Introduction
Multiple primary cancers are defined as the presence
of two or more independent primary cancers in an individual
(1). The incidence of multiple
primary cancers is between 2.3 and 5.2% of all cancer patients
(2-4).
Male sex, age, and timing of first cancer diagnosis are significant
relevant factors for multiple primary cancers (3). Multiple primary cancers in young men
are primarily due to genetic predisposition and secondarily related
to the treatment of the first cancer. In contrast, in adults, age
at diagnosis is known to be a strong factor in increasing the risk
of multiple primary cancers (5).
Cross-sectional studies have revealed that patients in their 70s
had the highest prevalence of multiple primary cancers (6), at 15% (7). Age has been reported as a predisposing
factor in many malignant tumors (8).
The total number of patients with multiple
malignancy is expected to continuously increase due to the
increased survival and longevity brought about by the development
of cancer treatment. In readiness for the increasing Japan's aging
population, clarification on the characteristics of patients with
primary malignancies and multiple primary cancers is required.
However, few studies have reported the incidence of multiple
primary cancers in patients with bone and soft tissue
malignancies.
This study aimed to analyze the clinical
characteristics of patients with multiple malignancies of the bone
and soft tissue. The incidence, frequency, prognosis, and
identification of simultaneous or heterochronous cancers were
assessed.
Materials and methods
Materials
This was a retrospective, institution-based study.
From our institutional database, 973 patients with bone or soft
tissue sarcoma were diagnosed according to the World Health
Organization histological classification (9). Of 973 cases, 89 were bone sarcoma and
884 were soft tissue sarcoma. These patients underwent surgery,
including biopsies, at our hospital from April 2008 to April 2017.
Inclusion criteria were as follows: i) Patients who underwent
surgery, including biopsies, at our hospital from April 2008 to
April 2017; ii) confirmed pathological diagnosis; and iii) patients
were diagnosed with two or more independent primary cancers
including bone or soft tissue sarcoma. We excluded patients
diagnosed with bony metastases and patients with incomplete medical
records from the study.
Overall, 30 patients with multiple primary cancers,
including bone or soft tissue sarcoma, matched these criteria. The
period from the first consultation date to the last consultation
date was defined as the follow-up interval.
Methods
Patient's age at sarcoma diagnosis, sex,
histological subtype, tumor location, clinical stage based on the
AJCC system (7th ed.), simultaneous cancer or heterochronous
cancer, history of smoking, family history, and prognosis were
reviewed.
In all cases, sarcoma surgery was performed to
produce a wide surgical margin, except in atypical lipomatous
tumors. Chemotherapy was administered to the patients with
osteosarcoma, Ewing sarcoma, rhabdomyosarcoma, and high-grade
sarcomas with unresectable and/or distant metastases. The dose
and/or intensity of chemotherapy was occasionally reduced according
to the patient's performance status (PS), age, and the general
condition of the patient. Indications for radiation therapy were as
follows: i) High risk of postoperative recurrence with marginal or
intra-surgical surgical margin, or ii) surgery could not be
performed due to poor patient condition. Informed consent was
obtained from all patients to present the data and this study was
approved by the institutional review board.
Statistical analysis
The 5-year probability of survival was calculated
using Kaplan-Meier analysis (10).
Statistical analysis was performed using the Excel Statistics
software for Windows (version 2018; SSRI Co., Ltd.).
Results
Patients and tumor histology
Of 973 patients, 30 (3.08%) had multiple bone and
soft tissue sarcomas. The median age at the time of bone or soft
tissue sarcoma diagnosis was 73.5 (range, 7-83) years; 21 patients
were male and 9 patients were female. The histological sarcoma
types were as follows: Atypical lipomatous tumor (n=5, 16.7%),
undifferentiated pleomorphic sarcoma (n=5, 16.7%), dedifferentiated
liposarcoma (n=3, 10%), leiomyosarcoma (n=3, 10%), pleomorphic
liposarcoma (n=3, 10%), chondrosarcoma (n=2, 6.7%),
myxofibrosarcoma (n=2, 6.7%), and 7 other types of sarcoma (n=1,
for each of the other 7 types, respectively) (Table I). The average follow-up was 32.6
(range, 1.1-84) months.
 | Table IPatients and tumor histology. |
Table I
Patients and tumor histology.
| Characteristics | Value |
|---|
| Total patients | 30 |
| Age, years
(range) | 73.5 (7-83) |
| Sex, n | |
|
Male | 21 |
|
Female | 9 |
| Location, n | |
|
Extremity | 20 |
|
Trunk | 10 |
| Histology, n | |
|
Atypical
lipomatous tumor | 5 |
|
Undifferentiated
pleomorphic sarcoma | 5 |
|
Dedifferentiated
liposarcoma | 3 |
|
Leiomyosarcoma | 3 |
|
Pleomorphic
liposarcoma | 3 |
|
Chondrosarcoma | 2 |
|
Myxofibrosarcoma | 2 |
|
Angioleiomyosarcoma | 1 |
|
Ewing
sarcoma | 1 |
|
Fibrosarcoma | 1 |
|
Granulocytic
sarcoma | 1 |
|
Malignant
peripheral nerve sheath tumor | 1 |
|
Extra-skeletal
myxoid chondrosarcoma | 1 |
|
Myxoid
liposarcoma | 1 |
| Clinical stage,
n | |
|
IA | 2 |
|
IB | 6 |
|
IIA | 2 |
|
IIB | 7 |
|
III | 6 |
|
IV | 7 |
Site of primary cancers
Table II shows the
data on multiple primary malignancies. Colorectal cancer was the
most common primary cancer (n=9), followed by gastric cancer (n=6),
malignant lymphoma (n=3), renal cancer (n=3), prostate cancer
(n=3), lung cancer (n=3), breast cancer (n=2), and others.
| Table IIMultiple primary malignancies. |
Table II
Multiple primary malignancies.
| Primary cancer | Number |
|---|
| Colorectal
cancer | 9 |
| Gastric cancer | 6 |
| Malignant
lymphoma | 3 |
| Renal cancer | 3 |
| Prostate cancer | 3 |
| Lung cancer | 3 |
| Breast cancer | 2 |
| Brain tumor | 1 |
| Bladder cancer | 1 |
| Cervical cancer | 1 |
| Chronic myelogenous
leukemia | 1 |
| Endometrial
cancer | 1 |
| Oesophageal
cancer | 1 |
| Osteosarcoma | 1 |
| Ovarian cancer | 1 |
| Thymic carcinoma | 1 |
| Thyroid cancer | 1 |
Simultaneous or heterochronous
There were 22 patients with double cancer, including
9 patients with simultaneous cancer and 13 with heterochronous
cancer. Five patients had triple cancer, including 1 patient with
simultaneous cancer and 4 patients with heterochronous cancers. Two
patients had quadruple heterochronous cancers and one patient was
identified with quintuple heterochronous cancers. Overall, 28.6 and
71.4% of all patients had simultaneous and heterochronous cancers,
respectively (Table III).
| Table IIISimultaneity and heterochrony. |
Table III
Simultaneity and heterochrony.
| Duplication | Simultaneity, n | Heterochrony, n | Total, n |
|---|
| Double cancer | 9 | 13 | 22 |
| Triple cancer | 1 | 4 | 5 |
| Quadruple cancer | 0 | 2 | 2 |
| Quintet cancer | 0 | 1 | 1 |
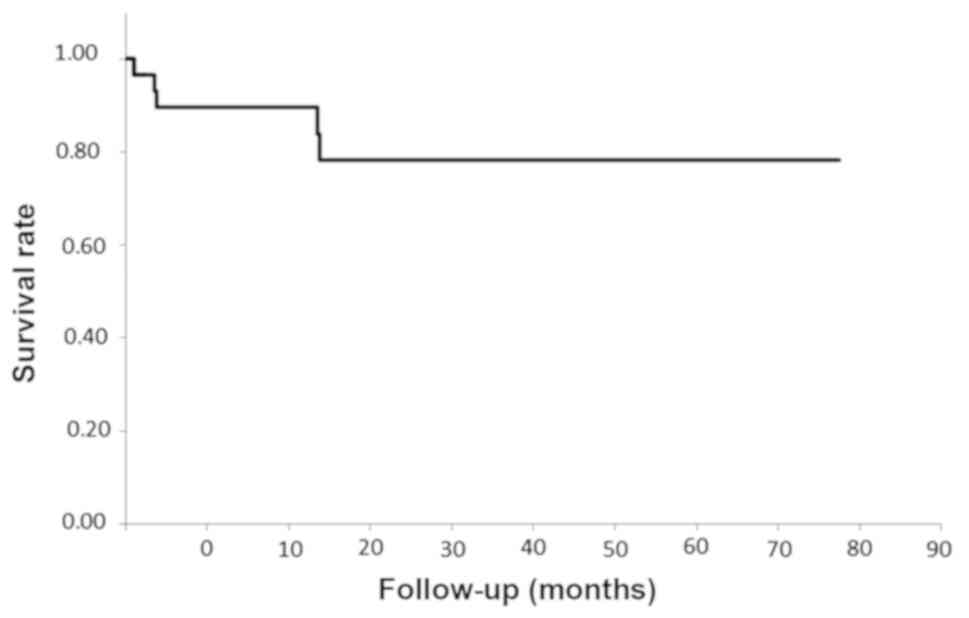
Clinical information on patients with
multiple primary malignancies
Table IV shows the
clinical data of those with multiple cancers, including bone and
soft tissue malignancies. One osteosarcoma case was suspected to be
a secondary cancer associated with Ewing sarcoma treatment
(11). The 5-year overall survival
for all patients was 75.6% (Fig.
1).
| Table IVClinical information of patients with
multiple primary malignancies. |
Table IV
Clinical information of patients with
multiple primary malignancies.
| Case | Sex | Sarcoma (age,
years) | Location | Multiple cancers
(age, years) | Timing | Smoking index | Family history | Follow-up
(months) | Outcome |
|---|
| 1 | F | Ewing (7) | Pelvis | OS (15) | Hetero. | No | No | 11 | DOD |
| 2 | F | Fibro (30) | Back | Brain (22) | Hetero. | 660 | No | 60 | NED |
| 3 | M | Myxoid lipo
(35) | Thigh | Colon (22), Liver
(31) | Hetero. | 85 | No | 23 | DOD |
| 4 | M | Angio (41) | Upper arms | CML (12) | Hetero. | No | No | 2 | NED |
| 5 | F | Leiomyo (40) | Neck | ML (22), Cervical
(23) | Hetero. | 100 | No | 39 | AWD |
| 6 | F | Chondro (41) | Humerus | Breast (39/43), ML
(44) | Hetero. | No | No | 71 | AWD |
| 7 | M | Pleomor. lipo
(55) | Lower leg | Colon (60) | Hetero. | 640 | No | 87 | NED |
| 8 | M | ALT (57) | Thigh | Spinal cord
(44) | Hetero. | No | No | 67 | NED |
| 9 | M | Granulocytic
(63) | Sternum | Colon (50), Gastric
(51) | Hetero. | 450 | No | 1 | DOD |
| 10 | F | Myxoid lipo
(58) | Armpit | Colon (58) | Simul. | No | No | 82 | AWD |
| 11 | M | Pleomor. lipo
(61) | Thigh | Colon (55) | Hetero. | 675 | No | 76 | NED |
| 12 | M | UPS (71) | Lower leg | Gastric (71) | Simul. | 900 | No | 31 | NED |
| 13 | F | ALT (72) | Head | Renal (72) | Simul. | No | No | 10 | AWD |
| 14 | M | Myxofib(70) | Abdomen | Lung (68), Gastric
(62), Renal (53), Thyroid (45) | Hetero. | No | No | 19 | NED |
| 15 | M | UPS (73) | Pelvis | Gastric (59) | Hetero. | No | No | 9 | AWD |
| 16 | M | UPS (74) | Thigh | Prostate (74) | Simul. | No | No | 3 | DOD |
| 17 | M | Dediff. lipo
(77) | Thigh | Lung (77) | Simul. | 1250 | No | 52 | AWD |
| 18 | M | ALT (77) | Thigh | Prostate (77),
Oesophagus (77) | Simul. | 1600 | No | 44 | NED |
| 19 | F | MPNST (78) | Thigh | Uterine (35) | Hetero. | No | No | 9 | AWD |
| 20 | F | Dediff. lipo
(78) | Lower leg | Ovarian (68) | Hetero. | No | Prostate
(brother) | 4 | NED |
| 21 | M | Extra chondro
(79) | Pelvis | ML (79) | Simul. | No | No | 5 | AWD |
| 22 | M | ALT (74) | Thigh | Thymic (76) | Hetero. | No | No | 67 | AWD |
| 23 | M | UPS (81) | Thigh | Colon (81) | Simul. | No | No | 2 | DOD |
| 24 | M | Dediff. lipo
(80) | Thigh | Renal (77), Bladder
(80), Prostate (81) | Simul. | No | No | 30 | NED |
| 25 | M | UPS (77) | Thigh | Gastric (75), Colon
(75) | Hetero. | 841 | No | 60 | AWD |
| 26 | M | ALT (78) | Thigh | Colon (73) | Hetero. | No | No | 49 | NED |
| 27 | M | Myxofib (82) | Buttock | Lung (83) | Simul. | 500 | No | 13 | AWD |
| 28 | M | Pleomor. lipo
(83) | Thigh | Gastric (80) | Hetero. | No | No | 4 | NED |
| 29 | M | Leiomyo (83) | Shoulder | Colon (83) | Simul. | No | No | 3 | DOD |
| 30 | F | Leiomyo (83) | Buttock | Breast (82) | Hetero. | No | Colon (mother) | 17 | NED |
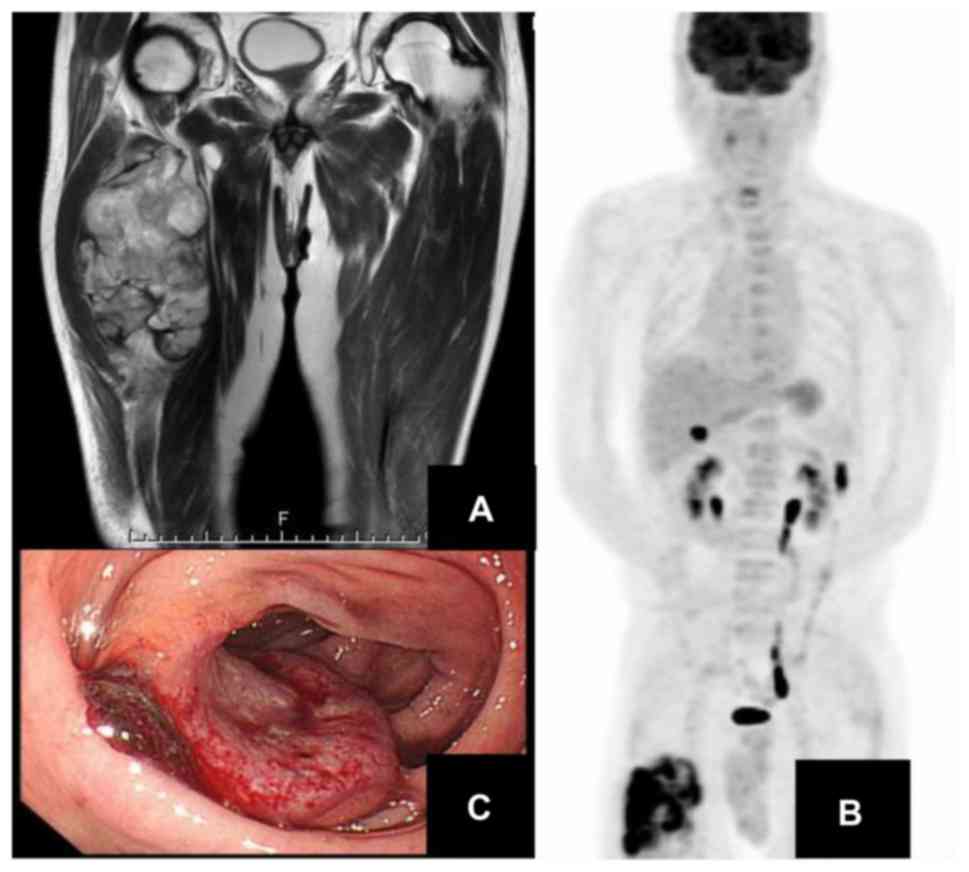
Case report
An 81-year-old man noticed a mass in his right thigh
8 months prior to his clinical presentation; after a soft tissue
tumor was identified at a local hospital, he was referred to our
hospital.
Axial T1-weighted and coronal T2-weighted magnetic
resonance images showed an iso-intense (T1) and heterogeneously
hyper-intense (T2) mass in the right vastus intermedius muscle
(Fig. 2A). Using positron emission
tomography-computed tomography, the maximum standardized uptake
value (SUV) within the tumor lesion was 16.95, with an abnormal
uptake in the colon (Fig. 2B).
Undifferentiated pleomorphic sarcoma was diagnosed based on
pathological needle biopsy assessment. We performed a wide tumor
resection. Postoperatively, colonoscopy revealed colorectal cancer
(Fig. 2C). The plan was for a
resection of the colorectal cancer; however, CT showed lymph node
metastases. Therefore, the best supportive care was selected, given
his age, activities of daily living, and general condition. He
eventually died of lung metastasis from colorectal carcinoma.
Discussion
Multiple primary cancers are defined as coexistent
cancers that occur simultaneously or sequentially in one
individual. In 1887, the first diagnostic criteria for multiple
cancer were defined by Billroth (12). Recently, the diagnostic criteria
often used are those defined by Warren and Gates in 1932. The
criteria are as follows: i) Each tumor individually presents with
malignant features at a certain state; ii) each tumor is situated
apart from the other; and iii) each tumor has been confirmed as not
being a metastasis of the other (13).
The occurrence rate of multiple primary cancers is
between 2.4 and 5.2% of all primary malignancies (2-4).
While several researches have reported multiple primary cancers,
few described multiple primary cancers focusing on bone and soft
tissue sarcoma. In this study, we identified only one patient with
double sarcoma that was diagnosed as osteosarcoma, being a
secondary cancer related to Ewing sarcoma treatment (11). Two studies have analyzed multiple
primary cancers with a focus on soft tissue sarcoma (5,14).
From the analysis of cancer registry records, 7 of 305 adults with
soft tissue sarcoma (2.3%) developed another primary malignant
cancer before or after diagnosis of soft tissue sarcoma (4). Because soft tissue sarcoma was not the
focus of the report, the characteristics of multiple primary
cancers with soft tissue sarcoma were not explored. Other studies
have investigated multiple primary cancers in patients with soft
tissue sarcoma and the incidence rate was found to be 9% (n=35/406;
with age range, 18-87 years) (5)
and 7.5% (n=28/375; with age range, 16-72 years) (14). Thus, the occurrence of multiple
primary malignancies with soft tissue sarcoma differs little from
that of other kinds of cancers. In this study, the incidence rate
of multiple primary cancers, including bone and soft tissue
sarcomas, was 3.08% (30/973), which was similar to that of multiple
primary cancers in all primary cancers.
Cancer that occurs within a year after another
cancer was detected is defined as simultaneous cancer, and cancer
occurring after 1 year of another is defined as heterochronous
cancer; our study adopted this definition. There are some reports
of simultaneous multiple primary cancers (15,16).
In this study, the rate of simultaneous multiple primary cancers
was 28.6% and the rate of heterochronous multiple primary cancers
was 71.4%.
It is necessary to distinguish between hereditary
and non-hereditary causes of multiple primary cancers. A hereditary
tumor occurs when an abnormality in one gene is inherited, along
with other genetic diseases, e.g., Li-Fraumeri syndrome, von
Hippel-Lindau disease, and multiple endocrine neoplasia (17). A hereditary tumor should be
suspected if the patient had multiple primary cancers at a younger
age or has a family history in the same organ. No patient had a
relevant family history in this study.
Kozawa et al (18) revealed that the incidence of
multiple primary cancers was 23% (23/100) in patients aged >65
years with high-grade soft tissue sarcoma. In general, older people
have a risk of multiple primary cancers (5). More than 50% of all cancers occur in
individuals aged >65 years (19). Furthermore, the accumulation of
genetic changes and inaccurate DNA repair become more common with
age (20). Advances in diagnostic
techniques and multidisciplinary treatment for patients with
malignant tumors are contributing factors to the increasing
frequency of multiple primary cancers diagnosed in older patients.
In this study, the median age was 73.5 years, which was relatively
older than that reported in previous studies.
Secondary cancers due to chemotherapy or radiation
therapy for primary cancers are also considered multiple primary
cancers. The occurrence rate of bone tumors as secondary cancers is
2.8% within 20 years, and radiation therapy-associated incidence
rates depend on the irradiation dose (21). Moreover, alkylating agents are
related to the incidence of secondary cancers in a dose-dependent
manner (22). In this study, we
presented a patient with osteosarcoma as a secondary cancer that
occurred in the right femur 7 years post treatment for left-sided
Ewing sarcoma of the pelvis. A high dose of alkylating agents was
used to treat the Ewing sarcoma (11).
Smoking is a common risk factor for multiple primary
malignancies. Cancers associated with smoking include oral,
esophageal, lung, bladder, and pancreatic cancers. Point mutations
in tumor suppressor gene p53 are familial for smoking-related
genetic changes (17). In this
study, 36.7% (11/30) of the study participants had a smoking
history which was higher than that reported in the national tobacco
smoker ratio survey, conducted by the Japan Tobacco Inc. in 2018
(17.9%) (23).
In this study, colorectal cancer was the most common
cancer (n=9) and gastric cancer was the second most common cancer
(n=6). The stomach, colon, lungs, and bladder have been listed as
organs with the highest frequency of multiple primary malignancies
(17). In combined gastric and
colorectal cancers, the frequency of microsatellite instability was
due to an abnormality in the DNA mismatch mechanism (24).
Patients with duplicated cancer are less likely to
develop metastasis, even in stages similar to those of patients
with single cancerous lesions, and the prognosis is relatively good
(25). Kozawa et al
(18) reported that prognosis for
patients with multiple cancers with soft tissue sarcoma was not
necessarily poor in elderly patients (>65 years). This may be
because careful follow-up of the first primary cancer can lead to
early detection of secondary cancer. In Japan, based on the
registry of 1,769 cases of soft tissue mass in 2015, 5-year overall
survival was about 78% (26). The
5-year overall survival rate for patients with bone sarcoma was
66.9% from 2008 to 2014, based on data from the Surveillance,
Epidemiology, and End Results (SEER) Program (27). In this study, the 5-year survival
rate of those with multiple primary cancers, including bone and
soft tissue sarcoma, was relatively good (75.6%). Early detection
of multiple primary malignancies in addition to aggressive
treatment is considered necessary for a good prognosis.
This study had several limitations. This was a
retrospective, institution-based study with a small sample size; in
addition, a relatively short follow-up period was used to identify
the definitive factors that affected patient prognosis.
Furthermore, those with an atypical lipomatous tumor, which is
considered an intermediate malignancy, were included.
In conclusion, as the frequency of multiple primary
cancers is expected to increase with the increase in the number of
elderly patients, careful follow-up after remission of primary
cancer is important. However, the occurrence of multiple primary
cancers is not necessarily associated with a poor prognosis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AS, MH and HN conceived or designed the work. AS,
NO, TI and NT collected data. AS, NO, TI and NT performed data
analysis and interpretation. AS drafted the article. MH and HN
critically revised the article. HN gave final approval of the
version to be published. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Study approval was obtained from the the Ethical
Committee of Osaka City University Graduate School of Medicine, and
all investigations were conducted in accordance with the ethical
principles of research.
Patient consent for publication
This study used only information such as medical
care information without patient invasion or intervention, and it
is not necessary to obtain direct consent from each target patient
based on the guidelines established by the government. Information
about the conduct of the research, including the purpose of the
research, is disclosed, and the opportunity for refusal is
guaranteed.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Irimie A, Achimas-Cadariu P, Burz C and
Puscas E: Multiple primary malignancies epidemiological analysis at
a single tertiary institution. J Gastrointestin Liver Dis.
19:69–73. 2010.PubMed/NCBI
|
|
2
|
Kobayashi Y, Arimoto H and Watanabe S:
Occurrence of multiple primary cancer at the National Cancer Center
Hospital, 1962-1989. Jpn J Clin Oncol. 21:233–251. 1991.PubMed/NCBI
|
|
3
|
Tsukuma H, Fujimoto I, Hanai A, Hiyama T,
Kitagawa T and Kinoshita N: Incidence of second primary cancers in
Osaka residents, Japan, with special reference to cumulative and
relative risks. Jpn J Cancer Res. 85:339–345. 1994.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ueno M, Muto T, Oya M, Ota H, Azekura K
and Yamaguchi T: Multiple primary cancer: An experience at the
Cancer Institute Hospital with special reference to colorectal
cancer. Int J Clin Oncol. 8:162–167. 2003.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tateishi U, Hasegawa T, Yamamoto S,
Yamaguchi U, Yokoyama R, Kawamoto H, Satake M and Arai Y: Incidence
of multiple primary malignancies in a cohort of adult patients with
soft tissue sarcoma. Jpn J Clin Oncol. 35:444–452. 2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Adami HO, Bergkvisit L, Krusemo U and
Persson I: Breast cancer as a risk factor for other primary
malignant diseases. A nationwide cohort study. J Natl Cancer Inst.
73:1049–1055. 1984.PubMed/NCBI
|
|
7
|
Luciani A, Ascione G, Marussi D, Oldani S,
Caldiera S, Bozzoni S, Codecà C, Zonato S, Ferrari D and Foa P:
Clinical analysis of multiple primary malignancies in the elderly.
Med Oncol. 26:27–31. 2009.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Balducci L and Ershler WB: Cancer and
aging: A nexus at several levels. Nat Rev Cancer. 5:655–662.
2005.PubMed/NCBI View
Article : Google Scholar
|
|
9
|
Fletcher CDM, Unni KK and Mertens F: World
Health Organization classification of tumors. Pathology and
genetics of tumors of soft tissue and bone. Lyon: IARC Press,
pp341-367, 2002.
|
|
10
|
Kaplan EL and Meier P:
Nonparametric-estimation from incomplete observations. J AM Stat
Assoc. 53:457–481. 1958.
|
|
11
|
Manabu H, Makoto I, Yamato K, Tokimasa S
and Nakamura H: Diagnosis of osteosarcoma in a patient previously
treated for Ewing sarcoma. Skeletal Radiol. 43:1319–1324.
2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Billroth T: Die allgemeine chirurgische
pathologie und therapie in 51 Vorlesungen: Ein handbuch fur
Studirende und Arzte, 14 Aufl. Berlin, G. Reimer, 1889. (In
German).
|
|
13
|
Warren S and Gates O: Multiple primary
malignant tumors: A survey of the literature and a statistical
study. Am J Cancer. 16:1358–1414. 1932.
|
|
14
|
Merimsky O, Kollender Y, Issakov J,
Bickels J, Flusser G, Gutman M, Lev-Chelouche D, Inbar M and Meller
I: Multiple primary malignancies in association with soft tissue
sarcomas. Cancer. 7:1363–1371. 2001.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Singh NJ, Tripathy N, Roy P, Manikantan K
and Arun P: Simultaneous triple primary head and neck malignancies:
A rare case report. Head Neck Pathol. 10:233–236. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ikeda Y, Tsukuda M, Ishitoya J, Arai Y,
Matsuda H, Katori H, Taguchi T, Yoshida T, Ono M, Sakuma Y, et al:
Four cases of simultaneous triple primary cancers of the
hypopharynx, esophagus, and stomach. Otolaryngol Head Neck Surg.
132:788–793. 2005.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Yuasa Y: Double cancer. Med Prac.
17:698–699. 2000.
|
|
18
|
Kozawa E, Sugiura H, Tsukushi S, Urakawa
H, Arai E, Futamura N, Nakashima H, Yamada Y, Ishiguro N and
Nishida Y: Multiple primary malignancies in elderly patients with
high-grade soft tissue sarcoma. Int J Clin Oncol. 19:384–390.
2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Extermann M: Management issues for elderly
patients with breast cancer. Curr Treat Options Oncol. 5:161–169.
2004.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Anismov VN: The relationship between aging
and carcinogenesis: A critical appraisal. Crit Rev Oncol Hematol.
45:277–304. 2003.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Tucker MA, D'Angio GJ, Boice JD Jr, Strong
LC, Li FP, Stovall M, Stone BJ, Green DM, Lombardi F, Newton W, et
al: Bone sarcomas linked to radiotherapy and chemotherapy in
children. N Engl J Med. 317:588–593. 1987.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Hawkins MM, Wilson LM, Burton HS, Potok
MH, Winter DL, Marsden HB and Stovall MA: Radiotherapy, alkylating
agents, and risk of bone cancer after childhood cancer. J Natl
Cancer Inst. 88:270–278. 1996.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Japan Tobacco Inc.'s annual survey. The
prevalence of smoking among Japan's adult population. https://www.jti.co.jp/corporate/enterprise/tobacco/data/smokers/index.html
(accessed 11 August 2019).
|
|
24
|
Horii A, Han H, Shimada M, Yanagisawa A,
Kato Y, Ohta H, Yasui W, Tahara E and Nakamura Y: Frequent
replication errors at microsatellite loci in tumors of patients
with multiple primary cancers. Cancer Res. 54:3373–3375.
1994.PubMed/NCBI
|
|
25
|
Baigrie RJ: Seven different primary
cancers in a single patient A case report and review of multiple
primary malignant neoplasia. Eur J Surg Oncol. 17:81–83.
1991.PubMed/NCBI
|
|
26
|
Japanese Orthopedic Association Committee
on Musculoskeletal Tumor. Soft tissue tumor registry in Japan 2015.
Tokyo: National Cancer Center. 2015.
|
|
27
|
National Cancer Institute. SEER Cancer
Stat Facts: Bone and Joint Cancer. Bethesda, MD, http://seer.cancer.gov/statfacts/html/bones.html.
|