest tightness for 1 month. His chest tightness was aggravated
with movement. He began to cough and developed hemoptysis after 11
days. The hemoptysis was a bright red and small amount. He did not
have a history of chemicals, fumes, or dust exposure and no history
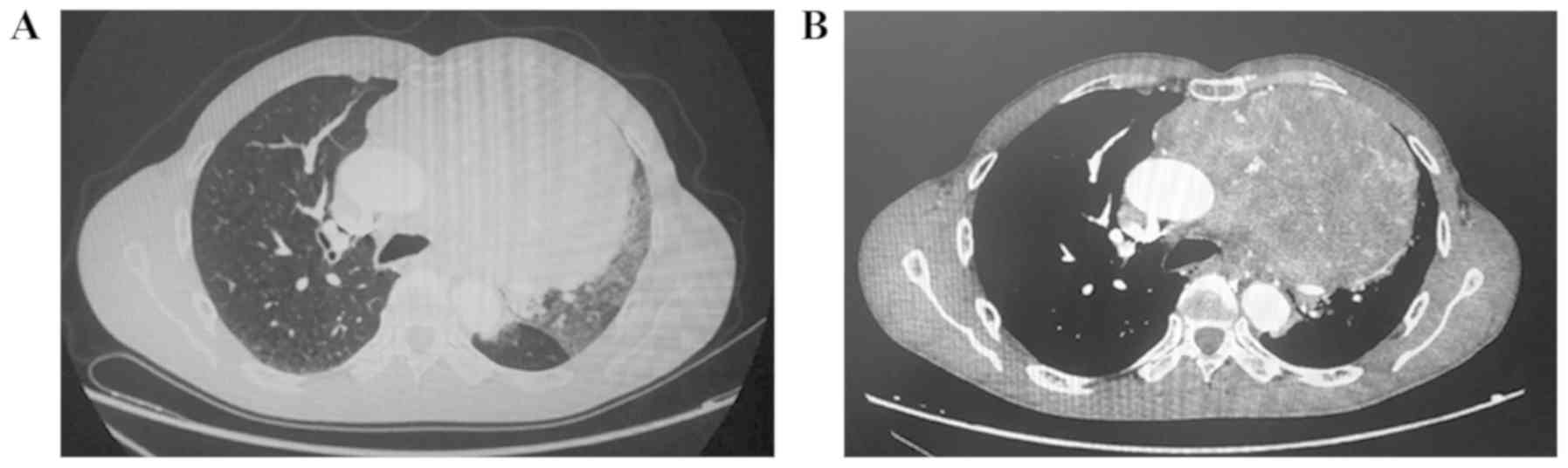
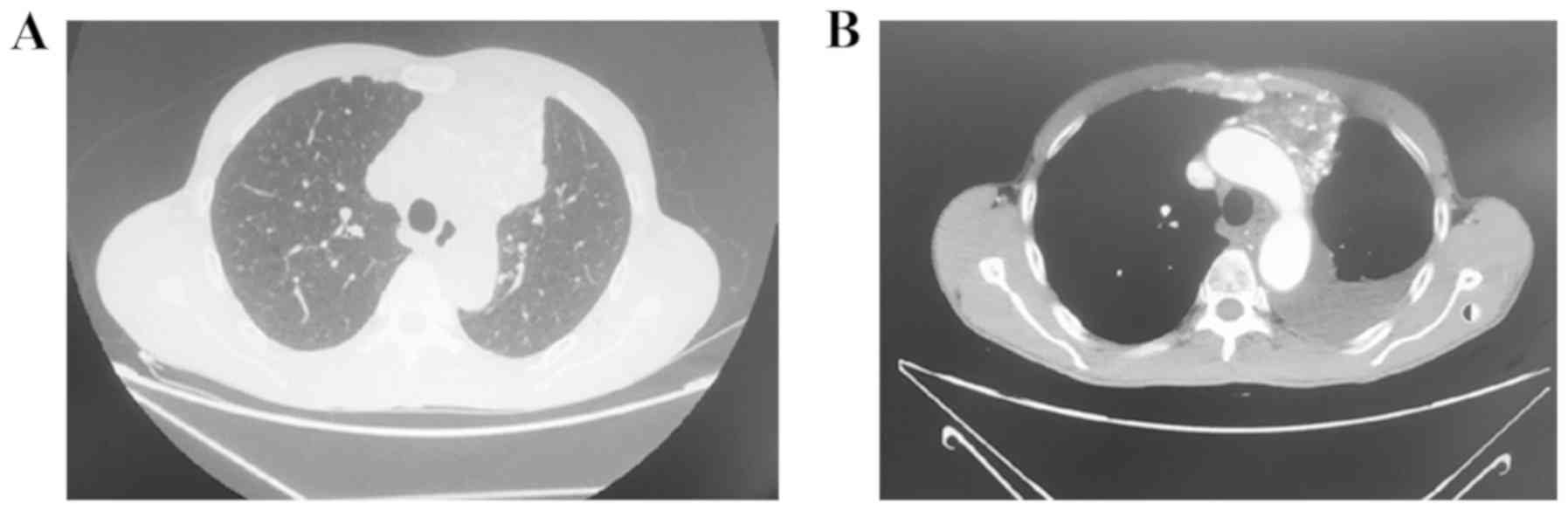
of tobacco or alcohol abuse. Chest enhanced CT demonstrated a
16.5x13.0 cm soft tissue mass in the left anterior mediastinum
(Fig. 1). Laboratory data revealed
the following values: Neuron Specific Enolase of 62.13 ng/ml
(reference range, 0-40 ng/ml), CYFRA21 of 3.01 ng/ml (reference
range, 0-3.3 ng/ml), CEA of 4.22 (0-6.5) ng/ml, SCC 0.5 (0-1.5)
ng/ml, CA125 67.24 (0-35) U/ml; AFP 23 (0-25) U/ml, CRP 96.7 mg/l
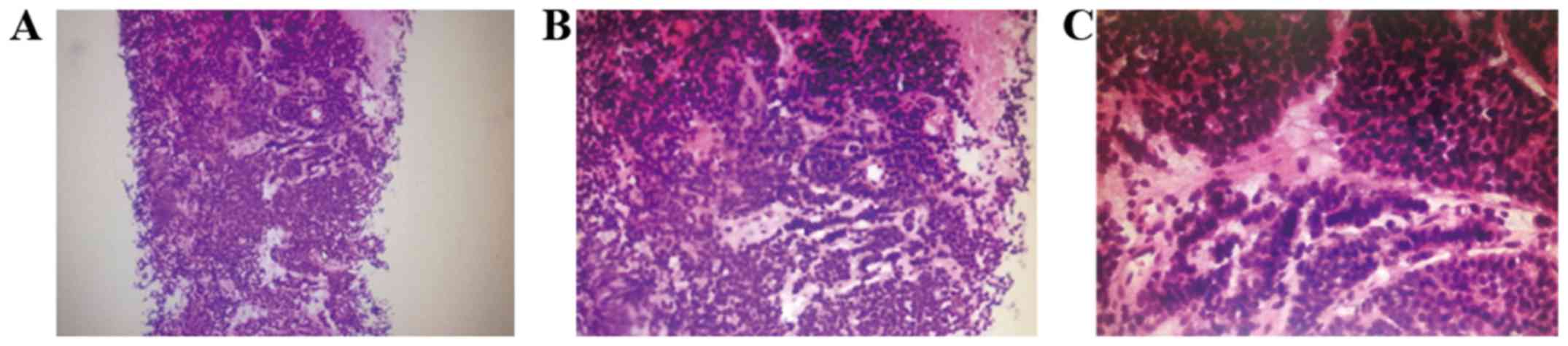
(0-10); PCT <0.05 ng/ml (0-0.05); ESR 48 mm/h (0-20). Tissue
pathology revealed tumor cells with small cell pattern, cell
proliferation activity was 10% (Fig.
2). Neuroendocrine carcinoma is characterized by invasive
growth, lymphatic and blood metastasis. Therefore, it has been
incorporated into low-grade malignancies by WHO. The cytoplasm of
atypical carcinoid contains neuroendocrine granules, which has a
secretory function and can lead to carcinoid syndromes such as
paroxysmal skin flushing, diarrhea, asthma, tachycardia, and
ectopic adrenocorticotropic syndrome. But these symptoms are not
presented rare, and there is no appeal, in this case, however,
thyroid, parathyroid and sex hormones assay were done and it was
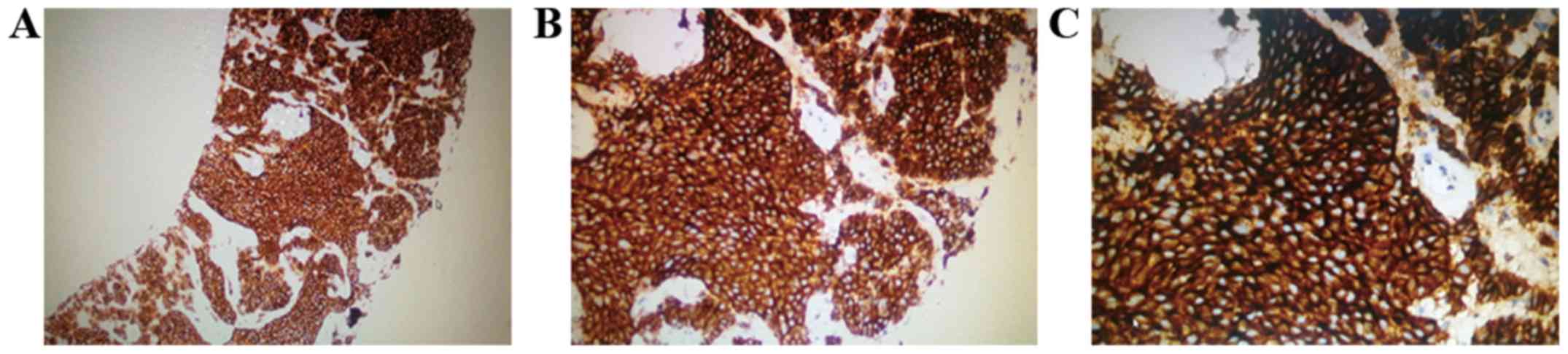
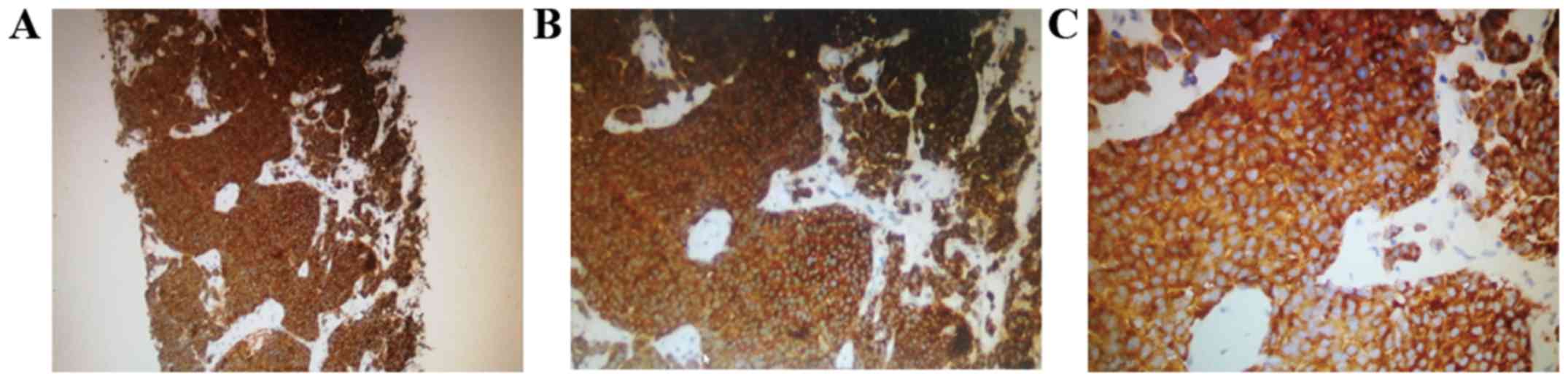
normal in this patient. The results of immunohistochemistry in this
patient's tissue biopsy show: CD117(+), CD1a(-), CD5(-), CD56(+),
CD99(-), CgA(+), CK(AE1/AE3)(+), CK19(+), Ki67(10%+), LCA(-),
SYN(+), TdT(-) TTF-1(-). Synaptophysin (Syn), chromaffin (CgA) and
CD56 are the immunohistochemical markers for the diagnosis of
neuroendocrine tumors (Figs. 3 and
4), recent research shows that Ki-67
is a potentially meaningful marker for sub-categorization of lung
neuroendocrine tumors, the cut-off value of Ki67 for
typical/atypical carcinoids was 7.5% with sensitivity and
specificity of 91.4 and 100% (area under curve is 0.9685) (14). CK19 assisted diagnosis of thymic
epithelial origin, TTF-1 assisted diagnosis of lung and thyroid
tissue origin. Therefore, the mediastinal mass is considered as a
neuroendocrine tumor originates from the thymus. Considering that a
tumor had been transferred to the pleural and multiple lymph nodes.
We decided to have surgical excision after combined chemotherapy
with bevacizumab + capecitabine + timozolamine. After the patient
was given chemotherapy, the symptom and CT showed improvement but
the patient and his family rejected surgery. On March 11, 2018 the
lesion progressed into the lymph and pleura. Patient was commenced
on radiotherapy and new chemotherapeutic regimen
(etoposide-carboplatin-bevacate). Another CT scan was performed
after a month which revealed a substantial decrease in tumor size
(Fig. 5). Subsequently CT scan was
performed for this patient which further revealed a decrease in
tumor size. Currently, patients have been treated with bevacizumab
maintenance therapy.
Discussion
Atypical carcinoid may occur in many organs and
tissues. They are more usually found in the gastro-entero-hepatic
or respiratory system (15,16). NETs of the mediastinum are very
uncommon and usually, thymic NETs are the most common they are
totally found in the anterosuperior mediastinum and account for 2
to 4% of all mediastinal tumors (17). Mediastinal NETs have been the
foundation of considerable care and disagreement among experts and
investigators because of their origin, that is still debatable.
Their terminology and grouping have evolved over the years. Likened
with bronchopulmonary carcinoid, primary NETs of the mediastinum
are described by a poor prognosis due to their high tendency for
local reappearance and previous distant metastases (13). The function of chemotherapy is
disputed; in this case chemotherapy was used for the patient and it
caused a reduction of tumor size and a decrease of proliferation
rate. In the previous cases, of mediastinal NETs successfully
treated by a combination of chemotherapy and Y-DOTATOC (18) or by radiotherapy alone (19) have been described. Hence, we utilized
both chemotherapy and radiotherapy. Various investigators debated
that a co-expression of CD117 (c-kit) and CD5 could be indicative
of a neoplasm of thymic origin (20). In this case report, only CD117 was
positive, thus not signifying a thymic origin. CD117 is frequently
positive in small cell lung carcinoma and large cell NET and it is
frequently negative in typical and atypical carcinoid. The
positivity detected for c-kit could have vital therapeutic
implication, such as the administration of etoposide (0.5
g)-carboplatin (0.4 g)-bevacate (0.4 g) . The prognosis of atypical
carcinoid is worse than that of typical carcinoid. Hence, it
requires a multidisciplinary team approach for optimal treatment.
This patient presented with pleural effusion. CT was progressive
and the primary tumor shrank. But the patient feels that the
general situation is okay and cannot be operated. It was first
discovered in the late stage, with lymph node metastasis and
pleural metastasis. We believe that further study of conservative
treatment of chemotherapy and radiotherapy is a treatment to
improve atypical carcinoid.
Acknowledgements
The authors would like to thank Dr Ayobami Olajuyin
and Dr Adefunke Olajuyin (Department of Respiratory and Critical
Care Medicine, The Provincial Hospital of Zhengzhou University,
Zhengzhou, Henan, China) for helpful comments and revision of the
manuscript.
Funding
The study was supported by the grant from Henan
Provincial Department of Science and Technology (no. 182102310168
to WXX). The authors appreciate Dr Ayobami Olajuyin and Dr Adefunke
Olajuyin (Department of Respiratory and Critical Care Medicine, the
People's Hospital of Zhengzhou University) for helpful comments and
significant revision of the manuscript.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article or are available from the
corresponding author on reasonable request.
Authors' contributions
XJZ conceived the project and designed the
experiments. WXX, JJL and YJS performed the experiments. WXX
analyzed the data. WXX and XJZ wrote the paper. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Henan Provincial People's Hospital (Zhengzhou, China).Written
informed consent was obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Melosky B: Advanced typical and atypical
carcinoid tumours of the lung: Management recommendations. Curr
Oncol. 25:S86–S93. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rindi G, Klersy C, Inzani F, Fellegara G,
Ampollini L, Ardizzoni A, Campanini N, Carbognani P, De Pas TM,
Galetta D, et al: Grading the neuroendocrine tumors of the lung: An
evidence-based proposal. Endocr Relat Cancer. 21:1–16.
2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ventura L, Gnetti L, Silini EM, Rindi G,
Carbognani P, Rusca M and Ampollini L: Primary atypical carcinoid
tumor of the mediastinum: A very rare finding. J Thorac Dis.
9:367–372. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Strosberg JR, Berry MF and Tanzelaar HD:
Thymic neuroendocrine (carcinoid) tumors. UpToDate. https://www.uptodate.com/contents/thymic-neuroendocrine-carcinoid-tumors.
Jul 23, 2019.
|
|
5
|
Gielda BT, Peng R, Coleman JL, Thomas CR
and Cameron RB: Treatment of early stage thymic tumors: Surgery and
radiationtherapy. Current treatment options in oncology. 9:259–268.
2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wick MR, Scott RE, Li CY and Carney JA:
Carcinoid tumor of the thymus: A clinicopathologic report of seven
cases with a review of the literature. Mayo Clin Proc. 55:246–254.
1980.PubMed/NCBI
|
|
7
|
Tiffet O, Nicholson AG, Ladas G, Sheppard
MN and Goldstraw P: A clinicopathologic study of 12 neuroendocrine
tumors arising in the thymus. Chest. 124:141–146. 2003.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Vinik AI, Silva MP, Woltering EA, Go VLW,
Warner R and Caplin M: Biochemical testing for neuroendocrine
tumors. Pancreas. 38:876–889. 2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Lin FCF, Lin CM, Hsieh CC, Li WY and Wang
LS: Atypical thymic carcinoid and malignant somatostatinoma in type
I multiple endocrine neoplasia syndrome: Case report. Am J Clin
Oncol. 26:270–272. 2003.PubMed/NCBI View Article : Google Scholar
|
|
10
|
John LC, Hornick P, Lang S, Wallis J and
Edmondson SJ: Giant thymic carcinoid. Postgrad Med J. 67:462–465.
1991.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Fukai I, Masaoka A, Fujii Y, Yamakawa Y,
Yokoyama T, Murase T and Eimoto : Thymic neuroendocrine tumor
(thymic carcinoid): A clinicopathologic study in 15 patients. Ann
Thorac Surg. 67:208–211. 1999.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Dutta R, Kumar A, Julka PK, Mathur SR,
Kaushal S, Kumar R, Jindal T and Suri V: Thymic neuroendocrine
tumour (carcinoid): Clinicopathological features 188 of four
patients with different presentation. Interact Cardiovasc Thorac
Surg. 11:732–736. 2010.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gal AA, Kornstein MJ, Cohen C, Duarte IG,
Miller JI and Mansour KA: Neuroendocrine tumors of the thymus: A
clinicopathological and prognostic study. Ann Thorac Surg.
72:1179–1182. 2001.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Garg R, Bal A, DAS A, Singh N and Singh H:
Proliferation marker (Ki67) in sub-categorization of neuroendocrine
tumours of the lung. Turk Patoloji Derg. 35:15–21. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Caplin ME, Baudin E, Ferolla P, Filosso P,
Garcia-Yuste M, Lim E, Oberg K, Pelosi G, Perren A and Rossi RE:
Pulmonary neuroendocrine (carcinoid) tumors: European
neuroendocrine tumor society expert consensus and recommendations
for best practice for typical and atypical pulmonary carcinoids.
Ann Oncol. 26:1604–1620. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Filosso PL, Guerrera F, Evangelista A,
Welter S, Thomas P, Casado PM, Rendina EA, Venuta F, Ampollini L
and Brunelli A: Prognostic model of survival for typical bronchial
carcinoid tumours: Analysis of 1,109 patients on behalf of the
European Association of Thoracic Surgeons, (ESTS) Neuroendocrine
Tumours Working Group. Eur J Cardiothorac Surg. 48:441–447.
2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Franco R, Marino FZ and Giordano A: The
Mediastinal Mass-A multidisciplinary approach: 2018. Springer
Link.
|
|
18
|
Fazio N, Grana C, Pelosi G, Torrisi R, Di
Meglio G, Tradati N, Lorizzo K and De Braud F: Successful
chemotherapy and 90Y-DOTATOC in a patient with mediastinal highly
aggressive neuroendocrine carcinoma. Acta Oncol. 45:627–629.
2006.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Furuta M, Hayakawa K, Kato S, Mitsuhashi
N, Nakajima T and Niibe H: Malignant neuroendocrine tumor
presenting a huge mediastinal mass controlled with radiation
therapy. Lung cancer. 22:55–58. 1998.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kriegsmann M, Muley T, Harms A, Tavernar
Goldmann T, Dienemann H, Herpel E and Warth A: Differential
diagnostic value of CD5 and CD117 expression
in thoracic tumors: A large scale study of 1,465 non-small cell
lung cancer cases. Diagn Pathol. 10(210)2015.PubMed/NCBI View Article : Google Scholar
|