Introduction
Cholangiocarcinoma (CCA) is the most common cancer
in the Northeast Thailand, especially in Khon Kaen region, although
the global incidence of CCA is low (1,2). CCA
is a malignant transformation of bile duct epithelium and can be
anatomically classified into intrahepatic and extrahepatic types
(3). While the former type is
common in the Greater Mekong Subregion including Northeast
Thailand, in relation to infection with carcinogenic liver fluke,
Opisthorchis viverrini, the latter is common in the rest of
the world (4). Currently CCA
patients are treated with surgery, radiotherapy and chemotherapy.
However, prognosis of intrahepatic CCA patients is extremely poor
because intrahepatic CCA is a silent tumor with rapid growth and
frequent metastasis, and reliable diagnostic markers have yet to be
identified (4,5). CCA genesis and progression are
multifactorial events. In liver fluke infection-associated
intrahepatic CCA, inflammatory cytokines, especially IL-6, play
roles in carcinogenesis and tumor progression (6,7).
However, little is known about the contribution of other cytokines
to CCA genesis and progression.
IL-25, also known as IL-17E, is a newly identified
member of the IL-17 family of inflammatory cytokines (8). It is produced by Th-17 cells and many
other cells, including mast cells, alveolar macrophages,
eosinophils and intestinal and respiratory epithelial cells
(9,10). IL-25 can induce the production of
various Th2-type cytokines such as IL-4, IL-5 and IL-13, which are
the key regulators of inflammatory and autoimmune diseases
(9,11). In relation to cancer, IL-25 produced
from tumor-associated fibroblasts can suppress metastasis of
mammary tumor (12). Presence of
IL-25 producing tumor-associated macrophages is a predictor for the
good prognosis of gastric cancer (13). According to ‘A pathology atlas of
the human cancer transcriptome’ by Uhlen et al, several
cancer types including CCA were positive for IL-25 protein
(14). In a previous study, using
secretome analysis of three CCA cell lines and one immortile
cholangiocyte cell line MMNK-1, it was found that APEX-1 was
overexpressed in CCA cell lines and serum APEX-1 level was a
potential biomarker for CCA (15).
In that study, several cytokines including IL-25 and some
cytokine-related molecules were upregulated in CCA cell lines.
In this study, therefore, using the same secretome
database, we first carried out a precise analysis on the expression
levels of cytokines and cytokine-related molecules in CCA cell
lines. The results showed that 6 cytokines and related molecules
were overexpressed in at least 2 of 3 CCA cell lines with the
predominant overexpression of IL-25. Then, using
immunohistochemistry, we examined IL-25 expression in CCA tissues
and found that IL-25 expression was significantly higher in the
cancerous tissue compared with the adjacent non-cancerous tissue.
In addition, the overexpresison of IL-25 in CCA was associated with
metastatic status and poor prognosis of CCA patients.
Patients and methods
Patients and specimens
The paraffin-embedded pathologically confirmed CCA
tumor tissue specimens from 20 patients were provided by the
Cholangiocarcinoma Research Institute (CARI), Faculty of Medicine,
Khon Kaen University, Thailand. The patients underwent surgery at
the Srinagarind Hospital, Khon Kaen University, between November
2010 and June 2012. According to reports from pathologists, 13 out
of 20 patients were positive for lymph node metastasis while 7
patients were negative for metastasis. In addition, 15 fresh frozen
CCA tissues together with the sera of corresponding patients were
also provided from CARI and Khon Kaen University (KKU), for protein
extraction. Tissues and sera that were used in this study were all
left-over specimens obtained during surgical treatment. Written
informed consent for the use of left-over specimen for research
purpose was obtained from the attending physicians prior to surgery
and the original copies of the documents were kept in CARI and KKU.
This series of experiments haves been approved (HE571283) by the
Ethics Committee of Khon Kaen University, Thailand, and all
specimens were anonymously coded according to the guidelines.
Required sample size of CCA tissues was calculated using PS: Power
and Sample Size Calculation version 3.1.2., Department of
Biostatistics, Vanderbilt University (16).
Candidate protein selection
To identify overexpressed proteins secreted from CCA
cells, previously we constructed a secretome database from three
CCA cell lines, KKU-213A, KKU-213B and KKU-100, and a control
immortalized cholangiocyte cell line, MMNK1(17). In brief, the cell lines were
cultured in Ham's F-12 culture medium supplemented with 10% fetal
bovine serum, 100 U/ml of penicillin and 100 µg/ml of streptomycin
at 37˚C in 5% CO2 air atmosphere. When the cells were
grown to 70% confluency, they were extensively washed with PBS
followed by serum-free medium. Then, the cells were incubated in 12
ml of serum-free medium in 15-cm dishes for 24 h. The conditioned
media containing secreted proteins were harvested and centrifuged
at 600 x g for 10 min to remove cell debris. The conditioned medium
samples were concentrated and desalted using Amicon ultra-15 tubes
(MW cut-off 3 kDa), centrifuged at 4,000 x g for 50 min at 4˚C, and
the supernatants were stored as secretome samples at -20˚C until
use.
Fifty micrograms of the secretome samples (15 µg
protein each) were dissolved in sample buffer, boiled for 5 min,
and were separated on 12.5% SDS-PAGE (ATTO AE-6530 system). After
electrophoresis, the gel was fixed, sensitized with 0.02%
Na2S2O3 for 2 min, and then
stained with silver nitrate solution (0.2% AgNO3) and
color developing solution. The stained gel was washed and scanned
using a GS-710 scanner (Bio-Rad) and stored in 0.1% acetic acid
until use.
For in-gel tryptic digestion, the gel lanes were
divided into 5 wide ranges according to the standard protein
markers and then sub-divided into 15 ranges. Each gel range was
chopped into small sections (1 mm3/section), and
transferred to 96-well plate (5-10 sections/well). The gel sections
were dehydrated twice in 100% acetonitrile and cysteine bonds were
reduced with dithiothreitol, and then alkylated with 100 mM
iodoacetamide. After reduction and alkylation, the gel sections
were dehydrated with 100% acetonitrile and tryptic digestion was
performed overnight at room temperature. The digested peptides were
extracted from the gel three times. Finally, the tryptic peptide
mixtures were dried and kept at -80˚C.
LC-MS/MS analysis
The extracted peptides sample was dissolved in 15 µl
of 0.1% formic acid, centrifuged at 12,000 x g for 5 min at 37˚C,
and then injected into LC-MS/MS system. Briefly, the peptides were
separated using a Dionex-Ultimate 3000 LC System. The mobile phase
A (0.1% formic acid) and the mobile phase B (0.1% formic acid in
50% ACN) were used to elute peptides using a multistep gradient of
10-70% of mobile phase B at 0-13 min (the time-point of retention),
90% of mobile phase B at 13-15 min, followed by a decrease to 10%
of mobile phase B at 15-20 min. Peptide fragment mass spectra were
acquired in data-dependent AutoMS mode with a scan range of
300-1,500 m/z; 3 averages and up to 5 precursor ions selected from
the MS scan of 50-3,000 m/z.
DeCyderMS differential analysis software (DeCyderMS,
GE Healthcare) was used for the quantitation of peptides based on
MS precursor signal intensities of individual LC-MS spectra. The
quantitation of peptides was performed using the PepDetect module.
From the secretome database analyses using the PepDetect and
PepMatch modules followed by the Mascot software search, we
identified that 1,138 proteins were commonly upregulated in at
least two CCA cell lines compared with those of MMNK1 cells.
Of 1,138 proteins, six proteins were identified as
cytokine and cytokine-related molecules (IL-28A,
interferon-stimulated exonuclease, IL-25 isoform 1, Dermokine-β2,
TGF-β1 and C-C chemokine receptor type 1) (Table I).
 | Table IExpression levels of the
cytokine-related molecules from the secretome data of fold
difference in CCA cell lines compare with control. |
Table I
Expression levels of the
cytokine-related molecules from the secretome data of fold
difference in CCA cell lines compare with control.
| | Cell line |
|---|
| Secreted
proteins | KKU-100 | KKU-213A | KKU-213B |
|---|
| IL-25 isoform 1
precursor | 6.9a | 0.7a | 7.6a |
| IL-28A | 2.4 | 1 | 4 |
| Interferon
stimulated exonuclease | -2.4 | -0.8 | -2 |
| Dermokine-β2 | 1.4 | 1.6 | -0.9 |
| TGF-β1 | -0.2 | -0.8 | 1.3 |
| C-C chemokine
receptor type 1 | 0.3 | 2.5 | 0.6 |
Immunohistochemistry
The sections of 20 paraffin-embedded CCA tissues
were cut at 4 µm thickness and deparaffinized by soaking in xylene
for 2 min, and rehydrated in a descending series of ethanol
(absolute, 95 and 70%) and then transferred into citrate buffer (pH
6.0). The sections in citrate buffer were boiled for 10 min and
washed in PBS. Endogenous peroxidase activity of the sections was
blocked with 3% H2O2 in methanol for 1 h in
the dark and then non-specific background binding was blocked with
20% fetal bovine serum for 2 h. The sections were incubated with
150 µl of rabbit polyclonal antibody against human IL-25 (Biorbyt)
at 1:300 dilution at 4˚C overnight. A tissue section for the
representative of negative control skipped this step. The sections
were washed in PBS-T and incubated with 150 µl of
peroxidase-labelled goat anti-rabbit Ig antibody of the EnVision
System DakoCytomation Inc.) for 1 h and developed the signal using
3,3'-diaminobenzidine (DakoCytomation) for 5 min in the dark. The
sections were washed with running tap water until clear and
counterstained with hematoxylin for 10 min. The sections were
dehydrated in the ascending series of ethanol and cleared in
xylene. Finally, the sections were mounted with
Permount® and sealed with a cover glass (18).
Evaluation of IL-25 expression in CCA
tissues by immunohistochemistry
The staining patterns of IL-25 protein in CCA
tissues were assessed microscopically at magnification, x400 using
H-score, recording both the intensity of staining (0, no staining;
1+, weak staining; 2+, moderate staining; and 3+, strong staining)
and the percentage of tumor cells stained (0-100%) leading to the
range of H-score 0-300 to each sample. The results were read around
10 fields per sample to decrease variation of detection. The
H-score was calculated as a sum of the intensity as follows;
H-score=(% of positively stained tumor cells at weak intensity x1)
+ (% of positively stained tumor cells at moderate intensity x2) +
(% of positively stained tumor cells at strong intensity x3).
Lastly, H-scores of 10 fields were averaged (19).
Protein extraction from surgical
specimen of CCA
The methods for protein extraction from solid
tissues followed those described previously (20-22).
Approximately 100-200 mg of freshly frozen cancerous and its
adjacent noncancerous tissues were obtained from 15 cases of human
CCA surgical materials. The tissues were separately washed with
ice-cold phosphate-buffered saline (PBS, 0.1 M sodium phosphate,
0.15 M sodium chloride, pH 7.2) to remove any blood clots and
excess connective tissues. Proteins were extracted using a T-PER™
Tissue Protein Extraction Reagent for Tissue (Thermo Fisher
Scientific). Firstly, tissue lysis buffer was prepared by adding
the protease inhibitor cocktail (cOmplete™, Roche) and phosphatase
inhibitor cocktail (PhosSTOP™, Roche) to the T-PER reagent just
before use according to the manufacturer's instructions with some
modifications. In brief, human CCA and adjacent non-cancerous
tissues were separately minced in 500 µl each of the tissue lysis
buffer and approximately 40-80 dounce strokes were carefully
homogenized on ice (23). The tubes
were centrifuged at 3,000 x g for 5 min at 4˚C to spin down
unbroken tissues and cell debris. The supernatants were collected
and protein contents were determined using the Bradford protein
assay (Thermo Fisher Scientific) method (24).
Western blot analysis
To investigate IL-25 protein expression in CCA and
adjacent non-cancerous tissues by semi-quantitative, western
blotting with ß-actin as a loading control was performed. All 15
samples of cancerous and noncancerous tissue proteins (30 µg
protein for each sample) were mixed with 4X loading dye at 1:4
proportion, and boiled for 5 min. The protein samples were loaded
on 12.5% SDS-PAGE and run at 150 V for 1 h in the cold room. The
electrophoresis was completed when the dye reached the end of the
gel, and the separated proteins were transferred onto PVDF membrane
at 300 V for 1 h at room temperature. The membrane was blocked with
5% skim-milk in 1X TBST for 1 h at room temperature. The membrane
was then incubated with 1:500 dilution of a primary antibody,
rabbit polyclonal antibody against human IL-25 (Biorbyt) overnight
at 4˚C. Next, the membrane was washed 3 times with 1X TBST for 10
min each, then incubated with 1:10,000 dilution of horseradish
peroxidase-conjugated goat anti-rabbit IgG-secondary antibody for 1
h at room temperature, followed by washing 3 times with 1X TBST 10
min each. Finally, the chemiluminescence was detected using an ECL
plus system (GE Healthcare) and visualized using Amersham Imager
600.
Potential interaction analysis
Potential interaction of the identified protein was
analyzed using the public-domain software STITCH 5.0, the search
tool for interacting chemicals known as STITCH 5.0 (date of access:
11/02/2019) (25,26). Interaction was performed for IL-25
signaling, which correlated with the metastatic pathway. In brief,
a set of input page icons of the software was shown at the start
page. The page icon named ‘multiple names’ was selected. The list
of proteins of interest was keyed in, e.g., IL-25 and/or other
specified metastatic proteins and an item ‘Homo sapiens’ was
selected as the organism, and then ‘SEARCH’ was clicked. The new
popup page with the list of the protein names of interest, for
example IL-25, and other proteins were identified and ‘Continue’
was clicked. The subsequent popup new page showed the confidence
view.
Statistical analyses
Statistical analyses were performed using SPSS
v.16.0 software (SPSS Inc.) and GraphPad Prism v.5 software
(GraphPad Software Inc.). The data were presented as mean ± SD and
the range (minimum to maximum). Shapiro Wilk and Kolmogorov Smirnov
normality tests were used to check normal distribution of the data.
The statistical difference between groups was determined using an
unpaired t-test. The correlation between groups was investigated
using Pearson's correlation. Cumulative survival time was
calculated using a Kaplan-Meier method and analyzed by log-rank
test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Selection of IL-25 from secretome
database analysis
Inflammatory cytokines play key roles in CCA
carcinogenesis (7). We identified 6
cytokine-related molecules which were over-expressed in the
secretomes of CCA cell lines compared with the immortal
cholangiocyte cell line, MMNK1. Those are interleukin 25 isoform 1
(IL-25), interleukin 28A (IL-28A), interferon-stimulated
exonuclease gene 20 (ISG20HEM45CD25), dermokine-β2, transforming
growth factor beta 1 (TGF-β1) and CC chemokine receptor (CCR) type
1 (Table I). Of those, IL-25 was
found to be the most overexpressed cytokine at least in two CCA
cell lines, KKU-100 and KKU-213B. Although IL-28A was also
overexpressed, the degree of overexpression of IL-28A was far less
than that of IL-25. Thus, IL-25 was chosen for further
analysis.
Immunohistochemical detection of IL-25
protein in CCA tissues
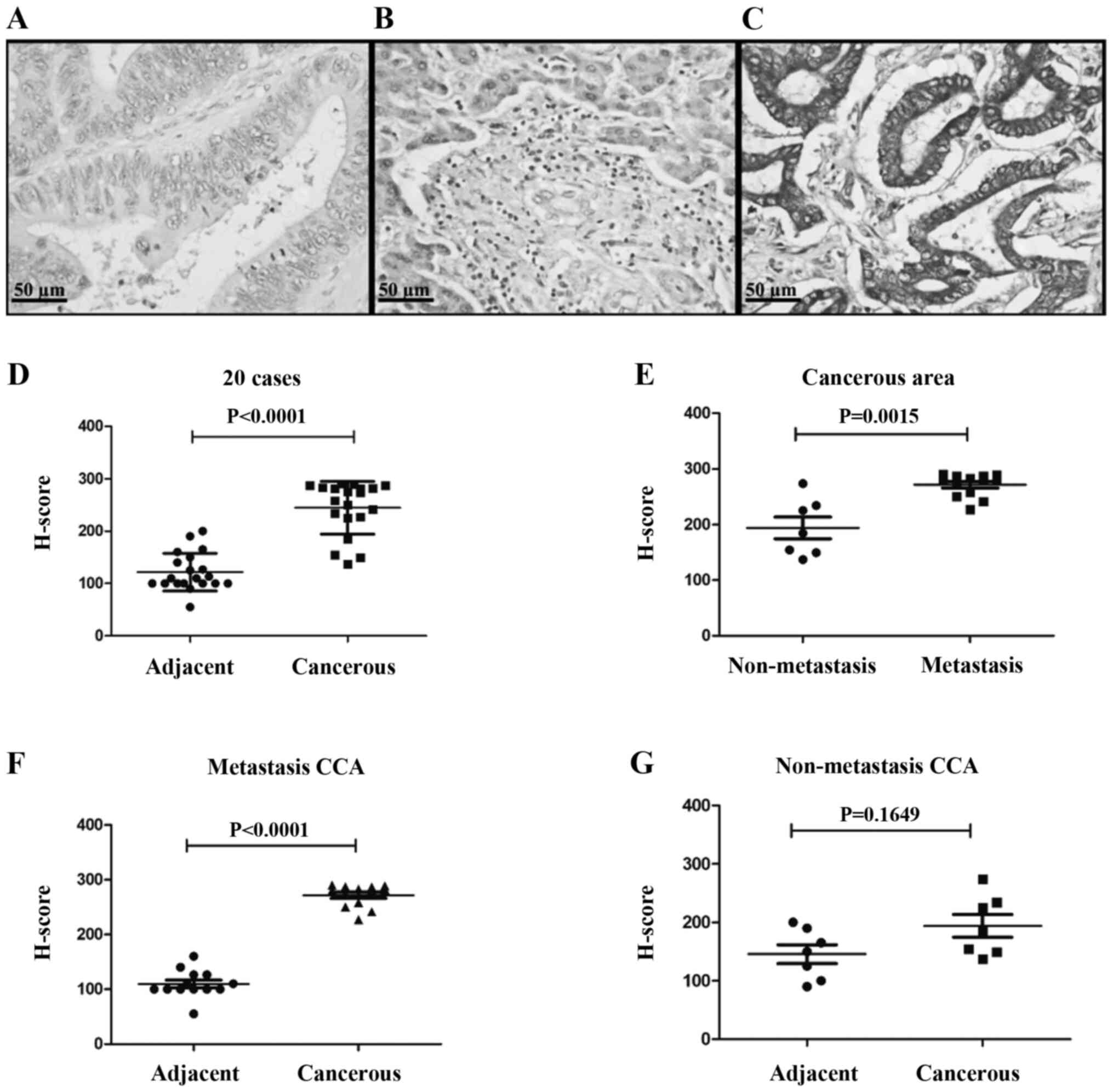
IL-25 expression was investigated for 20 CCA tissues
using immunohistochemistry, and the representative images of
negative control, cancerous area and adjacent area of CCA tissues
are shown in Fig. 1. Fig. 1A is a negative control staining of
CCA tissue. In the adjacent area to the CCA tissue, a monolayer of
normal cholangiocytes of the bile duct epithelium were stained with
pale brown (Fig. 1B). In cancerous
area, CCA cells were stained with dark brown in color showing high
expression of IL-25 in the cytoplasm (Fig. 1C). The scatter plot revealed that
the mean H score of cancerous tissues was significantly higher
(P<0.0001) than that of the normal bile ducts in the adjacent
non-cancerous tissue (Fig. 1D).
Since IL-25 is known to play a role in tumor
metastasis (7,20), CCA patients were divided into two
groups, those with and without metastasis, and IL-25 expressions
levels in the cancerous area of both groups were compared. As shown
in Fig. 1E, IL-25 expression level
in cancerous area of the patients with metastasis group was
significantly higher (P=0.0015) than that of the non-metastasis
group. When IL-25 expression levels in cancerous and non-cancerous
tissues of these two groups were compared, cancerous tissues were
overexpressed as compared to the metastasis group and the
difference was statistically significant (Fig. 1F, P<0.0001) but not in the
non-metastasis group (Fig. 1G,
P=1.6490).
IL-25 protein levels in CCA
tissues
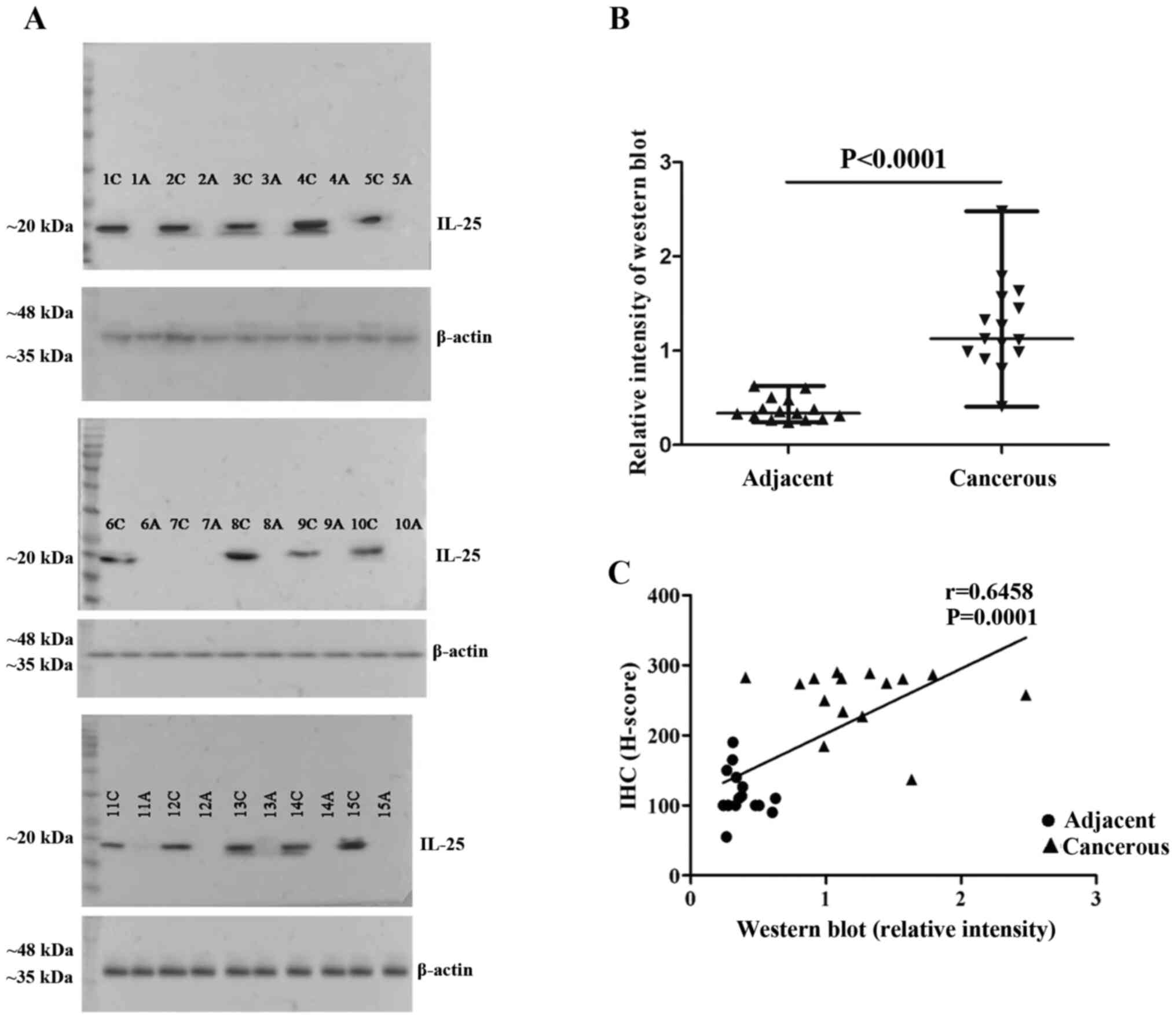
Fifteen frozen tissue specimens were used to
determine IL-25 protein expression in cancerous and non-cancerous
areas of CCA tissues. The proteins were extracted from each pair of
tissues separately and western blot analysis was performed. The
results revealed that IL-25 protein was strongly expressed in all
15 cancerous tissues but not in the adjacent non-cancerous tissues
(Fig. 2A), similar to the IHC
results. The relative intensity of IL-25 protein levels in
cancerous tissues was higher than that of the adjacent
non-cancerous tissues (Fig. 2B).
The IL-25 expression levels via western blot analysis were
correlated well with the expression levels determined by IHC
(Fig. 2C).
Association between IL-25 expression
in CCA tissues and the clinical parameters of the patients
To determine the association between IL-25
expression in CCA tissues and clinical parameters of the patients,
CCA patients were divided into high and low IL-25 expression groups
using the median value (265.71) of the H score of all 20 CCA
specimens as the cut-off value. Then, the patients' clinical
parameters were compared between high and low IL-25 expression
groups. The results showed that a higher IL-25 expression was
significantly associated with high frequency of lymph node
metastasis and shorter survival time (P=0.0369, P=0.0232; Table II).
| Table IIComparison of patients clinical
parameters between high IL-25 expression and low IL-25 expression
groupsa. |
Table II
Comparison of patients clinical
parameters between high IL-25 expression and low IL-25 expression
groupsa.
| Clinical
parameters | Low IL-25
expressionb
(median) | High IL-25
expressionb
(median) |
P-valuec |
|---|
| Age (years) | 56 | 59.5 | 0.6228 |
| Lymph node
metastasis | 1/10 | 10/10 | 0.0369a |
| Survival time
(days) | 784 | 203 | 0.0232a |
| Aspartate
aminotransferase (U/l) | 45.5 | 120.5 | 0.1403 |
| Alanine
aminotransferase (U/l) | 35 | 73 | 0.3443 |
| Alkaline
phosphatase (U/l) | 161 | 140 | 0.5966 |
| Total bilirubin
(mg/dl) | 0.7 | 2.35 | 0.3237 |
| Direct bilirubin
(mg/dl) | 0.3 | 1.5 | 0.1486 |
| Total protein
(mg/dl) | 7.4 | 7.85 | 0.5964 |
| Albumin
(mg/dl) | 3.9 | 3.7 | 0.9395 |
| Globulin
(mg/dl) | 3.2 | 3.45 | 0.9397 |
| Cholesterol
(mg/dl) | 183.5 | 184 | 0.9397 |
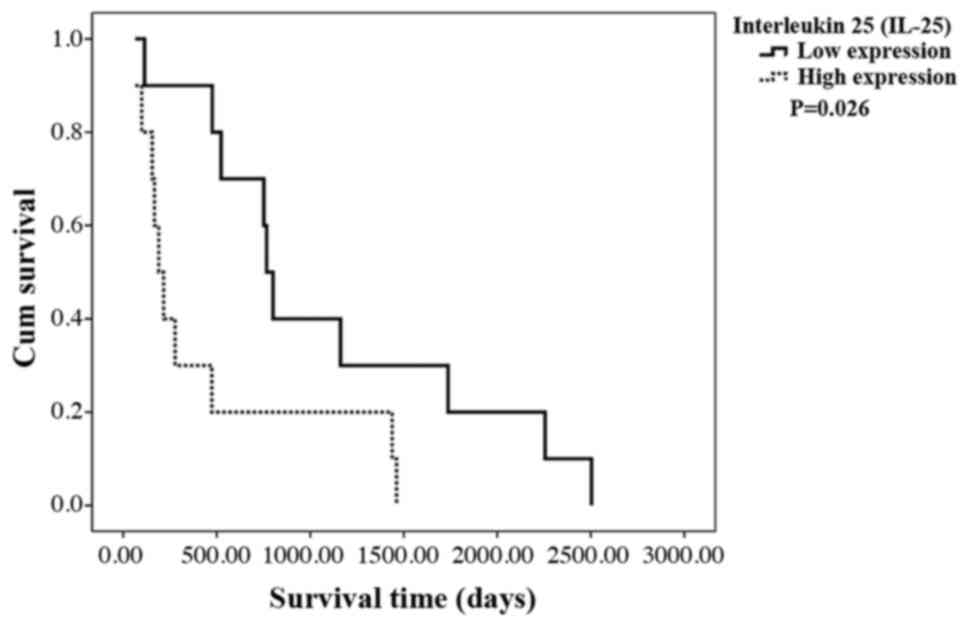
Survival time analysis of CCA
patients
Since the mean survival time of CCA patients was
significantly shorter in patients with high IL-25 expression in CCA
tissues, the overall survival (OS) of the patients in relation to
IL-25 expression level in CCA tissues was analyzed using a
Kaplan-Meier method and log-rank test. The results showed that
patients with a high IL-25 expression had shorter OS than those
with a low IL-25 expression (P= 0.0260; Fig. 3).
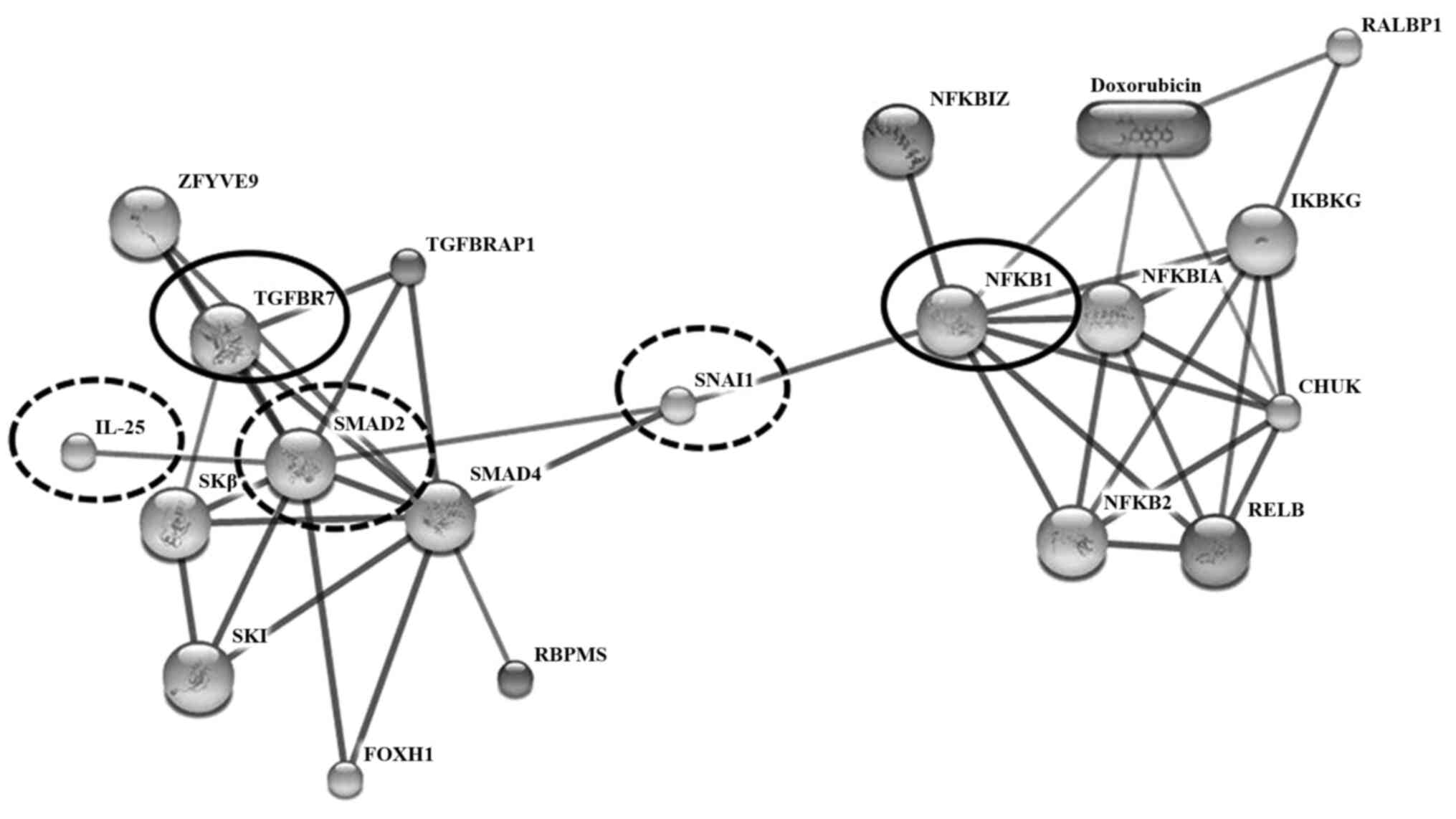
IL-25 protein interaction
To determine the potential role of IL-25 in CCA
metastasis, possible interaction of IL-25 with cancer
metastasis-related proteins was predicted using STITCH version 5.0
(Fig. 4). The results showed that
IL-25 directly interacted with SMAD family member 2 (SMAD2) and
indirectly interacted with transforming growth factor-beta 1
(TGF-β1). The expression of the TGF-β family signaling molecule
SMAD2 and TGF-β1 could elevate levels of IL-25(27). Moreover, the results revealed that
nuclear factor kappa-light-chain-enhancer of activated B cells
(NF-κB), Snail homolog 1 (Drosophila; SNAI 1) and
epithelial-mesenchymal transition (EMT) were indirectly interacted
with IL-25 with the high confidence score >0.7 (Fig. 4). Thus, SNAI 1 was enhanced by NF-κB
and SNAL 1-induced EMT involved the loss of E-cadherin and claudins
with concomitant upregulation of vimentin and fibronectin, among
other biomarkers; EMT is associated with metastasis (28).
Discussion
IL-25 is a newly identified inflammatory cytokine
involved in inflammation and autoimmune diseases (13). It is produced not only from immune
or inflammatory cells but also from epithelial cells. IL-25 protein
is also detected in several types of cancer (14), tumor-associated microenvironments
and implicated in tumor progression (12,29-32).
In this study, using immunohistochemical methods, we clearly
demonstrated that IL-25 is overexpressed in the majority of CCA
tissues. Overexpression of IL-25 in CCA is correlated with lymph
node metastasis and shorter survival time of the patients.
As was suggested by Ji and Zhang, the role of Th17
cells including IL-25 producing cells in cancer is a disputable
topic (31). In particular, IL-25
is produced, not only by immune inflammatory cells but also by
mucosal epithelial cells and also by some cancer cells, as
mentioned earlier. In this study, IHC and western blot analysis
revealed active IL-25 production by the majority of CCA cancer
cells compared with the adjacent non-cancerous tissues. Although we
have not quantified, accumulation of IL-25 producing
immune/inflammatory cells was not clearly seen in the cancer
stroma. Thus, IL-25 from CCA cells may exert its regulatory role on
cancer cells themselves on the one hand, while simultaneously
modulating immune inflammatory cells in the tumor microenvironment.
Thus, the role of IL-25 in cancer should be analyzed for both the
producing and target cells.
IL-25 produced and secreted from CCA cells may
confer its regulatory function on tumor cells in various ways. The
simplest explanation is that, as with other cytokines, it may
directly act as an autocrine or paracrine hormone to regulate
biological function of CCA cells. To test this possibility, IL-25
receptor expression on CCA cells should be determined. While our
present results suggested growth promotion activity of IL-25 to CCA
cells, Furuta et al reported that IL-25 can induce
caspase-dependent apoptosis of IL-25R-positive breast cancer
(32). Antitumor activity of IL-17E
(IL-25) against human melanoma, colon adenocarcinoma, NSCLC, breast
cancer, pancreatic cancer was demonstrated in murine xenograft
model (33).
Alternatively, IL-25 from CCA cells may modulate
tumor microenvironment in various ways. For example, IL-25
activates innate lymphoid cells (ILCs) which promote organ fibrosis
(34). Periductal fibrosis is a
hallmark of CCA genesis in association with elevation of serum IL-6
levels. However, IL-6 was not detected in our secretome database
(6). IL-25 is known to promote
airway angiogenesis in asthmatic patients (35). IL-17 (including IL-17E/IL-25)
promotes non-small cell lung cancer (NSCLC) growth via angiogenesis
(36).
In the present study, a high expression of IL-25 in
CCA cells is associated with tumor metastasis and shorter survival
time of the patients. Concerning the role of IL-25 in tumor
metastasis, Jiang et al (30) demonstrated a critical role of IL-25
in promoting tumor metastasis through modulating type 2 immune
response via targeting Th2 cells in breast cancer model. They also
found that IL-25 was expressed in all four major histopathological
types of human breast cancer (29).
In addition, in gastric cancer, the degree of infiltration of
IL-25-positive tumor-associated macrophages in tumor tissues is
correlated with the longer overall survival (13).
STITCH analysis for the interaction of IL-25 with
other molecules supported our results that IL-25 correlated with
molecules involved in tumor metastasis. IL-25 pathway induces
activation of NF-κB (37). NF-κB is
known as a pivotal regulator of the epithelial mesenchymal
transition (EMT) via SNAI 1 and EMT associated with metastasis in a
model of breast cancer progression (38). Thus, SMAD 2, which is an
intracellular signal transducer and transcriptional modulator was
activated by TGF-β1, and the activated SNAI 1 can induce EMT in
lung cancer (39).
A limitation of this study was the small sample
size. Therefore, a larger sample size should be used in future
studies for the identification of the clinical significance of
IL-25 in CCA genesis, progression and prognosis.
In summary, we have demonstrated that IL-25 was
expressed strongly in some, but not all of CCA cells/tissues.
Further functional studies are needed to shed more light on the
mechanisms by which IL-25 functions on CCA cells themselves and on
the tumor microenvironment by using gene silencing and
overexpression of IL-25 in CCA cell lines.
Acknowledgements
We thank Montira Janan for secretome database
support at the National Center for Genetic Engineering and
Biotechnology (BIOTEC), the National Science and Technology
Development Agency (NSTDA). We would like to thank Professor
Yukifumi Nawa for manuscript editing, along with the Publication
Clinic of the Research Affairs, Khon Kaen University for grant
support. We thank Dr Sittiruk Roytrakul, National Center for
Genetic Engineering and Biotechnology (BIOTEC), National Science
and Technology Development Agency, Pathumthani, Thailand, for
suggestions on secretome interpretation, Professor Sopit Wongkham
and Associate Professor Chaisiri Wongkham (Department of
Biochemistry, Faculty of Medicine, Khon Kaen University, Khon Kaen
40002, Thailand), for study design comments.
Funding
This project was supported by grants from the Khon
Kean University (MRG5280033), the Centre for Research and
Development of Medical Diagnostic Laboratories (CDML), Faculty of
Associated Medical Sciences, Khon Kaen University and the
Cholangiocarcinoma Research Institute (CARI), Faculty of Medicine,
Faculty of Associated Medical Sciences, Khon Kaen University.
Availability of data and materials
The materials using and the data analysis during
this study are available from the corresponding author on
reasonable request.
Authors' contributions
SK performed experiments and data analysis. TP, TL,
PT and SP conceived the study and revised the manuscript. AT
collected CCA tissue samples and were involved in conceptualization
of the study design. Methodology was completed by SK, DT, AT and
PS. PS contributed to suggest histological grading. SK drafted the
original manuscript. All authors have read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
This study protocol was approved by the Human Ethics
Committee of Khon Kaen University, Thailand (HE571283). Tissues and
sera that were used in this study were all left-over specimens
obtained during surgical treatment. Written informed consent for
the use of left-over specimens for research purpose were obtained
from the attending physicians prior to surgery and the original
copies of the documents were kept in the CARI and KKU.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kamsa-Ard S, Luvira V, Suwanrungruang K,
Kamsa-Ard S, Luvira V, Santong C, Srisuk T, Pugkhem A,
Bhudhisawasdi V and Pairojkul C: Cholangiocarcinoma trends,
incidence, and relative survival in Khon Kaen, Thailand from 1989
through 2013: A population-based cancer registry study. J.
Epidemiol:1–8. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Jusakul A, Kongpetch S and Teh BT:
Genetics of opisthorchis viverrini-related cholangiocarcinoma. Curr
Opin Gastroenterol. 28:258–263. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Blechacz B: Cholangiocarcinoma: Current
knowledge and new developments. Gut Liver. 11:13–26.
2017.PubMed/NCBI View
Article : Google Scholar
|
|
4
|
Wongkham S and Silsirivanit A: State of
serum markers for detection of cholangiocarcinoma. Asian Pac J
Cancer Prev. 13:17–27. 2012.PubMed/NCBI
|
|
5
|
Tshering G, Dorji PW, Chaijaroenkul W and
Na-Bangchang K: Biomarkers for the diagnosis of cholangiocarcinoma.
Am J Trop Med Hyg. 98:1788–1797. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sripa B, Thinkhamrop B, Mairiang E, Laha
T, Kaewkes S, Sithithaworn P, Periago MV, Bhudhisawasdi V,
Yonglitthipagon P, Mulvenna J, et al: Elevated plasma IL-6
associates with increased risk of advanced fibrosis and
cholangiocarcinoma in individuals infected by opisthorchis
viverrini. PLoS Negl Trop Dis. 6(e1654)2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yongvanit P, Pinlaor S and Bartsch H:
Oxidative and nitrative DNA damage: Key events in
opisthorchiasis-induced carcinogenesis. Parasitol Int. 61:130–135.
2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hurst SD, Muchamuel T, Gorman DM, Gilbert
JM, Clifford T, Kwan S, Menon S, Seymour B, Jackson C, Kung TT, et
al: New IL-17 family members promote Th1 or Th2 responses in the
lung: In vivo function of the novel cytokine IL-25. J Immunol.
169:443–453. 2002.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Saadoun D, Terrier B and Cacoub P:
Interleukin-25: Key regulator of inflammatory and autoimmune
diseases. Curr Pharm Des. 17:3781–3785. 2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Terrier B, Bièche I, Maisonobe T,
Laurendeau I, Rosenzwajg M, Kahn JE, Diemert MC, Musset L, Vidaud
M, Sène D, et al: Interleukin-25: A cytokine linking eosinophils
and adaptive immunity in churg-strauss syndrome. Blood.
116:4523–4531. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Fort MM, Cheung J, Yen D, Li J, Zurawski
SM, Lo S, Menon S, Clifford T, Hunte B, Lesley R, et al: IL-25
induces IL-4, IL-5, and IL-13 and Th2-associated pathologies in
vivo. Immunity. 15:985–995. 2001.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yin SY, Jian FY, Chen YH, Chien SC, Hsieh
MC, Hsiao PW, Lee WH, Kuo YH and Yang NS: Induction of IL-25
secretion from tumour-associated fibroblasts suppresses mammary
tumour metastasis. Nat Commun. 7(11311)2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Li J, Liao Y, Ding T, Wang B, Wang B, Yu
X, Chu Y, Xu J and Zheng L: Tumor-Infiltrating macrophages express
interleukin-25 and predict a favorable prognosis in patients with
gastric cancer after radical resection. Oncotarget. 7:11083–11093.
2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Uhlen M, Zhang C, Lee S, Sjöstedt E,
Fagerberg L, Bidkhori G, Benfeitas R, Arif M, Liu Z, Edfors F, et
al: A pathology atlas of the human cancer transcriptome. Science.
18(357)2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Tummanatsakun D, Proungvitaya T, Roytrakul
S, Limpaiboon T, Wongkham S, Wongkham C, Silsirivanit A, Somintara
O, Sangkhamanon S and Proungvitaya S: Serum apurinic/apyrimidinic
endodeoxyribonuclease 1 (APEX1) level as a potential biomarker of
cholangiocarcinoma. Biomolecules. 26(413)2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Dupont WD and Plummer WD Jr: Power and
sample size calculations: A review and computer program. Control
Clin Trials. 11:116–128. 1990.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Janan M, Proungvitaya S, Limpaiboon T,
Proungvitaya T, Roytrakul S, Wongkham C, Jearanaikoon P, Chur-in S
and Wongkham S: Serum adhesion molecule-1 (ICAM-1) as a potential
prognostic marker for cholangiocarcinoma patients. Asian Pac J
Cancer Prev. 13:107–114. 2012.PubMed/NCBI
|
|
18
|
Kim SW, Roh J and Park CS:
Immunohistochemistry for pathologists: Protocols, pitfalls, and
tips. J Pathol Transl Med. 50:411–418. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Pierceall WE, Wolfe M, Suschak J, Chang H,
Chen Y, Sprott KM, Kutok JL, Quan S, Weaver DT and Ward BE:
Strategies for H-score normalization of preanalytical technical
variables with potential utility to immunohistochemical-based
biomarker quantitation in therapeutic reponse diagnostics. Anal
Cell Pathol (Amst). 34:159–168. 2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Gillespie JW, Best CJ, Bichsel VE, Cole
KA, Greenhut SF, Hewitt SM, Ahram M, Gathright YB, Merino MJ,
Strausberg RL, et al: Evaluation of non-formalin tissue fixation
for molecular profiling studies. Am J Pathol. 160:449–457.
2002.PubMed/NCBI View Article : Google Scholar
|
|
21
|
De Petris L, Pernemalm M, Elmberger G,
Bergman P, Orre L, Lewensohn R and Lehtiö J: A novel method for
sample preparation of fresh lung cancer tissue for proteomics
analysis by tumor cell enrichment and removal of blood
contaminants. Proteome Sci. 8(9)2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ericsson C and Nistér M: Protein
extraction from solid tissue. Methods Mol Biol. 675:307–312.
2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lee JH, Hong CS, Lee S, Yang JE, Park Y
Il, Lee D, Hyeon T, Jung S and Paik SR: Radiating amyloid fibril
formation on the surface of lipid membranes through unit-assembly
of oligomeric species of α-synuclein. PLoS One.
7(e47580)2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Lowry OH, Rosebrough NJ, Farr AL and
Randall RJ: Protein measurement with the folin phenol reagent. J
Biol Chem. 193:265–275. 1951.PubMed/NCBI
|
|
25
|
Kuhn M, Szklarczyk D, Pletscher-Frankild
S, Blicher TH, Von Mering C, Jensen LJ and Bork P: STITCH 4:
Integration of protein-chemical interactions with user data.
Nucleic Acids Res. 42:D401–D107. 2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Szklarczyk D, Santos A, Von Mering C,
Jensen L and Bork P: STITCH 5: Augmenting protein-chemical
interaction networks with tissue and affinity data. Nucleic Acids
Res. 44:D380–D384. 2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Gregory LG, Jones CP, Walker SA, Sawant D,
Gowers KH, Campbell GA, Mckenzie AN and Lloyd CM and Lloyd CM:
IL-25 drives remodelling in allergic airways disease induced by
house dust mite. Thorax. 68:82–90. 2013.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Kaufhold S and Bonavida B: Central role of
snail1 in the regulation of EMT and resistance in cancer: A target
for therapeutic intervention. J Exp Clin Cancer Res.
33(62)2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Thelen TD, Green RM and Ziegler SF: Acute
blockade of IL-25 in a colitis associated colon cancer model leads
to increased tumor burden. Sci Rep. 6(25643)2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Jiang Z, Chen J, Du X, Cheng H, Wang X and
Dong C: IL-25 blockade inhibits metastasis in breast cancer.
Protein Cell. 8:191–201. 2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Ji Y and Zhang W: Th17 cells: Positive or
negative role in tumor. Cancer Immunol Immunother. 59:979–987.
2010.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Furuta S, Jeng YM, Zhou L, Huang L, Kuhn
I, Bissell MJ and Lee WH: IL-25 causes apoptosis of
IL-25R-expressing breast cancer cells without toxicity to
nonmalignant cells. Sci Transl Med. 13(78ra31)2011.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Benatar T, Cao MY, Lee Y, Lightfoot J,
Feng N, Gu X, Lee V, Jin H, Wang M, Wright JA and Young AH: IL-17E,
a proinflammatory cytokine, has antitumor efficacy against several
tumor types in vivo. Cancer Immunol Immunother. 59:805–817.
2010.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Mikami Y, Takada Y, Hagihara Y and Kanai
T: Innate lymphoid cells in organ fibrosis. Cytokine Growth Factor
Rev. 42:27–36. 2018.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Corrigan CJ, Wang W, Meng Q, Fang C, Wu H,
Reay V, Lv Z, Fan Y, An Y, Wang YH, et al: T-Helper cell type 2
(Th2) memory T cell-potentiating cytokine IL-25 has the potential
to promote angiogenesis in asthma. Proc Natl Acad Sci USA.
108:1579–1584. 2011.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Wu F, Xu J, Huang Q, Han J, Duan L, Fan J,
Lv Z, Guo M, Hu G, Chen L, et al: The role of interleukin-17 in
lung cancer. Mediators Inflamm. 2016(8494079)2016.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lee J, Ho WH, Maruoka M, Corpuz RT,
Baldwin DT, Foster JS, Goddard AD, Yansura DG, Vandlen RL, Wood WI
and Gurney AL: IL-17E, a novel proinflammatory ligand for the IL-17
receptor homolog IL-17Rh1. J Biol Chem. 276:1660–1664.
2001.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Huber MA, Azoitei N, Baumann B, Grünert S,
Sommer A, Pehamberger H, Kraut N, Beug H and Wirth T: NF-κB is
essential for epithelial mesenchymal transition and metastasis in a
model of breast cancer progression. J Clin Invest. 114,
2004:569–581. 2004.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Jayachandran A, Königshoff M, Yu H,
Rupniewska E, Hecker M, Klepetko W, Seeger W and Eickelberg O: SNAI
transcription factors mediate epithelial-mesenchymal transition in
lung fibrosis. Thorax. 64:1053–1061. 2009.PubMed/NCBI View Article : Google Scholar
|