Introduction
Medullary thyroid carcinoma (MTC), which accounts
for 1-2% of thyroid carcinomas, occurs sporadically or in a
hereditary form associated with two types of multiple endocrine
neoplasia (MEN), MEN2A and MEN2B, as well as familial MTC (FMTC)
(1-7).
MEN is inherited in an autosomal dominant manner (4,5). The
rearranged during transfection (RET) germline mutation is
associated with MEN2A, MEN2B and FTMC and most patients with MEN2B
have RET codon M918T mutation (2-7).
The RET codon M918T mutation is the highest risk factor for MTC,
according to American Thyroid Association (ATA) guidelines
(8). Although the diagnosis of
MEN2B at an early age is optimal, the majority of patients are
diagnosed after reaching an advanced state (9). MTC and MEN2B patients as well as
their relatives must be examined carefully due to the hereditary
characteristics of this disease. Genetic counseling is necessary in
numerous cases. The authors of the present study encountered four
cases of MTC with MEN2B in the same family. Sequencing by synthesis
was adopted for genetic testing of all four cases (10).
Case reports
Case 1
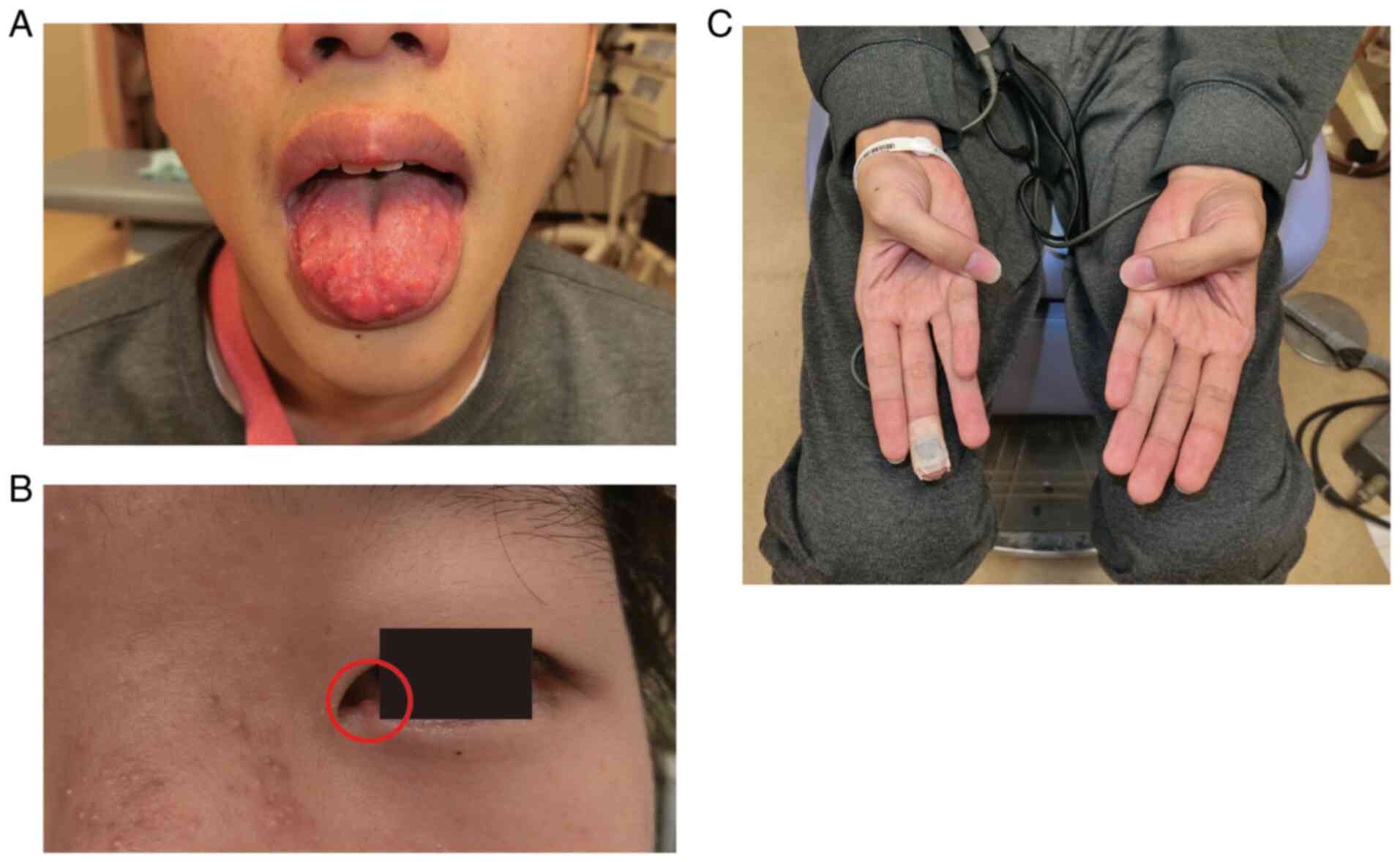
The first case was that of a 19-year-old male
presenting with cervical swelling, dyspnea and chronic diarrhea.
Peculiar physical features included neuromas of the tongue
(Fig. 1A) and eyelid (Fig. 1B), as well as marfanoid habitus
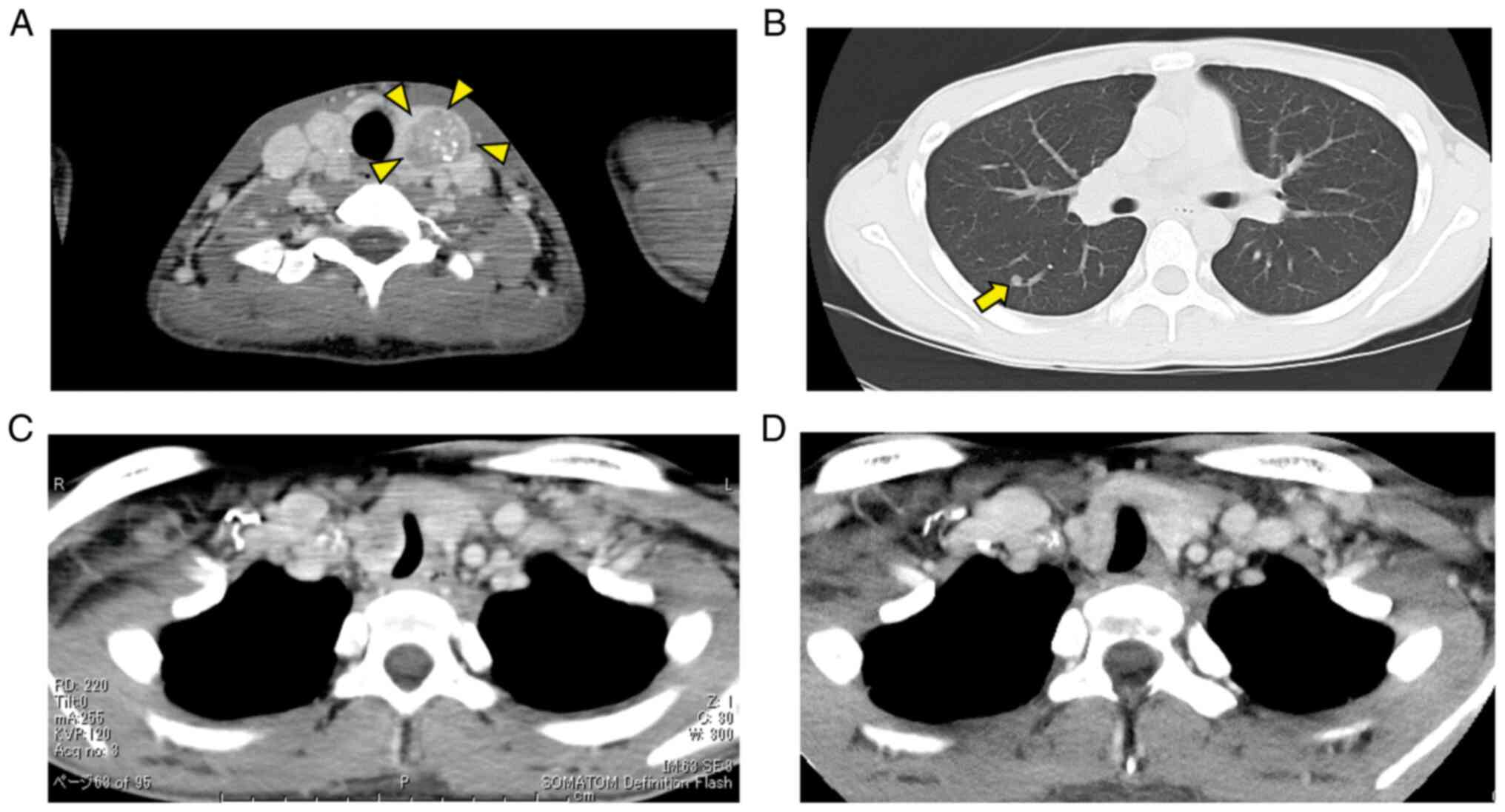
(Fig. 1C). A blood test revealed
high levels of carcinoembryonic antigen (CEA) and calcitonin (Ctn).
Computed tomography (CT) showed unresectable tumors of the thyroid,
bilateral neck lymphadenopathy (Fig.
2A) and multiple nodules in both lungs (Fig. 2B). The trachea was narrowed and
deviated due to a thyroid mass (Fig.
2C). Histologic examination confirmed a diagnosis of MTC
(cT4bN1bM1, stage IV). Due to lung metastases, vandetanib, a
tyrosine kinase inhibitor, was administered. The daily dose of
vandetanib was 300 mg. Cardiovascular monitoring was also performed
to control electrolyte disturbance-related adverse events due to
persistent diarrhea and arrhythmia, such as QT prolongation.
Although QT prolongation developed in the patient, the treatment
continued without complication. After starting treatment with
vandetanib, diarrhea persisted with varying severity. On the
contrary, the tumor size was mildly reduced (Fig. 2D). All the nodules in the lungs
disappeared. At 25 months after the initial treatment, the patient
remains in good condition and the disease has shown no progression.
Genetic testing identified the RET mutation in the M918T codon. As
the patient confirmed MEN2B, the authors suggested genetic
counseling for the family.
Case 2
The second case was that of the 43-year-old mother
of the patient in Case 1. She presented with eyelid neuromas. She
was treated for MTC surgically at another hospital when she was 12
years old. Regrettably, the hereditary nature of her disease was
not explained to her. It was not until her son was diagnosed as
MEB2B that she understood the disease. Genetic testing at Nara
Medical University identified her children's RET codon M918T
mutation. As her parents had no history of thyroid disease, she may
have been the first in her family to acquire an RET codon M918T
mutation and developed MTC. Records from her previous hospital
showed that she had undergone total thyroidectomy (TT) with
bilateral neck dissection and was negative for pheochromocytoma
(PHEO). In addition, she had been diagnosed with mucosal neuroma of
the tongue based on histopathologic examination. She has been
followed up at Nara Medical University and no recurrence or distant
metastasis has been observed.
Case 3
The third case was that of the 16-year-old elder
sister of the patient in Case 1. Although she had no symptoms of
MTC, she had tongue neuromas similar to those of her brother. She
underwent MTC assessment after her mother and brother were
diagnosed. Her blood tests showed abnormally high levels of CEA and
Ctn and thyroid masses were detected by ultrasonography. Although
an adrenal gland mass was detected by ultrasonography, she was
negative for PHEO based on blood test analysis and magnetic
resonance imaging. Eventually, MTC was confirmed histocytologically
by fine-needle aspiration cytology. Positron emission tomography
did not show any signs of lymph node or distant metastases. The
patient underwent TT with neck dissection in the central
compartment. She exhibits no signs of recurrence 24 months after
surgery. Genetic testing also revealed an RET codon M918T
mutation.
Case 4
The final case was that of the younger sister of the
patient in Case 1. She was 10 years old at the time of treatment.
She also had neuromas of the tongue and additional ophthalmologic
abnormalities. She had slightly high Ctn levels but no thyroid
masses. In addition, no adrenal gland tumors were detected and she
was also biochemically negative for PHEO. However, considering the
family history of MEN2B, it was decided that prophylactic TT was
necessary. Genetic testing identified an RET codon M918T mutation.
Postoperative histopathologic examination of the thyroid gland
revealed a small amount of MTC tissue. She exhibits no signs of
recurrence 21 months after surgery.
Discussion
MTC is a relatively rare type of thyroid malignancy
that arises from parafollicular C cells (1,11).
MTC may occur sporadically or may be inherited as a component of
MEN 2 syndrome (6,7). RET oncogenes were discovered by
Takahashi et al (12) in
1985. All patients with MEN 2 syndrome possess RET mutations. The
ATA classifies the risk according to the codon of the gene
mutation. Additionally, treatment recommendations are based on the
risk category (8). The RET codon
M918T mutation, which accounts for 95% of patients with MEN2B, is
classified in the highest risk category (4,5,8). TT
is recommended for all patients with resectable MTC without
evidence of distant metastases. In addition, prophylactic TT for
patients with MEN2B associated with RET codon M918T mutation is
recommended by the ATA guidelines, even in the first year of life,
as they are at high risk for MTC in the future (8).
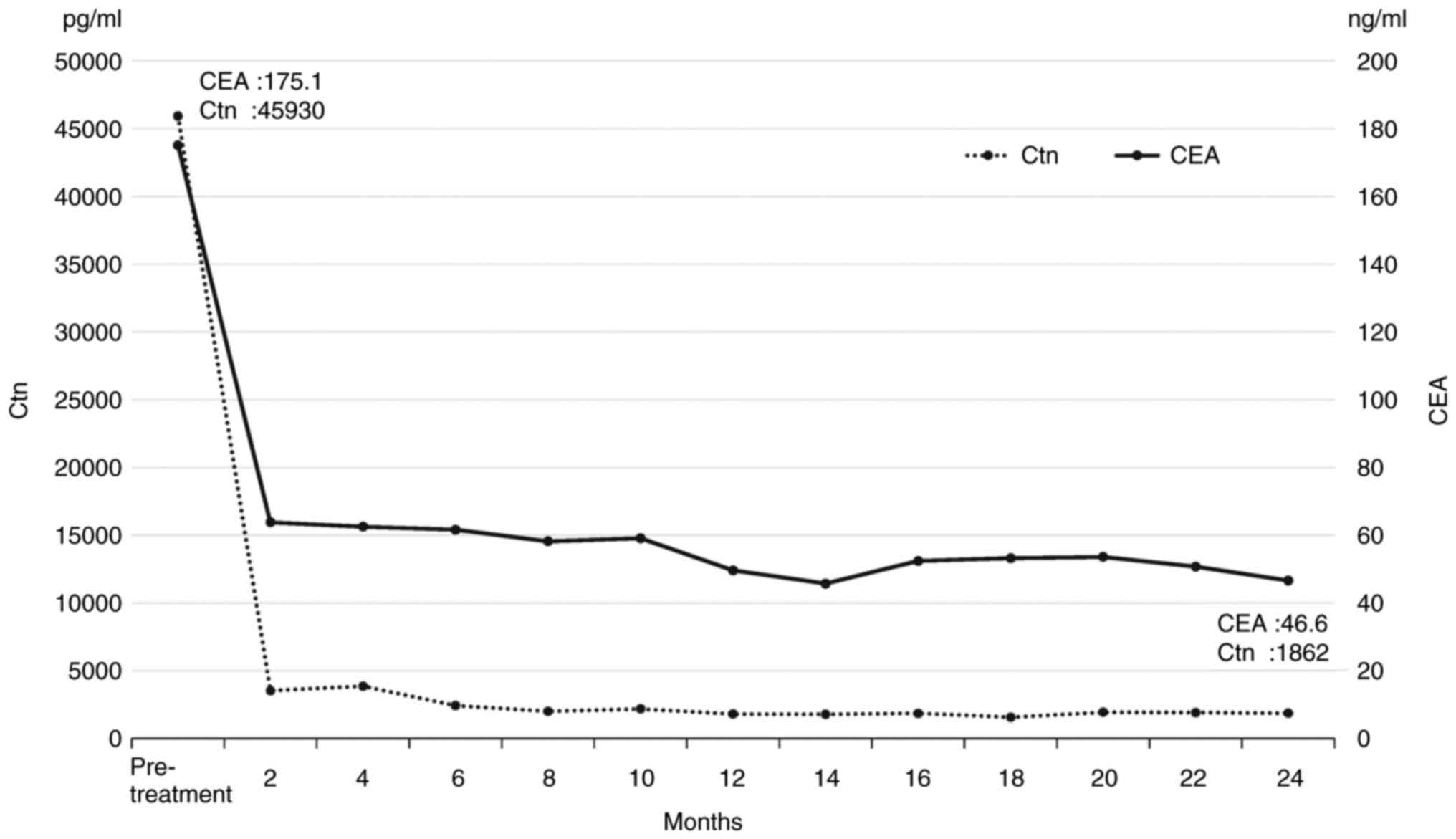
Although the patients in the present study responded
well to treatment, most patients with MTC associated with MEN2B are
diagnosed at an advanced state of the disease, as in Cases 1 and 3.
In Cases 1 and 3, the levels of Ctn and CEA decreased markedly
after their respective treatments (Figs. 3 and 4). The level of Ctn in Case 4 also
decreased after surgery although patients with MTC are likely to
maintain high Ctn levels after surgery (13).
In Japan, the treatment strategy for asymptomatic
MTC with MEN2B is still not standardized. This influenced our
treatment of Case 4, as the patient was asymptomatic but had the
gene mutation. We had to obtain approval from the ethics committee
and the director of our institution to perform prophylactic TT for
Case 4. Due to the lack of available local data, there is still no
consensus on the age group on which to perform prophylactic surgery
in Japan. In Case 4, postoperative histopathologic examination of
the thyroid gland revealed a small amount of MTC tissue and
prophylactic TT turned out to be significant.
The patient in Case 2 was not given adequate
information about her disease despite undergoing TT for MTC.
Therefore, genetic counseling and the lack thereof played an
especially important role in our cases. The mother faced difficulty
understanding the hereditary nature of their familial disease or
the necessity of genetic testing for her children. At first, she
was reluctant about genetic testing. However, she gradually
understood the significance of testing for RET germline mutations
through genetic counseling, which was performed by a
multidisciplinary team consisting of head and neck doctors, a
medical geneticist, oncologists, nurses and a genetic counselor.
Her consent to genetic testing was essential in detecting Cases 3
and 4. Follow-up genetic counseling is required whenever genetic
testing is conducted. In 2016, RET genetic testing for patients
with MTC received insurance coverage in Japan. However, RET
screening before clinical onset is not covered by insurance, even
if first-degree relatives have been diagnosed with hereditary MTC.
This may result in hesitation to genetic testing and a delay in
diagnosis.
In our cases, when the mother was diagnosed with
MTC-related MEN2B, there was still insufficient awareness of the
genetic characteristics of this disease. Considering this
background, the importance of family history and the need for
family screening are reaffirmed.
In conclusion, there is no consensus on the age to
perform prophylactic TT in Japan. In our case, prophylactic TT
prevented MTC from being detected in an advanced state. MEN2B
patients should be treated at the optimal time and appropriate
genetic counseling is essential in order to prevent delayed
diagnosis. We should be aware of the genetic characteristics of
MTC-related MEN2B and reaffirm the importance of family history and
the need for family screening.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AT made substantial contributions to conception and
acquisition of data and drafted the manuscript. AT, HU, CM, AN, YY
and IO were involved in obtaining the informed consent, literature
review, manuscript writing and patient management. TM and TK
provided cancer-related scientific inputs and critically revised
the manuscript. All authors have accepted responsibility for the
entire content of this manuscript and have approved its submission.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Nara Medical University Hospital and written informed
consent was obtained from the patients.
Patient consent for publication
Written informed consent was obtained from the
patients for the publication of this case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lim H, Devesa SS, Sosa JA, Check D and
Kitahara CM: Trends in thyroid cancer incidence and mortality in
the United States, 1974-2013. JAMA. 317:1338–1348. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Donis-Keller H, Dou S, Chi D, Carlson KM,
Toshima K, Lairmore TC, Howe JR, Moley JF, Goodfellow P and Wells
SA Jr: Mutations in the RET proto-oncogene are associated with MEN
2A and FMTC. Hum Mol Genet. 2:851–856. 1993.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mulligan LM, Kwok JB, Healey CS, Elsdon
MJ, Eng C, Gardner E, Love DR, Mole SE, Moore JK, Papi L, et al:
Germ-line mutations of the RET proto-oncogene in multiple endocrine
neoplasia type 2A. Nature. 363:458–460. 1993.PubMed/NCBI View
Article : Google Scholar
|
|
4
|
Carlson KM, Dou S, Chi D, Scavarda N,
Toshima K, Jackson CE, Wells SA Jr, Goodfellow PJ and Donis-Keller
H: Single missense mutation in the tyrosine kinase catalytic domain
of the RET protooncogene is associated with multiple endocrine
neoplasia type 2B. Proc Natl Acad Sci USA. 91:1579–1583.
1994.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hofstra RM, Landsvater RM, Ceccherini I,
Stulp RP, Stelwagen T, Luo Y, Pasini B, Höppener JW, van Amstel HK,
Romeo G, et al: A mutation in the RET proto-oncogene associated
with multiple endocrine neoplasia type 2B and sporadic medullary
thyroid carcinoma. Nature. 367:375–376. 1994.PubMed/NCBI View
Article : Google Scholar
|
|
6
|
Mulligan LM: 65 years of the double helix:
Exploiting insights on the RET receptor for personalized cancer
medicine. Endocr Relat Cancer. 25:T189–T200. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Eng C, Mulligan LM, Smith DP, Healey CS,
Frilling A, Raue F, Neumann HP, Pfragner R, Behmel A, Lorenzo MJ,
et al: Mutation of the RET protooncogene in sporadic medullary
thyroid carcinoma. Genes Chromosom Cancer. 12:209–212.
1995.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wells SA Jr, Asa SL, Dralle H, Elisei R,
Evans DB, Gagel RF, Lee N, Machens A, Moley JF, Pacini F, et al:
Revised American thyroid association guidelines for the management
of medullary thyroid carcinoma. Thyroid. 25:567–610.
2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Waguespack SG, Rich TA, Perrier ND,
Jimenez C and Cote GJ: Management of medullary thyroid carcinoma
and MEN2 syndromes in childhood. Nat Rev Endocrinol. 7:596–607.
2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bentley DR, Balasubramanian S, Swerdlow
HP, Smith GP, Milton J, Brown CG, Hall KP, Evers DJ, Barnes CL,
Bignell HR, et al: Accurate whole human genome sequencing using
reversible terminator chemistry. Nature. 456:53–59. 2008.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Williams ED: Histogenesis of medullary
carcinoma of the thyroid. J Clin Pathol. 19:114–118.
1966.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Takahashi M, Ritz J and Cooper GM:
Activation of a novel human transforming gene, ret, by DNA
rearrangement. Cell. 42:581–588. 1985.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Uchino S: Prognostic factors for medullary
thyroid cancer. J JAES JSTS. 36:158–164. 2019.
|