Introduction
The interaction between severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2) and autoimmune disease is an
emerging phenomenon, with numerous reports of patients with
COVID-19 developing autoantibodies and >10 distinct autoimmune
diseases (1,2). Thyroid disease is a common
manifestation, with cases of Graves' disease (3), Hashimoto's disease (3) and postpartum thyroiditis (4) subsequent to SARS-CoV-2 infection being
reported.
The present study reports a case of a patient who
experienced a relapse of Graves' disease following SARS-CoV-2
infection. In addition, this case is compared to similar reports
and the possible mechanisms underlying the association between
SARS-CoV-2 and Graves' disease are also discussed.
Case report
A 28-year-old female from mainland China, currently
residing in Trinidad, presented to the San Fernando General
Hospital (San Fernando, Trinidad and Tobago) in June, 2021 with a
19-day history of palpitations, increased sweating and tremors of
her hands. She had been diagnosed with COVID-19-related pneumonia
28 days earlier. Of note, 5 years prior, she had been treated for
Graves' disease medically; however, she had been biochemically
euthyroid and off anti-thyroid medications since 2019. Up to April,
2021, she was euthyroid: Free thyroxine (FT4), 13.2 pg/ml
(reference range, 8.9-17.2 pg/ml) and thyroid-stimulating hormone
(TSH), 1.1 µIU/ml (reference range, 0.3-4.5 µIU/ml) and a thyroid
ultrasound, also performed in April, 2021, had displayed a mildly
enlarged thyroid with no nodules.
In May, 2021, she presented to her local health
centre with a non-productive cough, fatigue and weakness. A
nasopharyngeal PCR swab test for SARS-CoV-2 yielded positive
results and she was diagnosed with COVID-19-related pneumonia. She
experienced palpitations, although she attributed these to the
intense fear from the diagnosis of COVID-19, as she was afraid she
would not survive. Her clinical status was followed via
telemedicine; her respiratory symptoms were treated symptomatically
and resolved within 5 days. However, her anxiety and palpitations
persisted. After 4 days, she began experiencing tremors and
increased sweating. She then presented to one of the authors (NM)
at San Fernando General Hospital, 28 days after her initial
diagnosis of COVID-19. A clinical examination revealed an anxious
female, with fine tremor of her hands, tachycardia (pulse, 120 bpm)
and a non-tender diffuse goitre with a bruit. There were no
dermatological or ocular features of Graves' disease. Thyroid
function tests were consistent with hyperthyroidism: Free
triiodothyronine (FT3), 18.3 pg/ml (reference range, 2.0-4.2
pg/ml), FT4, 46.2 pg/ml (reference range, 8.9-17.2 pg/ml) and TSH,
0.0 µIU/ml (reference range, 0.3-4.5 µIU/ml) (Table I). TSH receptor antibody (TR-Ab)
levels were elevated (3.2 mIU/ml; positive, >2.0 IU/l), as were
thyroid peroxidase antibody levels (42.5 IU/ml; reference range,
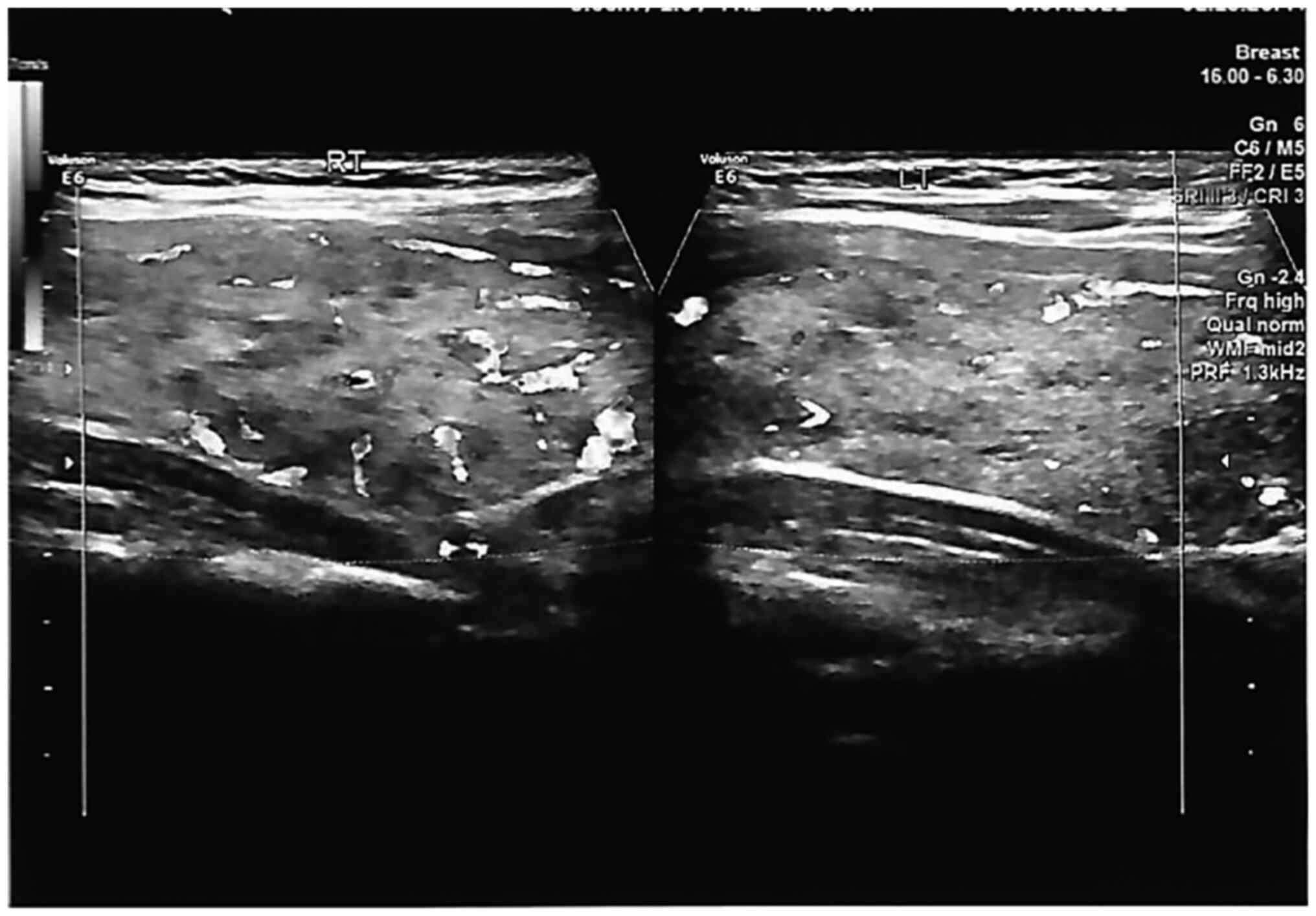
0.0-35.0 IU/ml). A thyroid ultrasound revealed a mildly enlarged
goitre with increased vascularity (Fig.
1 and Table II). Blood count,
erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
levels, and liver and renal functions were within normal limits.
She was diagnosed with a relapse of Graves' disease and began
treatment with carbimazole at 15 mg p.o., b.i.d. and atenolol at 50
mg once daily. The tremors, palpitations and increased sweating
ceased 1 week later, whilst her anxiety persisted for several weeks
before resolving. She has not reported any complications of
COVID-19 and was well at her last follow-up visit.
 | Table IThyroid function test results. |
Table I
Thyroid function test results.
| Test | Result | Reference rage | Flag |
|---|
| Thyroid stimulating
hormone | 0.0 | 0.3-4.5 µIU/ml | Low |
| Free T4 | 46.2 | 8.9-17.2 pg/ml | High |
| Free T3 | 18.3 | 2.0-4.2 pg/ml | High |
| Table IIThyroid ultrasound report. |
Table II
Thyroid ultrasound report.
| Thyroid ultrasound
characteristic | Description |
|---|
| Findings | The thyroid gland is
mildly enlarged and heterogeneous with diffusely increased
vascularity. The thyroid gland was larger than usual |
| | No retrosternal
extension or tracheal deviation |
| | The right lobe
measures 2.4x1.9x6.8 cm |
| | The left lobe
measures 2.4x2.4x6.8 cm |
| | The isthmus measures
0.4 cm AP |
| | There are bilateral,
small well-circumscribed, benign-appearing, hypoechoic thyroid
nodules measuring up to 0.8 cm with no dominant nodule on either
side |
| | Small reactive
anterior cervical lymph nodes were noted, measuring up to 0.3
cm |
| Impression | Moderately-enlarged
thyroid (larger than usual), with multiple well-defined, hypoechoic
nodules measuring up to 0.8 cm and diffusely increased vascularity.
These appearances are suggestive of Graves' disease |
Discussion
There have been isolated reports of either relapse
of, or newly diagnosed Graves' disease following the diagnosis of
SARS-CoV-2. The present study also conducted a literature search
evaluating these reports by searching PubMed and Google Scholar for
the following terms/keywords: ‘Graves' disease’, ‘SARS-CoV-2’ and
‘COVID-19’. The characteristics of the patients reported in the
literature are presented in Table
III.
| Table IIICharacteristics of the patients with
possible SARS-CoV-2-induced new onset, or relapse of, Graves'
disease identified in the literature. |
Table III
Characteristics of the patients with
possible SARS-CoV-2-induced new onset, or relapse of, Graves'
disease identified in the literature.
| Clinical
characteristic | Patient 1,
Mateu-Salat et al (5) | Patient 2,
Mateu-Salat et al (5) | Patient 3,
Jiménez-Blanco et al (6) | Patient 4,
Jiménez-Blanco et al (6) | Patient 5, Harris and
Mushref (7) | Patient 6, Lanzolla
et al (8) | Patient 7, Bayar
et al (9) | Patient 8, Khoury
et al (10) | Patient 9, Allam
et al (11) | Patient 10, Qureshi
and Bansal (12) | Patient 11 Montebello
(13) | Patient 12, Feghali
et al (3) |
|---|
| Age, years | 60 | 53 | 45 | 61 | 21 | 33 | 38 | 45 | 33 | 13 | 22 | 33 |
| Sex | Female | Female | Female | Female | Female | Female | Female | Male | Female | Male | Female | Female |
| Past thyroid
history | Graves' disease, in
remission for 35 years | None | 12-Year history of
Graves' disease. The patient relapsed on two occasions (2008 and
2015) and had one episode of Graves' ophthalmopathy in 2018.
Euthyroid prior to COVID-19 diagnosis | 17-Year history of
Graves' disease relapsed once in 2014 Euthyroid since 2016 | None | None | None | None | 9-Month history of
Graves' disease Euthyroid since January 2020 | None | Graves' disease since
2018 Biochemically euthyroid since September 2019 | None |
| Presenting
symptoms | Palpitations,
nervousness, fatigue | Asthenia, tremor,
palpitations | Palpitations,
nervousness | Palpitations | Tachycardia,
palpitations, anxiety and shortness of breath | Tachycardia, weight
loss, heat intolerance, nervousness | Asthenia, tremor,
palpitations | Palpitations,
light-headedness, dizziness | Bilateral ‘puffiness’
and proptosis of the eyes Weight loss, tremor | Fatigue, dizziness,
weight loss, difficulty sleeping, heat intolerance and an episode
of presyncope | Palpitations,
presyncope, hot flushes with associated chest tightness | Palpitations,
shortness of breath, fatigue. Thyroid ultrasound revealed mild
thyromegaly with heterogenous and diffusely hypervascular
appearance |
| Observations on
physical examination and investigations | No goitre | Non-tender
goitre | Hypervascularisation
of thyroid on ultrasound | Hypervascularisation
of thyroid on ultrasound | Mild diffuse
thyromegaly without tenderness, bilateral fine hand tremors and
hyperreflexia | Graves;
ophthalmopathy, | Non-tender
goitre | Tachycardia,
bilateral hand tremor. Atrial fibrillation on
electrocardiogram | Goitre with relative
diffuse reduction in vascularity and heterogenous parenchyma | Tachycardia,
thyromegaly, sinus tachycardia | Bilateral hand tremor
and increased ankle reflexes Pseudonodules and fibrous septations
throughout the thyroid noted on ultrasound | |
| Time to presentation
with symptoms following the diagnosis of COVID-19 | 35 Days after
positive IgG, 39 days after lung ultrasound compatible with
COVID-19 pneumonia | 34 Days after
confirmation by positive IgG, but 65 days after chest X-ray
compatible with COVID-19 pneumonia | Presented with
symptoms of COVID-19 and hyperthyroidism concurrently | ~1 Month | Unknown, three days
after resolution of symptoms of COVID-19 | ~2 Months | Within 2 months | 17 Days | Presented with
symptoms of COVID-19 and hyperthyroidism concurrently | 8 Weeks after
diagnosis of COVID-19 | ~8 Weeks | 7 Weeks |
| Treatment
administered | Thiamazole and
propranolol | Thiamazole and
propranolol | Methimazole 40 mg
daily - patient improved in three months Methimazole 5 mg daily
thereafter | Methimazole 10 mg
daily, patient was euthyroid three months later and continues with
5 mg daily | Selective beta
blocker twice daily, methimazole 30 mg daily for 3 months Since
then, thionamide titration with a planned trial discontinuation of
the beta blocker | Methimazole | Corticosteroid and
propranolol - the patient has leukopenia, thus anti-thyroid drugs
are contraindicated | Propranolol and
methimazole | Prednisolone (with
taper) and carbimazole | Methimazole 10 mg
daily for two months, after which propranolol 10 mg twice daily was
added | Carbimazole 40 mg
daily and propranolol 40 mg three times daily | Propranolol and
methimazole 10 mg |
| Time to resolution of
symptoms following the initiation of treatment | Unknown, improvement
of symptoms reported | Unknown, improvement
of symptoms reported | Three months after
treatment, her condition has improved | Euthyroid after three
months | Euthyroid after three
months | Unknown, improvement
of symptoms noted after treatment | Unknown, improvement
of symptoms noted after treatment | Biochemically
euthyroid 13 days later | Biochemically
euthyroid 3 months later | Biochemically
euthyroid 4 months later, but mixed thyroid and long COVID-19
symptoms persist | Unknown, biochemical
and physical improvement noted after 1 month of treatment but
worsened upon reduction of medication dosage. Currently well and on
carbimazole treatment | Symptomatic relief
within 2 weeks |
The majority of the patients identified in the
literature presented with symptoms of hyperthyroidism within 2
months of the diagnosis of COVID-19. In most cases, it is uncertain
how much time had elapsed between the resolution of the
COVID-19-related symptoms and the onset of hyperthyroid symptoms.
In the case presented herein, the patient's symptoms began 9 days
following the diagnosis of COVID-19. From the cases identified in
the literature, five had a history of thyroid disorders (Graves'
disease), although they were in remission, i.e., biochemically
euthyroid, similar to the patient in the present study. Most cases
reportedly experienced an improvement in symptoms soon after the
initiation of treatment. In the present case, the tremors,
palpitations and perspiration resolved within 1 week of treatment.
Graves' disease is the most common cause of hyperthyroidism, and it
is thus difficult to state with certainty that SARS-CoV-2 was the
cause of these cases, as the virus was not directly evidenced in
the thyroid tissue; the temporal relation suggests a role,
however.
It is well-established that viral infections can
contribute to the pathogenesis of autoimmune thyroid disorders
(14). Several plausible mechanisms
explaining the interplay between SARS-CoV-2 infection and Graves'
disease have been proposed. SARS-CoV-2 enters host cells via the
binding of its spike protein to angiotensin-converting enzyme-2
(ACE2) receptors and the subsequent recruitment of transmembrane
protease serine 2 (TMPRSS2) to facilitate cytoplasmic entry. The
thyroid gland expresses both ACE2 and TMPRSS2 in high quantities,
and this may allow SARS-CoV-2 to directly induce thyroid
dysfunction (15).
The levels of several cytokines, including IL-6,
IL-1β, TNF-α and IFN-γ are elevated in the hyperinflammatory state
induced by SARS-CoV-2. Croce et al (16) noted that these cytokines exert a
multitude of effects on the hypothalamic-pituitary-thyroid axis, on
circulating thyroid hormone binding proteins and the peripheral
metabolism of thyroid hormones. The pathogenesis of Graves' disease
is convoluted and the understanding of this disease is rapidly
increasing (17). The ‘cytokine
storm’ associated with SARS-CoV-2 may promote the hyperactivity of
the Th1/Th17 immune response (18).
Th17 lymphocytes synthesize several pro-inflammatory cytokines
which may play a role in direct tissue damage and contribute to
autoimmune disease (19). It has
been postulated that viral-induced Graves' disease may be mediated
by Th17(20). Elevated levels of
IL-6 have been reported in patients with Graves' disease (21) and a mechanistic link has been
proposed (17).
Psychological stress may contribute to the aetiology
of Graves' disease and may thus play a role in relapse (14), further confounding the relationship
between SARS-CoV-2 infection and thyroid disease.
Multiple plausible mechanisms may account for the
influence of SARS-CoV-2 on thyroid disease. One is a direct result
of viral uptake by thyroid cells (15), while another is a result of the
hyperinflammatory ‘cytokine storm’ and its effects on the
hypothalamic-pituitary-thyroid axis and T-cell immunity (16,18,19,20).
In conclusion, there is increasing evidence to
suggest that SARS-CoV-2 infection may be a precursor for autoimmune
disease. The present study reports the case of a 28-year-old female
of Chinese descent with a relapse of Graves' disease 28 days
following the diagnosis of COVID-19. Her symptoms began 9 days
after a positive nasopharyngeal PCR swab for SARS-CoV-2. Anecdotal
data may implicate SARS-CoV-2 as a trigger for relapse of, or new
onset Graves' disease.
It is thus recommended that clinicians follow-up
patients with COVID-19 with a previous history of autoimmune
thyroid disease, as it may trigger a relapse, as in this case.
Further research is required to elucidate the exact mechanism(s)
underlying the association between SARS-CoV-2 and autoimmune
conditions.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
NM and ST conceptualized the study. All authors
(SRM, MT, NM and ST) were involved in the design of the study, in
the writing, review and editing of the manuscript, as well as in
project administration. NM and ST supervised the study. SRM and MT
were involved in the writing of the original draft. SRM, MT and NM
were involved in obtaining medical images. NM, SRM, MT and ST were
involved in patient care/management. All authors (NM, SRM, MT and
ST) confirm the authenticity of all the raw data. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
Due to the present study being a retrospective case
report, ethical approval was not required. Informed consent was
obtained from the patient for all procedures conducted as part of
clinical care/management.
Patient consent for publication
The patient provided consent for the publication of
this report.
Competing interests
All authors declare that they have no competing
interests.
References
|
1
|
Dotan A, Muller S, Kanduc D, David P,
Halpert G and Shoenfeld Y: The SARS-CoV-2 as an instrumental
trigger of autoimmunity. Autoimmun Rev. 20(102792)2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Liu Y, Sawalha AH and Lu Q: COVID-19 and
autoimmune diseases. Curr Opin Rheumatol. 33:155–162.
2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Feghali K, Atallah J and Norman C:
Manifestations of thyroid disease post COVID-19 illness: Report of
Hashimoto thyroiditis, Graves' disease, and subacute thyroiditis. J
Clin Transl Endocrinol Case Rep. 22(100094)2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mizuno S, Inaba H, Kobayashi KI, Kubo K,
Ito S, Hirobata T, Inoue G, Akamizu T and Komiya N: A case of
postpartum thyroiditis following SARS-CoV-2 infection. Endocr J.
68:371–374. 2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Mateu-Salat M, Urgell E and Chico A:
SARS-COV-2 as a trigger for autoimmune disease: Report of two cases
of Graves' disease after COVID-19. J Endocrinol Invest.
43:1527–1528. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jiménez-Blanco S, Pla-Peris B and
Marazuela M: COVID-19: A cause of recurrent Graves'
hyperthyroidism? J Endocrinol Invest. 44:387–388. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Harris A and AI Mushref MA: Graves'
thyrotoxicosis following SARS-CoV-2 infection. AACE Clin Case Rep.
7:14–16. 2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lanzolla G, Marcocci C and Marinò M:
Graves' disease and Graves' orbitopathy following COVID-19. J
Endocrinol Invest. 44:2011–2012. 2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Bayar I, Tahri S, Hajji E, Ben AB, Sayadi
H, Héla M and Inès K: A case of Grave's disease following SARS-Cov
2 infection. Endocrine Abstracts. 73(AEP657)2021.
|
|
10
|
Khoury M, Tripathi P and Narayana S:
Abstract #1017450: COVID-19 Associated Grave's Disease Identified
in a 45-year-old Male. Endocrine Practice. 27:S186–S187. 2021.
|
|
11
|
Allam MM, El-Zawawy HT, Ahmed SM and Aly
Abdelhamid M: Thyroid disease and covid-19 infection: Case series.
Clin Case Rep. 9(e04225)2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Qureshi NK and Bansal SK: Autoimmune
thyroid disease and psoriasis vulgaris after COVID-19 in a male
teenager. Case Rep Pediatr. 2021(7584729)2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Montebello A: Recurrent Graves' disease
post SARS-CoV-2 infection. BMJ Case Rep. 14(e244714)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Marinò M, Latrofa F, Menconi F, Chiovato L
and Vitti P: Role of genetic and non-genetic factors in the
etiology of Graves' disease. J Endocrinol Invest. 38:283–294.
2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Duntas LH and Jonklaas J: COVID-19 and
thyroid diseases: A bidirectional impact. J Endocr Soc.
5(bvab076)2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Croce L, Gangemi D, Ancona G, Liboà F,
Bendotti G, Minelli L and Chiovato L: The cytokine storm and
thyroid hormone changes in COVID-19. J Endocrinol Invest.
44:891–904. 2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Rajaii F, McCoy AN and Smith TJ: Cytokines
as villains and potential therapeutic targets in thyroid-associated
ophthalmopathy: From bench to bedside. Expert Rev Ophthalmol.
9:227–234. 2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lania A, Sandri MT, Cellini M, Mirani M,
Lavezzi E and Mazziotti G: Thyrotoxicosis in patients with
COVID-19: The THYRCOV study. Eur J Endocrinol. 183:381–387.
2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Costela-Ruiz VJ, Illescas-Montes R,
Puerta-Puerta JM, Ruiz C and Melguizo-Rodríguez L: SARS-CoV-2
infection: The role of cytokines in COVID-19 disease. Cytokine
Growth Factor Rev. 54:62–75. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Murugan AK and Alzahrani AS: SARS-CoV-2
plays a pivotal role in inducing hyperthyroidism of Graves'
disease. Endocrine. 73:243–254. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Salvi M, Girasole G, Pedrazzoni M, Passeri
M, Giuliani N, Minelli R, Braverman LE and Roti E: Increased serum
concentrations of interleukin-6 (IL-6) and soluble IL-6 receptor in
patients with Graves' disease. J Clin Endocrinol Metab.
81:2976–2979. 1996.PubMed/NCBI View Article : Google Scholar
|