Introduction
The fibula is a rare site of primary bone tumour;
the most common location for both benign (58.3%) and malignant
(71.4%) tumours is the proximal fibula (1). Approximately half of all tumours are
malignant, with osteosarcoma, Ewing sarcoma and giant cell bone
tumour being the most common, the incidence of osteosarcoma and
giant cell tumour in the proximal fibula was 2.3 and 2.8-8%
respectively (2). The incidences
of osteosarcoma and giant cell tumour in the proximal fibula are
2.3 and 2.8-8%, respectively. The main clinical manifestations are
pain, common peroneal nerve palsy and swelling (3,4). The
proximal fibular cortex is thinner and has more muscles and
ligaments attached; these anatomical features lead to a higher
probability of proximal fibular malignancy invading the surrounding
soft tissue and developing into an extraosseous compartment tumour
(5).
The bone cortex at the proximal end of the fibula is
relatively thin, and the tumour can easily break through the bone
cortex and invade the muscle. Most patients have been found in
Enneking stage IIB; therefore, when selecting limb salvage surgery,
sufficient surgical boundaries should be identified to obtain good
oncological results (4,6). There is no unified surgical plan for
fibular proximal malignant tumours, and proximal fibula tumours are
usually treated with limb salvage surgery for extensive or radical
resection (2). However, the
proximal fibula is adjacent to the common peroneal nerve, the
anterior tibial artery and ligaments of the knee joint; therefore,
complications such as knee instability, tumour recurrence, peroneal
nerve paralysis and arterial dysfunction may occur after tumour
resection (6).
The present study retrospectively analysed the data
of patients with primary malignant and invasive tumours in the
proximal fibula and discussed the postoperative oncological
results, complications and postoperative functions of resection
operation.
Materials and methods
Patients
Between October 2005 and October 2019, 19 patients
(12 male, 7 female; age range, 8-62 years; average age 25.58) with
primary malignant or invasive tumours of the proximal fibula
received limb salvage treatment at Union Hospital, Tongji Medical
College, Huazhong University of Science and Technology (Wuhan,
China). The inclusion criteria were as follows: i) Fibular proximal
tumour, ii) pathological diagnosis of primary malignant or invasive
tumour, iii) complete resection adopted, iv) a follow-up time >6
months, and v) complete imaging data. The exclusion criteria were
as follows: i) Benign or metastatic tumours, ii) amputation or
intracapsular curettage as the first surgical procedure, iii)
patients lost to follow-up, and iv) follow-up time <6
months.
According to the pathological classification, there
were 10 cases of osteosarcoma, 3 cases of chondrosarcoma, 2 cases
of invasive giant cell tumour of osteosarcoma, 1 case of
epithelioid sarcoma, 1 case of leiomyosarcoma, 1 case of
fibrosarcoma and 1 case of lymphoma. All patients were initially
diagnosed and treated in our hospital, and pre-operative puncture
biopsy confirmed the pathological diagnosis. All patients were
eligible for limb salvage surgery, and 10 patients received 2
cycles of pre-operative and 4 cycles of postoperative neoadjuvant
chemotherapy.
Detailed medical history was collected. Physical
examination was conducted carefully, and imaging examinations,
including X-ray, CT, MRI, computed tomography angiography and
emission computed tomography, were performed; positron emission
tomography-CT) examination was performed when necessary. Enneking
staging was performed for fibular tumours to assess the degree of
malignancy and whether there was a breakthrough in the compartment
(7). Attention was also paid to
the relationship between the tumour and the surrounding tissue
structures (e.g., nerves, blood vessels and tibia). For
pre-operative C-arm guided puncture biopsy, the biopsy channel was
the shortest distance from the lesion to the skin and avoided major
nerve or blood vessel damage, particularly the common peroneal
nerve.
All excised tumour specimens were fixed in 10%
buffered-formalin for 24 h at 25˚C, embedded in paraffin and cut
into 4-µm-thick sections. Haematoxylin and eosin (H&E) staining
was performed for 20 min at 37˚C and the sections were observed
using an Olympus BX51 light microscope (magnification, x100;
Olympus Corporation).
Treatment
According to the Enneking stage, stage IB was found
in 2 cases, stage IIA in 2 cases and stage IIB in 15 cases. Malawer
I and II resection operations were performed in 3 and 16 cases,
respectively. After successful general anaesthesia, the patients
were placed in a semi-supine position with the affected limb
elevated by 45˚. According to the Malawer I excision method
(8), a longitudinal incision was
made, and the proximal fibula along with 2-3 cm of normal diaphysis
were removed. Simultaneously, a complete excision of the thin
muscle sleeve around the perimeter, including the insertion of the
lateral collateral ligament, was conducted. The common peroneal
nerve and its motor nerve branches were preserved. Finally, the
upper tibiofibular joint was excised through the capsular joint.
Using the ditto incision for Malawer II excision, the resected
proximal fibular tumour and its distal 2-3 cm normal diaphysis, the
lateral muscle septum, common peroneal nerve and anterior tibial
artery were excised (8). The
superior tibiofibular joint was excised laterally through the knee
joint. Gastrocnemius muscle flap transposition was required to
repair the defect after tumour resection. The incision included the
previous biopsy channel and 2-3 cm of the tissue at the edge.
During surgical excision, the continuity of the biceps femoris
tendon and lateral collateral ligament, as well as the continuity
of the lateral deep fascia and the iliotibial band, were retained
as much as possible. Using the rivet and non-absorbable nylon
thread, the biceps femoris tendon and the insertion point of the
lateral collateral ligament were closely sutured through the
perforation of the lateral tibial condylar cortex. Small holes were
made in the lateral cortex of the tibial condyle, the rivet and
non-absorbable nylon suture were used to reconstruct the insertion
point of the biceps femoris and lateral collateral ligament.
Patients with Malawer I resection underwent
rehabilitation exercises of knee flexion and extension at 3 weeks
post-surgery, whereas patients with Malawer II resection had to
delay exercise for 2-3 weeks. Foot sagging was caused by common
peroneal nerve resection. Ankle braces were used to assist walking
exercise at 6 weeks post-surgery.
Postoperative follow-up
Postoperative re-examination was conducted to
determine tumour recurrence, metastasis, complications and
postoperative limb function. The Musculoskeletal Tumour Society
(MSTS) functional score was used to evaluate lower limb extremity
function, with a total score of 30 and a high score indicating good
affected limb function (9). The
Chinese version of the Lysholm knee score (LKS) was used to assess
the knee function of patients, with a total score of 100 and a high
score indicating good function of the affected knee (10). The evaluation of knee stability was
mainly based on patient self-assessment and the medial stress test.
X-ray examination was performed under the medial stress of knee
flexion at 30˚; compared with the healthy side, an increase of
>5 mm in the affected side knee joint was considered unstable
(11).
This study was designed as a single-centre
retrospective study in Union Hospital, Tongji Medical College,
Huazhong University of Science and Technology and conducted in line
with The Declaration of Helsinki. The surgical procedure and data
collection were approved by the Huazhong University of Science and
Technology Committee on Human Research (2019-IEC-S274).
Results
The basic information of the patients is listed in
Table I; according to pathological
classification, there were 10 osteosarcoma cases, 3 chondrosarcoma
cases, 2 invasive giant cell osteosarcoma tumour cases, 1
epithelioid sarcoma case, 1 leiomyosarcoma case, 1 fibrosarcoma
case and 1 lymphoma case. According to the Enneking classification,
IB stage was found in 2 cases, IIA in 2 cases and IIB in 15 cases.
The indicators of treatment modalities and prognostic follow-up are
listed in Table II; a total of 3
patients underwent Malawer I resection, and 16 patients underwent
Malawer II resection. The follow-up time was 11-174 months, with an
average of 76.58 months. None of the patients had incision
infection or skin necrosis; however, there were two patients with
common peroneal nerve injury. Local recurrence occurred in three
patients (two with osteosarcoma and one with leiomyosarcoma); all
three patients underwent Malawer I resection. In addition, one
patient underwent amputation, one patient underwent extensive
resection and one patient underwent local radiotherapy. Seven
patients developed pulmonary metastasis, of which four of these
patients succumbed. After the resection of proximal fibula primary
and invasive tumours, the biceps femoris tendon and lateral
collateral ligament insertion point was reconstructed. After the
reconstruction of the biceps femoris tendon and lateral collateral
ligament, knee joint function was stable in all but one patient who
reported self-perceived instability of the knee joint. The MSTS
score at the last postoperative follow-up was 23-29 points, with an
average of 27.26 points (90.87%; postoperative MSTS score divided
by total MSTS score). The LKS was 65-84 points, with an average of
83 points. Most patients experienced pain relief and their daily
life was not affected. Patients with permanent common peroneal
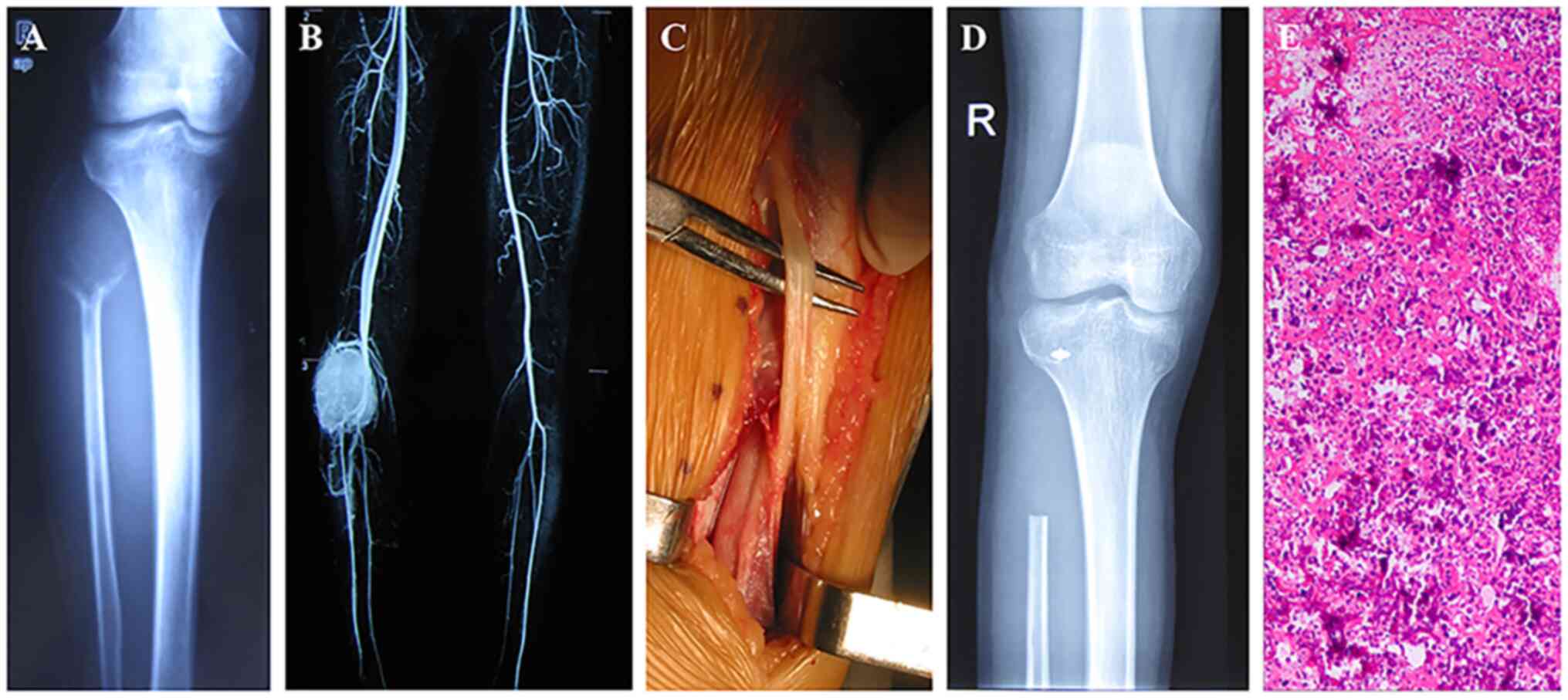
nerve palsy needed to wear braces to walk after surgery. Two
typical cases are presented in the figures, including an invasive
giant cell tumour of the proximal right fibula treated with Malawer
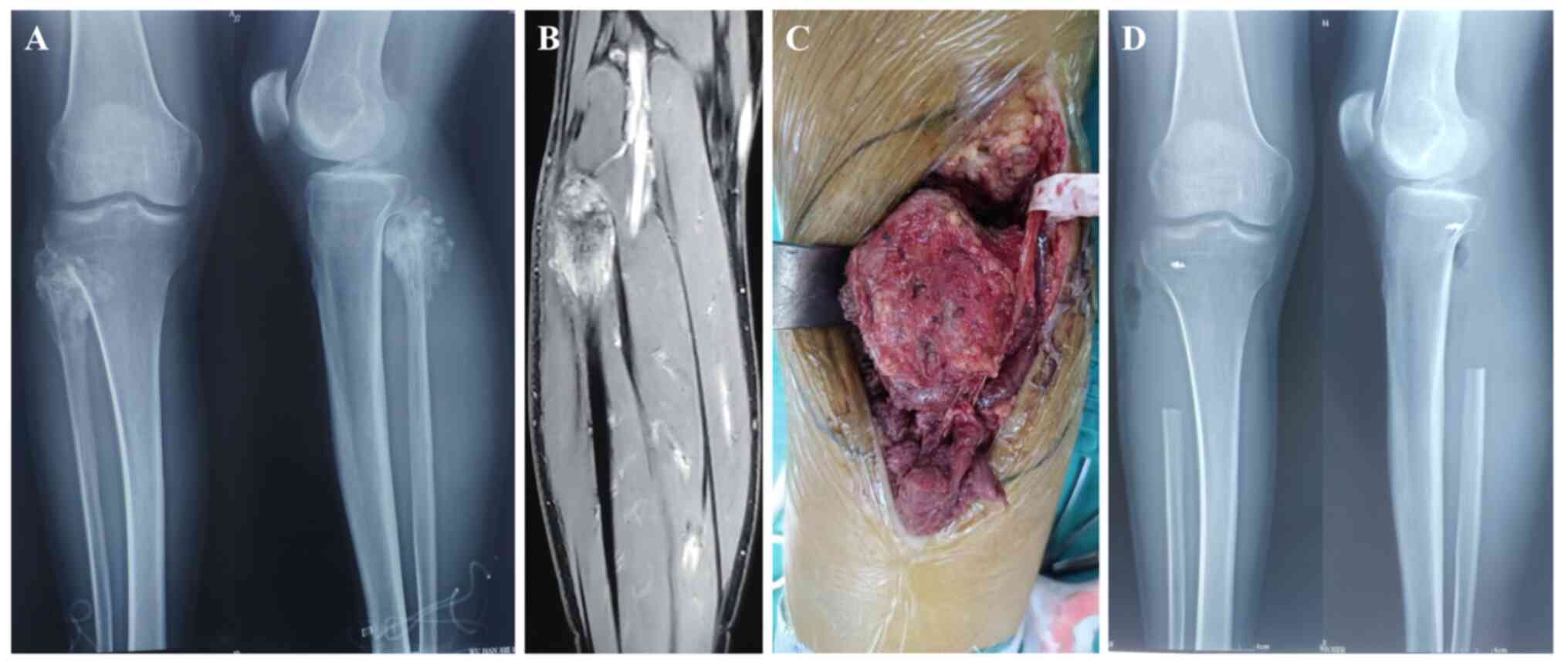
I resection (Fig. 1), and a
chondrosarcoma of the proximal left fibula treated with Malawer Ⅱ
resection (Fig. 2).
 | Table IPatient clinicopathological
characteristics. |
Table I
Patient clinicopathological
characteristics.
| Case no. | Sex | Age, years | Initial
symptom(s) | Follow-up time,
months | Pathological
classification | Enneking stage |
|---|
| 1 | Male | 14 | Pain, nerve palsy,
mass | 92 | Osteosarcoma | IIB |
| 2 | Male | 23 | Pain, nerve
palsy | 36 | Invasive giant cell
tumour of bone | IB |
| 3 | Female | 17 | Pain | 62 | Osteosarcoma | IIB |
| 4 | Female | 8 | Pain | 117 | Osteosarcoma | IIB |
| 5 | Male | 38 | Pain, nerve
palsy | 54 | Chondrosarcoma | IIB |
| 6 | Male | 15 | Pain, mass | 11 | Osteosarcoma | IIB |
| 7 | Male | 12 | Pain | 132 | Osteosarcoma | IIB |
| 8 | Female | 31 | Pain, nerve
palsy | 174 | Epithelioid
sarcoma | IIB |
| 9 | Male | 43 | Pain | 63 | Chondrosarcoma | IIA |
| 10 | Male | 51 | Pain, nerve
palsy | 113 | Fibrosarcoma | IIB |
| 11 | Male | 13 | Pain | 36 | Osteosarcoma | IIB |
| 12 | Male | 42 | Pain, nerve palsy,
mass | 52 | Chondrosarcoma | IIB |
| 13 | Female | 27 | Pain, nerve
palsy | 39 | Invasive giant cell
tumour of bone | IB |
| 14 | Male | 10 | Pain | 70 | Osteosarcoma | IIB |
| 15 | Male | 62 | Pain, mass | 63 | Lymphoma | IIB |
| 16 | Female | 12 | Pain, nerve
palsy | 29 | Osteosarcoma | IIB |
| 17 | Male | 37 | Pain, nerve
palsy | 124 | Leiomyosarcoma | IIA |
| 18 | Female | 14 | Pain | 82 | Osteosarcoma | IIB |
| 19 | Female | 17 | Pain, nerve palsy,
mass | 106 | Osteosarcoma | IIB |
| Table IIIndicators of treatment modalities
and prognostic follow-up. |
Table II
Indicators of treatment modalities
and prognostic follow-up.
| Case no. | Surgery method | Recurrence | Distant
metastases | Prognosis | Joint
stability | Increase of joint
space, mm | MSTS score | LNS |
|---|
| 1 | Malawer I | No | Yes | Death | Yes | 2 | 28 | 82 |
| 2 | Malawer I | No | No | Survival | Yes | 2 | 28 | 81 |
| 3 | Malawer I | Yes | No | Survival | Yes | 2 | 29 | 84 |
| 4 | Malawer I | No | No | Survival | Yes | 1 | 28 | 82 |
| 5 | Malawer I | No | No | Survival | Yes | 2 | 29 | 82 |
| 6 | Malawer I | No | No | Survival | Yes | 2 | 27 | 79 |
| 7 | Malawer I | No | Yes | Survival | Yes | 3 | 28 | 80 |
| 8 | Malawer II | No | Yes | Death | Yes | 2 | 26 | 78 |
| 9 | Malawer I | No | No | Survival | Yes | 3 | 29 | 82 |
| 10 | Malawer I | No | No | Survival | Yes | 3 | 25 | 76 |
| 11 | Malawer I | No | Yes | Death | Yes | 2 | 28 | 80 |
| 12 | Malawer II | No | No | Survival | No | 4 | 23 | 65 |
| 13 | Malawer I | No | No | Survival | Yes | 2 | 26 | 70 |
| 14 | Malawer I | No | No | Survival | Yes | 2 | 28 | 78 |
| 15 | Malawer I | No | Yes | Survival | Yes | 2 | 29 | 84 |
| 16 | Malawer I | Yes | Yes | Death | Yes | 2 | 27 | 80 |
| 17 | Malawer I | Yes | No | Survival | Yes | 3 | 26 | 79 |
| 18 | Malawer II | No | Yes | Survival | Yes | 2 | 29 | 82 |
| 19 | Malawer I | No | No | Survival | Yes | 2 | 25 | 70 |
Discussion
A rare primary malignant tumour of the proximal
peroneal bone presents a challenge for orthopaedic surgeons owing
to its proximity to the biceps femoris tendon, lateral collateral
ligament, common peroneal nerve and anterior tibial artery
(12,13). The classic surgical modalities for
the treatment of proximal fibular tumours were first reported by
Malawer in 1984(8). In the Malawer
I resection for marginal excision, the common peroneal nerve is
preserved, the tibial blood vessels are rarely ligated and cut off,
and the superior tibiofibular joint is excised intragastrically
(8). In the Malawer II method for
extensive resection, the common peroneal nerve and the anterior
tibial vessels are excised, and the tibiofibular joint is excised
outside the joint (8). The
avoidance of postoperative recurrence and metastasis are considered
as the main reference indicators in limb salvage surgery;
amputation should be performed in some cases, particularly in the
following (14,15): i) A large range of malignant
tumours that invade the tibia, ii) multiple invaded fascia
compartments, especially the posterior deep compartment, and iii)
previous biopsies and surgeries causing the contamination of
multiple fascia compartments.
Results from the present study are consistent with
those reported in the literature. For example, a previous study
comprising 112 cases of proximal fibula malignant tumours,
including 50 cases of amputation (45%), 29 cases of Malawer I
resection (26%), and 24 cases of Malawer II resection (21%),
reported that 56 (50%) patients had distant metastasis and 12 (11%)
had local recurrence (3). In
addition, local recurrence was found in six patients receiving
Malawer I and in three patients with Malawer II resection.
Takahashi et al (16)
examined 13 cases of proximal fibular osteosarcoma; according to
Enneking staging, there was 1 case of IA, 1 case of IIA and 11
cases of IIB. Limb salvage treatment was selected for all patients
at the first operative treatment, seven cases were extensively
resected, four cases were marginal resected, two cases were
curettage, and six cases had local recurrence postoperatively. In
the present study, 3 cases were treated with Malawer I resection
and 16 cases with Malawer II resection. Postoperative local
recurrence occurred in three patients, all of whom were treated
with Malawer I, and pulmonary metastasis occurred in seven patients
which treated with Malawer II.
During Malawer I and II resection, the lateral
collateral ligament, the biceps femoris tendon and other structures
that maintain the lateral stability of the knee must be removed to
obtain a safe range of excision (17). For stability and good function of
the knee joint postoperatively, the lateral stable structure of the
knee joint should be reconstructed (18,19).
Currently, the reconstruction of the biceps femoris tendon and the
lateral collateral ligament after removing the proximal fibula
tumour remains controversial. One study reported that the lateral
collateral ligaments and free tendons should be fixed on the
proximal tibia to restore knee stability (18). Malawer et al (8) and Faezypour et al (20) also been reported that the biceps
femoris tendon and the lateral collateral ligament should be
sutured to the surrounding tissues and the anterolateral joint
capsule using non-absorbable suture, which is a simple
reconstruction method. These studies found that none of the
patients complained of instability of the knee joint, no
arthrovarus was found on physical examination, and the medial
stress test was negative (8,20).
However, different opinions have been put forward in the relevant
literature. In the study by Einoder et al (21), no reconstruction of the lateral
stable structure of the knee was performed intraoperatively, and
the average follow-up period was 33 months. Although there was
clinical evidence of lateral knee instability in three patients,
there was no dysfunction, and all six patients could return to
their level of activity before disease diagnosis. It has also been
suggested that even if the lateral collateral ligament and the
tendon insertion of the biceps femoris are reconstructed during
proximal peroneal excision and the knee is still unstable, the gait
is not affected because once the ligament and tendon insertion are
damaged, it is impossible to restore the original position
(22). After reconstruction of the
biceps femoris tendon and lateral collateral ligament in all
patients in the present study, one patient reported self-perceived
instability of the knee joint in, whereas knee joint function in
all other patients was stable. Abdel et al (3) reviewed 112 cases of aggressive
proximal fibular tumours and found no long-term knee instability in
the 53 patients who underwent resection with lateral collateral
ligament reconstruction at a mean follow-up period of 7.4 years,
suggesting that ligament reconstruction is important for functional
knee recovery following operation. Most of these previous studies
have reinforced that, after the resection of proximal fibula
primary and invasive tumours, the biceps femoris tendon and lateral
collateral ligament insertion point was reconstructed. In our
opinion, continuity of the biceps femoris tendon, lateral
collateral ligament, lateral deep fascia and iliotibial band should
be retained as much as possible, and the insertion of the biceps
femoris and lateral collateral ligament should be reconstructed
through the hole in the lateral cortex of the tibial condyle; these
techniques can effectively reconstruct stability and restore knee
function.
There are a number of complications after resecting
proximal fibular tumours; in addition to common peroneal nerve
injury or knee instability, complications may include synovial
leakage, skin necrosis, wound infection and posterior tibial artery
thrombosis (23). Of the 112 cases
reported by Abdel et al (3), 14 (12.5%) had postoperative
complications after resection of proximal fibula tumours; Malawer
II resection was performed in these 14 patients, including 6 cases
of wound infection, 2 cases of posterior tibial artery thrombosis
and 2 cases of common peroneal nerve injury. There were two
patients with common peroneal nerve injury, and none of the
patients in the present study experienced complications, such as
wound infection or arterial thrombosis, which may be related to the
Malawer I resection used in most patients. Results from the present
study are consistent with those of the literature.
There are some limitations to the present study.
First, this was a retrospective study with a limited number of
patients; therefore, studies with larger sample sizes are
necessary. Second, this study lacked an appropriate control group;
therefore, appropriate control groups are necessary. And last, the
follow-up time was relatively short, and longer follow-up period
are necessary.
In summary, for patients with aggressive tumours
such as proximal fibular giant cell tumours or with osteosarcoma
with good pre-operative chemotherapy efficacy, marginal resection
can achieve safety and good postoperative function. For large
tumours with high degree of malignancy and sensitivity to
chemotherapy, extensive resection is necessary and feasible to
reduce recurrence and metastasis. At the same time, reconstruction
of the biceps femoris tendon and lateral collateral ligament after
removing the proximal fibula tumour can achieve knee stability.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by The National Natural
Science Foundation of China (grant nos. 82274559 and 81904231).
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FP and YY gathered the records of the treated
patients and documented the details of tumour, surgery and final
follow up. ZZ and JL analysed the follow-up data. JF, FC and ZS
made substantial contributions to conception and design. JF and FC
confirm the authenticity of all the raw data. All authors have read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
This article contains a study with human
participants, and the study protocol was approved by the Huazhong
University of Science and Technology Committee on Human Research
(Wuhan, China; reference no. 2019-IEC-S274). Written informed
consent to use the patient data for this study was obtained from
all patients.
Patient consent for publication
Consent for publication of images was obtained from
all patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gümüştaş SA, Çevik HB and Kayahan S: An
epidemiological study of primary bone tumors of the fibula. Arch
Bone Jt Surg. 9:548–553. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Arikan Y, Misir A, Ozer D, Kizkapan TB,
Yildiz KI, Saygili MS, Incesoy MA, Dincel YM, Gursu SS and Sahin V:
The incidence and distribution of primary fibula tumors and
tumor-like lesions: A 35-year experience. J Orthop Surg (Hong
Kong). 26(2309499018798180)2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Abdel MP, Papagelopoulos PJ, Morrey ME,
Inwards CY, Wenger DE, Rose PS and Sim FH: Malignant proximal
fibular tumors: Surgical management of 112 cases. J Bone Joint Surg
Am. 94(e165)2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Huntley K, Al-Hardan W and Pretell-Mazzini
J: Surgical management of benign tumors of the proximal fibula. J
Am Acad Orthop Surg Glob Res Rev. 5(e21)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Marinova VV, Slavchev SA, Patrikov KD,
Tsenova PM and Georgiev GP: Neoadjuvant and adjuvant treatment with
denosumab in aggressive giant-cell tumor of bone in the proximal
fibula: A case report. Folia Med (Plovdiv). 60:637–640.
2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Arikan Y, Misir A, Gur V, Kizkapan TB,
Dincel YM and Akman YE: Clinical and radiologic outcomes following
resection of primary proximal fibula tumors: Proximal fibula
resection outcomes. J Orthop Surg (Hong Kong).
27(2309499019837411)2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Steffner RJ and Jang ES: Staging of bone
and soft-tissue sarcomas. J Am Acad Orthop Surg. 26:e269–e278.
2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Malawer MM: Surgical management of
aggressive and malignant tumors of the proximal fibula. Clin Orthop
Relat Res. 172–181. 1984.PubMed/NCBI
|
|
9
|
Xu L, Li X, Wang Z, Xiong J and Wang S:
Functional evaluation for patients with lower extremity sarcoma:
Application of the Chinese version of Musculoskeletal Tumor Society
scoring system. Health Qual Life Outcomes. 15(107)2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wang W, Liu L, Chang X, Jia ZY, Zhao JZ
and Xu WD: Cross-cultural translation of the Lysholm knee score in
Chinese and its validation in patients with anterior cruciate
ligament injury. BMC Musculoskelet Disord. 17(436)2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
LaPrade RF, Heikes C, Bakker AJ and
Jakobsen RB: The reproducibility and repeatability of varus stress
radiographs in the assessment of isolated fibular collateral
ligament and grade-III posterolateral knee injuries. An in vitro
biomechanical study. J Bone Joint Surg Am. 90:2069–2076.
2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Futani H, Kumanishi S, Minakawa GO and
Yoshiya S: Osteoscopic surgery of giant cell tumor of bone for
preservation of proximal fibula. Anticancer Res. 38:2995–3000.
2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yao H, Wang B, Wen L, Jin Q, Li H, Huang
G, Yin J, Zou C, Xie X and Shen J: Comparison of clinical features,
management and outcomes of osteosarcoma located in proximal fibula
and proximal tibia: A propensity score matching analysis. BMC
Cancer. 18(1195)2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Malawer M, Buch R, Reaman G, Priebat D,
Potter B, Khurana J, Shmookler B, Patterson K and Schulof R: Impact
of two cycles of preoperative chemotherapy with intraarterial
cisplatin and intravenous doxorubicin on the choice of surgical
procedure for high-grade bone sarcomas of the extremities. Clin
Orthop Relat Res. 214–222. 1991.PubMed/NCBI
|
|
15
|
Atalay IB, Yilmaz S, Korkmaz I, Ekşioğlu
MF and Güngör BŞ: Surgical management of primary malignant proximal
fibular tumors: Functional and clinical outcomes of 23 patients.
Eklem Hastalik Cerrahisi. 30:24–31. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Takahashi S, Ogose A, Tajino T, Osanai T
and Okada K: Osteosarcoma of the proximal fibula. An analysis of 13
cases in the northern Japan. Ups J Med Sci. 112:366–372.
2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Dieckmann R, Gebert C, Streitburger A,
Budny TB, Henrichs MP, Vieth V, Gebert C and Hardes J: Proximal
fibula resection in the treatment of bone tumours. Int Orthop.
35:1689–1694. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bickels J, Kollender Y, Pritsch T, Meller
I and Malawer MM: Knee stability after resection of the proximal
fibula. Clin Orthop Relat Res. 454:198–201. 2007.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Tang X, Guo W, Yang R and Wang Y: Poor
prognosis and complications are common in limb salvage surgery for
malignant tumors of the proximal tibia invading the fibula. Arch
Orthop Trauma Surg. 134:299–304. 2014.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Faezypour H, Davis AM, Griffin AM and Bell
RS: Giant cell tumor of the proximal fibula: Surgical management. J
Surg Oncol. 61:34–37. 1996.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Einoder PA and Choong PF: Tumors of the
head of the fibula: Good function after resection without ligament
reconstruction in 6 patients. Acta Orthop Scand. 73:663–666.
2002.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Draganich LF, Nicholas RW, Shuster JK,
Sathy MR, Chang AF and Simon MA: The effects of resection of the
proximal part of the fibula on stability of the knee and on gait. J
Bone Joint Surg Am. 73:575–583. 1991.PubMed/NCBI
|
|
23
|
Ben Amotz O, Ramirez R, Husain T, Lehrman
C, Teotia S and Sammer DM: Complications related to harvest of the
proximal end of the fibula: A systematic review. Microsurgery.
34:666–669. 2014.PubMed/NCBI View Article : Google Scholar
|