Introduction
Aggressive fibromatosis (AF) is a rare, benign
neoplasm with an incidence of 2 to 4 per 1 million individuals
annually. It originates from musculoaponeurotic stromal structures
and aggressively grows and infiltrates local tissues, principally
the connective tissue of the muscle and overlying fascia or
aponeurosis (1). More commonly, AF
occurs in the head and neck region, followed by the face, oral
cavity, scalp, paranasal sinus and orbit. Specifically, 10% of
reported AF cases appear in the cervical region and only six cases
have reported involvement of the larynx (2). Specifically, AF of the head and neck
region tends to be more locally aggressive, making complete
resection difficult (3). As a
result, AF has a high recurrence rate despite successful surgical
resection. Therefore, there is of interest whether chemoadjuvant
therapies may reduce cancer resection after surgical resection. The
current study presented a case of aggressive recurrent fibromatosis
involving the left anterior cervical neck along with the thyroid in
a 70-year-old female who underwent multiple neck resections.
Case report
A 70-year-old female patient (body mass index, 23.6
kg/m2) presented at the Otolaryngology Department Clinic
at Texas Tech University Health Science Center (Lubbock, USA) with
an approximately three-to-four-year history of an enlarging left
neck mass. The patient did not seek any treatment previously
because she was afraid of the possible diagnosis. She denied any
pain, dysphagia or dyspnea. The patient's most noticeable symptom
was a higher vocal pitch. The family history of the patient
included pneumonia in the father, hypothyroidism in the patient's
sister and prostate cancer in the patient's brother. On
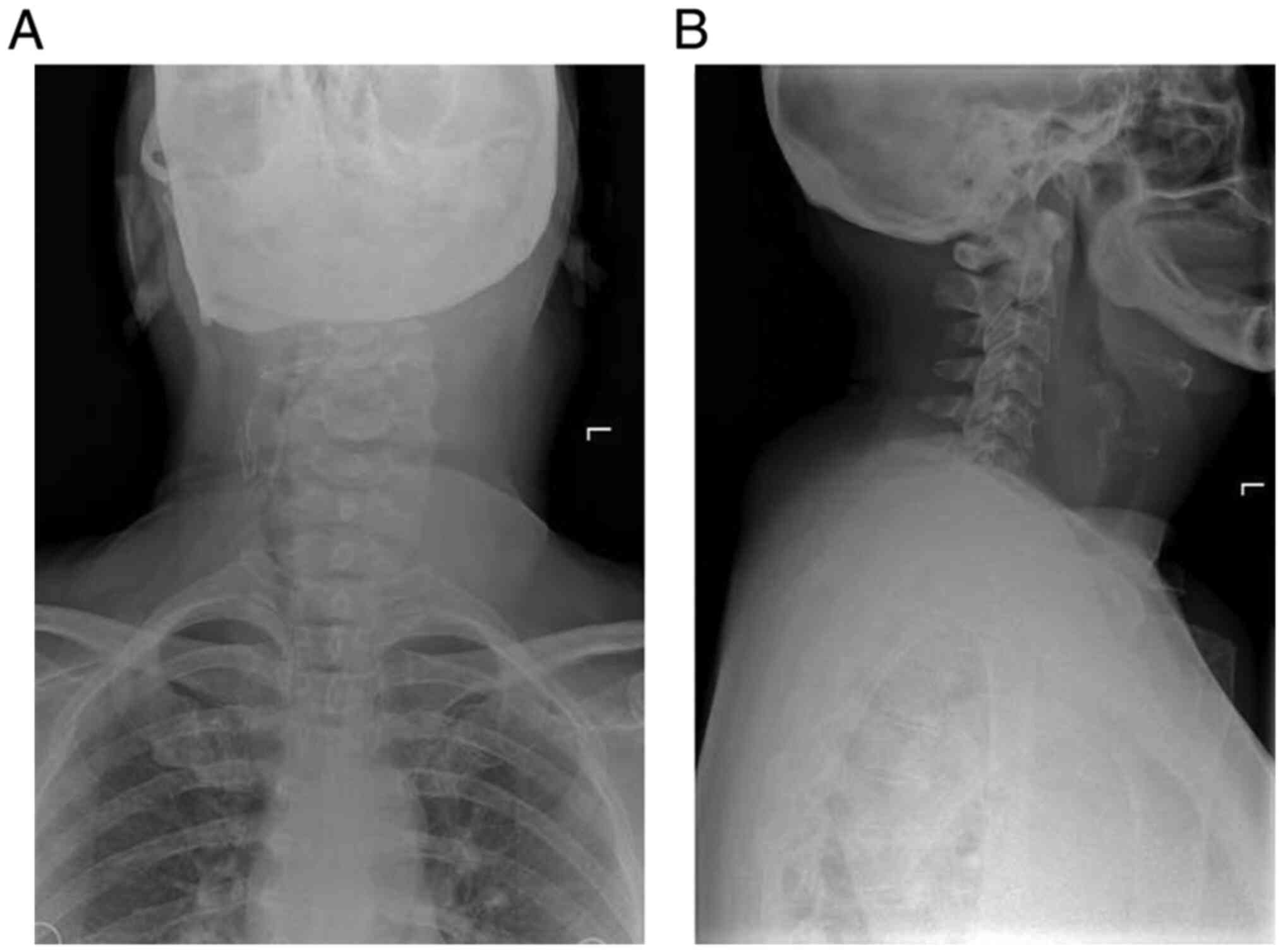
examination, an anterior displacement of the trachea at the C4-C5
level was detected. Upon further inspection, a fixed, firm
>10-cm mass with a superior boundary to the inferior portion of
the left mandible and an inferior boundary of the left thyroid
cartilage was noted. Anterior and lateral X-ray of the neck
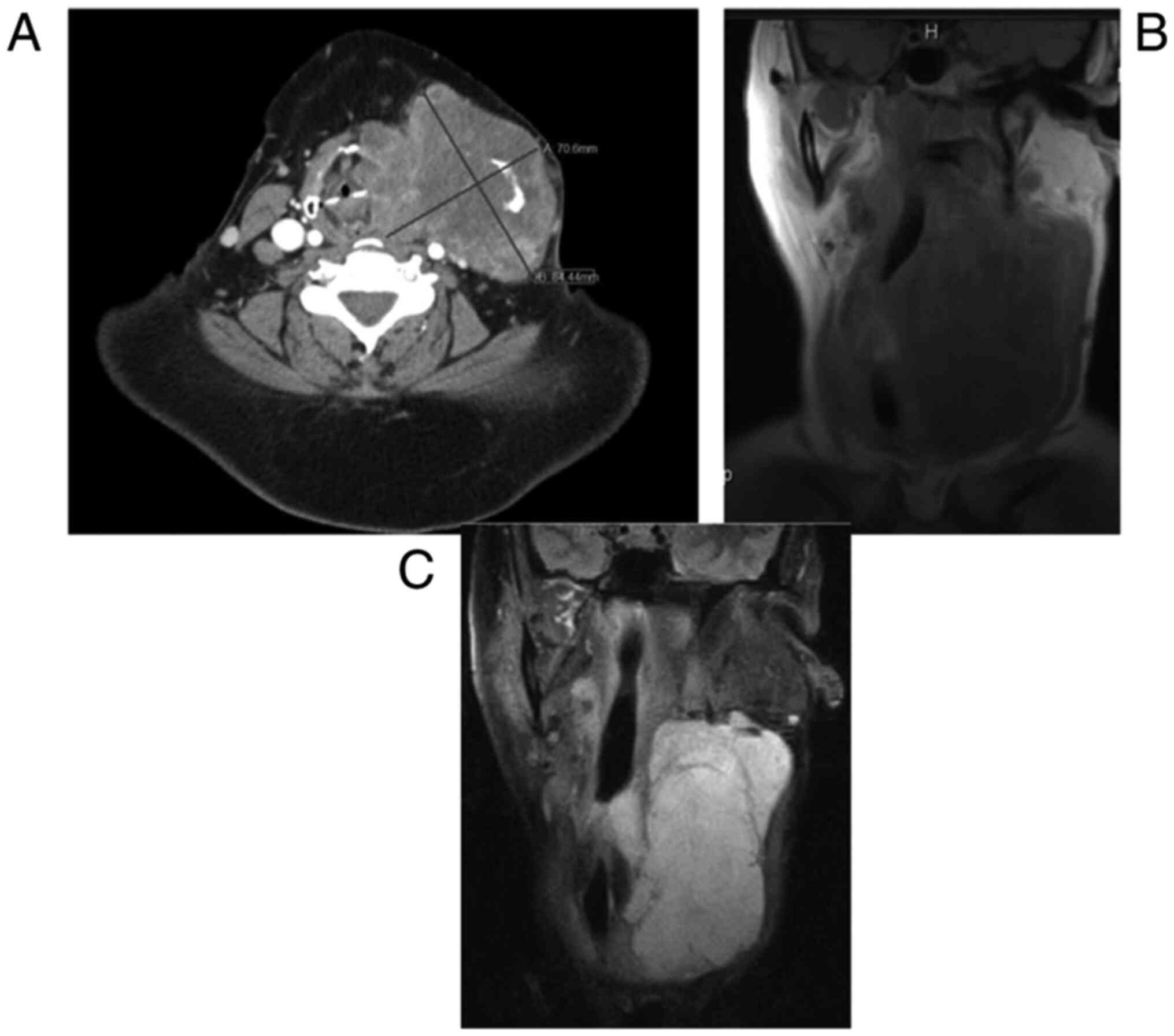
revealed a soft tissue mass on the neck (Fig. 1). MRI indicated a large, solid mass
measuring 10.8x7.5x9.7 cm, which expanded from the left anterior
cervical space displacing the trachea by 2-2.5 cm to the right
(Figs. 2 and 3). There was no involvement of any other
organs besides the larynx. Blood chemistry analysis was also
significant for leukopenia. The mass was inferior to the parotid
glands, invading medially and posteriorly to the trachea with
medial and inferior extension to the left lobe of the thyroid.
Histological analysis indicated an atypical and cellular spindle
cell neoplasm with low proliferative activity exhibiting fascicular
and storiform growth patterns. No necrosis was observed. A
diagnosis of a low-grade myofibroblastic sarcoma was made with a
pathological stage of rPT4aNxMx. Immunohistochemical analysis
indicated that the tumor was smooth muscle actin-positive,
SOX10-negative, desmin-negative, S100-negative, CD34-negative,
pancytokeratin-negative and β-catenin-negative. Genetic analysis of
the tumor suggested cyclin-dependent kinase 4 (CDK4) amplification,
erb-b2 receptor tyrosine kinase (ERBB3) amplification, MDM2
amplification, colony stimulating factor 3 receptor (CSF3R) G21R
mutation, FRS2 amplification, HMGA2-KERA fusion and RUNX family
transcription factor 1 (RUNX1) partner transcriptional co-repressor
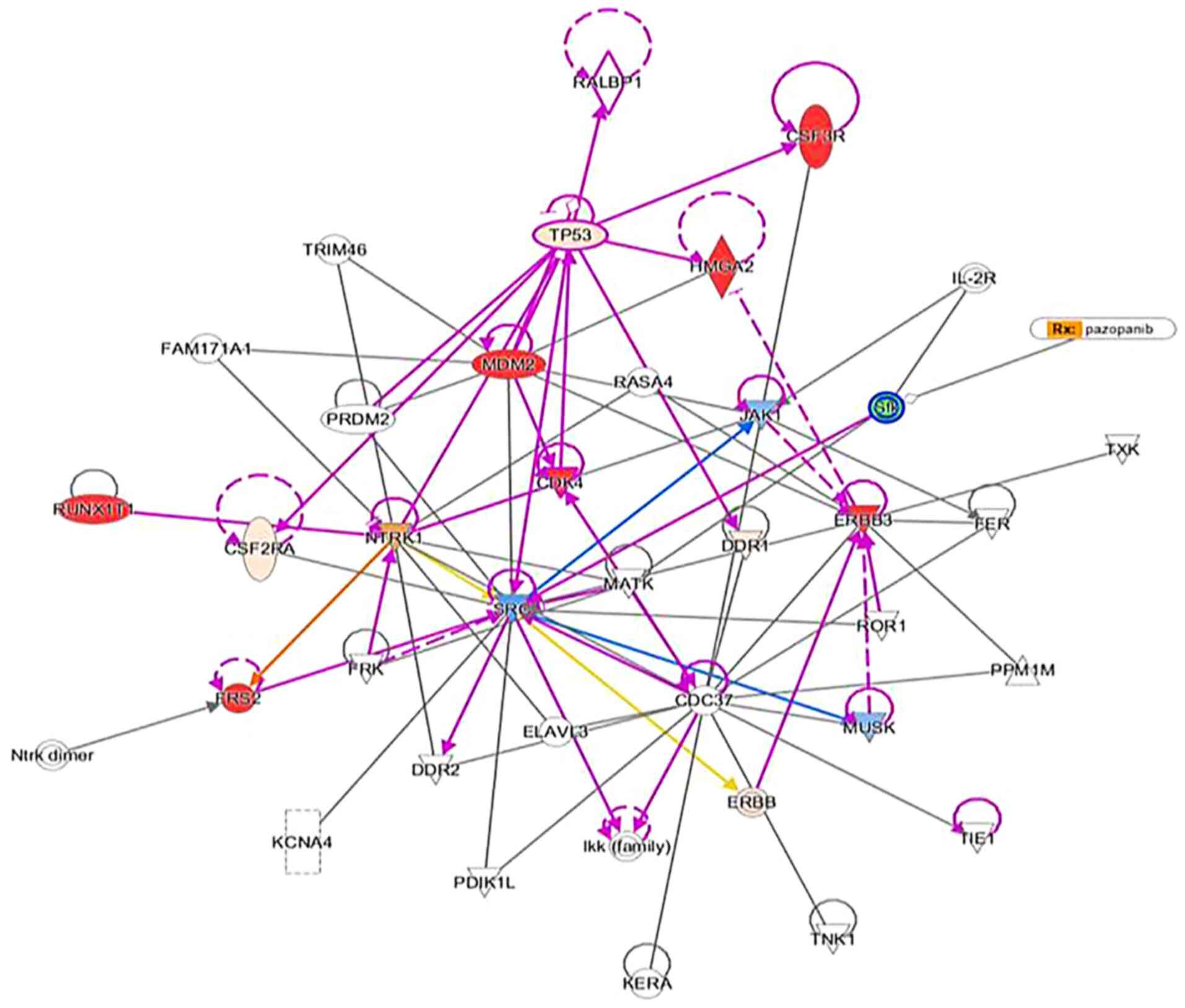
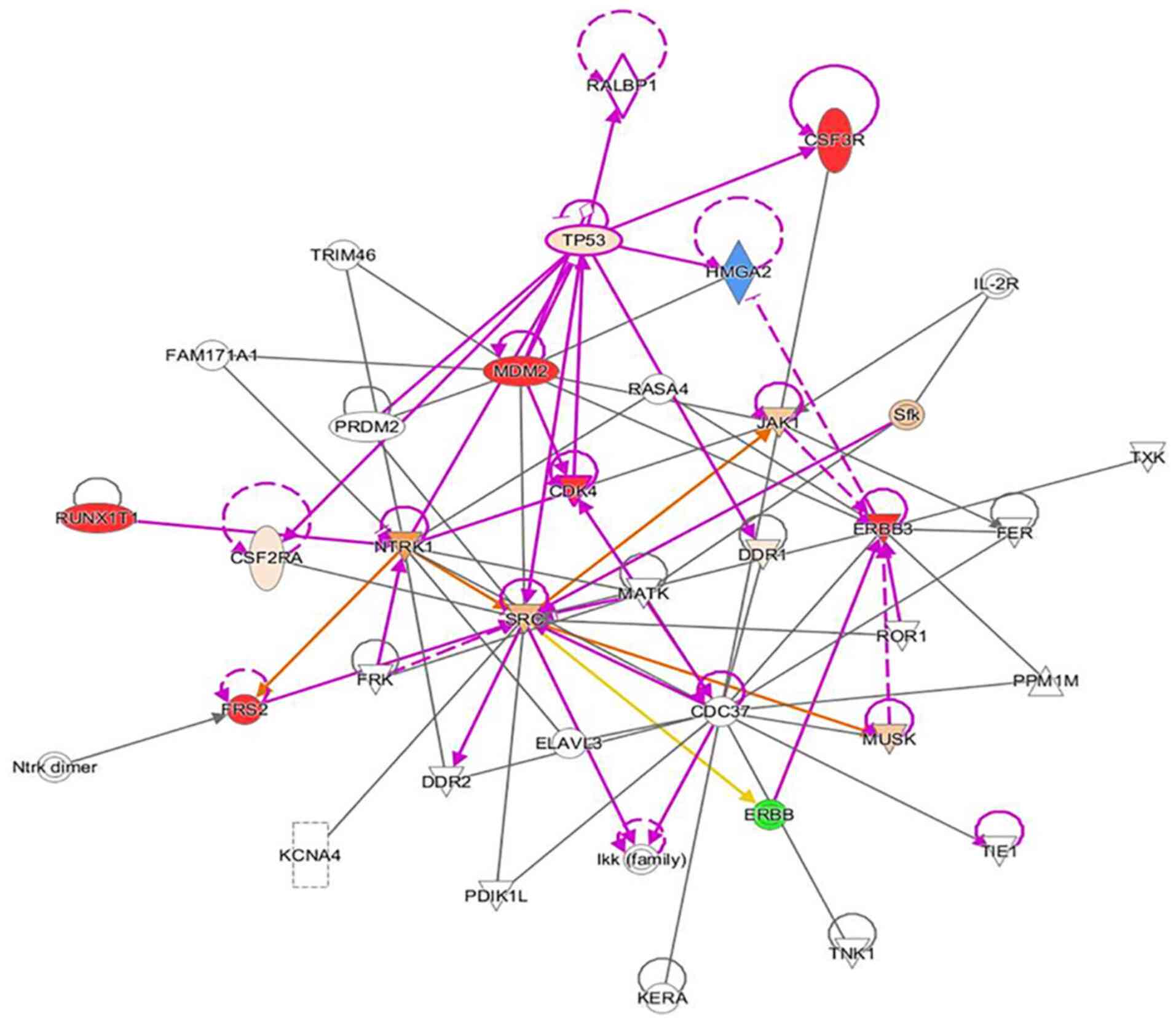
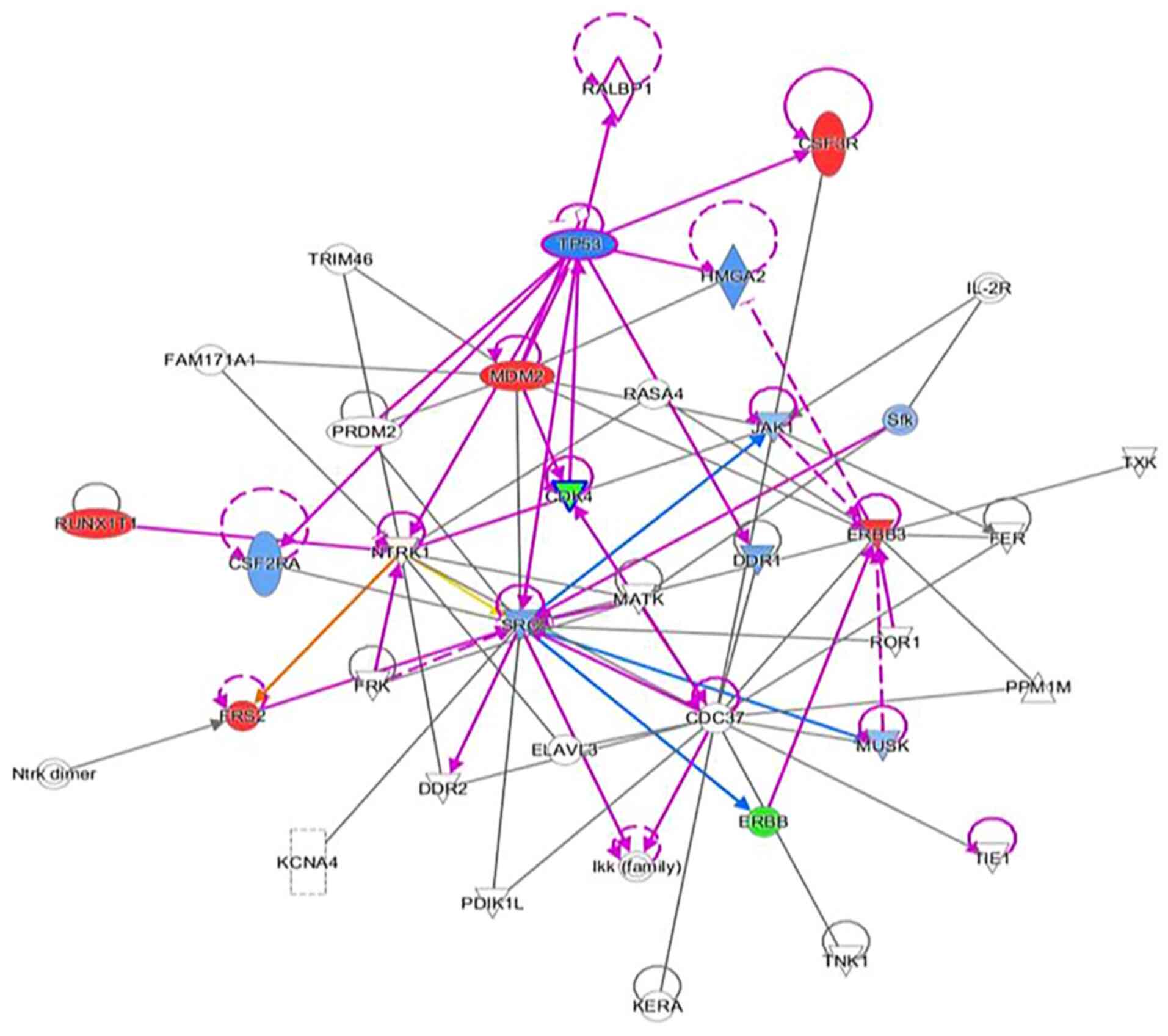
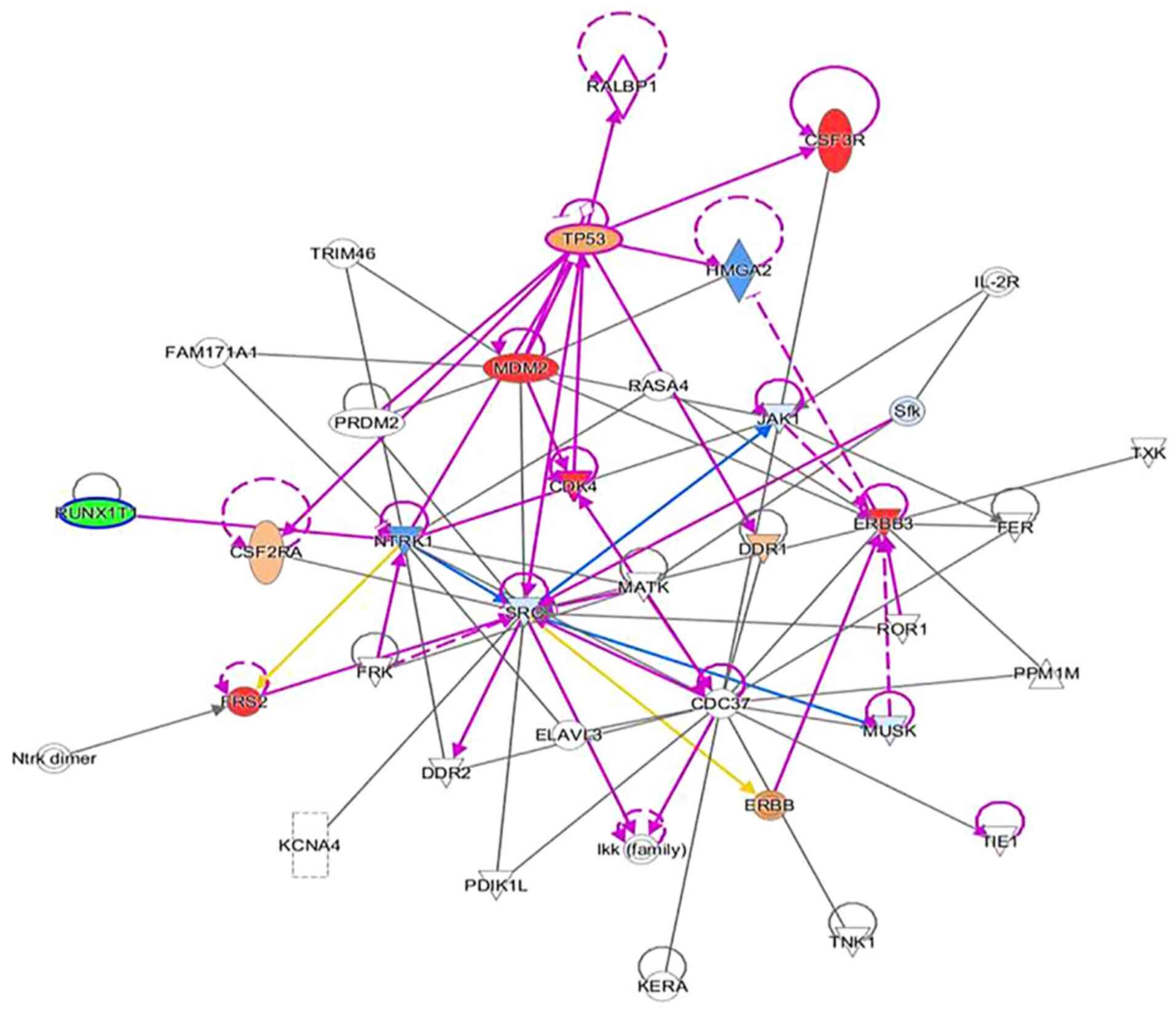
1 R373. An Ingenuity Pathway Analysis (IPA; Qiagen GmbH) was
performed using the aforementioned genetic analysis data in the
core IPA to develop an interactive network. The Qiagen IPA software
(Qiagen GmbH) was used to create the networks. The network was then
overlaid with a network activity predictor to determine the effects
of mutations on activating or de-activating proteins and/or
transcriptions factors in the interactive network. The analysis
suggested that these mutations affected numerous canonical
pathways, including regulation of epithelial-mesenchymal growth
factor pathways, Her-2 signaling, the BAG2 signaling pathway and
the p14 tumor suppressor. The resulting IPA images are presented in
Fig. 4, Fig. 5, Fig.
6 and Fig. 7.
The patient consented to surgery and the mass was
excised by left modified neck dissection through levels I-VI with
preservation of nerves, vessels and surrounding structures. The
mass was carefully removed from the carotid sheath, strap muscles,
anterior body of the thyroid and anterior trachea in succession.
The mass was noted to extend into both retro-pharyngeal and
retro-laryngeal spaces and was then removed posteriorly from the
posterior trachea, thyroid cartilage and thyroid. The dissection
was difficult due to aggressive local invasion; thus, clear margins
were not achieved. The mass was at least 12-15 cm in length, 10 cm
in width and 8 cm in height. It was sent for pathology, which
indicated spindle cell proliferation consistent with deep
fibromatosis with no clear margins. A post-operative CT scan with
contrast was performed 8 months after surgery and indicated
significant reduction of fibromatosis tissue in the left neck.
Another noteworthy finding included residual
fibromatosis tissue between the lower cricoid cartilage and the
medial aspect of the upper left thyroid lobe. At 15 months after
resection, the patient returned to the clinic with a new chief
complaint of left neck paresthesia with involvement of the left
ear. The patient mentioned that she had not been able to sing since
the operation. She confirmed hoarseness and dysphagia but denied
any change in pitch and dyspnea. On physical exam, a noticeable
mass of the left neck in the same location as the original mass was
present. On follow-up 5 months later, the mass had roughly doubled
in size. A CT with contrast indicated an 8.1x8.5x10.3 cm mass with
a superior border to the mandibular ramus and inferior border of
the left thyroid (Fig. 2).
Invasion of the left para-pharyngeal space, rightward deviation of
the airway and narrowing of the glottis was also noted on imaging.
The mass invaded deeper up to the lateral edge of the tonsil. And
into the left lateral margin of the tonsillar soft tissues and
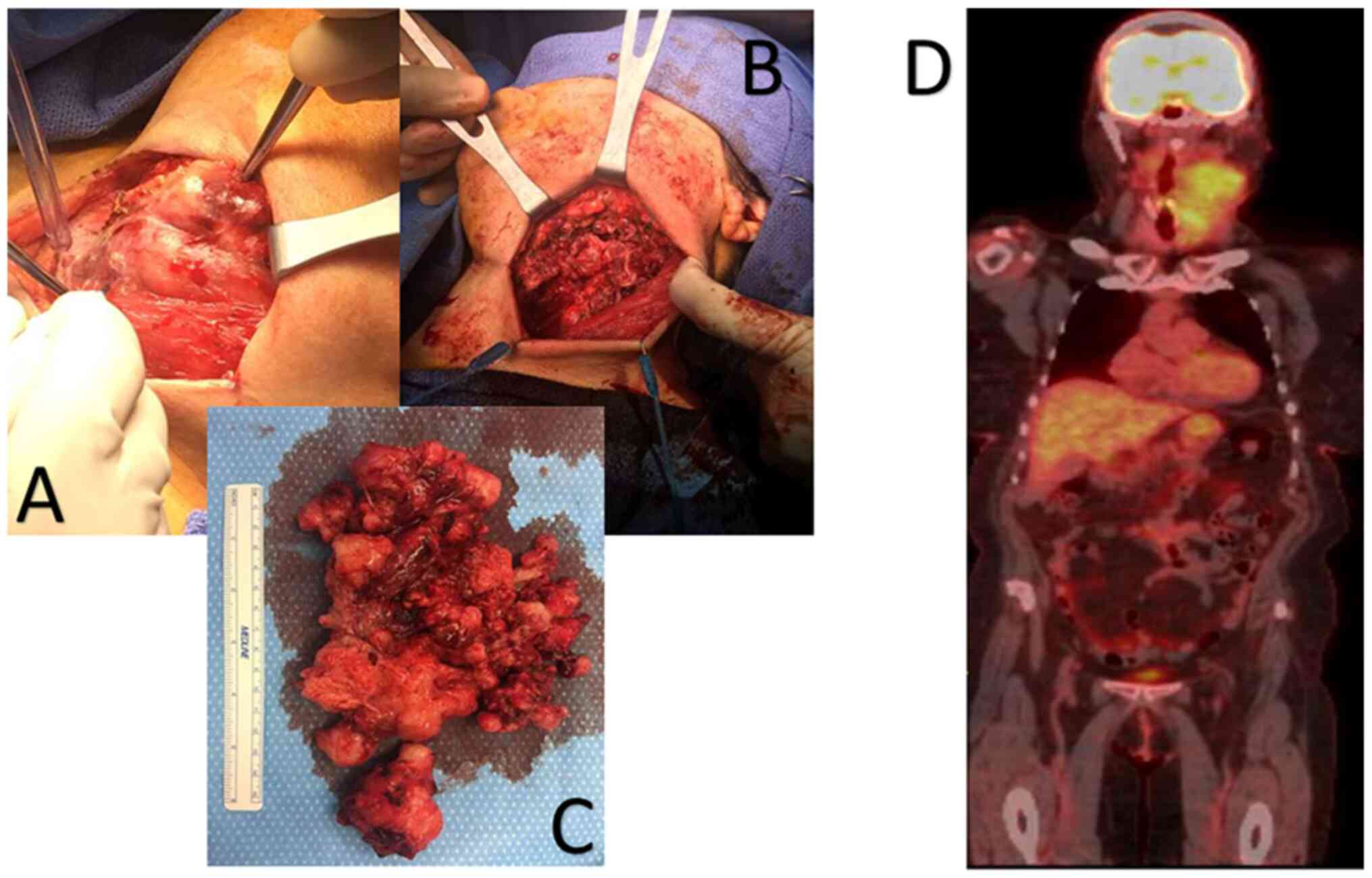
vallecula. The mass was resected ~21 months after the first
dissection (Fig. 4, Fig. 5, Fig.
6 and Fig. 7). Left radical
neck mass excision included levels II-IV, removing the mass from
the left thyroid bed, left carotid sheath, left parotid bed and
left posterior digastric muscle after careful mobilization of the
sternocleidomastoid muscle. Erosion of the left thyroid cartilage
into the pharynx was noted but the hyoid bone was left intact.
After resection, radiation oncology was consulted for possible
local radiation treatment to prevent tumor recurrence. A positron
emission tomography scan using 15.97 mCi of 18-fluoro
2-deoxyglucose indicated a hypermetabolic mass extending inferiorly
from the top of the left side of the thyroid and deviating and
possibly invading the larynx, which is consistent with known
primary malignancy (Fig. 8). The
patient was subsequently given a total dose of 6,600 cGy of
radiation in 33 fractions to her left neck and supraclavicular
area. The patient developed a minor skin reaction and hoarseness in
response to the radiation therapy but otherwise tolerated it well.
After radiation therapy, remnants of the sarcoma still remained in
the left neck. As presented in Fig.
4, Fig. 5, Fig. 6 and Fig. 7, an IPA analysis was performed to
determine which chemotherapy regimens would be most effective at
eliminating the sarcoma. The network suggested that pazopanib would
be a possible chemotherapeutic agent against AF by inhibiting the
actions of SRC proto-oncogene and megakaryocyte-associated tyrosine
kinase. According to the network analysis and activity predictors
of mutated proteins (i.e. whether a given mutation increases or
decreases the activity of a protein), the patient was subsequently
prescribed 800 mg/day of pazopanib, which is a tyrosine kinase
inhibitor for the treatment for advanced/metastatic renal cell
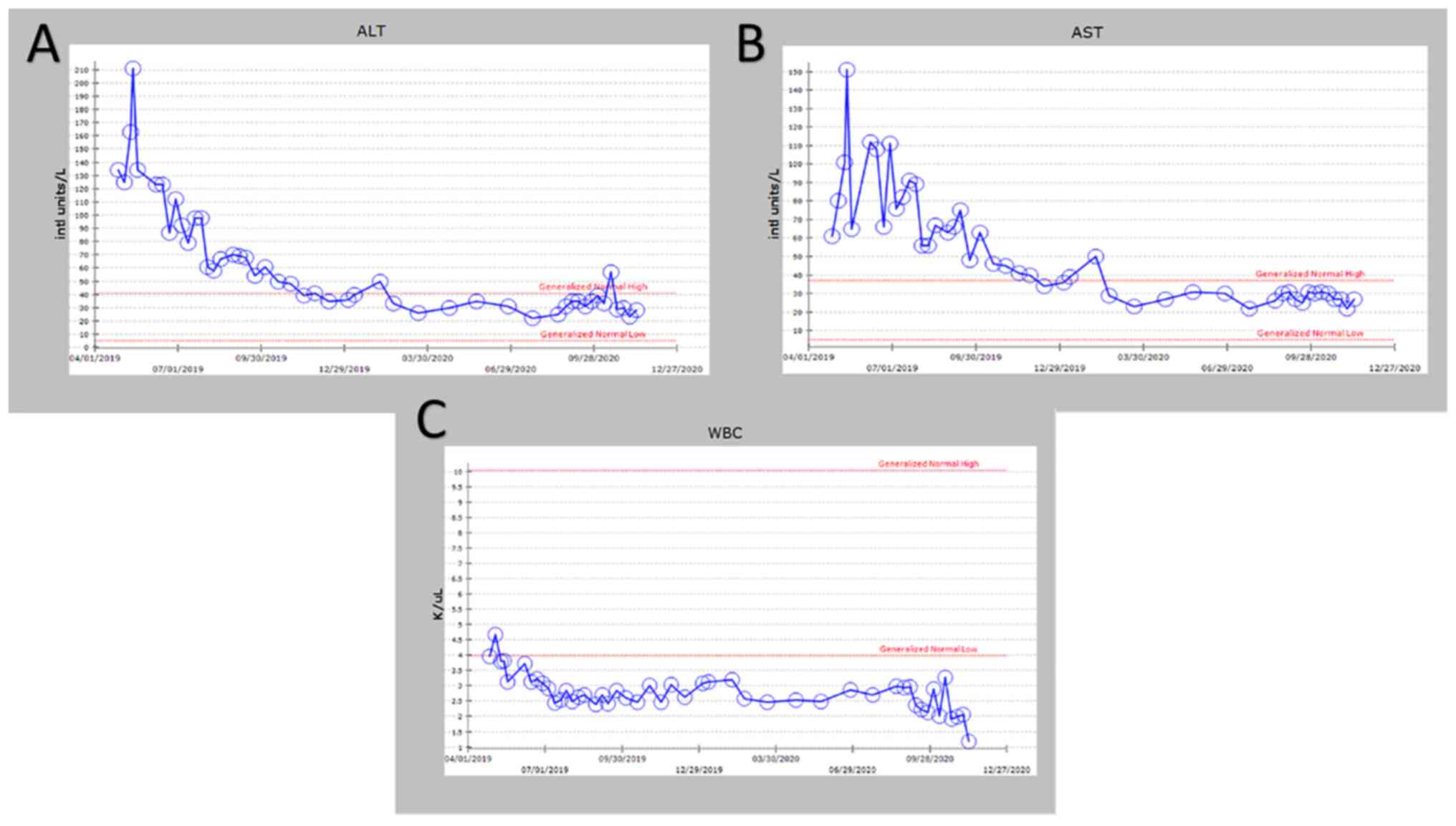
carcinoma and advanced soft tissue sarcomas. However, the patient
developed elevated liver enzymes (alanine aminotransferase and
aspartate aminotransferase >200 U/l) and mild hepatomegaly as
indicated by abdominal ultrasound. The course of liver enzymes and
white blood cell counts are presented in Fig. 8. Pazopanib was subsequently
titrated down to 200 mg/day, which reverted the liver enzyme levels
back to normal levels. During the course of chemotherapy, the
patient lost a total of 25 pounds in total body weight. The neck
mass continued to reduce in size. The patient denied any changes in
appetite, dysphagia or hoarseness. The dose of pazopanib was
subsequently increased to 800 mg/day without any further
complications. The mass continued to decrease in size. Since the
surgery two years ago and one year since chemotherapy ended, the
patient is continuing to do well without any further growth of the
primary tumor.
Discussion
AF is a benign, mesenchymal lesion composed of a
proliferation of well-differentiated fibroblasts (1-4).
The majority (two-thirds) of AF cases develop in the abdomen, while
the remainder are found extra-abdominally (3). Specifically, 19-49% of AF cases are
preceded by nonsurgical or surgical trauma. It is hypothesized that
the pathogenesis involves an abnormal healing response with
proliferation of immature fibroblasts, leading to a fibromatosis
tumor (3). Aggressive fibromatosis
of the head and neck regions are more aggressive variants of
fibromatosis; they tend to be locally aggressive and have been
known to erode bone, soft tissues and vital structures (3). As observed in the patient of the
present study, clinical features, such as paraesthesia and weakness
of the voice and hoarseness, occur because of pressure effects on
local nerves and vascular structures (3). After treatment, these tumors have a
high tendency to recur (40-70%) with most cases recurring within 18
months of surgical excision (3),
which was also observed in the present case. At present, the
literature available to guide the treatment of wide local invasive
AF is sparse. Treatment modalities include surgery, chemotherapy,
radiotherapy, hormonal therapy or combinations thereof (1). The choice of treatment modality
predominantly depends on the tumor location, tumor size, age of the
patient and tumor profile (5).
Given that the patient's AF had multiple mutations of unknown
significance, the choice of the best initial chemotherapy agent for
treating the AF was not obvious. Therefore, an IPA analysis was
performed to determine potential chemotherapy agents that may be
most effective. For the analysis, all amplification mutations were
assumed to be gain-of-function mutations. In the IPA network for
this patient's AF, the SRC protein was the central node for all the
proteins and transcriptions factor interactions. Among the
chemotherapy agents tested (pazopanib, ERBB, CDK4 and RUNX1
inhibitors), pazopanib was the only chemotherapy agent that was
predicted to directly inhibit the activity of SRC. Pazopanib was
started and dosed intermittently, and dosing was paused or reduced
upon worsening of liver enzymes or the white blood cell count. The
maximum response was seen within 6 months and subsequently, stable
thickening of the neck persisted due to both residual disease and
scarring resulting from treatment. At present, the patient remains
on 800 mg of pazopanib and is stable. If the tumor continues to
recur after treatment with pazopanib, other chemotherapeutic agents
will be screened using IPA analysis or repeat biopsies to interfere
with tumor recurrence. At present, the standard treatment for head
and neck AF is primary surgical excision with clear margins to
minimize the chance of recurrence. However, the recurrence rate of
AF is independent of the surgical margin status (1). Positive margins do not affect the
overall survival rate or 5-year disease-free survival, making
standard treatment with clear margins controversial (1). The few cases of AF that involve the
larynx have been treated using a total or hemi-laryngectomy
(2). The majority of reported
cases (66%) treated by hemi-laryngectomy and other less radical
surgical interventions experienced recurrence of the primary tumor;
of those that recurred in the larynx, 75% were treated by
laryngectomy (2). Other treatment
modalities, such as radiotherapy, appear to reduce local recurrence
rates of AF in adults. However, 40% of patients suffered from
severe complications, including pathologic fracture, pain,
contracture, impaired range of motion and skin cancer (1). Chemotherapy regimens, including
Vinblastine and Methotrexate, have lowered recurrence rates in
pediatric patients (1). The
decision regarding treatment regimens for patients with AF of the
head and neck is best made by a multidisciplinary team, consisting
of otolaryngologists, radiation oncologists and medical
oncologists. These multidisciplinary teams have been indicated to
improve decision-making and reduce waiting times for cancer
patients (6). Regardless of the
treatment modality applied, close follow-up and high suspicion of
recurrence are necessary.
Controversy over treatment and management of AF in
the head and neck region still exists. A minimal amount of
literature on the topic is currently available, with even less
available to guide the cases that involve the larynx. Case reports
in the literature agree that surgery is the best treatment option
but a consensus regarding the management of tumor recurrence has
not been reached. Treatment and management, due to the lack of
evidence in the literature, should be tailored to each individual
patient and education of the risks and benefits of treatment
modalities should be emphasized, since no treatment, even surgery
with clear margins, guarantees prevention of recurrence. The use of
multidisciplinary teams may improve decision making for these
patients. The treatment of AF in the head and neck region is a
topic that requires more attention and research. In the present
case report, it was assumed that amplification mutations activated
the proteins or transcription factors; further scientific analysis
would be required to confirm this assumption. In general, sarcomas
have more copy number alterations (amplifications, deletions,
translocations) than point mutations, which makes choosing
therapeutic targets difficult. Furthermore, numerous copy number
alterations are unknown with respect to their effect on activating
or deactivating proteins involved with critical functions in
cellular metabolism, growth or cell cycle control (7,8).
Therefore, the use of IPA may provide an alternative method for
determining chemotherapy agents to use for the treatment of
difficult or rare tumors with genetic variants of unknown
significance. In the present study, pazopanib was determined as an
alternative chemotherapy regimen using the IPA analysis software
and applied for treating the patient.
Administration of pazopanib is contraindicated for
patients with severe hepatic impairment due to reports of severe or
fatal hepatoxicity in clinical trials (9). The Food and Drug Administration (FDA)
recommends monitoring hepatic function and to pause, reduce or
discontinue dosing as indicated (9). Specifically, upon any indication of
hepatotoxicity, the dose should be reduced to 200 mg/day. The
patient of the present study did not have any hepatic impairment.
The FDA recommendations were followed and the dose of pazopanib was
reduced to determine whether the increase in liver function tests
(LFTs) was due to tumor breakdown or hepatic impairment. As was
demonstrated, the patient's LFTs did not increase after the dose of
pazopanib was increased to 800 mg/day. Therefore, caution should be
taken to completely withdraw a patient from pazopanib prior to
reducing the dose and increasing it again to determine whether LFTs
increase.
The current case report presented a rare and
difficult to treat AF tumor for which therapeutic management has
not been established. It was also demonstrated that even large
tumors may be resected and there is a benefit even if a positive
margin recurs through tumor burden reduction. Through the
interactive network from IPA, pazopanib was theoretically predicted
to be a potential treatment for this patient's AF. Pazopanib or
Votrient is an FDA-approved tyrosine kinase inhibitor used in
patients with advanced renal cell carcinoma or advanced soft tissue
sarcoma who have received prior chemotherapy (9). Specifically, pazopanib is a
multi-tyrosine kinase inhibitor of vascular endothelial growth
factor receptor-1, -2 and -3, platelet-derived growth factor
receptor-α and -β, fibroblast growth factor receptor-1 and -3,
cytokine receptor, interleukin-2 receptor inducible T-cell kinase,
leukocyte-specific protein tyrosine kinase and transmembrane
glycoprotein receptor tyrosine kinase (9). Pazopanib is given once daily at 200
or 800 mg/day depending on whether the patient has moderate renal
or hepatic impairment. As demonstrated in the present case report,
pazopanib may be an effective chemotherapy regimen in the treatment
of aggressive AF.
Acknowledgements
Not applicable.
Funding
Funding: No funding was obtained.
Availability of data and materials
The data that support the findings of this study are
available from the corresponding author upon reasonable
request.
Authors' contributions
NL wrote the initial draft of the manuscript and was
involved in the initial conception of the case report. JK
contributed to the conception and the design of the study and
contributed to the acquisition, analysis and interpretation of the
data. SA edited the manuscript and performed the IPA analysis. JC
reviewed the study for important intellectual content. All authors
read and approved the final manuscript. JC and SA checked and
approved the authenticity of the clinical and raw data used for the
IPA analysis.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of their data and images in this case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wang W, Koirala U, Ma S, Liu G, Ding M, Hu
X and Lei D: Age-based treatment of aggressive fibromatosis in the
head and neck region. J Oral Maxillofac Surg. 72:311–321.
2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Shinohara S, Suehiro A, Kikuchi M, Harada
H, Kishimoto I and Imai Y: A case of desmoid tumor co-existing with
recurrent squamous cell carcinoma in the larynx. Auris Nasus
Larynx. 44:365–369. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Prabhu R, Natarajan A, Shenoy R and Vaidya
K: Aggressive fibromatosis (desmoid tumour) of the head and neck: A
benign neoplasm with high recurrence. BMJ Case Rep.
2013(bcr2013200156)2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Simões-Pereira J, Cabrera RA and Leite V:
A case of thyroid fibromatosis, a rare lesion of this gland.
Endocrinol Diabetes Metab Case Rep. 2016:16–0019. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Salas S, Dufresne A, Bui B, Blay JY,
Terrier P, Ranchere-Vince D, Bonvalot S, Stoeckle E, Guillou L, Le
Cesne A, et al: Prognostic factors influencing progression-free
survival determined from a series of sporadic desmoid tumors: A
wait-and-see policy according to tumor presentation. J Clin Oncol.
29:3553–3558. 2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Specchia ML, Frisicale EM, Carini E, Di
Pilla A, Cappa D, Barbara A, Ricciardi W and Damiani G: The impact
of tumor board on cancer care: Evidence from an umbrella review.
BMC Health Serv Res. 20(73)2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Cheng L, Pandya PH, Liu E, Chandra P, Wang
L, Murray ME, Carter J, Ferguson M, Saadatzadeh MR,
Bijangi-Visheshsaraei K, et al: Integration of genomic copy number
variations and chemotherapy-response biomarkers in pediatric
sarcoma. BMC Med Genomics. 12 (Suppl 1):23:2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Cancer Genome Atlas Research Network:
Electronic address: simpleelizabeth.demicco@sinaihealthsystem.ca
and Cancer Genome Atlas Research Network. Comprehensive and
integrated genomic characterization of adult soft tissue sarcomas.
Cell. 171:950–965. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Highlights of Prescribing Information -
Votrient (pazopanib) tablets (2009). White Oak, Maryland: Food and
Drug Admini-stration. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/022465s021lbl.pdf.
|