Introduction
Abdominal aortic aneurysm (AAA) is a critical public
health concern with a prevalence ranging from 12.5 in males to 5.2%
in females (1). Aneurysm rupture is
associated with high morbidity and mortality rates, while can be
prevented by early diagnosis and appropriate intervention (2) An aneurysm, a localized permanent and
irreversible dilatation of the artery, is most common in males
>65 years of age and is associated with a number of factors,
including smoking, genetic factors, positive family history, a lack
of regular exercise and malnutrition (3). If left untreated, the risk of mortality
from continued dilation and thinning of the vessel wall is 80 to
90% (4). The optimal screening
method for AAA is ultrasonography, which is inexpensive, accurate,
safe, rapid, non-invasive and cost-effective (1).
Case report
Patient information
A 78-year-old male patient presented to the Giresun
University Training and Research Hospital Family Medicine Unit
(Giresun, Turkey) with symptoms of frequent urination and a burning
sensation while urinating, and to have his blood pressure
medications prescribed.
Clinical findings
His medical history included known cardiovascular
disease, including coronary artery disease with previous myocardial
infarction and a three-vessel coronary artery bypass graft. He also
had a history of 41 pack years of tobacco use, hypertension,
obesity (body mass index, 29.22 kg/m2) and benign
prostatic hypertrophy. There was no known history of aortic
aneurysm. His vital signs were stable. The patient's blood pressure
was 130/86 mmHg, his pulse rate was 54/min, his respiratory rate
was 16/min, his oxygen saturation was 97% in room air and his body
temperature was 36.5˚C. The results of the physical examination
revealed natural lung auscultation, a regular heart rate and rhythm
and an obese abdomen with distension; no hepatosplenomegaly was
palpated. The patient had mild palpation discomfort in the
abdominal region and complaints of hematuria.
The laboratory results were generally normal. The
urea level was 38 mg/dl (16.6-48.5), the white blood cell count was
7.11x103/l and the hematocrit was 35%. The patient was
diagnosed with benign prostatic hyperplasia and a complete
urinalysis and upper urinary tract ultrasound were performed
according to his complaints.
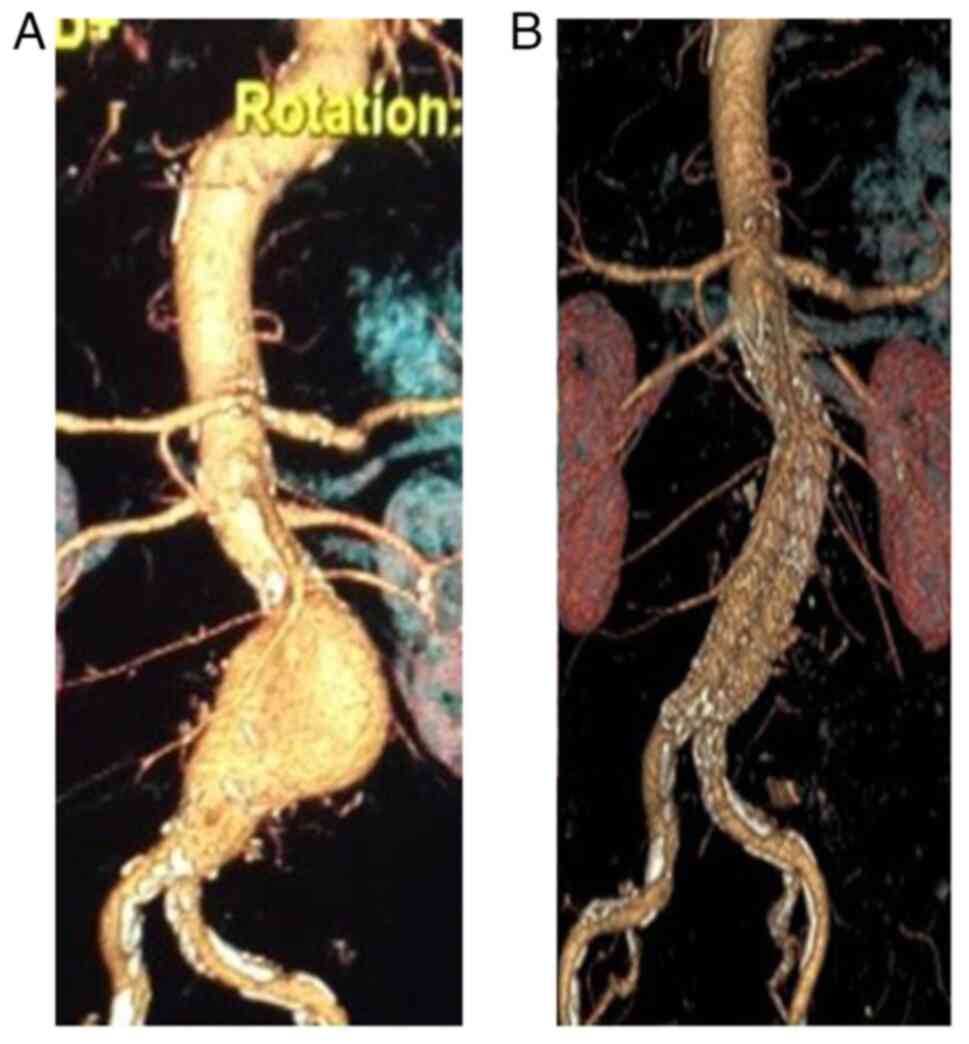
Diagnostic assessment
The diameter of the abdominal aorta at the
infrarenal level was measured as 7.5 cm. A contrast-enhanced
abdominal computerized tomography scan was performed for further
investigation and this revealed an aneurysmatic dilatation of the
abdominal aorta beginning inferior to the level of the renal
arteries and continuing to the iliac bifurcation, measuring 87 mm
at its widest point (Fig. 1A).
Therapeutic intervention
Endovascular abdominal aortic aneurysm repair (EVAR)
was planned under emergency conditions and an endovascular stent
graft was applied to the patient with an aneurysm diameter >87
mm. EVAR is a method used to repair abdominal aortic aneurysms
(4). Treatment with angiotensin 2
receptor blockers (1 per day/32 mg), acetylsalicylic acid (1 per
day/100 mg) and clopidogrel (1 per day/75 mg) was commenced. The
patient's general condition was good and his vital signs were
normal. His blood pressure was measured as 140/60 mmHg. After 3
months, the diameter of the aortic aneurysm decreased to 70 mm in
the follow-up with computed tomography (Fig. 1B). Lifestyle changes, such as
quitting smoking, exercise and a healthy diet were recommended. The
patient is currently being followed-up routinely by the Giresun
University Training and Research Hospital.
Discussion
AAA is defined as a permanent dilatation of the
abdominal aorta that is >3 cm in diameter and usually remains
asymptomatic until rupture (1). The
rupture of an AAA is usually fatal, with 25% of patients succumbing
before presenting to emergency services (2). Therefore, it is valuable to screen for
AAA in male patients >65 years of age with ultrasonography,
which is a simple and non-invasive method, taking into account the
atherosclerotic risk factor. The aim of the present study was to
contribute to future research on the role of common risk factors
such as hypertension, obesity, family history of AAA and to address
AAA screening to target the population at high risk. It is
recommended that males >66 years of age be informed about the
AAA screening program (5). The
Society for Vascular Surgery clinical practice guidelines
recommends ultrasound screening for AAA in all males >65 years
of age (6). The American College of
Preventive Medicine recommends 1-time screening in males 65 to 75
years of age who have ever been smokers; it does not recommend
routine screening in females (7).
The American College of Cardiology and the American Heart
Association jointly recommend 1-time screening for AAA with a
physical examination and an ultrasonography in males aged 65 to 75
years who have ever been smokers or in males ≥60 years who are the
sibling or offspring of an individual who has suffered an AAA
(8). Appropriate screening programs
for AAA reduce the mortality rates and are cost-effective (9).
In conclusion, with the continuous increase in life
expectancy, the importance of preventive health care is increasing.
Preventive health care is a fundamental aspect of modern medicine
and should be encouraged and supported in a health care system that
deals with the individual, not merely the disease itself, even if
the individual is healthy. Although AAA is associated with high
mortality rates when it ruptures, it is a preventable disease if
diagnosed at an early stage (2).
Preventive measures need to be promoted in a healthcare system that
takes care of the individual, even if the individual is in good
health (1). It is recommended that
the screening of individuals >65 years of age for AAA be
performed with ultrasonography, which is an inexpensive, accurate,
safe, rapid, non-invasive, reproducible and cost-effective
method.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed in the current
study are available from the corresponding author upon reasonable
request.
Author's contributions
AA designed and concaved the study, and wrote the
manuscript. AA visited the patient and was in charge of the
clinical follow-up. AA confirms the authenticity of all the raw
data. The author has read and approved the final manuscript.
Ethics approval and consent to
participate
The patient provided written informed consent for
participation in the study. All procedures performed in the present
protocol were in accordance with the Declaration of Helsinki.
Patient consent for publication
The patient provided written informed consent for
the publication of his data.
Competing interests
The author declares that she has no competing
interests.
References
|
1
|
Altobelli E, Rapacchietta L, Profeta VF
and Fagnano R: Risk factors for abdominal aortic aneurysm in
population-based studies: A systematic review and meta-analysis.
Int J Environ Res Public Health. 15(2805)2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Koç MA, Çetinkaya OA, Üstüner E, Peker AG,
Uungan M and Bengisun U: Abdominal aortic aneurysm screening: A
pilot study in Turkey. Ulus Travma Acil Cerrahi Derg. 27:17–21.
2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sakalihasan N, Michel JB, Katsargyris A,
Kuivaniemi H, Defraigne JO, Nchimi A, Powell JT, Yoshimura K and
Hultgren R: Abdominal aortic aneurysms. Nat Rev Dis Primers.
4(34)2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bakewell R, Krokidis M and Winterbottom A:
Endovascular abdominal aortic aneurysm repair: Overview of current
guidance, strategies, and new technologies, perspectives from the
United Kingdom. J Clin Med. 11(5415)2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
NICE guideline [NG156]. Abdominal aortic
aneurysm: diagnosis and management. Acceced on August 2, 2023.
https://www.nice.org.uk/guidance/ng156.
|
|
6
|
Chaikof EL, Brewster DC, Dalman RL,
Makaroun MS, Illig KA, Sicard GA, Timaran CH, Upchurch GR Jr and
Veith FJ: Society for Vascular Surgery. The care of patients with
an abdominal aortic aneurysm: The society for vascular surgery
practice guidelines. J Vasc Surg. 50 (4 Suppl):S2–S49.
2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lim LS, Haq N, Mahmood S and Hoeksema L:
ACPM Prevention Practice Committee; American College of Preventive
Medicine. Atherosclerotic cardiovascular disease screening in
adults: American college of preventive medicine position statement
on preventive practice. Am J Prev Med. 40:381.e1–381.e10.
2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hirsch AT, Haskal ZJ, Hertzer NR, Bakal
CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW,
Puschett JB, et al: ACC/AHA 2005 practice guidelines for the
management of patients with peripheral arterial disease (lower
extremity, renal, mesenteric, and abdominal aortic): A
collaborative report from the American association for vascular
Surgery/Society for vascular surgery, society for cardiovascular
angiography and interventions, society for vascular medicine and
biology, society of interventional radiology, and the ACC/AHA task
force on practice guidelines (Writing Committee to Develop
Guidelines for the Management of Patients With Peripheral Arterial
Disease): Endorsed by the American association of cardiovascular
and pulmonary rehabilitation; national heart, lung, and blood
institute; society for vascular nursing; TransAtlantic
inter-society consensus; and vascular disease foundation.
Circulation. 113:e463–e654. 2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Stather PW, Dattani N, Bown MJ, Earnshaw
JJ and Lees TA: International variations in AAA screening. Eur J
Vasc Endovasc Surg. 45:231–234. 2013.PubMed/NCBI View Article : Google Scholar
|