Introduction
RalA is a member of the Ras superfamily of small
GTPases (1). The Ras-like GTPases
are tumor antigens that are aberrantly induced during tumorigenesis
by oncogenic Ras (2). Human cancers
often contain RAS mutations (3),
and 37.9-49.6% of colorectal cancers contain RAS mutations
(4). RalA protein has been studied
in various cancers (5), including
colorectal cancer (6). RalA protein
have been reported as key cancer phenotypic markers and biomarkers
of cellular migration, invasion and metastasis (7,8).
We previously reported that serum IgG autoantibodies
were useful for detecting early-stage colorectal cancer (9), monitoring treatment response, and
monitoring after surgery (10-12).
Serum RalA antibodies (s-RalA-Abs) have been reported to be a
potential biomarker for various cancers (9,13-15).
However, previous reports rather than our own reports (16,17),
did not reveal details of the clinicopathological and prognostic
significance. Furthermore, the relationship between the
conventional serum markers, CEA and CA19-9, has not been
analyzed.
Therefore, we evaluated the clinicopathological and
prognostic significance of s-RalA-Abs status in colorectal cancer
patients. Moreover, the use of combinatorial assays of s-RalA-Abs
with CEA and/or CA19-9 was evaluated for their clinical impact.
Materials and methods
Patients
A total of 314 patients with colorectal cancer,
including 165 patients from Toho University Omori Medical Center
and 149 patients from Chiba Cancer Center, were analyzed to detect
serum antibodies against RalA. Samples from 73 healthy controls
were also obtained. Among the 314 patients, 194 were men (61.8%)
and 120 were women (38.2%), with a median age of 66 (range, 27-90)
years. The TNM stage of colorectal cancer was classified according
to the General Rules for the Clinical and Pathological Study of
Primary Colorectal Cancer (7th Edition) (18). All patients were classified as stage
0 (n=10), stage I (n=61), stage II (n=86), stage III (n=78), stage
IV (n=64), or recurrence (n=15). Serum RalA antibodies
(s-RalA-Abs), carcinoembryonic antigen (CEA), and carbohydrate
antigen 19-9 (CA19-9) were evaluated to compare clinicopathological
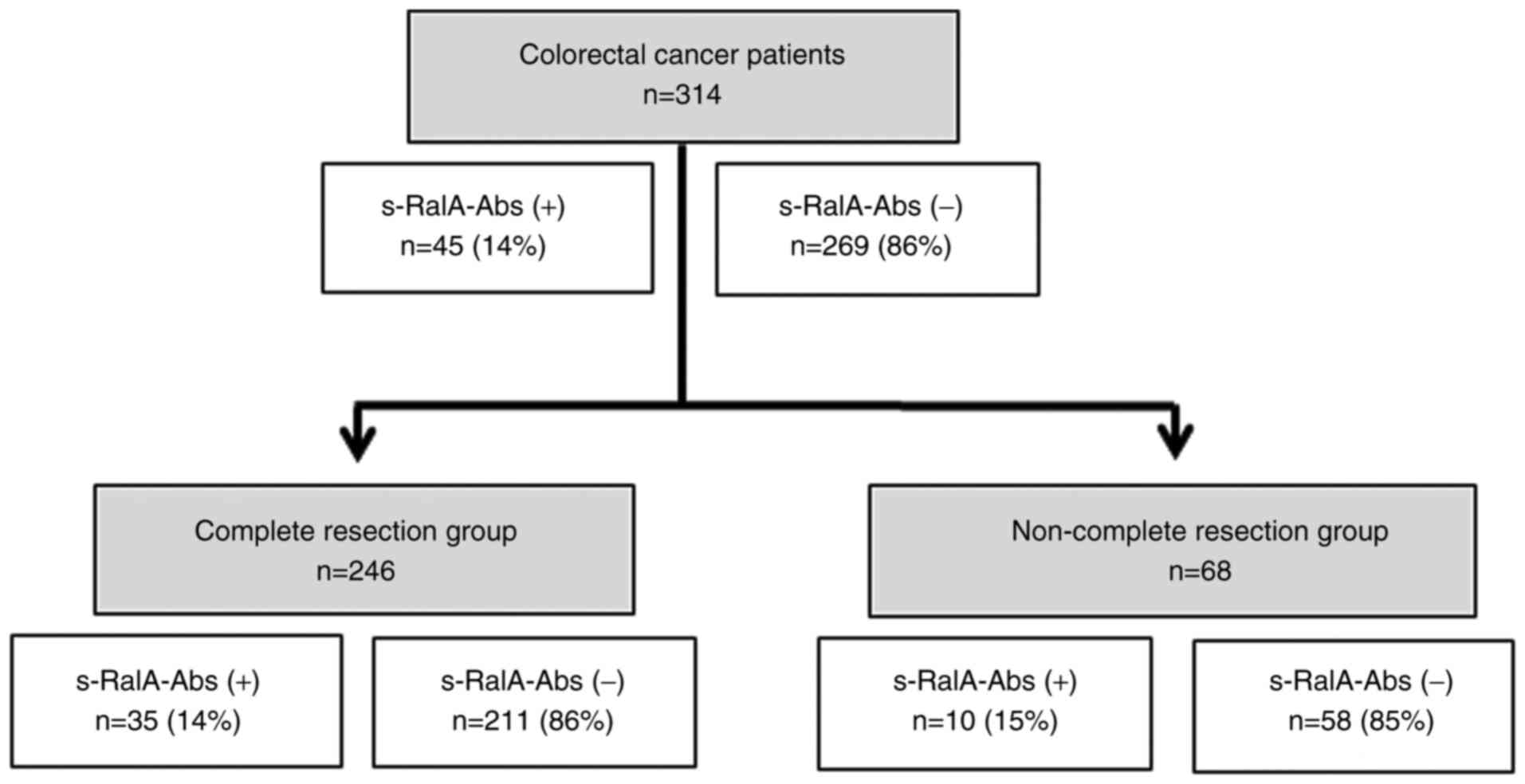
significance. A flowchart showing the patient subgroups and
s-RalA-Abs status is shown in Fig.
1. Written informed consent to publish any associated data was
provided and obtained from all study participants.
Analysis of s-RalA-Abs, CEA, and
CA19-9
Serum samples were analyzed by enzyme-linked
immunosorbent assay (ELISA) as previously described (19) using 96-well microtiter plates coated
with purified recombinant RalA protein. Absorbance was measured at
450 nm using a SUNRISE Microplate Reader (Tecan Japan Co., Ltd.)
(20). An optimized antibody titer
cutoff value and a standard cutoff value corresponding to a value
greater than that of the mean of the healthy control cohort plus
three standard deviations were applied to RalA antibodies, and
specificity was maintained at over 95% (21). The optical density cutoff value was
fixed at 0.324. Details of the three standard deviations of
autoantibody titers were described previously (22). The assay specificity was calculated
as the percentage of the healthy controls showing a negative
result. CEA and CA19-9 were measured as previously described
(14).
Statistical analysis
Fisher's exact test was used to analyze the
categorical variables. The age of the continuous variable in
Table I was divided into two
groups: Over or under 65 years old. Older age was analyzed using
Fisher's exact as a single category. In figures, Fisher's exact was
used to analyze the noteworthy positive rate between the two groups
for comparison. Clinicopathological parameters associated with
survival were evaluated by univariate analysis using log-rank test
based on the Kaplan-Meier survival curves. Multivariate analyses
were performed using the Cox proportional hazards model. All
statistical analyses were performed using EZR statistical software
(23). P-values <0.05 were
considered statistically significant.
 | Table IComparison of clinicopathological
features among 314 patients with colorectal cancer according to
s-RalA-Abs status. |
Table I
Comparison of clinicopathological
features among 314 patients with colorectal cancer according to
s-RalA-Abs status.
| Variable | Total number
(n=314) | s-RalA-Abs positive
(n=45) | s-RalA-Abs negative
(n=269) | P-valuee |
|---|
| Age (years) | | | | 0.75 |
|
≥65 | 172 | 26 | 146 | |
|
<65 | 142 | 19 | 123 | |
| Sex | | | | 0.51 |
|
Male | 194 | 30 | 164 | |
|
Female | 120 | 15 | 105 | |
| Locationa | | | | 0.73 |
|
Rectum | 107 | 16 | 91 | |
|
Colon | 192 | 25 | 167 | |
| Tumor
depthb | | | | 0.64 |
|
T4 | 46 | 7 | 39 | |
|
T1,T2,T3 | 234 | 30 | 204 | |
| Lymph node
metastasisc | | | | 0.59 |
|
Positive | 116 | 17 | 99 | |
|
Negative | 166 | 20 | 146 | |
| Stage | | | | 0.29 |
|
0/I | 71 | 6 | 65 | |
|
II | 86 | 14 | 72 | |
|
III | 78 | 13 | 65 | |
|
IV | 64 | 8 | 56 | |
|
Recurrence | 15 | 4 | 11 | |
| Complete
resection | | | | |
|
No | 68 | 10 | 58 | 1.00 |
|
Yes | 246 | 35 | 211 | |
|
Histologyd | | | | |
|
Muc,
Por | 18 | 0 | 18 | 0.087 |
|
Tub1,
Tub2 | 285 | 43 | 242 | |
| Adjuvant
chemotherapy | | | | |
|
No | 79 | 10 | 69 | 0.22 |
|
Yes | 85 | 17 | 68 | |
| CEA (cut off, 5.0
ng/ml) | | | | |
|
Positive | 129 | 21 | 108 | 0.42 |
|
Negative | 185 | 24 | 161 | |
| CA19-9 (cut off,
37.0 U/ml) | | | | |
|
Positive | 59 | 7 | 52 | 0.69 |
|
Negative | 255 | 38 | 217 | |
Results
Comparison of clinicopathological
features in colorectal cancer patients according to s-RalA-Abs
status
Among 314 patients with colorectal cancer, 45 (14%)
were positive for s-RalA-Abs (Fig.
1). The positive rate of s-RalA-Abs in 246 patients in the
complete resection (R0) group was 14%. The presence of s-RalA-Abs
was slightly associated with differentiated type (P=0.087). No
other clinicopathological factors were significantly associated
with s-RalA-Abs (Table I).
Furthermore, the presence of s-RalA-Abs was not significantly
associated with CEA and CA19-9.
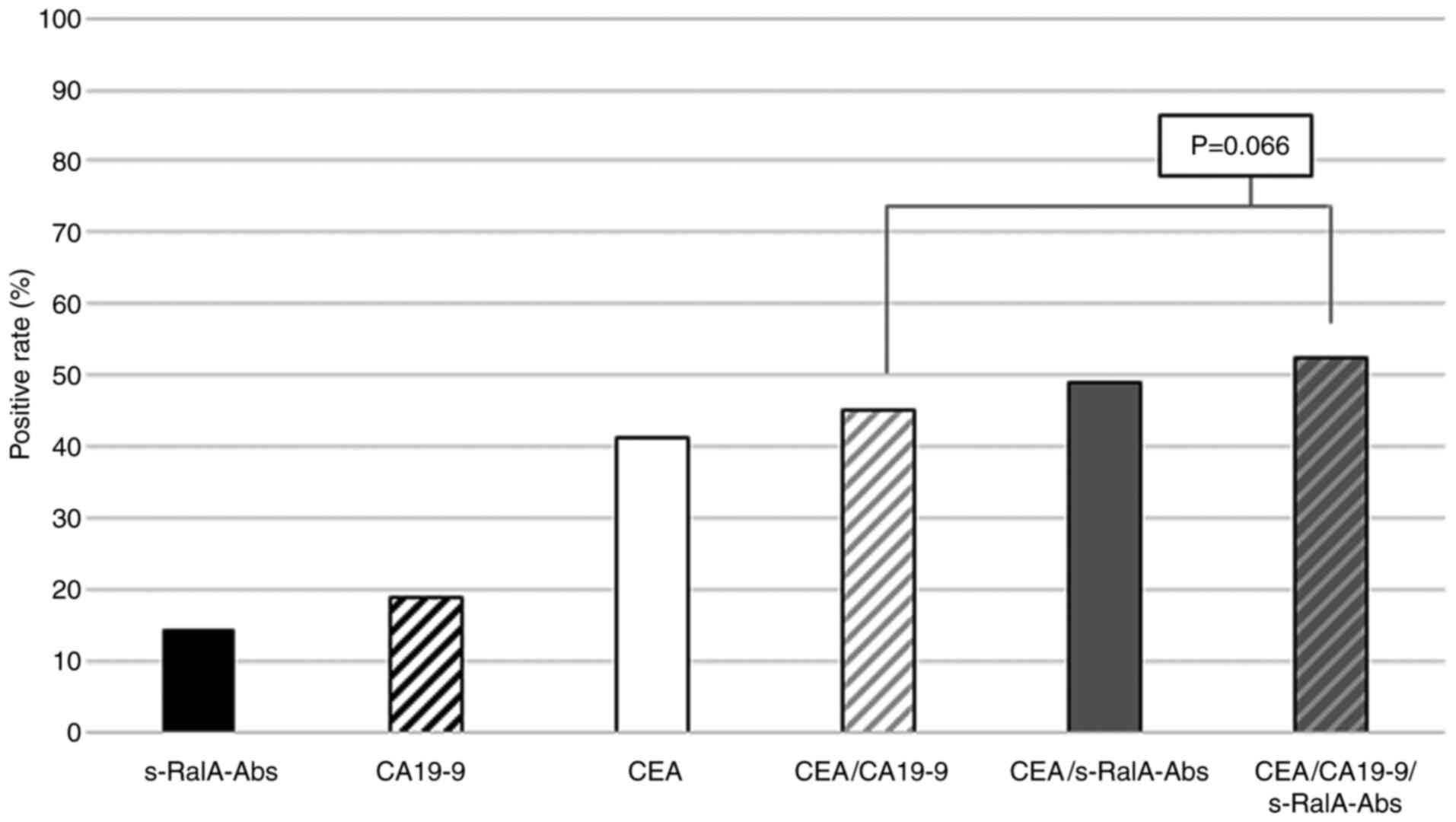
Positive rates of combined s-RalA-Abs,
CEA and CA19-9
The positive rates of s-RalA-Abs, CA19-9 and CEA in
all 314 patients were 14, 19 and 41%, respectively (Fig. 2). The positive rate of combined
CEA/s-RalA-Abs was higher than that of combined CEA/CA19-9.
Furthermore, the positive rate of combined CEA/CA19-9/s-RalA-Abs
was higher than that of combined CEA/CA19-9 (53 vs. 45%, P=0.066)
(Fig. 2).
Positive rates of serum markers in
colorectal cancer patients according to stage
There was no significant difference in the positive
rates of s-RalA-Abs among the stage 0/I-IV, and recurrence groups
(8, 16, 17, 13 and 27%, respectively). The positive rates of
combined CEA/s-RalA-Abs were higher than that of combined
CEA/CA19-9 in stage 0/I, II and III, although the differences were
not statistically significant (Fig.
3).
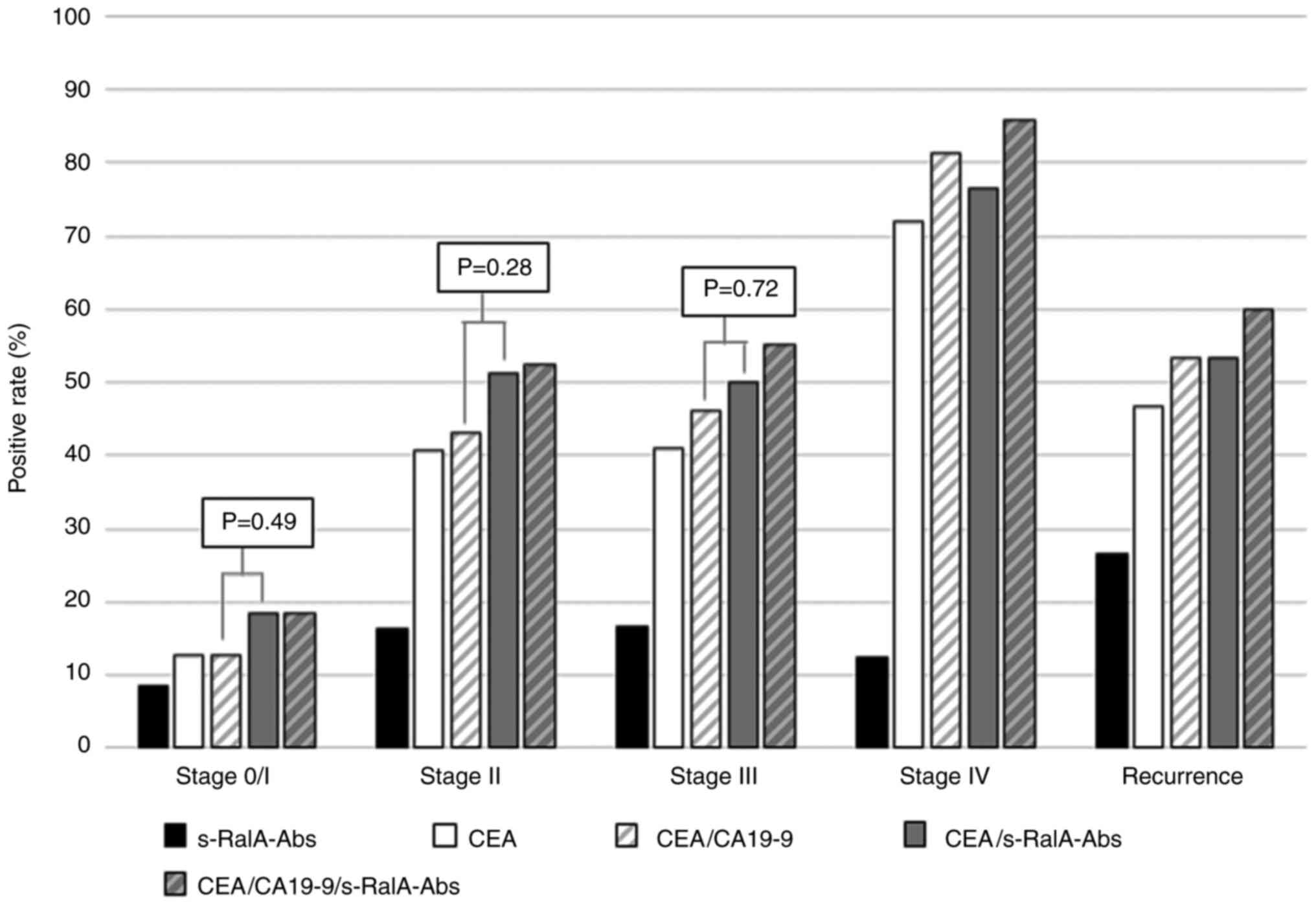 | Figure 3Positive rates for serum markers in
patients with colorectal cancer according to stage. In patients at
stage 0/I, the positive rates of s-RalA-Abs, CEA, CEA/CA19-9,
CEA/s-RalA-Abs and CEA/CA19-9/s-RalA-Abs were 8, 13, 13, 18 and
18%, respectively. At stage 0/I, II, and III, the positive rates of
combined CEA/s-RalA-Abs were higher than that of combined
CEA/CA19-9, although the differences were not statistically
significant. s-RalA-Abs, serum RalA antibodies; CEA,
carcinoembryonic antigen; CA19-9, carbohydrate antigen 19-9. |
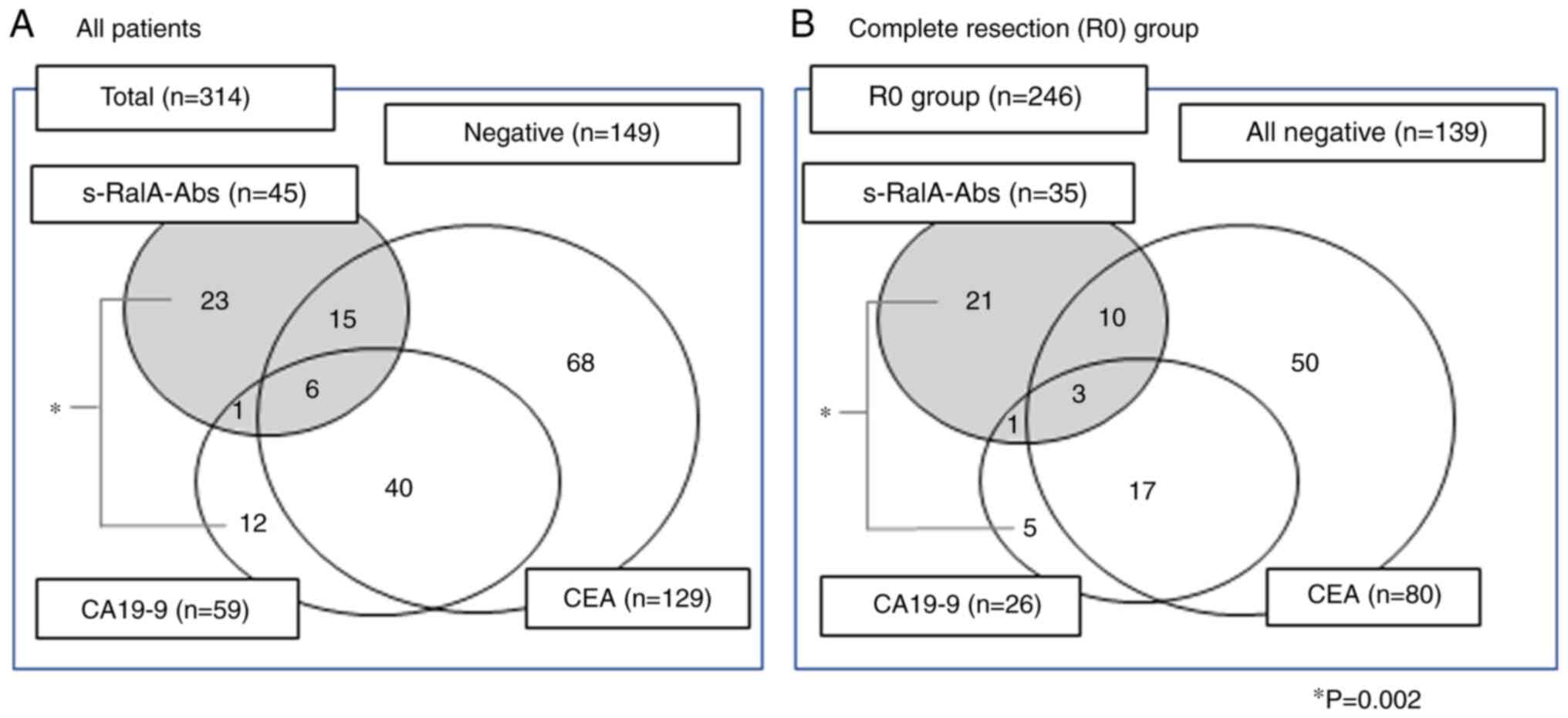
Correlation between s-RalA-Abs, CEA,
and CA19-9
Positive tumor markers were found in 165 out of 314
(52.5%) patients in total (Fig.
4A). Among s-RalA-Abs-positive patients, 23 out of 45 (51%)
were positive for s-RalA-Abs only. On the other hand, among
CA19-9-positive patients, 12 out of 59 (20%) were positive for
CA19-9 only. This tendency was also found in the complete resection
group (Fig. 4B). Among
s-RalA-Abs-positive patients, 21 out of 35 (60%) were positive for
s-RalA-Abs only. On the other hand, among CA19-9-positive patients,
5 out of 26 (19%) were positive for CA19-9 only. The s-RalA-Abs
single positive rate was significantly higher than that for CA19-9
(P=0.002).
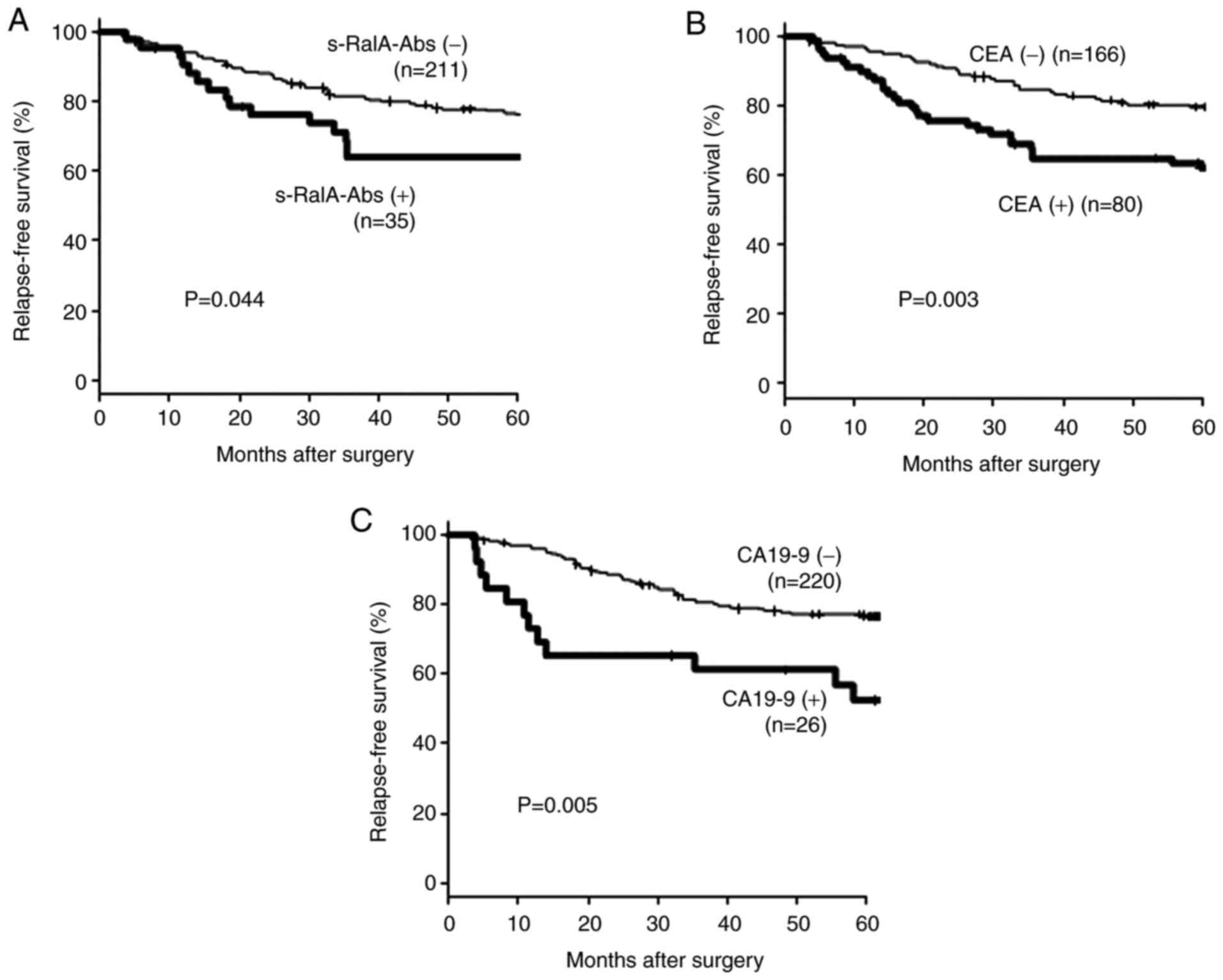
Relapse-free survival in patients in
the completed resection group
Fig. 5 shows the
relapse-free survival of 246 patients with complete resection
according to the preoperative serum marker status. Patients with a
positive preoperative status for tumor markers were significantly
associated with poor prognosis.
Relapse-free survival according to
tumor marker combination status for patients in the complete
resection group
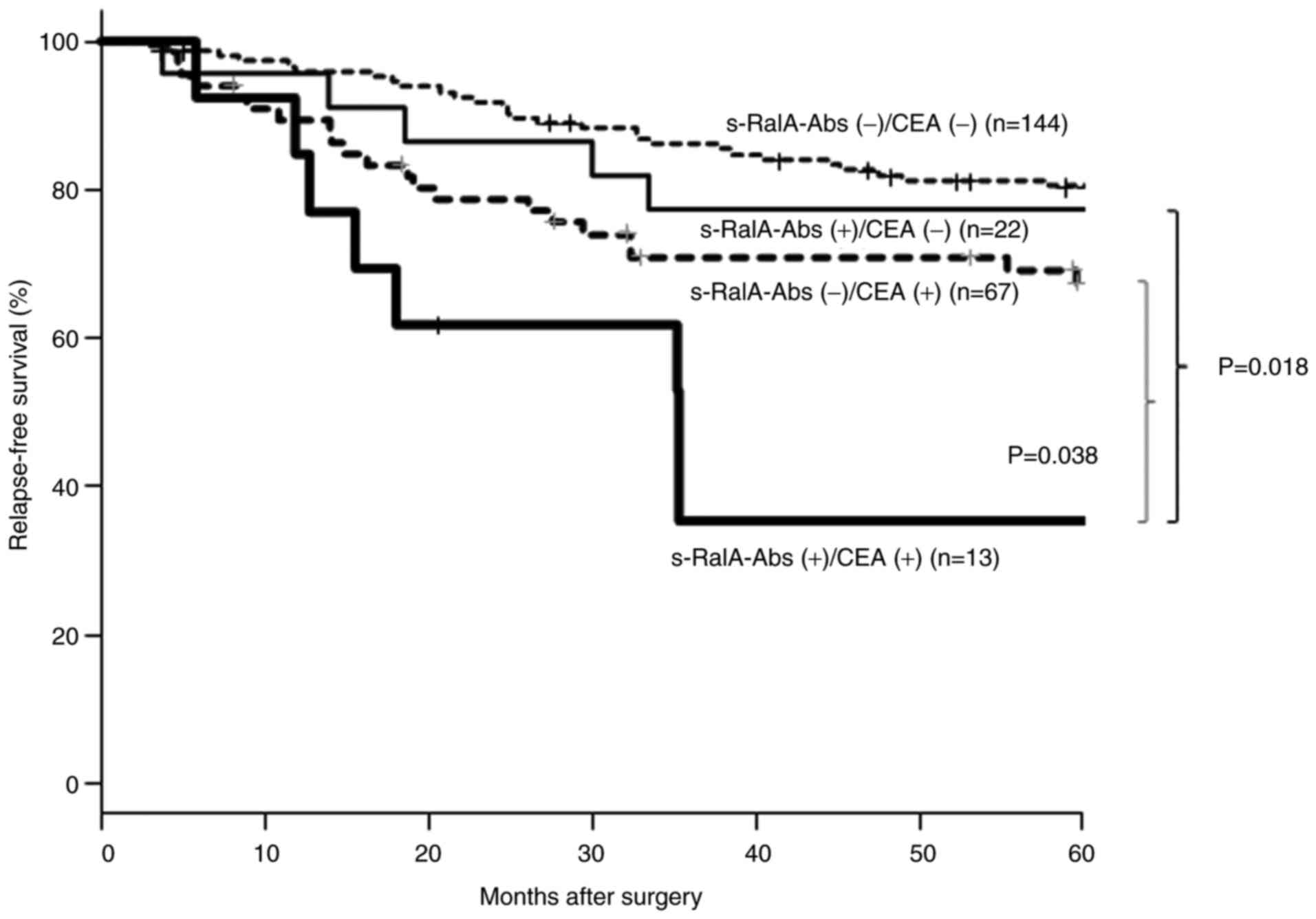
Fig. 6 shows a
comparison of relapse-free survival according to tumor marker
combination status. Among CEA(-) patients, the s-RalA-Abs(+) group
showed worse relapse-free survival than the s-RalA-Abs(-) group;
however, the difference was not statistically significant. On the
other hand, in the CEA (+) groups, the s-RalA-Abs(+) group showed
significantly worse relapse-free survival than that of the
RalA-Abs(-) group (P=0.038). The double-positive
s-RalA-Abs(+)/CEA(+) group showed the worst relapse-free
survival.
Univariate and multivariate analyses
of risk factors for relapse-free survival in the complete resection
group
Table II shows the
association of risk factors with relapse-free survival. Univariate
and multivariate analyses revealed that T4, lymph node metastasis,
and CEA(+)/s-RalA-Abs(+) double-positivity were significant poor
risk factors for reduced relapse-free survival.
| Table IIAnalysis of the risk factors
associated with relapse-free survival in patients with colorectal
cancer patients with complete resection (n=246). |
Table II
Analysis of the risk factors
associated with relapse-free survival in patients with colorectal
cancer patients with complete resection (n=246).
| | Univariate | Multivariate |
|---|
| Variable | Total number |
P-valuee | Hazard ratio | 95% CI |
P-valuef |
|---|
| Age (years) | | 0.51 | | | |
|
≥65 | 109 | | | | |
|
<65 | 137 | | | | |
| Sex | | 0.11 | 1.65 | 0.97-2.80 | 0.063 |
|
Male | 148 | | | | |
|
Female | 98 | | | | |
|
Locationa | | 0.48 | | | |
|
Rectum | 83 | | | | |
|
Colon | 156 | | | | |
| Tumor
depthb | | <0.001 | 2.29 | 1.18-4.45 | 0.015 |
|
T4 | 22 | | | | |
|
T1,T2,T3 | 217 | | | | |
| Lymph node
metastasisc | | <0.001 | 2.84 | 1.71-4.71 | <0.001 |
|
Positive | 83 | | | | |
|
Negative | 156 | | | | |
|
Histrogyd | | 0.24 | | | |
|
Muc,
Por | 12 | | | | |
|
Tub1,
Tub2 | 232 | | | | |
| s-RalA-Abs (+)/CEA
(+) | | <0.001 | 2.35 | 1.06-5.20 | 0.035 |
|
Yes | 13 | | | | |
|
No | 233 | | | | |
|
CEA(+)/CA19-9(+) | | 0.071 | 1.75 | 0.74-4.13 | 0.20 |
|
Yes | 17 | | | | |
|
No | 229 | | | | |
Discussion
The overall s-RalA-Abs positive rate was 14% in
colorectal cancer patients. However, s-RalA-Abs status was not
associated with any clinicopathological factors and was not
associated with CEA and CA19-9 status. Combined CEA/s-RalA-Abs and
CEA/CA19-9/s-RalA-Abs showed higher positive rates than CEA/CA19-9;
however, this difference did not reach statistical significance.
The s-RalA-Abs(+) group showed poor relapse-free survival,
particularly in the CEA(+) group.
The s-RalA-Abs positive rate was not high using a
single biomarker. Since s-RalA-Abs was independent of CEA or
CA19-9, it could be useful to apply this in combination with CEA.
Although the s-RalA-Abs positive rates in patients with esophageal
cancer gradually increased in association with tumor stages
(13), we were unable to confirm a
similar tendency in colorectal cancer patients. In the present
study, the s-RalA-Abs positive rate of stage 0/I/II was similar to
that of stage III/IV.
Although s-RalA-Abs was not associated with tumor
stage, the s-RalA-Abs(+) group showed a significantly poor
relapse-free survival. The malignant potential of RalA(+) cancer
cells was partly explained by the biological effects of the RalA
molecule on cancer progression and/or metastases (24,25).
Interestingly, these effects of s-RalA-Abs seemed to be limited in
the CEA(+) group. However, the potential mechanisms for the
biological effects of RalA/s-RalA-Abs remain unclear.
The present study has two major limitations. First,
s-RalA-Abs titers were not monitored after surgery. Previous
studies based on s-p53-Abs monitoring after surgery showed that the
presence of s-p53-Abs, even after surgery, indicated residual
cancer cells (26). Therefore,
further assessment should be performed in future. Second, there was
a lack of data for RalA immunoreactivity of the tumor cells. Since
RalA is a tumor antigen that induces serum antibodies, there may
have been tumor cell overexpression of RalA protein in the sera of
the s-RalA-Abs(+) group. Such a positive association has been
confirmed in patients with esophageal cancer (13).
In conclusion, although the positive rate was not
high, s-RalA-Abs may be a candidate biomarker to detect colorectal
cancer and may also be a useful predictor of poor relapse-free
survival in colorectal cancer patients after curative
resection.
Acknowledgements
The authors would like to thank Ms. Seiko Otsuka
(Toho University) for her support with sampling and data
presentation for the current study.
Funding
The present study was supported by a research grant
from JSPS KAKENHI (grant no. JP26462029).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
MU, HSh and YN conceived and designed the current
study. MU, HSo, NT, TK and KF acquired patient samples. MU, HSo,
NT, TK and KF contributed to the acquisition of the patient's
clinicopathological data. AK supported the development of the ELISA
system used to measure antibody titers. MU, FS, IH and HSh analyzed
patient data. MU and HSh drafted the manuscript. All authors read
and approved the final manuscript.
Ethics approval and patient consent to
participate
The present study was performed in adherence to the
international and national regulations in accordance with the
Declaration of Helsinki. Informed consent was obtained from all
participants for sampling, analyses and publication. The current
study was approved by the Ethics Committee of Toho University Omori
Medical Center (approval nos. 26-255 and M19213) and the Chiba
Cancer Center (approval no. 30-220).
Patient consent for publication
Written informed consent to publish any associated
data was provided and obtained from all study participants.
Competing interests
HSh received a research grant from Medical &
Biological Laboratories Co., Ltd. AK is an employee of Medical
& Biological Laboratories Co., Ltd.. All other authors declare
that there they have no competing interests.
References
|
1
|
Shirakawa R and Horiuchi H: Ral GTPases:
Crucial mediators of exocytosis and tumorigenesis. J Biochem.
157:285–299. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Moghadam AR, Patrad E, Tafsiri E, Peng W,
Fangman B, Pluard TJ, Accurso A, Salacz M, Shah K, Ricke B, et al:
Ral signaling pathway in health and cancer. Cancer Med.
6:2998–3013. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Schubbert S, Shannon K and Bollag G:
Hyperactive ras in developmental disorders and cancer. Nat Rev
Cancer. 7:295–308. 2007.PubMed/NCBI View
Article : Google Scholar
|
|
4
|
Guo TA, Wu YC, Tan C, Jin YT, Sheng WQ,
Cai SJ, Liu FQ and Xu Y: Clinicopathologic features and prognostic
value of KRAS, NRAS and BRAF mutations and DNA mismatch repair
status: A single-center retrospective study of 1,834 Chinese
patients with stage I-IV colorectal cancer. Int J Cancer.
15:1625–1634. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yan C and Theodorescu D: RAL GTPases:
Biology and potential as therapeutic targets in cancer. Pharmacol
Rev. 70:1–11. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Martin TD, Samuel JC, Routh ED, Der CJ and
Yeh JJ: Activation and involvement of ral GTPases in colorectal
cancer. Cancer Res. 71:206–215. 2011.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Oxford G, Owens CR, Titus BJ, Foreman TL,
Herlevsen MC, Smith SC and Theodorescu D: RalA and RalB:
Antagonistic relatives in cancer cell migration. Cancer Res.
65:7111–7120. 2005.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Smith SC, Baras AS, Owens CR, Dancik G and
Theodorescu D: Transcriptional signatures of ral GTPase are
associated with aggressive clinicopathologic characteristics in
human cancer. Cancer Res. 72:3480–3491. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ushigome M, Nabeya Y, Soda H, Takiguchi N,
Kuwajima A, Tagawa M, Matsushita K, Koike J, Funahashi K and
Shimada H: Multi-panel assay of serum autoantibodies in colorectal
cancer. Int J Clin Oncol. 23:917–923. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Takeda A, Shimada H, Nakajima K, Imaseki
H, Suzuki T, Asano T, Ochiai T and Isono K: Monitoring of p53
autoantibodies after resection of colorectal cancer: Relationship
to operative curability. Eur J Surg. 167:50–53. 2001.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Suzuki T, Shimada H, Ushigome M, Koike J,
Funahashi K, Nemoto T and Kaneko H: Three-year monitoring of serum
p53 antibody during chemotherapy and surgery for stage IV rectal
cancer. Clin J Gastroenterol. 9:55–58. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ushigome M, Shimada H, Miura Y, Yoshida K,
Kaneko T, Koda T, Nagashima Y, Suzuki T, Kagami S and Funahashi K:
Changing pattern of tumor markers in recurrent colorectal cancer
patients before surgery to recurrence: Serum p53 antibodies, CA19-9
and CEA. Int J Clin Oncol. 25:622–632. 2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Nanami T, Shimada H, Yajima S, Oshima Y,
Matsushita K, Nomura F, Nagata M, Tagawa M, Otsuka S, Kuwajima A
and Kaneko H: Clinical significance of serum autoantibodies against
ras-like GTPases, RalA, in patients with esophageal squamous cell
carcinoma. Esophagus. 13:167–172. 2016.
|
|
14
|
Wang P, Qin J, Ye H, Li L, Wang X and
Zhang J: Using a panel of multiple tumor-associated antigens to
enhance the autoantibody detection in the immunodiagnosis of
ovarian cancer. J Cell Biochem. 120:3091–3100. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kubota Y, Ogata H, Otsuka S, Kuwajima A,
Saito F and Shimada H: Presence of autoantibodies against ras-like
GTPases in serum in stage I/II breast cancer. Toho J Med.
3:125–130. 2017.
|
|
16
|
Okada R, Otsuka Y, Wakabayashi T, Shinoda
M, Aoki T, Murakami M, Arizumi S, Yamamoto M, Aramaki O, Takayama
T, et al: Six autoantibodies as potential serum biomarkers of
hepatocellular carcinoma: A prospective multicenter study. Int J
Cancer. 23(1002)2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Nanami T, Hoshino I, Ito M, Yajima S,
Oshima Y, Suzuki T, Shiratori F, Nabeya Y, Funahashi K and Shimada
H: Prevalence of autoantibodies against ras-like GTPases, RalA, in
patients with gastric cancer. Mol Clin Oncol. 13(28)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A (eds): AJCC Cancer Staging Manual, 7th
edition. Springer, New York, NY, 2010.
|
|
19
|
Li Y, Karjalainen A, Koskinen H, Hemminki
K, Vainio H, Shnaidman M, Ying Z, Pukkala E and Brandt-Rauf PW: P53
autoantibodies predict subsequent development of cancer. Int J
Cancer. 114:157–160. 2005.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hoshino I, Nagata M, Takiguchi N, Nabeya
Y, Ikeda A, Yokoi S, Kuwajima A, Tagawa M, Matsushita K, Satoshi Y
and Hideaki S: Panel of autoantibodies against multiple
tumor-associated antigens for detecting gastric cancer. Cancer Sci.
108:308–315. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Zhang JY, Casiano CA, Peng XX, Koziol JA,
Chan EL and Tan EM: Enhancement of antibody detection in cancer
using panel of recombinant tumor-associated antigens. Cancer
Epidemiol Biomarkers Prev. 12:136–143. 2003.PubMed/NCBI
|
|
22
|
Okada R, Shimada H, Tagawa M, Matsushita
K, Otsuka Y, Kuwajima A and Kaneko H: Profiling of serum
autoantibodies in Japanese patients with hepatocellular carcinoma.
Toho J Med. 3:84–92. 2017.
|
|
23
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tchevkina E, Agapova L, Dyakova N,
Martinjuk A, Komelkov A and Tatosyan A: The small G-protein RalA
stimulates metastasis of transformed cells. Oncogene. 24:329–335.
2005.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Yan C, Liu D, Li L, Wempe MF, Guin S,
Khanna M, Meier J, Hoffman B, Owens C, Wysoczynski CL, et al:
Discovery and characterization of small molecules that target the
GTPase ral. Nature. 515:443–447. 2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Shimada H, Okazumi S, Matsubara H,
Shiratori T, Akutsu Y, Nabeya Y, Tanizawa T, Matsushita K, Hayashi
H, Isono K and Ochiai T: Long-term results after dissection of
positive thoracic lymph nodes in patients with esophageal squamous
cell carcinoma. World J Surg. 32:255–261. 2008.PubMed/NCBI View Article : Google Scholar
|