Introduction
Prostate cancer is the second most commonly
diagnosed malignancy in men worldwide, with an estimated 1.5
million new cases and approximately 400,000 deaths annually
(1). In Japan, diagnosis and
treatment decisions are guided by prostate-specific antigen (PSA)
levels, Gleason score, and the National Comprehensive Cancer
Network (NCCN) risk classification (2).
Radiotherapy remains a key treatment option for
localized prostate cancer. Volumetric Modulated Arc Therapy (VMAT),
an advanced technique within intensity-modulated radiotherapy,
delivers highly conformal dose distributions while minimizing
exposure to surrounding normal tissues (3). Despite these advantages, early
urinary toxicities-including frequency, dysuria, and reduced
urinary flow-remain common. Even low-grade (Grade 1) toxicities can
significantly affect quality of life. However, robust biomarkers
capable of predicting such events are still lacking.
Radiation exposure not only causes direct and
indirect DNA damage but also induces substantial alterations in
proteins and lipids, leading to oxidative stress and inflammatory
responses (4). These biological
disturbances are reflected in shifts in metabolite profiles.
Metabolomics, which comprehensively characterizes small molecules
in biological samples, has therefore gained increasing attention in
radiation research as a means to capture these downstream effects
(5,6). Urinary metabolomics, in particular,
offers a non-invasive method to monitor treatment-related
physiological changes (7). In our
previous analysis of this dataset, we examined the role of
phospholipase A2 (PLA2) activity during VMAT and identified its
potential as a predictor of acute urinary toxicity (8). Although this finding highlighted an
important enzymatic pathway, it provided only a partial perspective
on the broader metabolic disruptions caused by irradiation. A
narrow focus on PLA2 leaves open the question of whether other
lipid-related pathways-such as triglyceride (TG) hydrolysis, bile
acid (BA)-mediated mechanisms, or cholesterol ester turnover-also
contribute to urinary adverse events.
A secondary analysis of the same comprehensive
dataset provides an opportunity to overcome this limitation. By
re-evaluating all 630 quantified metabolites with a focus on
treatment-related toxicity rather than a single enzymatic pathway,
we can uncover novel candidate biomarkers, delineate alternative
metabolic routes, and reinforce the biological rationale for
metabolomic monitoring in radiotherapy. In particular,
correlation-based ranking and network analysis enable the detection
of coordinated alterations across lipid classes, rather than
isolated enzymatic signals. In the present study, we conducted a
secondary analysis of a previously published urinary metabolomics
dataset generated in an original clinical study during VMAT
(8) and deposited in MetaboBank
(accession numbers MTBKS242 and MTBKS243). No new patient
recruitment or urine collection was performed for this secondary
analysis.
Accordingly, the present study aimed to identify
urinary metabolites and metabolic pathways associated with early
urinary adverse events during VMAT, extending beyond PLA2 to
achieve a more integrative understanding of lipid metabolism under
irradiation.
Materials and methods
Study design
The present study is a secondary analysis of a
previously published urinary metabolomics dataset originally
generated in a clinical study during VMAT and made publicly
available in MetaboBank (8). No
new patient recruitment, intervention, sample collection, or
metabolomic data generation was performed as part of the present
study. As this study exclusively analyzed de-identified data
obtained from a public repository, additional ethical approval was
not required. The cohort comprised 11 males (0 females), with a
median age of 70 years (range, 59-75), who underwent VMAT at
Hirosaki University Hospital between June 2021 and March 2022, as
described in the original report (8). All patients received 76 Gy in 38
fractions (2 Gy per fraction, five fractions weekly). Clinical
characteristics-including age, PSA level, Gleason score, TNM stage,
NCCN risk classification, prior or concurrent hormone therapy, and
acute adverse events-were documented in the initial publication
(8). Seven patients experienced
Grade 1 urinary toxicities (frequency, dysuria, or decreased flow),
while four patients reported no acute urinary events. Toxicities
were graded according to the Common Terminology Criteria for
Adverse Events, version 5.0(9).
Metabolomics profiling
In the original clinical study (8), daily first-morning urine samples (10
ml) had been self-collected during the treatment period using a
standardized collection device and stored at -80˚C until analysis,
as previously described (8).
Metabolomic profiling was performed with the MxP® Quant 500 kit
(Biocrates Life Sciences AG, Innsbruck, Austria), enabling
quantification of 630 metabolites, comprising 107 small molecules
and 523 lipids. Sample preparation, LC-MS/MS acquisition, and
quality control procedures followed the manufacturer's standard
operating protocol and were fully detailed in the original report
(8). Briefly, metabolite
concentrations were determined using multiple reaction monitoring
with isotope-labeled internal standards and normalized to urinary
creatinine to correct for dilution variability. The complete
metabolomics dataset is publicly available in MetaboBank under
accession numbers MTBKS242 (https://mb2.ddbj.nig.ac.jp/study/MTBKS242.html) and
MTBKS243 (https://mb2.ddbj.nig.ac.jp/study/MTBKS243.html), as
described in the original report (8).
Statistical analysis
Because this study is exploratory and
hypothesis-generating, statistical interpretation focused on the
direction and magnitude of associations rather than confirmatory
inference. For each patient and each metabolite, Spearman's rank
correlation coefficient (ρ) was calculated between the number of
delivered radiation fractions and the creatinine-normalized
metabolite concentration. Patient-level ρ values were summarized
within each group [AE(+) vs. AE(-)], and metabolites were ranked by
the median ρ in each group. To screen for group-specific metabolic
alterations, we used a bidirectional rank-based screening as
follows: (i) the top 60 metabolites with the highest median ρ in
AE(+) were compared with the bottom 60 metabolites with the lowest
median ρ in AE(-); and (ii) the top 60 metabolites in AE(-) were
compared with the bottom 60 metabolites in AE(+). Overlapping
metabolites across these contrasted sets were carried forward for
network analysis (a predefined exploratory threshold). Network
analyses of the selected metabolites were performed using OmicsNet
2.0 (https://www.omicsnet.ca) (10), which integrates curated
metabolite-enzyme and pathway interaction data from public
databases including KEGG, HMDB, Reactome, and SMPDB. Networks were
generated under the Homo sapiens setting using the platform's
default metabolite-enzyme interaction resources. Statistical
analyses were carried out with Statcel 5 (OMS Publishing Inc.,
Saitama, Japan). Between-group differences in patient-level ρ
values were assessed using Mann-Whitney U tests. P-values were
adjusted for multiple testing using the Benjamini-Hochberg false
discovery rate (FDR) procedure; nominal p-values and FDR-adjusted
q-values are reported. FDR adjustment was implemented in Python
(Google Colab) using statsmodels.stats.multitest (method=̔fdr_bh’).
In addition, changes in metabolite levels (Δ) were calculated for
each patient as the difference between metabolite levels at the end
of radiotherapy (fraction 38) and baseline (fraction 0). These Δ
values were compared between the AE(+) and AE(-) groups using the
Mann-Whitney U test. This analysis was performed as a complementary
evaluation of pre-post changes.
Sensitivity analysis
To assess potential confounding by concomitant
ursodeoxycholic acid (UDCA) treatment, we repeated the
between-group comparison after excluding the single AE(+) patient
receiving UDCA (Pt.7) and summarized the results for the key
metabolites in Tables SI and
SII.
Results
Patient characteristics
The clinical profiles of the 11 patients included in
this secondary analysis are summarized in Table I. The median age was 70 years
(range, 59-75). Median PSA level was 7.23 ng/ml, and the median
Gleason score was 7. According to the NCCN risk classification, 6
patients (54.5%) were categorized as high risk. Seven patients
(63.6%) developed Grade 1 urinary adverse events [AE(+)], while 4
patients (36.4%) experienced no acute urinary events [AE(-)].
 | Table IClinical characteristics of
patients. |
Table I
Clinical characteristics of
patients.
| Patient no. | TNM
classification | Stage (risk
level) | Gleason score (prior
to the start of irradiation) | Age, years | Delivered
fractions | Urine samples, n | PSA, ng/ml | Hormone therapy | AE | CC |
|---|
| 1 |
cT3N0M0 | III (high) | 5+4 | 69 | 38 | 8 | 5.10 | CAB (leuprorelin
acetate + estramustine phosphate sodium hydrate); leuprorelin
acetate SR | (+) | Urethral pressure,
painful urination |
| 2 |
cT3aN0M0 | III (high) | 4+3 | 69 | 38 | 8 | 18.44 | CAB; leuprorelin
acetate SR | (+) | Urethritis, painful
urination, difficulty urinating, frequent urination |
| 3 |
cT2bN0M0 | II (mid) | 5+4 | 72 | 38 | 8 | 26.60 | CAB | (+) | Frequent
urination |
| 4 |
cT3aN0M0 | III (high) | 5+3 | 61 | 38 | 8 | 23.30 | CAB; bicalutamide for
8 weeks | (+) | Urethritis,
difficulty urinating |
| 5 |
cT3N0M0 | III (high) | 4+5 | 75 | 38 | 7 | 4.05 | NHT | (+) | Frequent urination,
decreased urinary flow |
| 6 |
cT1cN0M0 | II (mid) | 3+4 | 71 | 38 | 7 | 8.80 | Bicalutamide | (+) | Frequent
urination |
| 7 |
cT2bN0M0 | II (mid) | 4+3 | 71 | 38 | 7 | 4.44 | CAB using
bicalutamide and leuprorelin acetate SR, and ursodeoxy cholic
acid | (+) | Frequent urination,
decreased urinary flow |
| 8 |
cT2bN0M0 | II (mid) | 3+4 | 68 | 38 | 5 | 7.23 | CAB | (-) | - |
| 9 |
cT2aN0M0 | II (high) | 4+4 | 73 | 38 | 5 | 4.38 | Degarelix acetate +
estramustine phosphate sodium hydrate | (-) | - |
| 10 |
cT1cN0M0 | I (mid) | 3+3 | 70 | 38 | 5 | 27.20 | CAB; leuprorelin
acetate SR | (-) | - |
| 11 |
cT1cN0M0 | I (low) | 3+3 | 59 | 38 | 5 | 6.97 | - | (-) | - |
Correlation analysis of urinary
metabolites
In total, 630 urinary metabolites quantified by the
MxP® Quant 500 kit were analyzed. For each patient,
Spearman's rank correlation coefficients (ρ) were calculated
between the number of delivered radiation fractions and the
creatinine-normalized concentrations of each metabolite, yielding a
patient-level ρ for each metabolite. Between-group differences in
patient-level ρ values were then assessed using Mann-Whitney U
tests, and p-values were adjusted using Benjamini-Hochberg FDR
correction. After FDR correction across 630 metabolites, none of
the metabolites remained significant (minimum q-value=0.49)
(Table SII). Therefore, the
metabolites highlighted below should be interpreted as exploratory
candidates based on consistent directional differences and nominal
associations. We focused on metabolites that demonstrated strong
positive or negative correlations with radiation fraction number
based on rank order of patient-level Spearman's ρ values.
Specifically, because the sample size was limited and the analysis
involved a large number of metabolites (n=630), strict
multiple-testing correction markedly reduced statistical power.
Therefore, to identify biologically meaningful directional patterns
while limiting the number of candidates for downstream network
analysis, a rank-based screening strategy focusing on metabolites
showing the strongest positive or negative correlations with
radiation fraction number was adopted. Specifically, this approach
aimed to identify metabolites showing opposite directional trends
between groups [those increasing with treatment in the AE(+) group
while decreasing in the AE(-) group, and vice versa]. Specifically,
the top 60 metabolites showing the strongest positive correlations
with fraction number in AE(+) patients and the 60 metabolites
showing the strongest negative correlations (lowest ρ values) in
AE(-) patients were selected. Thus, the ‘top 60’ refers to
metabolites with the most extreme correlation coefficients in each
direction based on rank order, including those with the strongest
negative correlations. Conversely, metabolites with the opposite
directional patterns [top 60 metabolites with the strongest
positive correlations in AE(-) patients and top 60 metabolites with
the strongest negative correlations in AE(+) patients] were also
examined. This bidirectional screening approach was designed to
identify metabolites exhibiting consistent but opposite directional
changes between the AE(+) and AE(-) groups. The overlap structure
of these ranked sets is summarized in Fig. 1, and this bidirectional screening
yielded 9 overlapping metabolites (Tables II and III). Of these, 4
metabolites-cholesteryl ester [CE(20:4)], taurodeoxycholic acid
(TDCA), TG(18:0_32:2), and TG(18:3_34:1)-showed positive
correlation in AE(+) but negative correlation in AE(-). Conversely,
5 metabolites-phosphatidylcholine (PC aa C42:2), PC ae C42:1,
TG(16:0_38:1), fatty acid [FA(20:2)], and diglyceride
[DG(18:1_18:1)]-demonstrated the opposite trend (positive in AE(-),
negative in AE(+)). As a complementary analysis, changes in
metabolite levels (Δ) between baseline (fraction 0) and the end of
radiotherapy (fraction 38) were compared between AE(+) and AE(-)
groups. The results of this Δ-based comparison are summarized in
Table SI. Overall, several
metabolites exhibited opposite directional changes between groups,
consistent with the correlation-based findings. Among these, TG
(16:0_38:1) and DG (18:1_18:1) showed nominally significant
differences between groups in the primary analysis, although this
was not consistently observed in the sensitivity analysis. These
results should be interpreted as exploratory.
| Table IIMedian (range) patient-level
Spearman's rank correlation coefficients (ρ) between radiation
fraction number and metabolite concentration in the AE(+) and AE(-)
groups for metabolites showing opposite directional
correlations. |
Table II
Median (range) patient-level
Spearman's rank correlation coefficients (ρ) between radiation
fraction number and metabolite concentration in the AE(+) and AE(-)
groups for metabolites showing opposite directional
correlations.
| | Metabolites |
|---|
| AE group | CE (20:4) | TDCA | TG (18:0_32:2) | TG (18:3_34:1) |
|---|
| AE(+) | 0.34 (0.10 to
0.67) | 0.22 (-0.20 to
0.70) | 0.22 (-0.16 to
0.46) | 0.21 (-0.16 to
0.46) |
| AE(-) | -0.35 (-0.80 to
0.30) | -0.37 (-0.78 to
-0.30) | -0.46 (-0.90 to
0.05) | -0.60 (-0.90 to
-0.40) |
| Table IIIMedian (range) patient-level
Spearman's rank correlation coefficients (ρ) between radiation
fraction number and metabolite concentration in the AE(-) and AE(+)
groups for metabolites showing opposite directional
correlations. |
Table III
Median (range) patient-level
Spearman's rank correlation coefficients (ρ) between radiation
fraction number and metabolite concentration in the AE(-) and AE(+)
groups for metabolites showing opposite directional
correlations.
| | Metabolites |
|---|
| AE group | PC aa C42:2 | TG (16:0_38:1) | PC ae C42:1 | FA (20:2) | DG (18:1_18:1) |
|---|
| AE(-) | 0.61 (0.53 to
0.90) | 0.48 (0.20 to
0.67) | 0.36 (0.20 to
0.80) | 0.35 (-0.20 to
0.60) | 0.32 (-0.90 to
0.90) |
| AE(+) | -0.19 (-0.77 to
0.06) | -0.23 (-0.57 to
0.05) | -0.15 (-0.45 to
0.29) | -0.22 (-0.76 to
0.36) | -0.35 (-0.76 to
-0.02) |
Network analysis of lipid
metabolism
To explore the biological significance of the
overlapping metabolites, interaction networks were generated using
OmicsNet 2.0. Metabolites that increased in AE(+) patients were
enriched in pathways involving cholesterol esters, BAs, and TGs
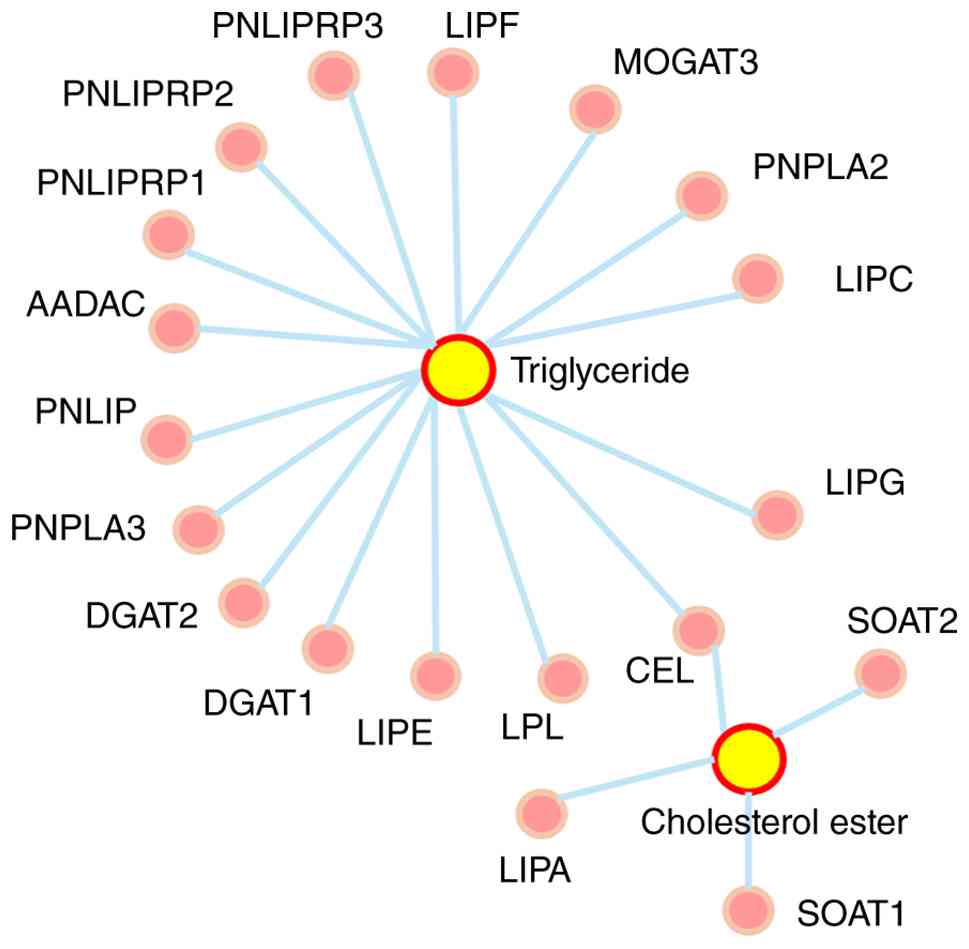
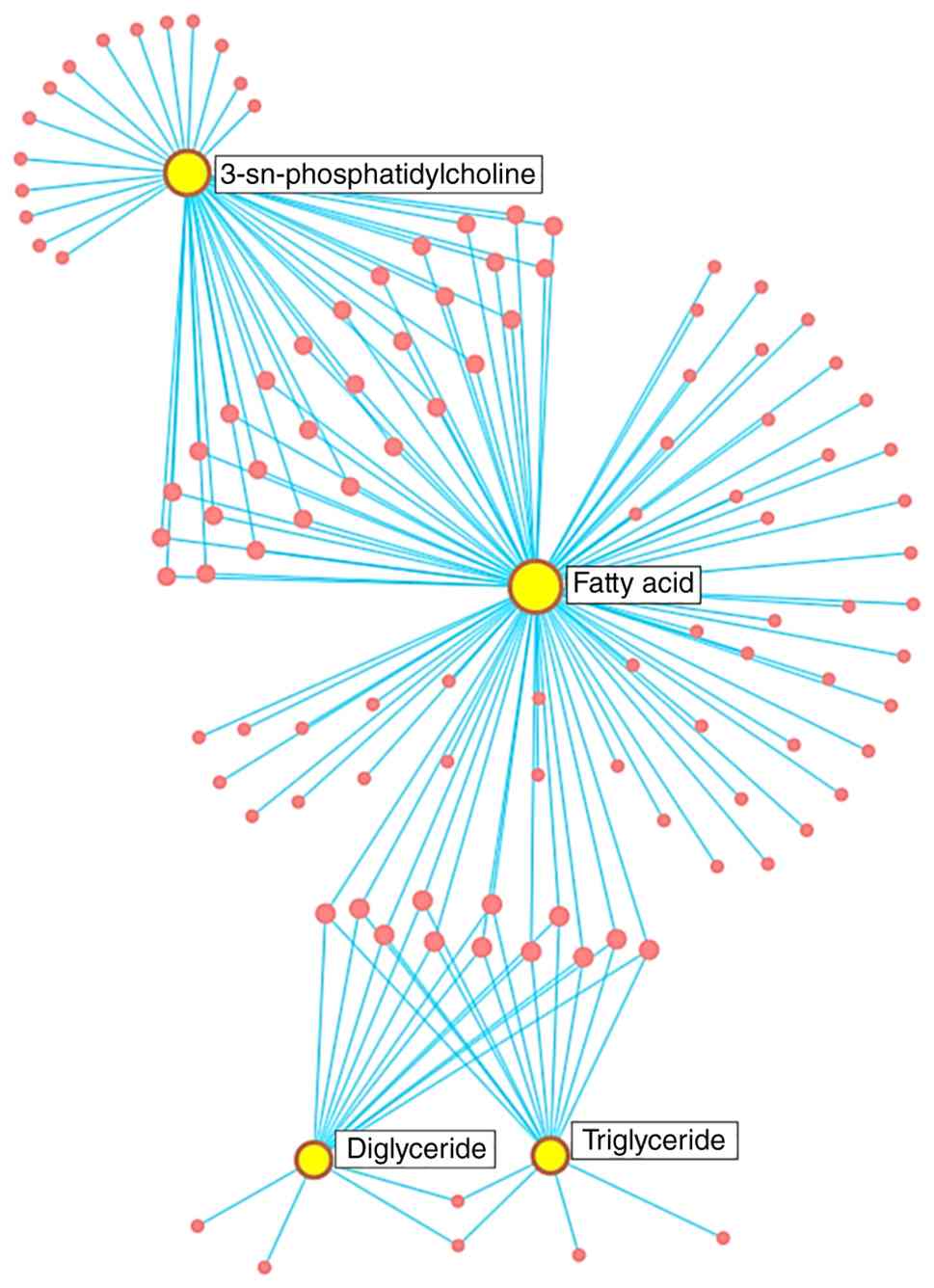
(Fig. 2). In contrast, those that
decreased in AE(+) were predominantly linked to diglycerides, fatty
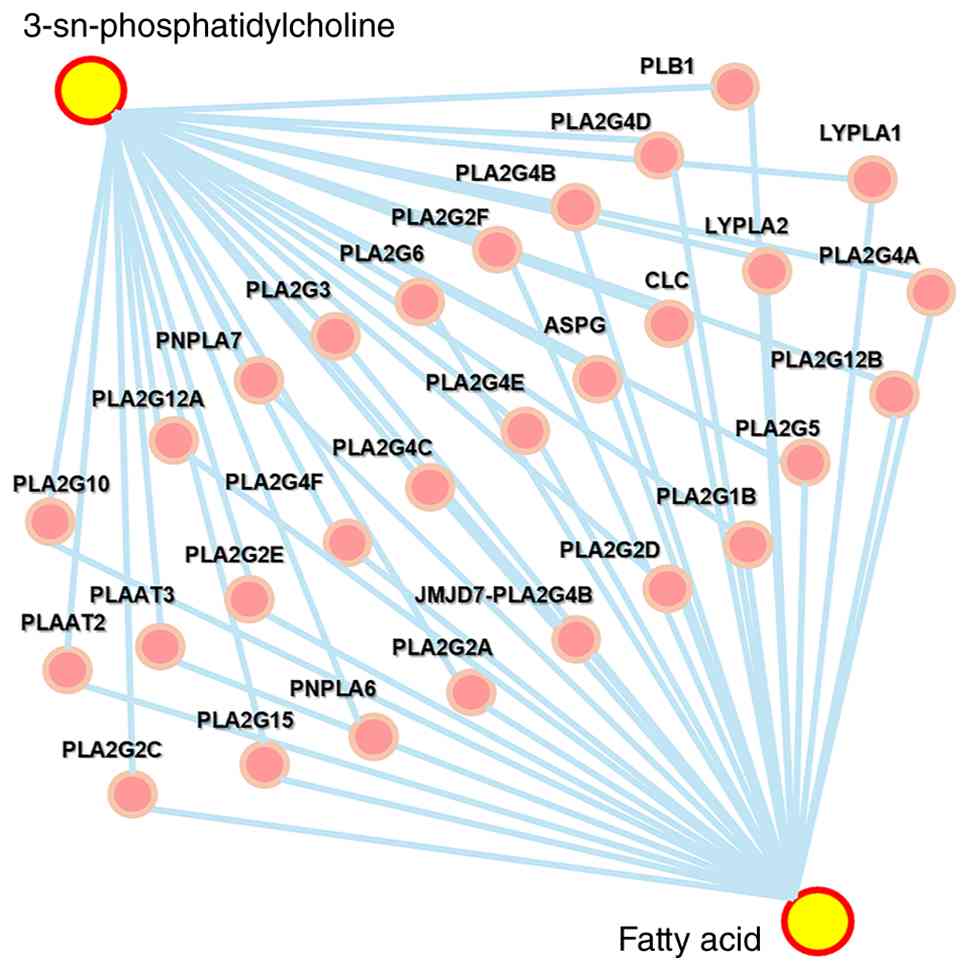
acids, and PCs (Fig. 3). Expanded
network analysis further identified 29 metabolites connecting PCs
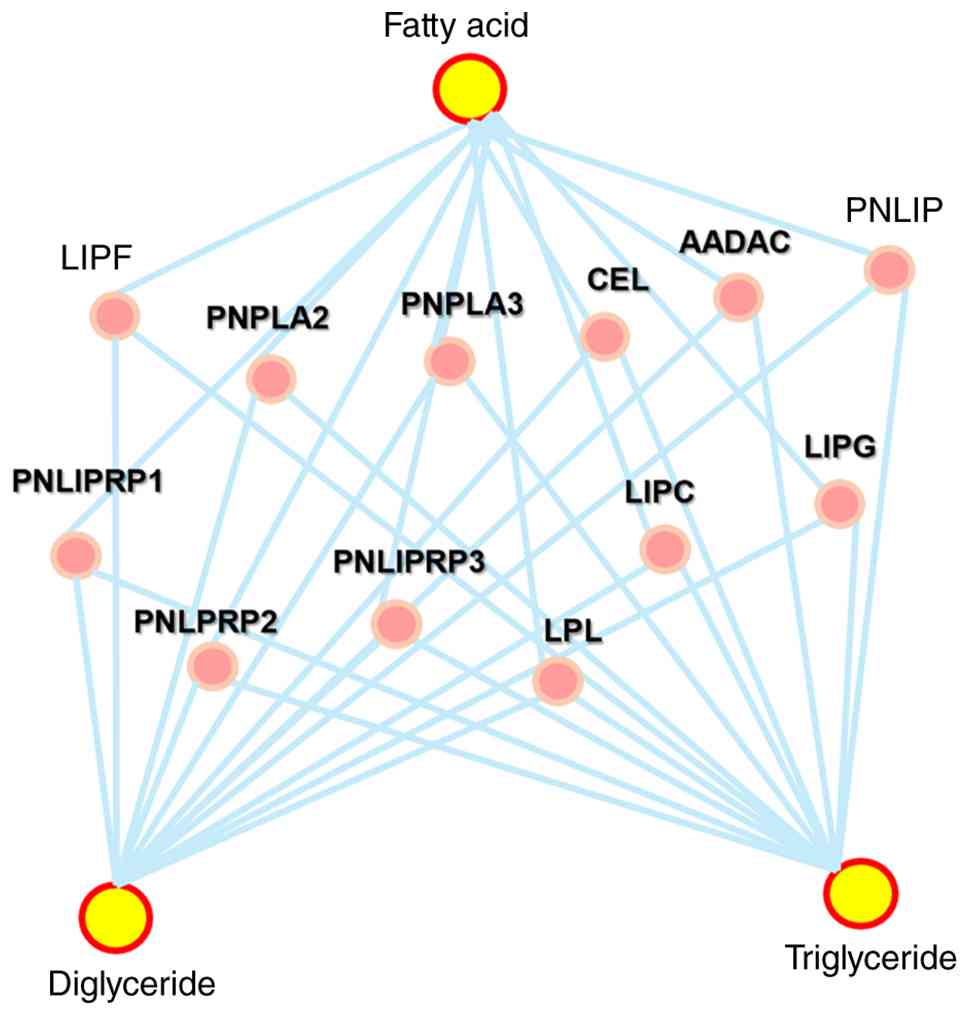
with FAs (Fig. 4; Table SIII) and 12 metabolites bridging
fatty acids with diglycerides/TGs (Fig. 5; Table SIV). These coordinated alterations
pointed to a disruption in lipolytic processes. Sensitivity
analysis excluding the UDCA-treated patient (Pt.7) showed that the
nominal associations and directional patterns for the key
metabolites were largely preserved (Table SII).
In particular, TDCA remained nominally different
between groups (p=0.01), although q-values increased after
exclusion due to reduced sample size.
Hypothesized involvement of TG
hydrolysis
Building on these results, we focused on the
lipolysis pathway, which converts TGs into fatty acids and
glycerides. A schematic representation is shown in Fig. 6 (Table SV). The simultaneous increase in
specific TG isomers and paradoxical reduction in their
corresponding fatty acids suggested a potential inhibition of
lipolysis. In addition, alterations in cholesteryl ester metabolism
appeared to be involved. Collectively, these exploratory findings
suggest that early urinary adverse events during VMAT may be linked
to dysregulated lipid metabolism, particularly impaired hydrolysis
of TGs into fatty acids.
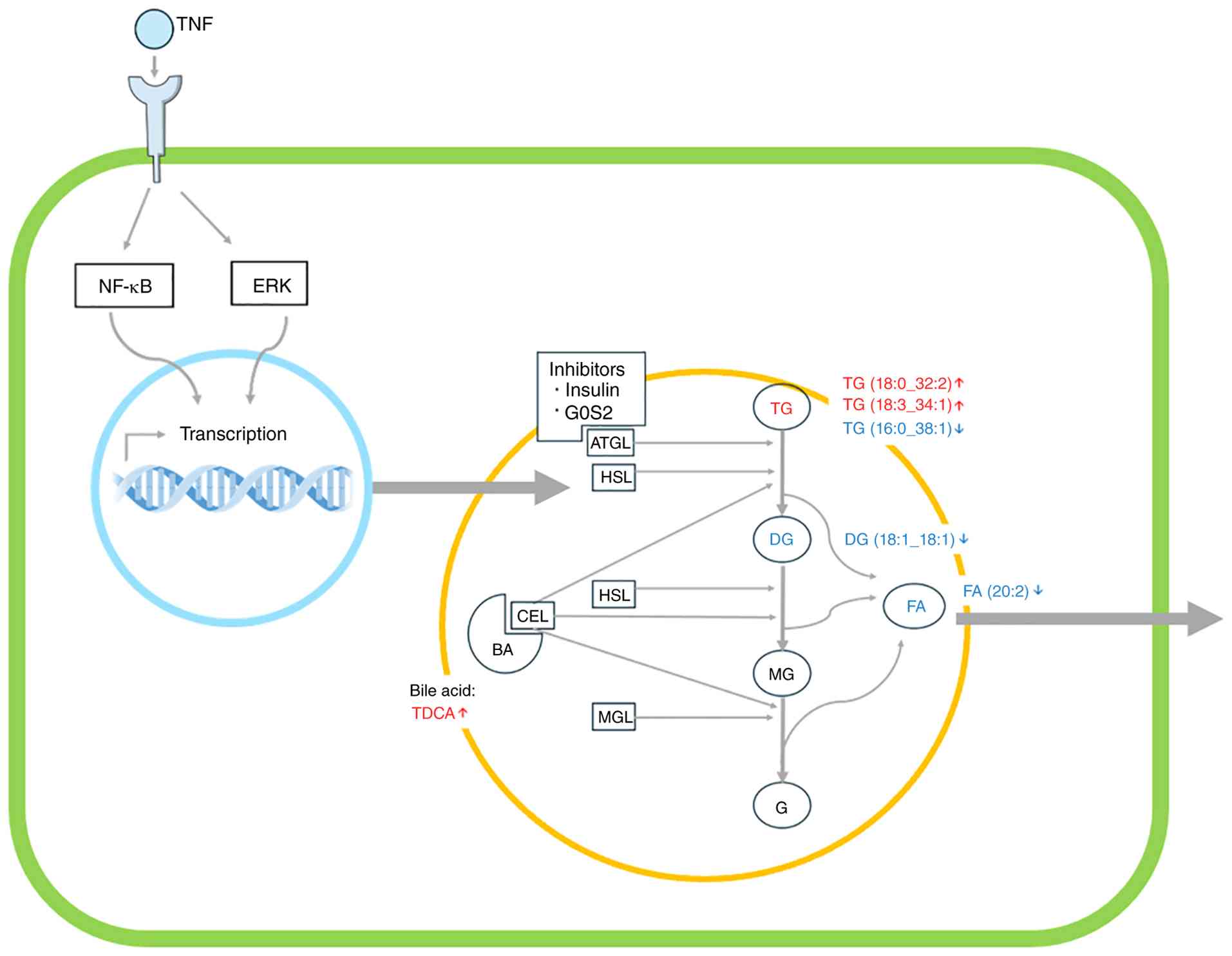 | Figure 6Schematic of TG hydrolysis (lipolysis)
and associated intermediates. TNF signaling via NF-κB and ERK may
influence transcriptional regulation of lipolytic enzymes.
Inhibitors, including insulin and G0S2, suppress ATGL activity.
Observed metabolite changes in the adverse event-positive group are
indicated by arrows. ATGL, adipose triglyceride lipase; HSL,
hormone-sensitive lipase; MGL, monoglyceride lipase; CEL, carboxyl
ester lipase; TG, triglyceride; DG, diglyceride; MG, monoglyceride;
FA, fatty acid; BA, bile acid; TDCA, taurodeoxycholic acid; G,
glycerol. |
Discussion
In this secondary analysis of urinary metabolomics
from patients receiving VMAT for localized prostate cancer, we
observed distinct lipid metabolic alterations showing directional
differences between AE(+) and AE(-) groups; however, none of the
metabolites remained statistically significant after FDR
correction. Four metabolites-CE(20:4), TDCA, TG(18:0_32:2), and
TG(18:3_34:1)-showed positive correlations with radiation fractions
in AE(+) but negative correlations in AE(-), whereas five
metabolites-PC aa C42:2, PC ae C42:1, TG(16:0_38:1), FA(20:2), and
DG(18:1_18:1)-displayed the opposite pattern. Network analysis
revealed convergence on lipid pathways, particularly TG hydrolysis
into fatty acids.
We previously reported phospholipase A2 (PLA2)
activity in urinary metabolites as a potential biomarker for
predicting acute toxicities during VMAT (8). While that work emphasized
phospholipid remodeling, the present analysis broadens the
perspective to the lipid network as a whole. The discordant
behavior of TGs and their corresponding fatty acids points to
impaired lipolysis as a candidate mechanism for urinary AEs,
thereby complementing earlier findings by shifting from a single
enzymatic activity to a pathway-level view.
Lipolysis proceeds through sequential hydrolysis of
TGs by adipose TG lipase (ATGL), hormone-sensitive lipase (HSL),
and monoglyceride lipase, ultimately producing free fatty acids and
glycerol (11). Cholesteryl ester
lipase also contributes by hydrolyzing cholesterol esters and TGs
(12). The paradoxical
accumulation of certain TG species with reduced levels of
corresponding fatty acids in AE(+) patients suggests suppression of
this pathway. Possible inhibitory mechanisms include G0/G1 switch
gene 2 (G0S2), a direct ATGL inhibitor (11), and insulin-mediated downregulation
of HSL via cAMP signaling (12).
Furthermore, cytokines such as TNF-α are known to influence
lipolysis through NF-κB and ERK pathways, potentially intersecting
with radiation-induced inflammation (13). Collectively, these findings are
consistent with the possibility that radiation perturbs lipolytic
regulation, leading to TG accumulation, reduced fatty acid release,
which may be associated with urinary toxicity.
Only limited urinary biomarkers have been
investigated for predicting early urinary AEs during radiotherapy.
Previous studies have primarily focused on inflammatory cytokines
(e.g., IL-6, IL-8), oxidative stress markers such as
8-hydroxy-2'-deoxyguanosine (8-OHdG), or tubular injury markers
including NGAL and β2-microglobulin. These markers reflect
downstream inflammation or tissue injury but do not capture broader
metabolic pathway alterations. To our knowledge, comprehensive
urinary metabolomic profiling integrated with fraction-dependent
correlation analysis has not previously been applied to early
urinary toxicity during VMAT. Our pathway-oriented, lipid-focused
analysis therefore provides a systems-level perspective that
extends beyond single-marker approaches. The identification of
lipid metabolic dysregulation highlights the potential of urinary
metabolomics for toxicity monitoring. The involvement of bile
acid-related metabolites such as TDCA further underscores the need
to consider background medications when interpreting metabolomic
findings.
This study has several limitations. First, the
sample size was small (n=11), which precludes statistical
generalization and limits power. Second, only Grade 1 urinary
toxicities were observed, leaving it unclear whether similar
metabolic alterations would be observed in higher-grade AEs. Third,
as a secondary analysis of an existing dataset, this work is
hypothesis-generating rather than causal. In addition, none of the
identified metabolites remained statistically significant after FDR
correction, underscoring the exploratory nature of these findings.
Although Grade 1 urinary AEs are clinically mild, we consider them
to reflect early radiation-induced biological perturbations in the
urinary tract that may precede more severe toxicity. Whether
similar or amplified metabolic patterns are observed in Grade ≥2
urinary AEs should be evaluated in larger prospective cohorts. One
AE(+) patient received ursodeoxycholic acid (UDCA), which could
theoretically influence BA-related metabolites. However, a
sensitivity analysis excluding this patient yielded similar nominal
associations and preserved the directional patterns of the key
metabolites (Table SI and
SII), suggesting that our main
interpretation was unlikely to be entirely driven by this single
case.
Future research should validate these findings in
larger, prospectively collected cohorts with broader toxicity
profiles. Complementary experimental approaches, such as in vitro
irradiation models or enzymatic assays, may help clarify whether
the paradoxical increase in TGs alongside reduced fatty acids
reflects inhibition of lipolysis. Such studies would provide
mechanistic evidence for the associations reported here and enhance
the translational potential of urinary metabolomics in
radiotherapy.
In summary, this study suggests that early urinary
AEs during VMAT may be associated with dysregulated lipid
metabolism, particularly impaired hydrolysis of TGs into fatty
acids. These results build upon our prior findings on PLA2 activity
(8) and support the potential of
urinary metabolomics as a non-invasive biomarker platform for
predicting radiotherapy-related toxicities. Although exploratory,
this analysis generates testable hypotheses that warrant validation
in larger cohorts and mechanistic studies to better define the role
of lipid metabolism in radiation-induced urinary toxicity.
Supplementary Material
Comparison of metabolite changes (Δ)
between baseline (fraction 0) and end of radiotherapy (fraction 38)
between AE(+) and AE(-) groups, with and without exclusion of the
UDCA-treated patient (patient 7).
Correlation-based sensitivity analysis
of patient-level Spearman’s rank correlation coefficients (ρ) with
and without exclusion of the UDCA-treated patient (patient 7).
Enzymes and genes associated with the
phosphatidylcholine-fatty acid interaction network identified by
OmicsNet analysis.
Enzymes and genes associated with the
fatty acid-diglyceride/triglyceride interaction network identified
by OmicsNet analysis.
Enzymes associated with the
hypothesized triglyceride-fatty acid lipolysis pathway identified
in the network analysis.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Japan Society
for the Promotion of Science, Grants-in-Aid for Scientific Research
(B) (grant no. 23K21419) and Grant-in-Aid for Challenging Research
(grant no. 25K22722).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
MF and SM designed the study, prepared the
manuscript draft and substantively participated in the manuscript
revision. MF, YT, HO and SM analyzed all biological data. SM
supervised the study, critically reviewed the manuscript, and
provided final approval of the version to be submitted and
published. MF, YT, HO and SM confirm the authenticity of all the
raw data. All authors have read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: GLOBOCAN estimates of
incidence and mortality worldwide for 36 cancers in 185 countries.
CA Cancer J Clin. 74:229–263. 2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kohjimoto Υ, Uemura Η, Yoshida Μ, Hinotsu
S, Takahashi S, Takeuchi T, Suzuki K, Shinmoto H, Tamada T, Inoue
T, et al: Japanese clinical practice guidelines for prostate cancer
2023. Int J of Urol. 31:1180–1221. 2024.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Japanese Society for Radiation Oncology
(ed): JASTRO Guidelines 2024 for Radiotherapy Treatment Planning.
6th edition. Kanehara & Co., Ltd., Tokyo, 2024 (In Japanese).
https://www.kanehara-shuppan.co.jp/books/detail.html?isbn=9784307071314.
|
|
4
|
Kim JH, Jenrow KA and Brown SL: Mechanisms
of radiation-induced normal tissue toxicity and implications for
future clinical trials. Radiat Oncol J. 32:103–115. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Johnson CH, Patterson AD, Krausz KW, Lanz
C, Kang DW, Luecke H, Gonzalez FJ and Idle JR: Radiation
metabolomics. 4. UPLC-ESI-QTOFMS-Based metabolomics for urinary
biomarker discovery in gamma-irradiated rats. Radiat Res.
175:473–484. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
6
|
Goudarzi M, Weber WM, Mak TD, Chung J,
Doyle-Eisele M, Melo DR, Brenner DJ, Guilmette RA and Fornace AJ
Jr: Metabolomic and lipidomic analysis of serum from mice exposed
to an internal emitter, cesium-137, using a shotgun LC-MS(E)
approach. J Proteome Res. 14:374–384. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Chen CL, Chen YT, Liao WY, Chang YS, Yu JS
and Juo BR: Urinary metabolomic analysis of prostate cancer by
UPLC-FTMS and UPLC-Ion Trap MSn. Diagnostics (Basel).
13(2270)2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Obara H, Tatara Y, Monzen S, Murakami S,
Yamamoto H, Kimura N, Suzuki M, Komai F, Narita M, Hatayama Y and
Aoki M: Exploring predictive molecules of acute adverse events in
response to volumetric-modulated arc therapy for prostate cancer
using urinary metabolites. Mol Clin Oncol. 21(62)2024.PubMed/NCBI View Article : Google Scholar
|
|
9
|
National Cancer Institute: Common
Terminology Criteria for Adverse Events (CTCAE), Version 5.0.
Bethesda, MD: U.S. Department of Health and Human Services,
National Institutes of Health, 2017. https://dctd.cancer.gov/research/ctep-trials/for-sites/adverse-events/ctcae-v5-5x7.pdf.
|
|
10
|
Zhou G and Xia J: OmicsNet: A web-based
tool for creation and visual analysis of biological networks in 3D
space. Nucleic Acids Res. 46:W514–W522. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lass A, Zimmermann R, Haemmerle G,
Riederer M, Schoiswohl G, Schweiger M, Kienesberger P, Strauss JG,
Gorkiewicz G and Zechner R: Adipose triglyceride lipase-mediated
lipolysis of cellular fat stores is activated by CGI-58 and
defective in Chanarin-Dorfman Syndrome. Cell Metab. 3:309–319.
2006.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Hui DY and Howles PN: Carboxyl ester
lipase: Structure-function relationship and physiological role in
lipoprotein metabolism and atherosclerosis. J Lipid Res.
43:2017–2030. 2002.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Grant RW and Stephens JM: Fat in flames:
Influence of cytokines and pattern recognition receptors on
adipocyte lipolysis. Am J Physiol Endocrinol Metab. 309:E205–E213.
2015.PubMed/NCBI View Article : Google Scholar
|















![Venn diagram of rank-based metabolite
sets derived from patient-level Spearman’s rank correlation
coefficients (ρ). Metabolites were ranked according to the median ρ
between radiation fraction number and metabolite concentration
within each group. Four ranked sets were defined: Positive
correlation [AE(+)], positive correlation [AE(-)], negative
correlation [AE(-)] and negative correlation [AE(+)]. Overlaps
among these sets with opposing correlation directions between the
AE(+) and AE(-) groups were examined to identify metabolites
showing opposite directional correlation patterns. AE, adverse
event; negative correlation [AE(-)], top 60 negatively correlated
metabolites in the AE(-) group; negative correlation [AE(+)], top
60 negatively correlated metabolites in the AE(+) group; positive
correlation [AE(-)], top 60 positively correlated metabolites in
the AE(-) group; positive correlation [AE(+)], top 60 positively
correlated metabolites in the AE(+) group.](/article_images/mco/25/1/mco-25-01-02953-g00.jpg)