Introduction
Solitary fibrous tumors (SFT) are derived from
mesenchymal cells originating mainly from the pleura, and cases
arising in the head and neck region are rare (especially those that
bleed). Many studies reporting tongue SFT treatments exist
(1-6),
but none have focused on the usefulness of preoperative arterial
embolization. According to a recent systemic review of the
literature that analyzed 2,629 studies on oral and maxillofacial
SFT (7), larger tumors are more
likely to be malignant and more aggressive, necessitating a
complete excision. For bleeding oral tumors, it is necessary to
consider the surgical procedure carefully because bleeding during
surgery and postoperative care may lead to incomplete resection and
airway problems. We treated a 32-year old woman with a gradually
increasing and dysarthria of hypervascular tongue SFT by applying
preoperative arterial embolization and then removed the tumor
safely and completely. At the time of this report, two years have
passed without recurrence.
Case report
A 32-year-old woman without remarkable medical or
family histories had been aware of a mass on the lower surface of
her tongue that had increased in size for half a year before her
first consultation. Her face was bilaterally symmetric without
regional lymph node swelling, but we noticed she had dysarthria
(probably due to the mass). Her routine laboratory blood work was
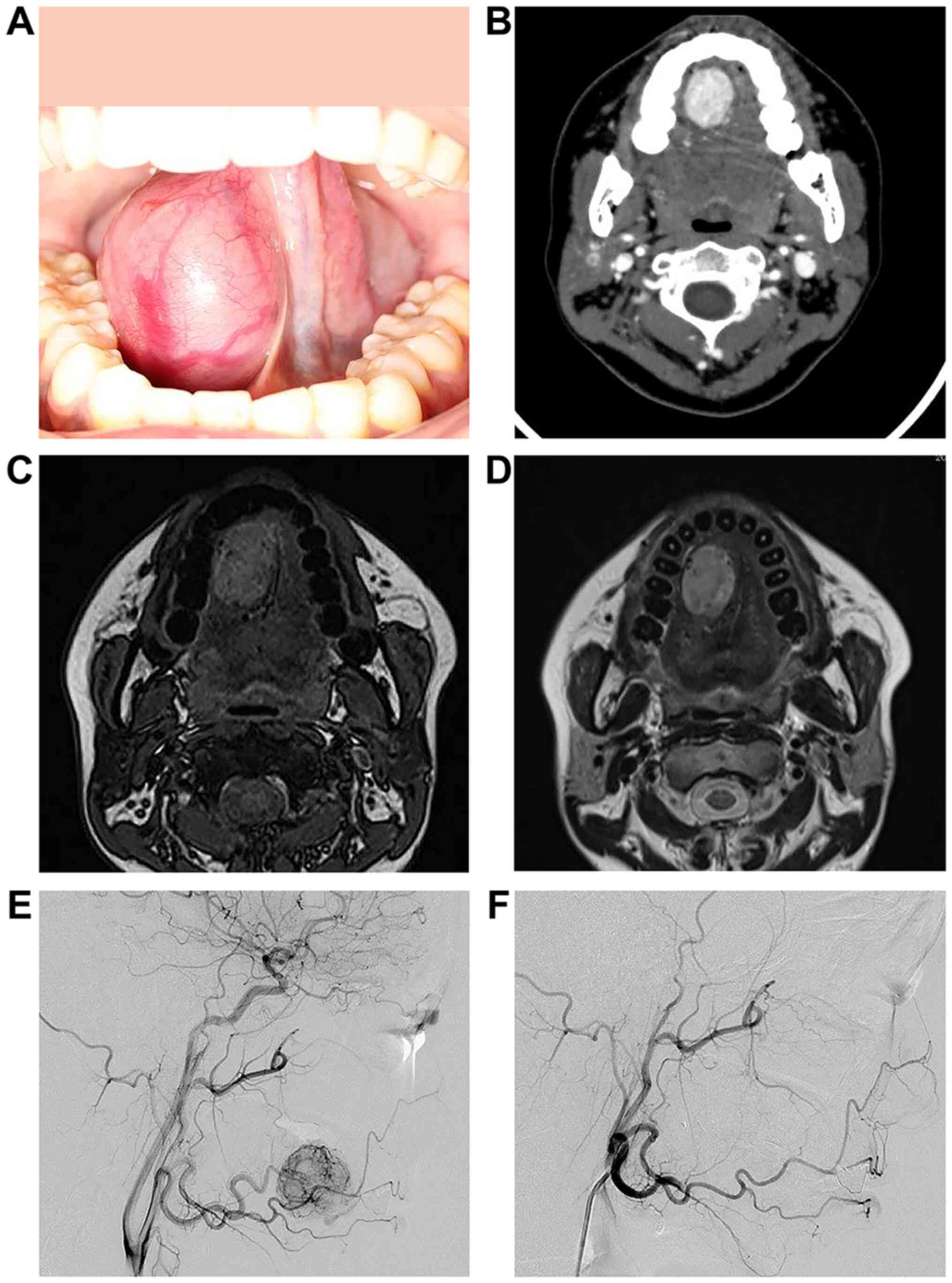
normal. We found an elastic and hard 30-mm tumor in the right lower
part of the tongue. Non-contrast-enhanced computed tomography (CT)
images revealed a tumor shadow with a clear border and uniform
margins in the right sublingual gap. Dynamic CT images of arterial
phase showed a strong enhancement with the inflow from an enlarged
right lingual artery thought to be a nutrient vessel. Dynamic CT
images of venous phase showed washed out contrast media.
Non-contrast-enhanced T1-weighted images showed many point-like low
and high signal areas, which is called a salt and pepper
appearance. T2-weighted image consisted mainly of high signals
compared with spinal cord and was partly accompanied by a cord-like
low signal area. An ultrasound showed a pulsatile blood flow signal
into the mass. We did not perform a histopathological examination
to avoid massive bleeding. We diagnosed the patient with
hypervascular tongue tumor, and at this stage, paraganglioma was
suspected.
We performed a transarterial embolization for the
right lingual artery embolization with 300-500 and 500-700-µm
embosphere microspheres (BioSphere Medical) through a vascular
catheter the day before the operation. The angiography after the
embolization confirmed the disappearance of the dense tumor
(Fig. 1). The next day, we
completely excised the encapsulated tumor under general anesthesia
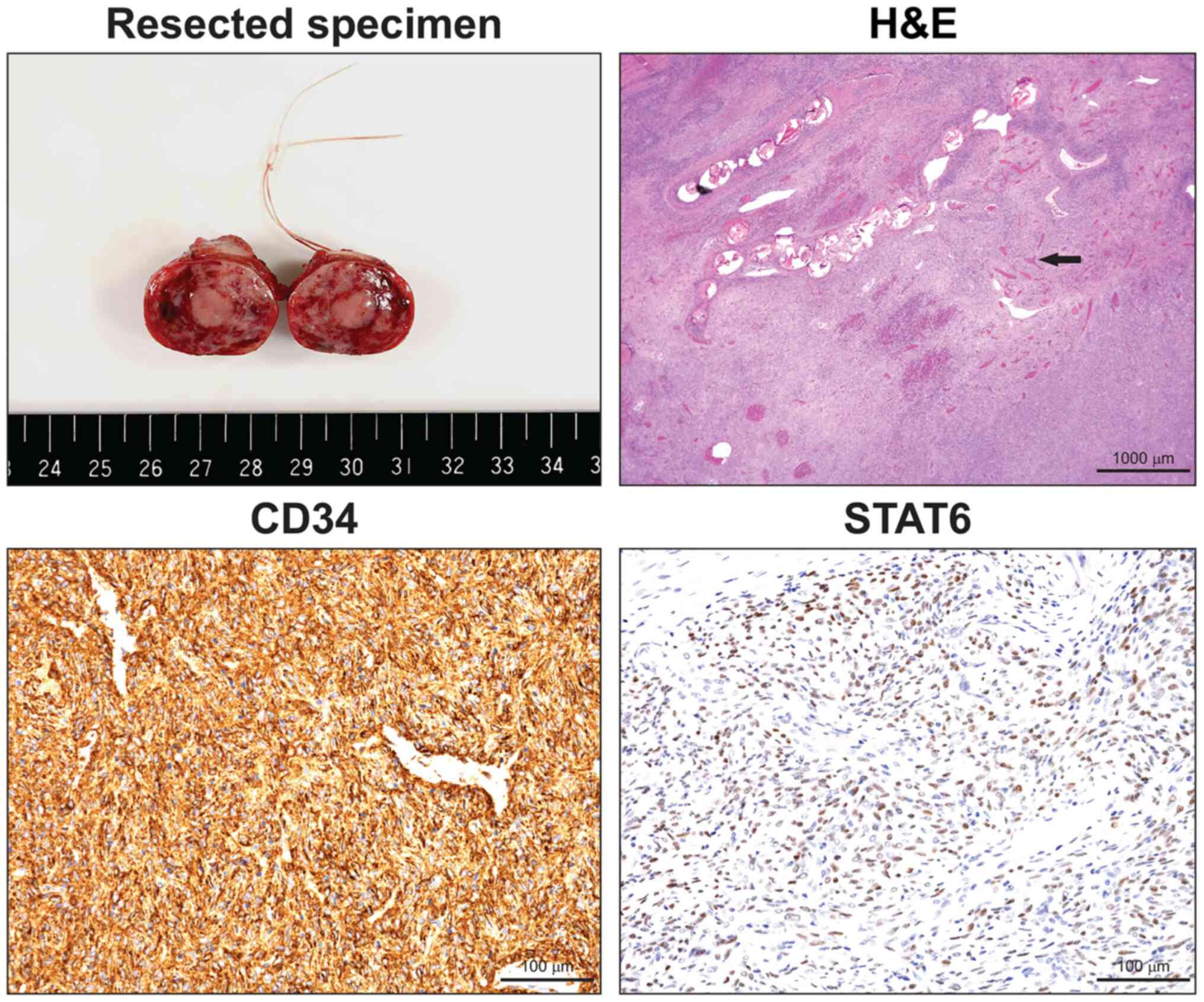
with little to no bleeding during the operation. The size of the
resected specimen after surgery was 31x28x18 mm, which was slightly
smaller than the size from preoperative CT findings. In addition,
the tumor was wrapped in a thin fibrous capsule with a reddish
white and solid appearance.
Pathology reported disordered growth of the tumor
cells with different densities, and an intricate structure and
floral arrangement. In addition, the tumor presented a cleft-like
blood vessel, and a staghorn-like blood vessel cavity.
Immunohistochemical staining showed spindle cells
with CD34-positive diffusivity, and scattered positive STAT6
spindle cells. S-100 protein was negative. The final diagnosis
based on findings was tongue SFT (Fig.
2).
Discussion
SFT was first reported as a pleural tumor in 1931 by
Klemperer and Rabin, and since a long time it has been thought to
be derived from the pleura (8).
According to the 2013 WHO bone/soft tissue tumor classification,
the tumor is a moderate malignant tumor and rarely occurs in the
oral region (9). Few polycystic
SFTs on the tongue have been reported.
Histopathological findings of SFTs show horn-like
blood vessels and tumor cells distributed in a ‘pattern-less’
pattern. According to Chan's diagnostic criteria, CD34 is an
effective diagnostic marker (10).
Robinson et al (11)
described 51 SFTs with NAB2 and STAT6 genes fusions. Thus, we
evaluated both markers (CD34 and STAT6) in our patient. Since this
case was that of a hypervascular tumor, histopathological
examination was not performed before surgery. In the image,
paragangliomas indicate the differential diagnosis.
The first choice of treatment is surgical resection,
and preoperative embolization is effective for highly irrigated
tumors to avoid intraoperative bleeding and incomplete removal,
which leads to high local recurrence rates (12). SFT surgery combined with
preoperative vascular embolism has already been reported (13-16),
but not in the tongue. Intraoperative and postoperative bleeding
can also lead to airway problems. To avoid unnecessary tracheostomy
and ligation of the maxillary artery, preoperative vascular
embolism may be considered aggressively when removing large tumors
or tumors with high blood flow. In the case of our patient, we
embolized the right lingual artery on the day before the resection,
and were able to excise the encapsulated tumor successfully under
general anesthesia the next day with little to no bleeding.
Many SFTs are benign and have a relatively good
prognosis. However, this tongue tumor is considered to be of
intermediate malignancy, and Fletcher et al (9) have reported a 10% recurrence rate. In
some cases, recurrences or metastases have been reported after more
than 10 years, and follow-ups are required for at least the first
two years after the resection (17). In addition to regular
contrast-enhanced CT examinations, we will consider abdominal
ultrasonography and chest radiographs. At the time of this report,
2 years have passed and the patient has followed a good course
without recurrence. We plan for a long-term follow-up.
We treated a patient with tongue SFT by applying
preoperative arterial embolization, and then removed the tumor
safely and completely. Transarterial embolization should be
actively combined with surgery for safe and reliable removal of
hypervascular oral tumors in the oral cavity.
Acknowledgements
The authors would like to thank Dr Toshitaka Nagao
and Dr Ai Enomoto of the Department of Anatomic Pathology, Tokyo
Medical University professional opinion about pathological
discussion and Dr Kazuhiro Saito of the Department of Radiology,
Tokyo Medical University for excellent management of the
embolization procedure.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
OH acquired patient data, performed the literature
review and edited the manuscript. DC conceived and designed the
present study. MW and MK acquired the data, provided clinical
advice and revised the manuscript. DY gave radiological advice. OH
wrote the manuscript. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
A signed written informed consent was obtained from
the patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Piatelli A, Fioroni M and Rubini C:
Solitary fibrous tumor of the tongue. Oral Oncol. 34:431–434.
1998.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Yamashita Y, Satoh T and Goto M: Solitary
fibrous tumor of the tongue: A case report with immunohistochemical
studies. Int J Oral Maxillofac Surg. 31:681–683. 2002.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Vafiadou M, Dimitrakopoulos I,
Georgitzikis I, Hytiroglou P, Bobos M and Karakasis D: Solitary
fibrous tumor of the tongue: Case report and literature review. Int
J Oral Maxillofac Surg. 37:1067–1069. 2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Migita M, Yoshino M, Kobayashi D, Shiomi
S, Enatsu K, Shigematsu S and Ohata H: A large solitary fibrous
tumor of the tongue. J Oral Maxillofac Surg. 70:871–874.
2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Shnayder Y, Greenfield BJ, Oweity T and
DeLacure MD: Malignant solitary fibrous tumor of the tongue. Am J
Otolaryngol. 24:246–249. 2003.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kaneko T, Kawano R, Horie N and Shimoyama
T: Solitary fibrous tumour of the tongue: A case report. Oral Surg.
11:65–68. 2018.
|
|
7
|
De Morais EF, Martins HD, Rodrigues KS, de
Franca GM, da Silveira ÉJ and Freitas RA: Clinicopathologic
analysis of oral and maxillofacial solitary fibrous tumor. Am J
Clin Pathol. 154:15–22. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Klempere P and Rabin CB: Primary neoplasm
of the pleura: A report of 5 cases. Arch Pathol. 11:385–412.
1931.
|
|
9
|
Fletcher CDM, Bridge JA and Lee JC:
Extrapleural solitary fibrous tumor. In: WHO classification of
tumors of soft tissue and bone. Fletcher CD, Bridge JA, Hogendoorn
PC and Mertens F (eds). IARC Press, Lyon, pp80-82, 2013.
|
|
10
|
Chan JK: Solitary fibrous
tumor-everywhere, and a diagnosis in vogue. Histopathology.
31:568–576. 1997.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Robinson DR, Wu YM, Kalyana-Sundaram S,
Cao X, Lonigro RJ, Sung YS, Chen CL, Zhang L, Wang R, Su F, et al:
Identification of recurrent NAB2-STAT6 gene fusions in solitary
fibrous tumor by integrative sequencing. Nat Genet. 45:180–185.
2013.PubMed/NCBI View
Article : Google Scholar
|
|
12
|
Craven JP, Quigley TM, Bolen JW and Raker
EJ: Current management and clinical outcome of hemangiopericytoma.
Am J Surg. 163:490–493. 1992.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Weiss B and Horton DA: Preoperative
embolization of a massive solitary fibrous tumor of the pleura. Ann
Thorac Surg. 73:983–985. 2002.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zeitler DM, Kanowitz SJ and Har-El G:
Malignant solitary fibrous tumor of the nasal cavity. Skull Base.
17:239–246. 2007.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Yokoyama Y, Hata K and Kanazawa T: Giant
solitary fibrous tumor of the pelvis successfully treated with
preoperative embolization and surgical resection: A case report.
World J Surg Oncol. 13:164–167. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yammine K, Nasser HA, Hadi U, Natout MA,
Najjar V and Tayar C: Salvage preoperative embolization of an
infratemporal solitary fibrous tumor: A case report with review of
the literature. Medicine (Baltimore). 97(e0251)2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Daigeler A, Lehnhardt M, Langer S,
Steinstraesser L, Steinau HU, Mentzel T and Kuhnen C:
Clinicopathological findings in a case series of extrathoracic
solitary fibrous tumors of soft tissues. BMC Surg.
6(10)2006.PubMed/NCBI View Article : Google Scholar
|