Introduction
Colorectal cancer is the third and second most
common cancer in males and females respectively (1). Rectal cancers comprise a third of
colorectal cancer cases and more commonly affects the elderly with
a peak incidence at 80-84 years (2).
Management of non-metastatic, locally advanced
rectal cancer is challenging and requires multidisciplinary care.
Elderly patients are at risk of aged-based disparities in cancer
treatment, which may include being under-treated due to their
chronological age, or over-treated for their degree of frailty
(3). It is often challenging for
the treating physician to find the optimal balance between
attaining good disease control and limiting the toxicities of
treatment for the elderly patient who may also have competing
comorbidities. Data to guide treatment of elderly patients with
rectal cancer is limited as the elderly patients are often
under-represented in prospective clinical trials (4). The optimal treatment approach in this
group will likely become even more nuanced with the gradual
paradigm shift toward non-operative approaches in locally advanced
rectal cancer (5).
The current standard surgical management of rectal
cancer involves performing a total mesorectal excision (TME) for
improved local control of disease and survival (6,7).
Other operative approaches for selected patients with low risk
early rectal cancers include transanal endoscopic microsurgery
(TEM) and local excision (8,9). For
locally advanced rectal cancer (clinical ≥T3 or node positive),
trimodality therapy consisting of neoadjuvant chemoradiotherapy
followed with surgery, with adjuvant post-operative chemotherapy,
is the current standard of care (10). Trimodality therapy has been shown
to have a survival benefit in elderly patients. Cancer specific
survival was shown to be 70% in patients aged >75 who received
neoadjuvant therapy, compared to 52% with surgery alone and 60%
with adjuvant therapy (11).
Multiple studies have found that older patients are less likely to
receive neoadjuvant therapy, and that this is associated with
poorer cancer-specific survival (12-14).
One study found that each 5 years over the age of 70 was associated
with a 37% increase in cancer-related mortality (13).
The reasons for a lower uptake of trimodality
therapy in the older patients is multifactorial, including an
increased incidence of treatment-related complications. The
literature is divided on this, with some studies demonstrating an
increase in complication rates (15-17),
and some reporting a good tolerance of treatment (18-20).
Taking the evidence into account, the literature
suggests that selected elderly patients should be treated in the
same way, if comorbidity allows (21-23).
The likelihood of initiation of therapy was found to be 22% lower
in elderly patients, even after adjusting for comorbidities and
other variables (24).
There is also data to suggest that elderly patients
may have a different biology to younger patients. Patients over the
age of 75 were found to have a lower likelihood of having distant
metastases (12) and less advanced
stage at presentation (13).
Given the lack of clarity in the literature, we
aimed to examine the treatment patterns and outcomes of the elderly
population with non-metastatic rectal cancer.
Materials and methods
Study population
The study received approval from the South Western
Sydney Local Health District and the Illawarra Shoalhaven Local
Health District ethics committees. The study was performed in
accordance with the Declaration of Helsinki. The need for informed
consent was waived due to the low and negligible risk, and
retrospective nature, of the work.
We utilised data from prospectively collated
electronic records to identify patients with a histological
diagnosis of rectal adenocarcinoma from 2006-2015, treated in the
South Western Sydney and Illawarra Shoalhaven Local Health
Districts, Australia. Patients with metastatic disease at diagnosis
were excluded. Stage of disease was based on the 8th edition of the
American Joint Committee on Cancer and College of American Joint
Pathologists (AJCC) (25). Staging
was based on clinical stage in patients undergoing neoadjuvant
therapy, or pathological stage for patients who had surgery
upfront. Clinicopathological variables, treatment modalities,
recurrence and survival data were analysed.
Relapse-free survival was defined as the date of
diagnosis to recurrence locally or distantly. Cancer specific
survival was defined as date of diagnosis to death from rectal
cancer. Overall survival was defined as the date of diagnosis to
death from any cause. Patients who had not recurred and are still
alive were censored at the date of last follow up.
Statistical analysis
Clinicopathological factors and treatment
utilisation rates between patients <70 and ≥70 years were
compared using Chi-Square. Median values for survival and
corresponding 95% confidence intervals (CI) were calculated using
Kaplan-Meier methods, and the log rank test was used to calculate
P-values. Unadjusted and multivariable Cox proportional hazards
regression analyses were used to estimate the association of age
with survival outcomes, and to calculate corresponding hazard
ratios (HRs) and 95% confidence intervals. The following variables
were included in the multivariate model: Age, grade, lymphovascular
invasion, perineural invasion, TNM stage, and receipt of adjuvant
treatment. All statistical analyses were performed using SAS 9.2
software (SAS Institute, Inc.).
Results
Clinicopathological variables
We identified 736 patients with localized (stage
I-III) rectal cancer, with median follow-up of 3.4 years. Of these,
326 (44.2%) were ≥70 years (median age at diagnosis 67 years, range
21-94). Elderly patients were more likely to present with earlier
stage disease (stage III 47.6 vs. 57.1%, P=0.03), but there were no
differences in other histopathological variables with age (Table I).
 | Table IClinicopathological characteristics,
surgical management and outcomes stratified by age. |
Table I
Clinicopathological characteristics,
surgical management and outcomes stratified by age.
| | Age, years, n
(%) | |
|---|
| Clinicopathological
characteristics | <70 | ≥70 | Total, n (%) | P-value |
|---|
| Total | 410 (66.0) | 326 (44.0) | 736 (100.0) |
| Sex, male | 269 (65.6) | 202 (62.0) | 471 (64.0) | 0.3000 |
| TNM stage | | | | |
|
I | 77 (18.8) | 80 (24.5) | 157 (21.3) | 0.0300 |
|
II | 99 (24.1) | 91 (27.9) | 190 (25.8) | |
|
III | 234 (57.1) | 155 (47.6) | 389 (52.9) | |
| Lymphovascular
invasiona | 82 (20.8) | 62 (21.3) | 144 (21.1) | 0.8700 |
| Perineural
invasionb | 50 (13.2) | 30 (10.8) | 80 (12.2) | 0.3700 |
| Positive
marginc | 21 (5.3) | 16 (5.5) | 37 (5.4) | 0.3900 |
| Grade 3d | 37 (9.2) | 28 (9.2) | 65 (9.2) | 0.9800 |
| Discussed at MDT | 222 (59.5) | 155 (50.2) | 377 (55.3) | 0.0100 |
| Surgerye | | | | |
|
Anterior
resection | 271 (66.6) | 175 (54.2) | 446 (61.1) | <0.0001 |
|
APR | 93 (23.9) | 81 (25.1) | 174 (23.8) | |
|
Hartmann's
procedure | 6 (1.5) | 19 (5.9) | 25 (3.4) | |
|
Local
Resection | 9 (2.2) | 21 (6.5) | 30 (4.1) | |
|
Other,
including palliative surgery | 20 (4.9) | 3 (0.9) | 23 (3.1) | |
|
No
surgery | 8 (2.0) | 24 (7.4) | 32 (4.4) | 0.0014 |
| Death within 30
days of surgery | 0 (0.0) | 8 (2.5) | 8 (1.1) | 0.0014 |
Treatment modalities
Elderly patients were more likely to be treated with
a non-operative approach across all stages (7.4 vs. 2.0%,
P=0.0014). In the management of stage I rectal cancer, a small
percentage of elderly patients were treated non-operatively whilst
all patients <70 years had curative intent surgery (8.8 vs. 0%,
P=0.0079). In patients with stage III disease, elderly patients
were more likely to be treated with surgery alone (25.2 vs. 4.3%,
P<0.001), less likely to receive neoadjuvant (36.8 vs. 54.3%,
P=0.007) or adjuvant therapy (47.1 vs. 79.1%, P<0.001). These
results are shown in Table II.
Two hundred and eight patients received neoadjuvant
chemoradiotherapy and only 4 (2%) patients did not complete the
entire radiotherapy course. Of these, 3 patients were <70 years
and 1 patient was ≥70 years.
| Table IITreatment modalities stratified by
stage. |
Table II
Treatment modalities stratified by
stage.
| A, Stage I
(n=157) |
|---|
| | Age, years | |
|---|
| Treatment
modalities | <70 | ≥70 | P-value |
|---|
| Total | 77 | 80 | |
| Non-operative
approach | 0 | 7 | |
| Curative
resection | 77 | 73 | 0.0079 |
|
Surgery
only | 74 | 70 | 0.0510 |
|
Neoadjuvant
therapy | 3 | 1 | 0.2900 |
|
Adjuvant
therapy | 2 | 2 | 0.9600 |
| B, Stage II
(n=190) |
| | Age, years | |
| Treatment
modalities | <70 | ≥70 | P-value |
| Total | 99 | 91 | |
| Non-operative
approach | 5 | 7 | |
| Curative
resection | 94 | 84 | 0.4500 |
|
Surgery
only | 29 | 59 | <0.0001 |
|
Neoadjuvant
therapy | 52 | 22 | <0.0001 |
|
Adjuvant
therapy | 34 | 10 | 0.0001 |
| C, Stage III
(n=389) |
| | Age, years | |
| Treatment
modalities | <70 | ≥70 | P-value |
| Total | 234 | 155 | |
| Non-operative
approach | 5 | 16 | |
| Curative
resection | 229 | 139 | 0.0005 |
|
Surgery
only | 10 | 39 | <0.0010 |
|
Neoadjuvant
therapy | 127 | 57 | 0.0070 |
|
Adjuvant
therapy | 185 | 73 | <0.0010 |
Surgical modality also differed with age, with the
elderly patients less likely to undergo anterior resection and more
likely to have a Hartmann's procedure (P<0.0001). The elderly
cohort were also more likely to die within 30 days of surgery
(P=0.0014) and less likely to be discussed at a multidisciplinary
meeting (P=0.01), as depicted in Table
I. The majority of post-operative deaths were from emergency
surgeries for acute presentations such as bowel perforation.
Relapse and survival data
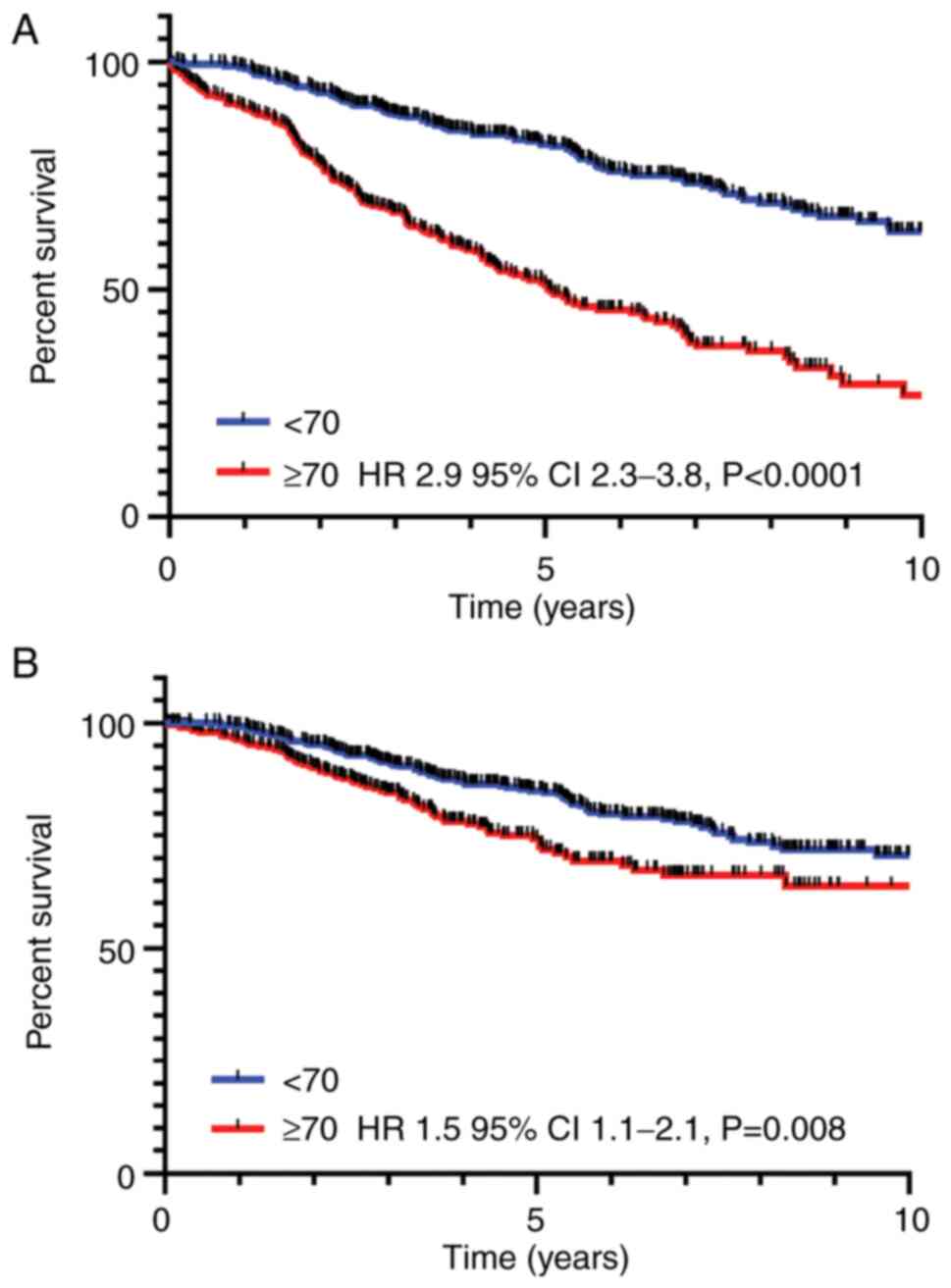
Overall survival was poorer in the elderly cohort (5
year overall survival 52 vs. 82%, P<0.0001), Fig. 1A. Univariate analyses for overall
survival showed age, grade, presence of lymphovascular or
perineural invasion, stage and adjuvant therapy to be significant
predictors (Table III). Age,
tumour grade, perineural invasion and adjuvant treatment remained
significant in multivariate analyses.
| Table IIIUnivariate and multivariate analyses
for overall survival and cancer-specific survival. |
Table III
Univariate and multivariate analyses
for overall survival and cancer-specific survival.
| A, Overall
survival |
|---|
| Clinicopathological
characteristics | Univariate HR (95%
CI) | P-value | Multivariate HR
(95% CI) | P-value |
|---|
| Age <70,
years | 1.0 | | | |
| Age ≥70, years | 2.9 (2.3-3.8) | <0.0001 | 2.6 (2.0-3.5) | <0.0001 |
| Grade 1-2 | 1.0 | | | |
| Grade 3 | 1.8 (1.3-2.6) | 0.0010 | 1.5 (1.0-2.2) | 0.0420 |
| Lymphovascular
invasion | 1.6 (1.2-2.1) | 0.0040 | 1.3 (0.9-1.8) | 0.1600 |
| Perineural
invasion | 2.1 (1.5-2.8) | <0.0001 | 2.2 (1.6-3.2) | <0.0001 |
| TNM stage | | | | |
|
I | 1.0 | 0.0500 | 1.0 | 0.2800 |
|
II | 1.5 (1.1-2.2) | | 1.4 (0.9-2.1) | |
|
III | 1.2 (0.9-1.7) | | 1.4 (0.9-2.2) | |
| Adjuvant
treatment | 0.6 (0.4-0.7) | <0.0001 | 0.6 (0.5-0.9) | 0.0045 |
| Neoadjuvant
treatment | 0.9 (0.7-1.1) | 0.3600 | 1.0 (0.8-1.4) | 0.9600 |
| B, Cancer-specific
survival |
| Clinicopathological
characteristics | Univariate HR (95%
CI) | P-value | Multivariate HR
(95% CI) | P-value |
| Age ≥70, years | 1.5 (1.1-2.1) | 0.0080 | 1.5 (1.0-2.1) | 0.0400 |
| Grade 3 | 2.8 (1.8-4.2) | <0.0001 | 2.1 (1.4-3.4) | 0.0008 |
| Lymphovascular
invasion | 2.1 (1.5-3.2) | <0.0001 | 1.5 (1.0-2.3) | 0.0400 |
| Perineural
invasion | 2.6 (1.7-3.9) | <0.0001 | 1.9 (1.2-2.9) | 0.0040 |
| TNM stage | | | | |
|
I | 1.0 | <0.0001 | 1.0 | 0.0020 |
|
II | 7.3 (3.1-17.1) | | 6.2 (2.2-17.7) | |
|
III | 7.2 (3.1-16.3) | | 6.7 (2.3-19.6) | |
| Adjuvant
treatment | 1.04 (0.8-1.4) | 0.8000 | 0.8 (0.5-1.2) | 0.3400 |
| Neoadjuvant
treatment | 1.3 (0.9-1.8) | 0.1200 | 1.1 (0.8-1.6) | 0.6000 |
Cancer specific survival was also poorer in the
elderly cohort (5 year cancer specific survival 75 vs. 85%,
P=0.008), Fig. 1B. For
cancer-specific survival, age and histopathological variables were
significant, but treatment modality did not impact outcomes in
multivariate analysis (Table
III).
Relapse-free survival was affected significantly by
grade, lymphovascular and perineural invasion, as well as stage
(Table IV). Use of neoadjuvant
and adjuvant therapy predicted for worse survival in univariate
analyses but were not significant in multivariate analyses.
| Table IVUnivariate and multivariate analyses
for relapse-free survival. |
Table IV
Univariate and multivariate analyses
for relapse-free survival.
| Clinicopathological
characteristics | Univariate HR (95%
CI) | P-value | Multivariate HR
(95% CI) | P-value |
|---|
| Age ≥70 | 0.9 (0.7-1.2) | 0.5000 | 1.0 (0.7-1.3) | 0.9900 |
| Grade 3 | 2.1 (1.5-3.2) | <0.0001 | 1.9 (1.2-2.8) | 0.0030 |
| Lymphovascular
invasion | 1.9 (1.4-2.5) | <0.0001 | 1.4 (1.0-2.0) | 0.0400 |
| Perineural
invasion | 2.2 (1.5-3.1) | <0.0001 | 1.7 (1.1-2.4) | 0.0108 |
| TNM stage | | | | |
|
I | 1.0 | <0.0001 | 1.0 | 0.0030 |
|
II | 3.4 (2.0-5.8) | | 2.9 (1.6-5.5) | |
|
III | 3.8 (2.3-6.2) | | 2.7 (1.4-5.1) | |
| Adjuvant
treatment | 1.5 (1.2-2.0) | 0.0030 | 1.1 (0.8-1.6) | 0.6000 |
| Neoadjuvant
treatment | 1.5 (1.2-2.0) | 0.0030 | 1.2 (0.9-1.6) | 0.4000 |
Cancer-specific survival stratified by
age
Elderly patients with stage III disease have worse
outcomes compared to younger patients (Table V). However, elderly patients who
received neoadjuvant +/- adjuvant therapy did not have
significantly different outcomes compared to younger patients.
| Table VUnivariate analyses of
cancer-specific survival stratified by age. |
Table V
Univariate analyses of
cancer-specific survival stratified by age.
| Stages | Univariate HR (95%
CI)a | P-value |
|---|
| Stage I | 0.8 (0.1-4.5) | 0.8000 |
| Stage II | 1.1 (0.6-1.9) | 0.8000 |
| Stage III | 2.1 (1.4-3.2) | 0.0002 |
| Stages II/III and
received neoadjuvant therapyb | 1.4 (0.8-2.4) | 0.2600 |
| Stages II/III and
received neoadjuvant and adjuvant therapyc | 1.4 (0.7-3.2) | 0.3200 |
Summary of salient findings
Elderly patients composed almost half of the cohort,
and presented with earlier stage disease. They were less likely to
undergo trimodality therapy or discussed in a multidisciplinary
meeting. Surgery in the elderly patients was more commonly a
Hartmann's procedure, and surgery was associated with increased
immediate post-operative mortality. Elderly patients had worse
overall survival and cancer-specific survival, particularly evident
in stage III disease. Elderly patients in this subgroup treated
with trimodality therapy had similar survival outcomes to younger
patients.
Discussion
Our study found that almost half of patients with
non-metastatic rectal cancer undergoing treatment were over the age
of 70. Although the majority (>90%) of elderly rectal cancer
patients were treated with curative intent, this was significantly
less than in younger patients. Elderly patients were less likely to
receive trimodality therapy or be discussed in a multidisciplinary
meeting. The more conservative approach toward treatment in the
elderly may be largely due to the uncertainty around clinical
decision making in this group, as they are largely excluded from
clinical trials. In addition, the elderly have competing
comorbidities which may complicate treatment. The elderly group was
also less likely to undergo an anterior resection, and more likely
to undergo a Hartmann's procedure or abdominoperineal resection.
Surgery was associated with a higher death rate within 30 days
post-operatively, albeit rates are still low (2.5%) with most of
these being emergency surgeries for acute presentations such as
bowel perforation.
In this study, the overall survival and cancer
specific survival for elderly patients with non-metastatic rectal
cancer was significantly worse compared to younger patients. In
stage III patients, we found that cancer-specific outcomes were
more than two times poorer compared to younger patients. However,
in the subgroup treated with trimodality therapy, outcomes were not
inferior to the younger patients. These findings are consistent
with previous studies in the literature which have reported lower
utilisation of trimodality therapy in the elderly patients
(12-14).
The literature also reports inferior cancer specific outcomes in
the older population (11,13). However we did not find significant
differences in recurrence rates in the elderly patients, suggesting
that cancer specific survival may potentially be impacted by
variable treatment modalities at the time of recurrence, or
alternatively differences in surveillance post curative intent
therapy.
The elderly population in our study presented with
earlier stage disease which may reflect a difference in tumour
biology or be attributed to incidental findings whilst screening
for other conditions. This is consistent with some studies in the
literature (12,13). A study exploring the genomic makeup
of colorectal tumours found that older patients, defined as ≥70,
had a greater index of genetic mutations, and a higher incidence of
KRAS and BRAF mutations but less PTEN/PIK3CA mutations (26).
Limitations of this study include its retrospective
nature, and the inability to assess the benefits of treatment due
to selection bias. Fitter patients are expected to be selected to
undergo adjuvant therapy thereby affecting overall survival, and
patients with poor biology or very locally advanced disease are
expected to undergo trimodality therapy hence translating to worse
cancer specific outcomes. We recognise that we did not collect data
on comorbidities and performance status which may impact on
treatment pattern selection. Future research focused on the
geriatric population will require information on comorbidities,
nutritional status, cognitive status, and can employ the use of
geriatric screening tools.
The toxicities and morbidity associated with
trimodality therapy for locally advanced rectal cancer impact
deliverability, especially in the elderly population. These
patients are often excluded in clinical trial populations and hence
the best management strategies and outcomes of treatment are
unclear. There is also a shift towards a non-operative approach in
the treatment of locally advanced rectal cancer (5), making treatment decision making in
the older patients even more nuanced. Our study adds valuable
insight into the treatment practices and outcomes in these
patients, which comprise a large proportion of the patient
population. Consideration should be given into deciding whether an
‘elderly’ patient should receive trimodality therapy, depending on
their biological age and comorbidities, and not purely on
chronological age alone. Elderly patients would benefit from being
discussed in a multidisciplinary meeting. This is especially the
case as life expectancy continues to rise, chronic illnesses are
better managed, and definitions of the older patient are likely to
shift upwards with time.
Acknowledgements
The authors would like to acknowledge Dr Sharlyn
Kang (Illawarra Cancer Care Centre, University of Wollongong,
Wollongong, New South Wales, Australia) for her contribution to the
research in this manuscript before her passing and would like to
dedicate this work to her memory. The abstract was presented in
poster form at the American Society of Clinical Oncology (ASCO)
Gastrointestinal Cancers Symposium January 2019 in San Francisco,
CA and published as abstract no. 4 in Journal of Clinical Oncology
Volume 37 (Suppl) (February 01, 2019) 678-678.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SK, KJW, DB and SHSL designed and conceived the
present study. SK, KJW, DB, WC, WN, JC, EN, ML, KW, LB, RW, SP, CSL
and SHSL were all responsible for the provision of patient
materials and data collection. SK, KJW, DB and SHSL performed data
analysis and interpretation. SK, KJW and DB confirm the
authenticity of all the raw data. All authors wrote the manuscript.
All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the South Western
Sydney Local Health District (approval no. HREC/12/LPOOL/102) and
the ethics committee of the Illawarra Shoalhaven Local Health
District (approval no. LNR/15/WGONG/61). This study was performed
in accordance with the Declaration of Helsinki. The need for
informed consent was waived due to the low and negligible risk, and
retrospective nature of the work.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386.
2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Australian Institute of Health and Welfare
2015. Australia's Welfare 2015. Australia's welfare series no. 12.
Cat. no. AUS 189. Canberra, 2015.
|
|
3
|
Lawler M, Selby P, Aapro MS and Duffy S:
Ageism in cancer care. BMJ. 348(g1614)2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Hurria A, Dale W, Mooney M, Rowland JH,
Ballman KV, Cohen HJ, Muss HB, Schilsky RL, Ferrell B, Extermann M,
et al: Designing therapeutic clinical trials for older and frail
adults with cancer: U13 conference recommendations. J Clin Oncol.
32:2587–2594. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Greer JB and Hawkins AT: Non-operative
management of rectal cancer. Semin Colon Rectal Surg. 30:79–84.
2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Heald RJ and Ryall RD: Recurrence and
survival after total mesorectal excision for rectal cancer. Lancet.
1:1479–1482. 1986.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kapiteijn E, Putter H and van de Velde CJ:
Cooperative investigators of the Dutch ColoRectal Cancer Group.
Impact of the introduction and training of total mesorectal
excision on recurrence and survival in rectal cancer in The
Netherlands. Br J Surg. 89:1142–1149. 2002.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ahn T: What should be considered for local
excision in early rectal cancer? Ann Coloproctol. 35:155–157.
2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Althumairi AA and Gearhart SL: Local
excision for early rectal cancer: Transanal endoscopic microsurgery
and beyond. J Gastrointest Oncol. 6:296–306. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Sauer R, Liersch T, Merkel S, Fietkau R,
Hohenberger W, Hess C, Becker H, Raab HR, Villanueva MT, Witzigmann
H, et al: Preoperative versus postoperative chemoradiotherapy for
locally advanced rectal cancer: Results of the German
CAO/ARO/AIO-94 randomized phase III trial after a median follow-up
of 11 years. J Clin Oncol. 30:1926–1933. 2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Wan JF, Zhu J, Li GC, Sun WJ and Zhang Z:
Implications for determining the optimal treatment for locally
advanced rectal cancer in elderly patients aged 75 years and older.
Oncotarget. 6:30377–30383. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Jung B, Pahlman L, Johansson R and Nilsson
E: Rectal cancer treatment and outcome in the elderly: An audit
based on the Swedish Rectal Cancer Registry 1995-2004. BMC Cancer.
9(68)2009.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Chang GJ, Skibber JM, Feig BW and
Rodriguez-Bigas M: Are we undertreating rectal cancer in the
elderly? An epidemiologic study. Ann Surg. 246:215–221.
2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Thiels CA, Bergquist JR, Meyers AJ,
Johnson CL, Behm KT, Hayman AV, Habermann EB, Larson DW and Mathis
KL: Outcomes with multimodal therapy for elderly patients with
rectal cancer. Br J Surg. 103:e106–e114. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Shahir MA, Lemmens VE, van de Poll-Franse
LV, Voogd AC, Martijn H and Janssen-Heijnen ML: Elderly patients
with rectal cancer have a higher risk of treatment-related
complications and a poorer prognosis than younger patients: A
population-based study. Eur J Cancer. 42:3015–3021. 2006.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Margalit DN, Mamon HJ, Ancukiewicz M,
Kobayashi W, Ryan DP, Blaszkowsky LS, Clark J, Willett CG and Hong
TS: Tolerability of combined modality therapy for rectal cancer in
elderly patients aged 75 years and older. Int J Radiat Oncol Biol
Phys. 81:e735–e741. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Francois E, Azria D, Gourgou-Bourgade S,
Jarlier M, Martel-Laffay I, Hennequin C, Etienne PL, Vendrely V,
Seitz JF, Conroy T, et al: Results in the elderly with locally
advanced rectal cancer from the ACCOR12/PRODIGE 2 phase III trial:
Tolerance and efficacy. Radiother Oncol. 110:144–149.
2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Choi Y, Kim JH, Kim JW, Kim JW, Lee KW, Oh
HK, Kim DW, Kang SB, Song C and Kim JS: Preoperative
chemoradiotherapy for elderly patients with locally advanced rectal
cancer-a real-world outcome study. Jpn J Clin Oncol. 46:1108–1117.
2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Guimas V, Boustani J, Schipman B, Lescut
N, Puyraveau M, Bosset JF and Servagi-Vernat S: Preoperative
chemoradiotherapy for rectal cancer in patients aged 75 Years and
older: Acute toxicity, compliance with treatment, and early
results. Drugs Aging. 33:419–425. 2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Pasetto LM, Friso ML, Pucciarelli S, Basso
U, Falci C, Bortolami A, Toppan P, Agostini M, Rugge M, Serpentini
S, et al: Rectal cancer neoadjuvant treatment in elderly patients.
Anticancer Res. 26 (5B):3913–3923. 2006.PubMed/NCBI
|
|
21
|
Jiang DM, Raissouni S, Mercer J, Kumar A,
Goodwin R, Heng DY, Tang PA, Doll C, MacLean A, Powell E, et al:
Clinical outcomes of elderly patients receiving neoadjuvant
chemoradiation for locally advanced rectal cancer. Ann Oncol.
26:2102–2106. 2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Tougeron D, Roullet B, Paillot B, Hamidou
H, Tourani JM, Bensadoun RJ, Michel P and Silvain C: Safety and
outcome of chemoradiotherapy in elderly patients with rectal
cancer: Results from two French tertiary centres. Dig Liver Dis.
44:350–354. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Dobie SA, Warren JL, Matthews B, Schwartz
D, Baldwin LM and Billingsley K: Survival benefits and trends in
use of adjuvant therapy among elderly stage II and III rectal
cancer patients in the general population. Cancer. 112:789–799.
2008.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Bohac GC, Guaqueta D, Cheng DM, Aschengrau
A and Hartshorn KL: Disparity in the use of combined modality
therapy for rectal cancer in the older adult. J Geriatr Oncol.
4:90–97. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The Eighth Edition AJCC cancer staging manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Berg M, Danielsen SA, Ahlquist T, Merok
MA, Agesen TH, Vatn MH, Mala T, Sjo OH, Bakka A, Moberg I, et al:
DNA sequence profiles of the colorectal cancer critical gene set
KRAS-BRAF-PIK3CA-PTEN-TP53 related to age at disease onset. PLoS
One. 5(e13978)2010.PubMed/NCBI View Article : Google Scholar
|