Introduction
Clear-cell carcinoma (CCC) is responsible for ≤5% of
all uterine carcinomas (1), and 1/3
CCC cases are diagnosed when distant metastases are present.
However, options for systemic therapy remain limited, and it has
been reported that CCC has a low response rate to chemotherapy
(2). Moreover, clinical
recommendations do not offer distinct treatment plans for rare
uterine histologies, including CCC, and their molecular mechanisms
are different from endometroid cancer types.
CCC has one of the lowest expression levels of
estrogen receptors (ER) and progesterone receptors (PR) among the
uterine cancer types (1). Hormonal
treatment usage is limited to endometrioid histologies, and has not
been studied or used for other types (3).
It has been revealed that 3-40% of all the uterine
cancer types express human epidermal growth factor receptor 2
(HER2) (4,5). Furthermore, upregulation of HER2 in
uterine carcinomas is associated with poor characteristics of the
tumor, such as serous or clear cell histology and high grade, as
well as unfavorable prognosis. HER2 is upregulated in a 1/2 of all
serous tumors and 1/3 of CCC (5).
Trastuzumab has demonstrated efficacy in patients with serous
histology, with progression-free survival being significantly
improved in experimental groups (6). However, to the best of our knowledge,
there are no reports on anti-HER2 treatment in patients with
CCC.
Case report
A female patient (born 1954) was examined in January
2016 due to dysuria. Ultrasound results identified multiple
enlarged paraaortic lymph nodes, which compressed both ureters.
Ureteral stents were installed. Concurrently, multiple bone lesions
were detected. The female patient was admitted in N.N. Blokhin
National Medical Research Center of Oncology 1 month later, in
February 2016, with severe back pain. 18F-FDG-PET/CT was
performed, which detected bone metastases, metastatic lesions in
paraaortic lymph nodes and metastatic node on the uterus stump (the
partial amputation of the uterus was performed in 1995 most likely
due to leyomyoma).
Biopsy from left iliac bone revealed adenocarcinoma.
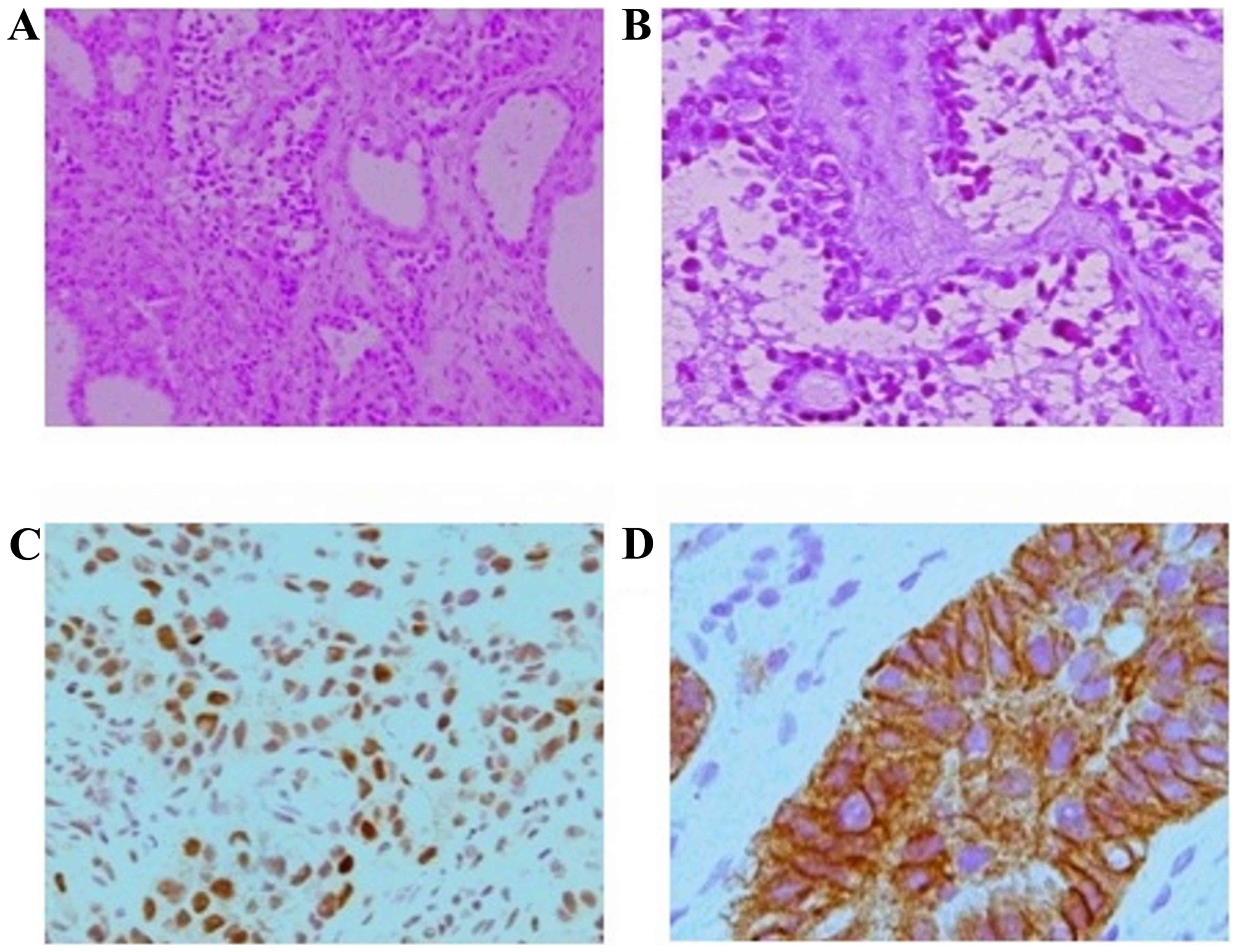
Morphological examination from the metastatic site in the bone
identified bone marrow tissue with three hematopoietic cell lines
and a tumor, which had the appearance of adenocarcinoma, containing
various patterns and cell types (Fig.
1A). A total of three major types of structures were observed:
Tubule-cystic, papillary and solid, which were disorderly and
intermixed on the fibrocollagenous, partly hyalinized, background.
The tumor cells in the solid structures were large with an
eosinophilic granular or clear vacuolated cytoplasm, voluminous
nuclei and occasional eosinophilic nucleoli. The lining of the
tubule-cystic structures displayed a continuum of cells from
flattened to cuboid, or highly prismatic cells. The large bulbous
nuclei often protruded into lumen, acquiring the appearance of
hobnail cells. The cellular covering of papillae with different
complexity was analogous to that of cystic linings. The cystic
cavities contained colloid type material and the cells with
eosinophilic hyaline bodies (Fig.
1B). The PAS reaction was positive in the cell cytoplasm. The
IHC results, using Springer antibodies, ER (SP1, Spring Bioscience
1:100), PR (SP2, Spring Bioscience 1:400), Her2 neu (SP3, Spring
Bioscience 1:400), demonstrated that the tumor cells were positive
for ER (Fig. 1C), Her2/neu (3+)
(Fig. 1D), CK7, Pax8 and napsin.
The diagnosis of clear cell carcinoma was considered.
Based on the pathology findings, the presence of the
node on uterus stump and the absence of other suspected primary
tumors, the patient was diagnosed with metastatic CCC of the
uterus.
Treatment started with radiotherapy: The first part
of irradiation covered the soft-tissue mass at the Th7-12 spinal
cord level (30 Gy in 10 fractions) and the second covered lesions
in pelvis (30 Gy in 10 fractions). Radiotherapy resulted in a
substantial decrease in pain. Due to requirement for systemic
low-toxic treatment during radiotherapy and based on the pathology
examination results, systemic therapy with aromatase inhibitors
(letrozole in standard dose) and zoledronic acid was initiated in
March 2016. The patient remained stable without chemotherapy, and
thus in June 2016 hormonal therapy was continued and
Herticad®, a Russian biosimilar of trastuzumab, was
added (Biocad, loading dose 8 mg/kg, followed by 6 mg/kg every 3
weeks). This approach resulted in clinical improvement and a
partial radiological response with a significant decrease in
metastatic lesions, both in size and FDG-uptake.
A total of 27 months after initiation of the
treatment, the patient began to complain of dizziness. Therefore, a
brain MRI was performed, which revealed one lesion in cerebellum.
PET/CT results did not demonstrated any sign of progression with
respect to extracranial lesions. In July 2018 the lesion was
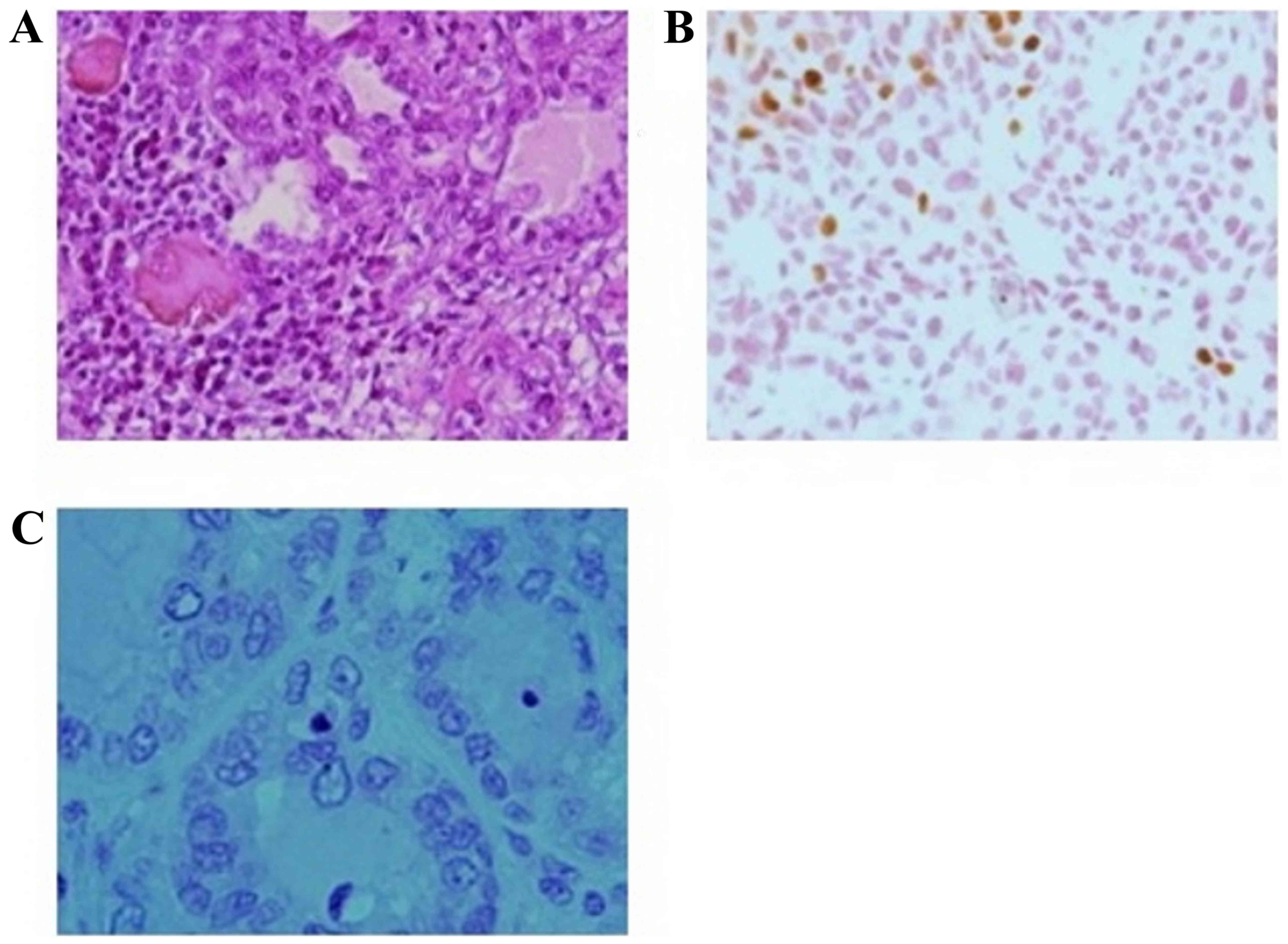
surgically removed. The structure of brain metastasis (Fig. 2A) was principally identical to that
of bone metastasis obtained previously during biopsy. The brain
lesion differed in terms of high cellular density, elevated
polymorphism and marked dystrophy in both the cytoplasm and nuclei.
The clear cell component was obvious, together with extensive
necrosis, hemorrhages and marked lymphoplasmocytic infiltration,
which was not necessarily confined to necrotic foci. The
significant finding was the negative HER2 reaction (Fig. 2C) in the cancer cells in metastatic
foci, as well as the notable reduction of reactivity to ERs both in
number of positively stained cells and the intensity of the
staining itself (Fig. 2B).
Due to the long-lasting clinical and radiological
benefit and surgical removal of HER2 non-expressing tissue, it was
decided to continue with anti-HER2 and endocrine therapy. Then,
trastuzumab was switched to lapatinib, based on its ability to
cross the blood-brain barrier. The patient started the new
combination (letrozole + lapatinib in standard dose) in June 2018
and remains stable until December 2019, with the only sign of
disease being in one paraaortic lymph node. Figs.
3-5 present the radiological response to treatment.
Discussion
CCC is a rare type of uterine carcinoma associated
with an unfavorable prognosis. Current treatment options for this
tumor type do not differ from endometroid tumors, and only include
chemotherapy. However, an individual approach for every patient
remains a milestone of cancer treatment. In the metastatic setting,
the aim of treatment is to increase the survival of the patient, as
well as improve the quality of life. Thus, the present study aimed
to use hormonal and targeted agents whenever possible.
In the present clinical case pathologic report
investigated not only the histological subtype and grade, but also
multiple characteristics that had a significant influence on the
treatment decision. Both the morphological findings and the
observed benefit allowed the ability to prescribe non-toxic and
long-lasting effective treatment.
The follow-up period for this patient was 47 months.
Median overall survival for patients with metastases with the same
condition is 12-15 months (7). The
current patient complained of reduced clarity of speech after
removal of metastasis from cerebellum, but was otherwise stable.
The patient continues treatment with hormonal and anti-HER2 therapy
without any signs of toxicity.
Thus, the present report demonstrated the efficacy
of combined hormonal and anti-HER2 therapy (a biosimilar of
trastuzumab, followed by lapatinib) in a patient with a rare and
aggressive disease, which otherwise would be treated with
chemotherapy due to current approaches.
In conclusion, standard approaches and guidelines on
cancer treatment often do not cover treatment possibilities for
rare tumors due to a lack of evidence. Current diagnostical
opportunities allow the possibly to identify a molecular pattern of
every tumor. Thus, the present report aimed to identify novel
options and appropriate solutions for patients whose tumor is not
mentioned in current guidelines. The present results demonstrated a
benefit of using hormonal and anti-HER2 therapy in a patient with
clear cell uterine carcinoma, as the treatment lead to prolonged
survival without any significant toxicity.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the present
study.
Authors' contributions
LAM, AAM and OOG were treating physicians. NAM was
responsible for radiology diagnosis. AIK was responsible for
pathology diagnosis. OOG, AAM and AIK drafted the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report and the
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jones NL, Xiu J, Chatterjee-Paer S, de
Meritens AB, Burke WM, Tergas AI, Wright JD and Hou JY: Distinct
molecular landscapes between endometrioid and nonendometrioid
uterine carcinomas. Int J Cancer. 140:1396–1404. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Glasspool RM and McNeish IA: Clear cell
carcinoma of ovary and uterus. Curr Oncol Rep. 15:566–572.
2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Abu-Rustum NR, Yashar CM, Bradley K, et
al: NCCN Clinical Practice Guidelines in Oncology. Uterine
Neoplasms. Version 4, 2019.
|
|
4
|
Yan M, Schwaederle M, Arguello D, Millis
SZ, Gatalica Z and Kurzrock R: HER2 expression status in diverse
cancers: Review of results from 37,992 patients. Cancer Metastasis
Rev. 34:157–164. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Halle MK, Tangen IL, Berg HF, Hoivik EA,
Mauland KK, Kusonmano K, Berg A, Hurtado A, Kalland KH, Øyan AM, et
al: HER2 expression patterns in paired primary and metastatic
endometrial cancer lesions. Br J Cancer. 118:378–387.
2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Fader AN, Roque DM, Siegel E, Buza N, Hui
P, Abdelghany O, Chambers SK, Secord AA, Havrilesky L, O'Malley DM,
et al: Randomized phase II trial of carboplatin-paclitaxel versus
carboplatin-paclitaxel-trastuzumab in uterine serous carcinomas
that overexpress human epidermal growth factor receptor 2/neu. J
Clin Oncol. 36:2044–2051. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lindahl B, Persson J, Ranstam J and Willén
R: Long-term survival in uterine clear cell carcinoma and uterine
papillary serous carcinoma. Anticancer Res. 30:3727–3730.
2010.PubMed/NCBI
|