Introduction
Solitary fibrous tumor (SFT) represent rare tumors
of mesenchymal origin and account for < 2% of all soft tissue
tumors (1,2). The etiology of SFT remains unknown
(1). Commonly, they are
slow-growing tumors with a favorable prognosis. However, cases with
malignant features have been described (3). Although SFT may be found in any site
of the body, the most common location is the thorax (1). The kidney represents an unusual
location for SFT and both diagnosis and treatment of renal SFT
remains challenging. Clinically, these tumors remain asymptomatic
for long time. Moreover, radiologic features are not specific and
renal SFT are usually diagnosed as renal cell carcinoma (RCC) and
managed as such (2). Currently,
there are no clear evidence-based guidelines for the diagnostic and
therapeutic management of these tumors, and radical nephrectomy is
the treatment of choice perferred by most authors. Definitive
diagnosis is based on histological evaluation and
immunohistochemical investigations are often required to confirm
the diagnosis. Recently, the use of immunohistochemistry for signal
transducer and activator of transcription 6 (STAT6) has been
introduced and has been showed to be highly sensitive and specific
for SFTs (4). To date, STAT6
immunoreactivity has been reported only in few cases of SFT of the
kidney (3). We describe a case of a
renal SFT incidentally discovered in a 52-year-old female
characterized by STAT6 immunoreactivity.
Case report
A 52-year-old woman presented to our outpatient
department for a routinely screening visit. She denied pain, fewer,
lower urinary tract symptoms, and hematuria. Medical history was
relevant for arterial hypertension, chronic obstructive pulmonary
disease, and intestinal polyposis. She smoked 25 cigarettes a day.
Physical examination and laboratory data failed to reveal
pathological findings. An abdominal ultrasound was required showing
a 7-cm hypoechoic lesion involving the right kidney. A
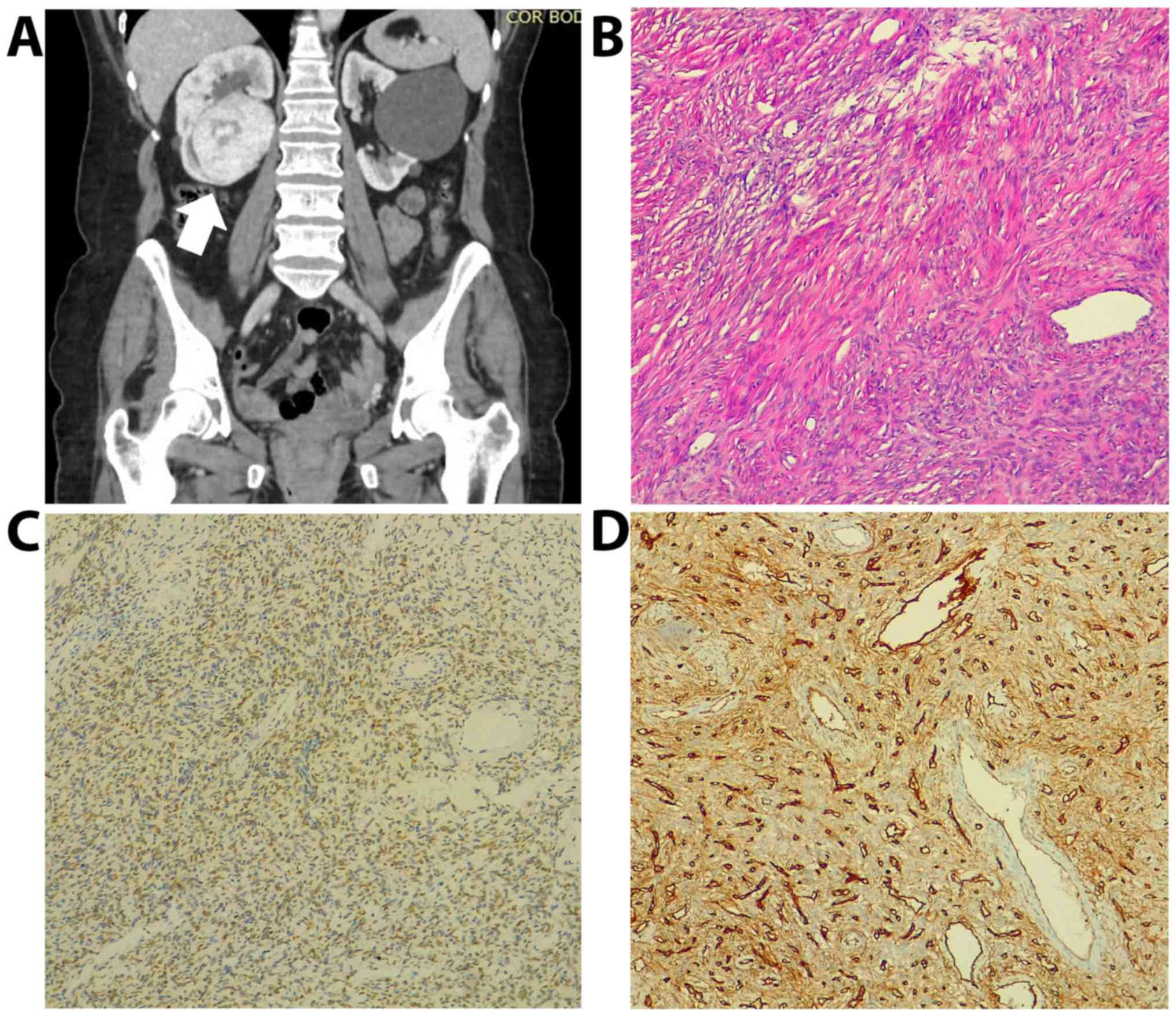
contrast-enhanced abdominal computed tomography (CT) confirmed the
presence of an inhomogeneous, 7x6 cm solid lesion involving the
lower pole of the right kidney. The mass was well-circumscribed and
contained areas of enhancement. There was no CT evidence of
vascular invasion, lymph nodes involvement or metastases. The mass
compressed the lower calyceal system and caused obstruction of the
upper calyces with subsequent hydrocalyx (Fig. 1A). The left kidney was characterized
by a 12-cm simple cystic lesion. On a subsequent Magnetic Resonance
Imaging (MRI), the lesion involving the right kidney appeared as
solid, isointense on T1-weighted images and inhomogeneous in
T2-weighted images with suspect hemorrhagic foci. The lesion was
highly hypervascular without significant wash-out of contrast
medium. No significant intralesional adipose tissue was detected.
Overall, CT and MRI imaging were judged as atypical, but highly
suspect for a malignant neoplasm. A Tc99m-DTPA renal scan revealed
a glomerulal filtration rate of 44.95 ml/min and of 84.98 ml/min on
the right, and left kidney, respectively. The patient underwent a
right laparoscopic radical nephrectomy. The intra- and
postoperative course was uneventful and the patient was discharged
home on postoperative day 8. Macroscopic examination showed a well
circumscribed, white, firm tumor confined to the lower pole which
measuring cm 7.4x6.3x5.8. There was no macroscopic capsular
involvement. Formalin-Fixed Paraffin- Embedded tissue specimens,
mounted in a thin layer on a miroscope slide covered with a jet
cover 75 by 26 mm and approximately 1 mm thick), and observed under
a microscope. Microscopic examination showed a well mesenchymal
neoplasm surrounded by fibrous tissue occasionally separated by
strip-like bands of collagen. The proliferation was composed of
long spindle cell with acidophilic cytoplasm and vesicular nuclei,
round to oval, organized in a patternless architecture with a
combination of alternating hypocellular and hypercellular areas
separated from each other by thick bands of hyalinized collagen. It
also showed a thick-walled vessel. Mitotic activity was irrelevant
and mild atypia was observed. There was no evidence of necrosis.
Immunohistochemical staining showed reactivity for CD34 and for
STAT6. These findings established the positive diagnosis of SFT of
the kidney (Fig. 1B-D).
Discussion
SFT of kidney represent a rare entity that poses
diagnostic and therapeutic challenges (5-7).
To date, a total of 56 SFT of the kidney have been reported
worldwide (5). Median age at the
diagnosis is 51 years (range: 4-85) and the incidence has been
reported to be higher in female subjects (7). Although about 15% of SFT of the kidney
have been reported to be located in the renal capsule and 3% in the
renal pelvis, the site of origin remains unknown in the majority of
cases (5). The majority of SFT of
the kidney are benign with about 14% of cases exhibiting malignant
behavior (6,7). Like RCC, most of these tumors are
asymptomatic and are incidentally discovered on radiologic
evaluations. Mean tumor size at the diagnosis is 7.6 cm (range 2-20
cm) (7). Unfortunately, imaging
features of renal SFT are non-specific. Indeed, CT may reveal
findings such as heterogeneous enhancement, areas of necrosis, and
calcifications while MRI features are highly variable. In some
cases, MRI can help in the detection of fibrosis and dense collagen
content as low signal intensity on T2-weighted images (1). However, these features overlap with
other renal neoplasm such as papillary RCC (1). The clinical case we describe
corroborates existing evidences about the diagnostic challenges
associated with clinical and radiological diagnosis of SFT of
kidney. Interestingly, the lesion we described was isointense to
the kidney in T1 weighted image and had heterogenous intensity in
T2 weighted image. This uncommon finding was also described by
Zaghbib et al (2).
Currently, renal biopsy is indicated before ablative therapy and
systemic therapy without previous pathology and in select patients
who are considering active surveillance. To date there are no
evidences about the role of renal biopsy in patients with SFT of
the kidney. Consequently, as in the present case, the definitive
diagnosis of SFT of the kidney is commonly performed after
histological and immunohistochemical examination of the surgical
specimen. Histologically SFT are mesenchymal neoplasms with
fibroblastic features that can be defined as cellular or fibrous
based on the predominant histopathologic pattern (1). The differential diagnosis of SFT of
the kidney mainly includes angiomyolipoma, fibromas, fibrosarcomas,
and sarcomatoid variant of RCC (6).
Typically, a strong CD34 immunocytochemical reactivity is found in
the fibrous variant (1). However,
this marker lacks specificity. In recent years, sequencing studies
on SFT lead to the identification of an intrachromosomal
inversion-derived gene fusion juxtaposing the neighboring NGFI-A
binding protein 2 (NAB2) gene and STAT6 gene on 12q13(8).
NAB2-STAT6 fusion is considered an initiating
pathognomonic event in both benign and malignant SFT. STAT6
immnoreactivity has recently been found to be a more sensitive and
specific marker for SFT, helpful when diagnosis is controversial
(3). To date, however, the
prognostic role of NAB2-STAT6 fusion deserves further
investigations (8). To date, no
clear evidence-based guidelines for the management of SFT of the
kidney exist. Surgical resection is the mainstay of therapy of SFT
involving the kidney (6). The role
of nephron-sparing surgery in patients with SFT of the kidney is
unclear and, currently, the standard treatment is radical
nephrectomy due to the malignant potential associated with the
disease and lack of recurrence after radical surgery (1,5).
Although most renal SFTs are benign, the behavior of
renal SFTs is unpredictable and long-term follow-up is advocated
(1).
SFT of the kidney is a rare clinic-pathological
entity characterized by challenging diagnostic work-up.
Immunostaining for CD34 and STAT6 are useful diagnostic tools.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
LDL, MaC, FC, BB, CI, VM, NL analyzed and
interpreted the clinical patient data. MaC drafted the manuscript.
FM and FF were involved in revising it critically for important
intellectual content. LI, MiC, MRC performed the histological
examination of the kidney. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The patient provided written informed consent for
the publication data and images.
Patient consent for publication
The patient provided written informed consent for
the publication data and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fursevich D, Derrick E, O'Dell MC, Vuyyuru
S and Burt J: Solitary fibrous tumor of the kidney: A case report
and literature review. Cureus. 8(e490)2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zaghbib S, Chakroun M, Essid MA, Saadi A,
Bouzouita A, Derouiche A, Slama MR, Ayed H and Chebil M: Solitary
fibrous tumor of the kidney: A case report. Int J Surg Case Rep.
62:112–114. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Yang Y, Miller CR, Clement C, Hes O and
Eyzaguirre E: Malignant solitary fibrous tumour of the kidney with
lymph node and liver metastases: Beware of STAT6 expression in
dedifferentiated liposarcoma with a solitary fibrous tumour-like
morphology: Author reply. Pathology. 49:671–672. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Geramizadeh B, Marzban M and Churg A: Role
of immunohistochemistry in the diagnosis of solitary fibrous tumor,
a review. Iran J Pathol. 11:195–203. 2016.PubMed/NCBI
|
|
5
|
Kopel J, Sharma P and Warriach I: A
solitary fibrous tumor of the kidney. Urol Case Rep.
28(101072)2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wang H, Liao Q, Liao X, Wen G, Li Z, Lin C
and Zhao L: A huge malignant solitary fibrous tumor of kidney: Case
report and review of the literature. Diagn Pathol.
9(13)2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Cuello J and Brugés R: Malignant solitary
fibrous tumor of the kidney: Report of the first case managed with
interferon. Case Rep Oncol Med. 2013(564980)2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tai HC, Chuang IC, Chen TC, Li CF, Huang
SC, Kao YC, Lin PC, Tsai JW, Lan J, Yu SC, et al: NAB2-STAT6 fusion
types account for clinicopathological variations in solitary
fibrous tumors. Mod Pathol. 28:1324–1335. 2015.PubMed/NCBI View Article : Google Scholar
|