Introduction
The chronic and progressive nature of knee
osteoarthritis (OA) often results in a poor quality of life, and
the disability created by this joint disease creates a significant
social and economic burden for both patients and caregivers
(1). In the past, OA was only
considered to be a degenerative joint disease; however, recent
research has demonstrated a more complex pathogenesis, which has
encouraged the development of new treatment strategies. There is
currently no cure for OA, and the available treatments mainly focus
on symptom relief and improving disability rather than halting
progression of the disease (2). For
optimal management of knee OA, a combination of non-pharmacological
and pharmacological modalities is required, and surgery is
recommended for intractable cases (3). The pharmacological and
non-pharmacological treatment options for the management of knee OA
include changes to daily living activities, weight loss through
dietary interventions and exercise, manual therapy, physical
therapy, electrotherapy [transcutaneous electrical nerve
stimulation (TENS), therapeutic ultrasound (US) and the use of
lasers], taping, the use of assistive devices, bracing,
non-steroidal anti-inflammatory drugs, acetaminophen, opioids and
injection therapies (dextrose prolotherapy, ozone, platelet-rich
plasma and hyaluronic acid) (4,5).
Prolotherapy is as a non-surgical regenerative
technique, in which small amounts of an irritant solution are
injected to the site of painful or degenerated tendon insertions,
joints, ligaments and adjacent joint spaces, with the aim of
promoting normal cell and tissue growth (6). Hypertonic dextrose at concentrations of
12.5 to 25% is the most widely used prolotherapy solution, and
multiple clinical trials have reported favorable outcomes. For
several decades, musculoskeletal pain has been treated with
intra-articular or extra-articular injections of dextrose
infiltration over ligament and tendon insertions. Previous
controlled trials have reported that these treatments with
hypertonic dextrose prolotherapy (HDP) are effective in patients
with symptomatic knee degeneration. For example, in a previous
randomized controlled trial, 90 adults who had been experiencing
painful knee OA for a minimum of 3 months were randomly assigned to
one of three groups: Blinded prolotherapy, saline injections, or
at-home exercise. The participants were then followed-up with
visits at the 52-week mark. Upon follow-up, individuals who
underwent dextrose prolotherapy exhibited better WOMAC scores
compared to those who received saline injections or engaged in
at-home exercise. Moreover, the patients who received dextrose
prolotherapy reported high levels of satisfaction (7). Reeves and Hassanein (8) conducted a study involving patients with
knee laxity who underwent dextrose prolotherapy treatment. Their
findings revealed that following a 12-month follow-up period, the
group receiving the treatment exhibited notable enhancement in
laxity when compared to the control group (8). Although the mechanisms of prolotherapy
are not yet fully understood, some researchers have provided
results supporting the theory that HDP injection triggers an
inflammatory cascade following cell shrinkage, which then increases
the release of collagen deposition and growth factors (9). The aim of the present study was to
compare the efficacy of HDP with conventional physiotherapy (CPT)
in improving pain, movement restriction, walking speed, activities
of daily living and isokinetic muscle performance in female
patients with knee OA.
Patients and methods
Study participants
The present study with a randomized prospective
study which included a total of 60 female patients with a confirmed
diagnosis of knee OA in accordance with the Kellgren-Lawrence
criteria (10), who were referred to
the PM&R outpatient clinic of Hatay Mustafa Kemal University
Medical School (Antakya, Turkey) between July, 2020 and December,
2021. The main inclusion criterion was the radiographically
confirmed presence of mechanical knee pain, around the knee joint,
which had been ongoing for at least 3 months. The study exclusion
criteria were defined as an age <50 years, the presence of an
inflammatory rheumatological disease, grade 1 or 4 OA based on the
Kellgren-Lawrence radiological criteria, a history of knee surgery
or joint replacement, trauma, any intra-articular injection
(hyaluronic acid, steroids or platelet-rich plasma) over the past 6
months, malignancy, or any other neurological disorder that could
contribute to the symptoms. Approval for the present study was
granted by the Medical Ethics Committee of Hatay Mustafa Kemal
University (decision no. 2020/75). Written informed consent was
provided by all the study participants. The present study was
registered in the ClinicalTrials.gov database (NCT04958213).
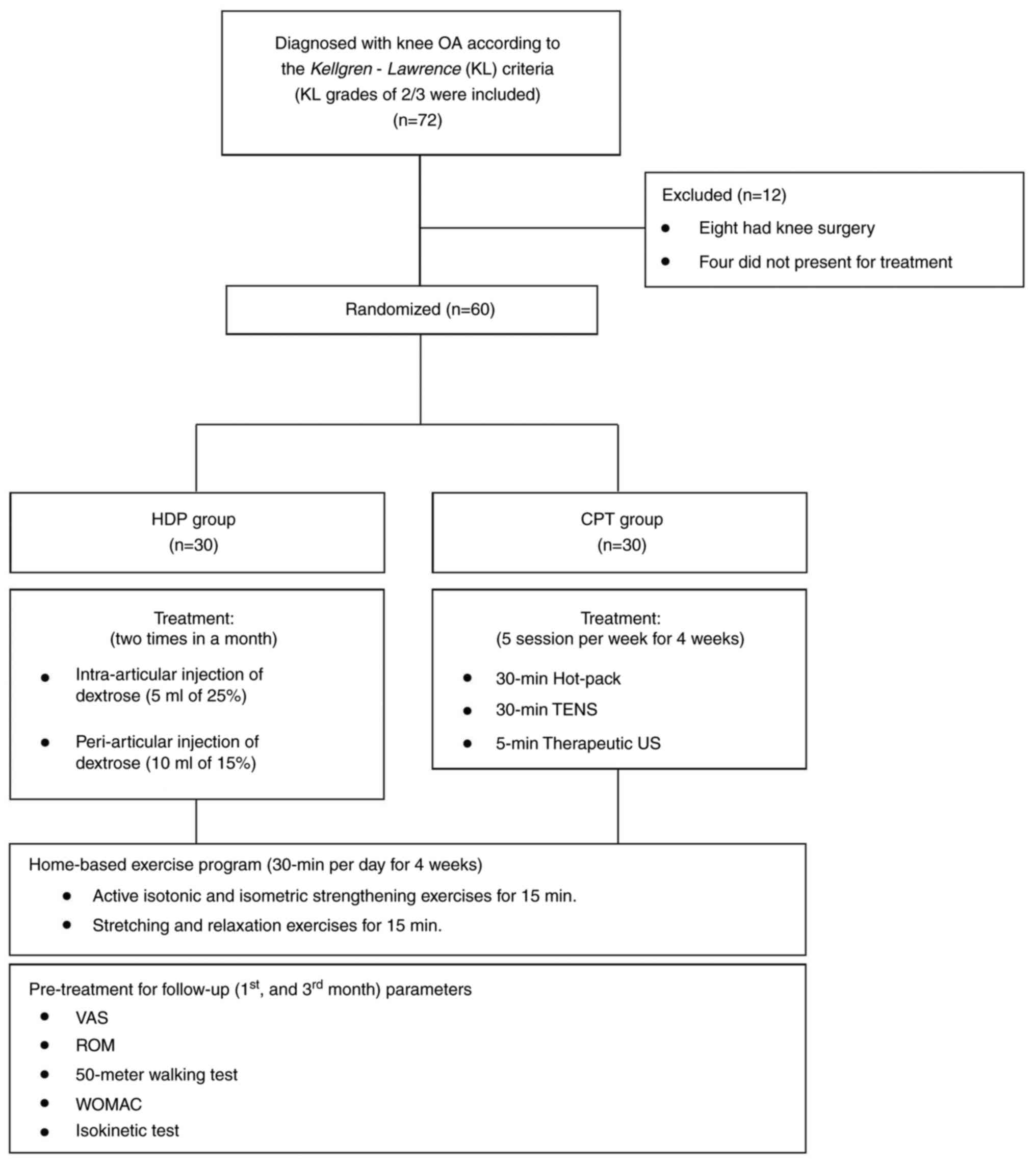
The patients were assigned to the HDP or CPT group
using a simple randomization method using a table of random
numbers, assigning 30 patients to each group. All the patients had
been recommended to perform knee exercises for 1 month. Throughout
the study period, the patients were requested not to take any
painkillers, but were permitted to take paracetamol if deemed
necessary. The study flowchart is presented in Fig. 1.
HDP
The procedure was performed by a qualified physical
medicine and rehabilitation physician. With the patient placed in
the supine position, and the knee was placed at 20-30˚ flexion, the
injection area on the lateral side of the knee was identified.
Using a 27-G needle, aspiration and correct needle placement in the
joint were ensured, and the injection was then performed. In the
HDP group, all the patients received an intra-articular injection
of 5 ml 25% dextrose (2.5 ml 20% dextrose + 2.5 ml 30% dextrose),
and a peri-articular injection of 10 ml 15% dextrose (5 ml 0.9%
NaCl + 5 ml 30% dextrose) to each ligament-bone insertion. The
injection sites were identified using anatomic landmarks; two
injections were performed at a 2-week interval. The injection
points were designated as the medial and lateral coronary
ligaments, proximal and distal medial and lateral collateral
ligaments, the quadriceps tendon region of the patella upper edge,
and the distal and proximal region of the patellar tendon, and the
tendon region of pes anserine (Fig.
2). In the HDP group, mild warmth and redness around the knee
were observed for 3 days in 2 patients after the injection;
however, this condition improved without any issues during the
follow-up.
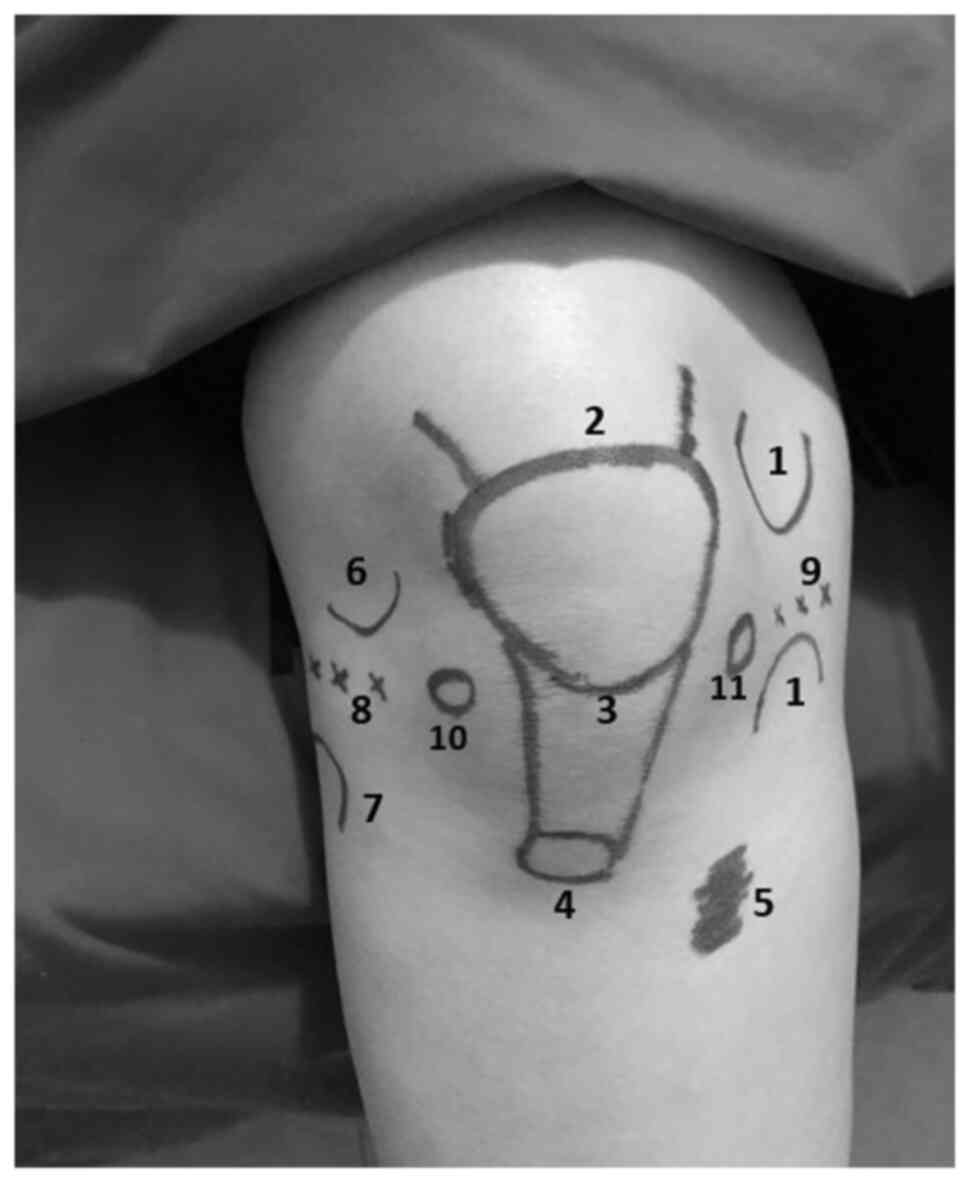 | Figure 2The figure shows schematically
possible prolotherapy points in a healthy model. The injection
sites used for hypertonic dextrose prolotherapy. 1, proximal and
distal medial collateral ligament; 2, quadriceps tendon region of
the patella upper edge; 3, proximal region of the patellar tendon;
4, distal of the patellar tendon; 5, tendon region of pes anserine;
6, proximal lateral collateral ligament; 7, distal lateral
collateral ligament; 8, lateral coronary ligament; 9, medial
coronary ligament; 10 and 11, intra-articular injection sites. |
CPT
In the CPT group, all the patients received combined
hot pack (HP), US and TENS treatments. A physical therapy program
was applied to patients in the CPT group 5 days a week for 4 weeks
as a total of 20 sessions. Using a two-channel portable TENS unit
(BTL-4620, BTL Corporate), TENS therapy was applied around the knee
region for 30 min with two electrodes in conventional mode, at a
frequency of 100 Hz and a pulse width of 60 msec and intensity
adjusted according to the threshold for each patient without
causing pain or muscular contraction. US sessions of 5 min
continuously were performed 5 days a week for 4 weeks for a total
of 20 sessions, using a power of 1 W/cm2, and frequency
of 1 MHz (BTL-4000 Professional, BTL Corporate). HP therapy was
applied for 30 min per session for a total of 20 sessions as a part
of the conventional physiotherapy.
Exercise
A home-based exercise program was performed by all
the patients in both groups 5 days a week for 4 weeks. The program
included active isotonic and isometric strengthening exercises for
15 min, and stretching and relaxation exercises for 15 min.
Outcome evaluations
Before treatment, and at 1 and 3 months after the
final injection, both groups completed the standard questionnaire
including the Western Ontario and McMaster Universities Arthritis
Index (WOMAC) (11), and visual
analog scale (VAS).
The severity of pain felt in the knee was measured
using the VAS scores ranging from 0 (no pain) to 10 (worst possible
pain). The WOMAC scale was used to evaluate the functional status
of the patients. WOMAC is a measure of performance that examines
three categories of function, including pain (five items) and
physical function (17 items). Each item is scored as follows: None,
0; mild, 1; moderate, 2; severe, 3; or very severe, 4, with lower
scores indicating a better condition. Active knee joint range of
movement (ROM) was measured using a manual universal goniometer,
the 50-meter walking time, and the measurements of isokinetic knee
extensor/flexor muscle peak torque (PT). These evaluations were
made prior to treatment, and at 1 and 3 months post-treatment.
Isokinetic muscle strength was measured using the
Humac® NORM isokinetic dynamometer (Computer Sports
Medicine Inc.). The extensor and flexor muscles of the affected
knee of the patients in both groups were evaluated with isokinetic
tests prior to treatment, and at 1 and 3 months post-treatment.
Each patient was seated on the dynamometric chair and stabilized
with waist and chest belts in a 90˚ sitting position for the
isokinetic measurement. Following five submaximal warm-up
contractions, an evaluation was made of the concentric PT values of
the quadriceps and hamstring at 60 and 180˚ per second angular
velocities. The protocol for the isokinetic test protocol was five
repetitions at 60˚ per second, 30 sec of rest, and 15 repetitions
at 18˚ per second.
Statistical analysis
The data obtained in the present study were analyzed
statistically using SPSS version 22.0 software (IBM Corp.).
Descriptive statistical results are presented as the mean ±
standard deviation (SD) values for continuous data, and as number
and percentage for categorical data. Demographic data were analyzed
using the independent samples t-test for continuous variables and
the Chi-squared test for categorical variables. The differences in
the scores of each group at the different times measured were
analyzed using the repeated measures analysis of variance (ANOVA)
test. Following repeated measures ANOVA, the paired t-test with the
Bonferroni correction was used. Differences between the groups were
compared using the independent samples t-test. A value of P<0.05
was considered to indicate a statistically significant
difference.
The power of the study was calculated using the
G*Power 3.1.9.4 program after the study. In the evaluation using
the difference between two independent means, the power of the
study was found to be 99%. The effect size was calculated as 1.26
using the post-treatment VAS parameter.
Results
No statistically significant differences were
determined between the groups as regards age, weight, height, body
mass index, symptom duration, Kellgren-Lawrence grade, VAS at rest,
knee ROM, the 50-m walking test, WOMAC and isokinetic muscle
performance values (P>0.05 for all). The demographic, clinical,
radiographic and isokinetic data are presented in Table I.
 | Table IDemographic and clinical features of
the groups of patients. |
Table I
Demographic and clinical features of
the groups of patients.
| Parameter | HDP (n=30) | CPT (n=30) | P-value |
|---|
| Age, years | 60.07±6.82 | 60.60±6.10 | 0.751 |
| Weight, kg | 81.07±13.52 | 77.60±8.66 | 0.242 |
| Height, cm | 159.23±5.38 | 158.40±5.34 | 0.550 |
| Symptom duration,
months | 18 (1-240) | 21 (6-48) | 0.893 |
| Body mass index,
kg/m2 | 31.84±5.19 | 30.88±2.83 | 0.380 |
| Kellgren-Lawrence,
grade n (%) | | | |
|
Grade 2 | 13 (43.3) | 16 (53.3) | 0.596 |
|
Grade 3 | 17 (56.7) | 14 (46.7) | |
| Baseline
evaluations | | | |
|
VAS for
pain | 7.33±1.34 | 7.20±1.42 | 0.748 |
|
50 m walking
test | 52.30±6.32 | 54.10±6.83 | 0.294 |
|
Range of
motion | 123.33±3.77 | 123.53±3.36 | 0.829 |
|
WOMAC, total
scores | 59.83±11.23 | 60.70±10.45 | 0.758 |
| Isokinetic
evaluation, PT (Nm) | | | |
|
60˚/sec AV -
extensor | 43.37±16.63 | 39.63±17.49 | 0.400 |
|
60˚/sec AV -
flexor | 17.57±10.29 | 21.90±13.01 | 0.158 |
|
180˚/sec AV
- extensor | 29.27±9.25 | 30.27±10.66 | 0.699 |
|
180˚/sec AV
- flexor | 11.67±6.84 | 19.90±9.60 | 0.001 |
In both the HDP and CPT groups, there were
statistically significant differences between pre- and
post-treatment (at 1 and 3 months) in terms of the clinical
assessments: VAS (P<0.001), ROM (P<0.001), WOMAC
(P<0.001), 50-m walking test (P<0.001) and isokinetic
parameters (P<0.001) (Tables II
and III). Comparisons between the
groups of the VAS, WOMAC and isokinetic parameters revealed
significant differences between the HDP and the CPT groups as
regards the VAS score and flexor PT (180˚/sec AV) at 1 and 3 months
post-treatment, and in the 50-m walking test scores at 3 months
post-treatment (Tables II and
III). Significantly greater
improvements were observed in the HDP group compared with the CPT
group as regards the VAS, WOMAC and extensor PT (60˚/sec AV) at 1
and 3 months post-treatment Table
IV).
| Table IIBaseline and after treatment (at 1 and
3 months) follow-up results of the clinical measurements of the
groups. |
Table II
Baseline and after treatment (at 1 and
3 months) follow-up results of the clinical measurements of the
groups.
| Parameter | HDP (n=30) | CPT (n=30) | P-value |
|---|
| | Mean ± SD | |
| VAS for pain | | | |
|
Baseline | 7.33±1.34 | 7.20±1.42 | 0.748 |
|
After
treatment | | | |
|
1st
month |
4.47±1.77a |
5.60±1.22a | 0.006 |
|
3rd
month |
2.43±1.85a,b |
4.40±1.03a,b | 0.001 |
| Knee ROM
(degree) | | | |
|
Baseline | 123.33±3.77 | 123.53±3.36 | 0.829 |
|
After
treatment | | | |
|
1st
month |
124.43±3.66a |
124.50±3.40a | 0.942 |
|
3rd
month |
126.20±3.47a,b |
125.60±3.50a,b | 0.508 |
| WOMAC (total
score) | | | |
|
Baseline | 59.83±11.23 | 60.70±10.45 | 0.758 |
|
After
treatment | | | |
|
1st
month |
55.77±11.35a |
58.20±10.78a | 0.398 |
|
3rd
month |
51.93±11.13a,b |
55.93±10.84a,b | 0.164 |
| 50-m walking test
(sec) | | | |
|
Baseline | 52.30±6.32 | 54.10±6.83 | 0.294 |
|
After
treatment | | | |
|
1st
month |
49.57±6.06a |
52.07±6.77a | 0.137 |
|
3rd
month |
46.97±6.23a,b |
50.40±6.79a,b | 0.046 |
| Table IIIBaseline and after treatment (at 1
and 3 months) follow-up results of isokinetic parameters of the
groups. |
Table III
Baseline and after treatment (at 1
and 3 months) follow-up results of isokinetic parameters of the
groups.
| Parameter | HDP (n=30) | CPT (n=30) | P-value |
|---|
| | Mean ± SD | |
| Extensor PT | | | |
|
60˚/sec AV
(Nm) | | | |
|
Baseline | 43.37±16.63 | 39.63±17.49 | 0.400 |
|
After
treatment | | | |
|
1st
month |
53.10±17.06a |
46.70±18.37a | 0.167 |
|
3rd
month |
63.17±16.84a,b |
54.67±16.89a,b | 0.056 |
|
180˚/sec AV
(Nm) | | | |
|
Baseline | 29.27±9.25 | 30.27±10.66 | 0.699 |
|
After
treatment | | | |
|
1st
month |
37.30±9.24a |
39.57±12.32a | 0.424 |
|
3rd
month |
47.73±10.55a,b |
46.03±11.91a,b | 0.561 |
| Flexor PT | | | |
|
60˚/sec AV.
(Nm) | | | |
| Baseline | 17.57±10.29 | 21.90±13.01 | 0.158 |
| After
treatment | | | |
|
1st
month |
23.73±11.83a |
28.50±15.99a | 0.195 |
|
3rd
month |
32.27±15.38a,b |
37.00±21.00a,b | 0.324 |
|
180˚/sec AV.
(Nm) | | | |
| Baseline | 11.67±6.84 | 19.90±9.60 | 0.001 |
| After
treatment | | | |
|
1st
month |
17.67±7.41a |
28.80±12.61a | 0.001 |
|
3rd
month |
25.77±10.08a,b |
35.30±15.24a,b | 0.006 |
| Table IVComparison of the differences between
the scores of the groups. |
Table IV
Comparison of the differences between
the scores of the groups.
| Δ% | BT to AF (1
month) | BT to AF (3
months) | AF (1 month) to AF
(3 months) |
|---|
| | Mean ± SD | |
| VAS for pain | | | |
|
HDP | 1.86±1.00 | 3.90±1.24 | 2.03±0.71 |
|
CPT | 1.60±0.49 | 2.80±0.76 | 1.20±0.40 |
|
P-value | 0.001 | 0.001 | 0.001 |
| WOMAC | | | |
|
HDP | 4.06±1.66 | 7.90±2.29 | 3.83±2.18 |
|
CPT | 2.50±0.86 | 4.761.43 | 2.26±1.17 |
|
P-value | 0.001 | 0.001 | 0.001 |
| Extensor PT,
60˚/sec AV | | | |
|
HDP | -9.73±5.53 | -19.80±8.03 | -10.06±5.70 |
|
CPT | -7.06±3.05 | -15.03±4.03 | -7.96±3.32 |
|
P-value | 0.010 | 0.001 | 0.001 |
| Extensor PT,
180˚/sec AV | | | |
|
HDP | -8.03±5.34 | -18.46±8.07 | -10.43±4.70 |
|
CPT | -9.30±3.71 | -15.76±4.63 | -6.46±2.52 |
|
P-values | 0.202 | 0.005 | 0.001 |
| Flexor PT, 60˚/sec
AV | | | |
|
HDP | -6.16±5.98 | -14.70±9.91 | -8.53±5.80 |
|
CPT | -6.60±5.28 | -15.10±9.47 | -8.50±5.52 |
|
P-value | 0.930 | 0.128 | 0.911 |
| Flexor PT, 180˚/sec
AV | | | |
|
HDP | -6.00±4.57 | -14.10±6.94 | -8.10±5.18 |
|
CPT | -8.90±5.09 | -15.40±7.42 | -6.50±3.97 |
|
P-value | 0.001 | 0.840 | 0.001 |
Discussion
The aim of the present study was to compare the
efficacy of HDP and CPT in patients with knee OA. The results
demonstrated that both groups achieved successful outcomes, as
measured by the lower WOMAC and VAS scores, and increased knee ROM
and muscle strength. The efficacy of HDP was found to be more
prominent than that of CPT, as regards VAS, WOMAC and ROM. When the
two groups were compared, it was found that at the end of the 1st
month, HDP was more effective than CPT in terms of VAS scores and
isokinetic parameters (flexor PT at 180˚/sec AV) and at the end of
the 3rd month, HDP was found to be more effective CPT in three
parameters (VAS, 50-m walking test and flexor PT at 180˚/sec
AV).
It has been stated that the more common treatment,
CPT, is safe and effective in cases of knee OA, particularly as
regards reducing pain, improving function and developing muscle
strength. The current therapy for rehabilitation of knee OA focuses
on reducing pain and improving function and joint ROM (12). CPT management includes thermal
modalities that decrease spasms and pain, and help to improve joint
ROM, and electrotherapy, which includes TENS, US and exercise
(13). According to a previous
systematic review that evaluated the efficacy of CPT in knee OA,
thermotherapy, electrotherapy and exercise therapy resulted in
reduced pain and improved function (14). The results of the present study
demonstrated that CPT had positive effects on a number of
parameters in patients with knee OA at 1 and 3 months
post-treatment. Previous randomized clinical trials of patients
with knee OA have reported a greater efficacy of HDP in terms of
pain relief and improvement in function compared with conservative
treatments (physiotherapy or exercise programs) (15,16). The
most likely reason for this effect is that HDP provides an
analgesic effect based on both neurogenic mechanisms and through
the repair of soft tissues and cartilage.
Prolotherapy is an injection therapy which is used
in the treatment of chronic painful musculoskeletal conditions,
including knee OA. The results of other randomized controlled
trials, systematic reviews and meta-analyses have demonstrated an
improvement in knee pain, function and stiffness scores in patients
with knee OA of a moderate-to-severe degree (2,7,17-19).
The standard injection protocol for prolotherapy includes a
whole-joint approach with both intra-articular and extra-articular
injections to the bony soft tissue attachments (20). In many studies that have investigated
HDP used for the treatment of knee OA, the effectiveness has been
compared with other treatments. A systematic review released in
2019 concurred that prolotherapy demonstrated superior
effectiveness compared to local anesthetic infiltrations in terms
of reducing pain and enhancing functional improvement (21). In addition, in that review,
prolotherapy exhibited similarity to hyaluronic acid, ozone, or
radiofrequency infiltrations, but showed lower efficacy compared to
platelet-rich plasma (PRP) and erythropoietin over the short,
medium, and long-term durations, according to available research
(21). In another study, the
intra-articular dextrose concentration used has ranged from 10 to
25%, with wide variations in the number of injections, break
durations and follow-up periods (2).
HDP has been shown to have a more beneficial effect than saline and
home-based exercise therapies (7)
and a similar effect to that of PRP in reducing pain (17). As it is simple to implement, the
WOMAC scale is the most frequently used patient-reported outcome
for knee OA. In the present study, both the HDP and CPT groups
exhibited significant improvements in the WOMAC scores at 1 and 3
months post-treatment, compared to the baseline scores, with no
apparent superiority of one treatment method over the other.
The currently proposed mechanisms of action are
focused on the generation of low-grade inflammation related to the
injection of hyperosmolar solutions. This process primarily relies
on the generation of cytokines (22). At the fibro-osseous junction of
ligaments and tendons, this inflammation leads to a healing cascade
of various paracrine pathways relating to cell growth and repair.
The direct needling of the tissue may also stimulate repair, with
the disruption of cellular membranes and local blood supply
resulting in the release of healing and inflammatory blood factors,
such as calcitonin gene-related protein (CGRP), bradykinin and
prostaglandins (23). The direct
injection of hyperosmotic solutions, such as dextrose may also
promote the activation of pain receptors, such as the capsaicin
pain receptor. The upregulation of these channels results in an
increase in substance P, CGRP and nitric oxide, which are
considered to have a suppressive effect on receptors. In addition,
the transmission of pain via the alpha-delta nerve fiber may result
in endogenous opioid-mediated pain suppression, as described in the
gate-control theory (22,23).
The evaluation of muscle performance with the
isokinetic test is an objective method that is frequently used. The
isokinetic test has been shown to be a valid and reliable
measurement of the strength of the knee flexor and extensor muscles
(24). Low angular velocity tests
are more accurate in the measurement of muscle strength and high
angular velocity tests are used to evaluate the muscle function and
endurance (25,26). The tests used in the present study
were 60˚/sec and 180˚/sec angular velocity. The presence of knee OA
is known to reduce isometric knee strength and this will worsen
with disease severity. Functional measurements have been shown to
be associated with knee strength measurements performed with
isokinetic dynamometers (27,28).
Both groups in the present study exhibited improved results in the
isokinetic test following treatment. Based on these findings, it
can be ascertained that HDP and CPT may increase muscle strength in
patients with knee OA.
There were several limitations to the present study.
First, the present study did not examine whether the patients with
OA performed the home-based exercise program regularly. Secondly,
the patients were not questioned about their history of drug use.
Thirdly, patients with mild and severe OA (Kellgren-Lawrence grade
I and IV) were excluded from the study. Finally, the 3-month period
of treatment may not have been sufficient for a definitive
evaluation of muscle performance.
In conclusion, in light of the results of the
present study, both HDP and CPT may be considered effective
treatment modalities to reduce pain, and increase functionality and
strength in patients with knee OA. However, prolotherapy was
observed to have led to more notable improvements in pain and
functionality.
Acknowledgements
Not applicable.
Funding
Funding: Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request. The present study was registered in the ClinicalTrials.gov database (NCT04958213).
Authors' contributions
All authors (KMY, MTY, HO, HG and ADT)
conceptualized the study. KMY, MTY and HO made a substantial
contribution to data analysis and interpretation, and wrote and
prepared the draft of the manuscript. HG and ADT analyzed the data
and provided critical revisions. HG and ADT confirm the
authenticity of all the data. All authors contributed to manuscript
revision, and have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Approval for the present study was granted by the
Medical Ethics Committee of Hatay Mustafa Kemal University
(decision no. 2020/75). Written informed consent was provided by
all the patients.
Patient consent for publication
The patient provided verbal consent for publication
and for her data and any related images in the present study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Uysal A, Yildizgoren MT, Guler H and
Turhanoglu AD: Effects of radial extracorporeal shock wave therapy
on clinical variables and isokinetic performance in patients with
knee osteoarthritis: A prospective, randomized, single-blind, and
controlled trial. Int Orthop. 44:1311–1319. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wee TC, Neo EJR and Tan YL: Dextrose
prolotherapy in knee osteoarthritis: A systematic review and
meta-analysis. J Clin Orthop Trauma. 19:108–117. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kolasinski SL, Neogi T, Hochberg MC, Oatis
C, Guyatt G, Block J, Callahan L, Copenhaver C, Dodge C, Felson D,
et al: 2019 American College of rheumatology/arthritis foundation
guideline for the management of osteoarthritis of the Hand, Hip,
and Knee. Arthritis Care Res (Hoboken). 72:149–162. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Öğüt H, Güler H, Yıldızgören MT, Velioğlu
O and Turhanoğlu AD: Does kinesiology taping improve muscle
strength and function in knee osteoarthritis? A single-blind,
Randomized and controlled study. Arch Rheumatol. 33:335–343.
2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Basedow M, Runciman WB, March L and
Esterman A: Australians with osteoarthritis; the use of and beliefs
about complementary and alternative medicines. Complement Ther Clin
Pract. 20:237–242. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Reeves KD, Sit RW and Rabago DP: Dextrose
prolotherapy: A narrative review of basic science, clinical
research, and best treatment recommendations. Phys Med Rehabil Clin
N Am. 27:783–823. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Rabago D, Patterson JJ, Mundt M, Kijowski
R, Grettie J, Segal NA and Zgierska A: Dextrose prolotherapy for
knee osteoarthritis: A randomized controlled trial. Ann Fam Med.
11:229–237. 2013.PubMed/NCBI View
Article : Google Scholar
|
|
8
|
Reeves KD and Hassanein K: Randomized
prospective double-blind placebo-controlled study of dextrose
prolotherapy for knee osteoarthritis with or without ACL laxity.
Altern Ther Health Med. 6:68–74, 77-80. 2000.PubMed/NCBI
|
|
9
|
Rezasoltani Z, Taheri M, Mofrad MK and
Mohajerani SA: Periarticular dextrose prolotherapy instead of
intra-articular injection for pain and functional improvement in
knee osteoarthritis. J Pain Res. 10:1179–1187. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kohn MD, Sassoon AA and Fernando ND:
Classifications in Brief: Kellgren-Lawrence classification of
osteoarthritis. Clin Orthop Relat Res. 474:1886–1893.
2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Roos EM, Klässbo M and Lohmander LS: WOMAC
osteoarthritis index. Reliability, validity, and responsiveness in
patients with arthroscopically assessed osteoarthritis. Western
Ontario and MacMaster Universities. Scand J Rheumatol. 28:210–215.
1999.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nguyen C, Lefèvre-Colau MM, Poiraudeau S
and Rannou F: Rehabilitation (exercise and strength training) and
osteoarthritis: A critical narrative review. Ann Phys Rehabil Med.
59:190–195. 2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Brosseau L, Yonge KA, Robinson V, Marchand
S, Judd M, Wells G and Tugwell P: Thermotherapy for treatment of
osteoarthritis. Cochrane Database Syst Rev.
2003(CD004522)2003.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Goh SL, Persson MSM, Stocks J, Hou Y, Lin
J, Hall MC, Doherty M and Zhang W: Efficacy and potential
determinants of exercise therapy in knee and hip osteoarthritis: A
systematic review and meta-analysis. Ann Phys Rehabil Med.
62:356–365. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Soliman DMI, Sherif NM, Omar OH and El
Zohiery AK: Healing effects of prolotherapy in treatment of knee
osteoarthritis healing effects of prolotherapy in treatment of knee
osteoarthritis. Egyptian Rheumatol Rehab. 43:47–52. 2016.
|
|
16
|
Dumais R, Benoit C, Dumais A, Babin L,
Bordage R, de Arcos C, Allard J and Bélanger M: Effect of
regenerative injection therapy on function and pain in patients
with knee osteoarthritis: A randomized crossover study. Pain Med.
13:990–999. 2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Rahimzadeh P, Imani F, Faiz SHR, Entezary
SR, Zamanabadi MN and Alebouyeh MR: The effects of injecting
intra-articular platelet-rich plasma or prolotherapy on pain score
and function in knee osteoarthritis. Clin Interv Aging. 13:73–79.
2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hassan F, Trebinjac S, Murrell WD and
Maffulli N: The effectiveness of prolotherapy in treating knee
osteoarthritis in adults: A systematic review. Br Med Bull.
122:91–108. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Rabago D, Zgierska A, Fortney L, Kijowski
R, Mundt M, Ryan M, Grettie J and Patterson JJ: Hypertonic dextrose
injections (prolotherapy) for knee osteoarthritis: Results of a
single-arm uncontrolled study with 1-year follow-up. J Altern
Complement Med. 18:408–414. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wang J, Liang J, Yao J, Song HX, Yang XT,
Wu FC, Ye Y, Li JH and Wu T: Meta-analysis of clinical trials
focusing on hypertonic dextrose prolotherapy (HDP) for knee
osteoarthritis. Aging Clin Exp Res. 34:715–724. 2022.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Arias-Vázquez PI, Tovilla-Zárate CA,
Legorreta-Ramírez BG, Burad Fonz W, Magaña-Ricardez D,
González-Castro TB, Juárez-Rojop IE and López-Narváez ML:
Prolotherapy for knee osteoarthritis using hypertonic dextrose vs
other interventional treatments: Systematic review of clinical
trials. Adv Rheumatol. 59(39)2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Hsu C, Vu K and Borg-Stein J:
Prolotherapy: A narrative review of mechanisms, techniques, and
protocols, and evidence for common musculoskeletal conditions. Phys
Med Rehabil Clin N Am. 34:165–180. 2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Han DS, Lee CH, Shieh YD, Chang CT, Li MH,
Chu YC, Wang JL, Chang KV, Lin SH and Chen CC: A role for substance
P and acid-sensing ion channel 1a in prolotherapy with
dextrose-mediated analgesia in a mouse model of chronic muscle
pain. Pain. 163:e622–e633. 2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
van Tittelboom V, Alemdaroglu-Gürbüz I,
Hanssen B, Heyrman L, Feys H, Desloovere K, Calders P and Van den
Broeck C: Reliability of isokinetic strength assessments of knee
and hip using the biodex system 4 dynamometer and associations with
functional strength in healthy children. Front Sports Act Living.
4(817216)2022.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Şahin N, Baskent A, Ugurlu H and Berker E:
Isokinetic evaluation of both knee extensor/flexor muscle strength
in patients with hypermobility syndrome. Rheumatol Int. 28:643–648.
2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Myers BJ: Isokinetic Testing of Muscle
Strength in Older Adults with Knee Osteoarthritis: An Integrative
Review. Isokin Exer Sci. 8:269–290. 2020.
|
|
27
|
Baert IAC, Meeus M, Mahmoudian A, Luyten
FP, Nijs J and Verschueren SMP: Do psychosocial factors predict
muscle strength, pain, or physical performance in patients with
knee osteoarthritis? J Clin Rheumatol. 23:308–316. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Gür H, Cakin N, Akova B, Okay E and
Küçükoğlu S: Concentric versus combined concentric-eccentric
isokinetic training: Effects on functional capacity and symptoms in
patients with osteoarthrosis of the knee. Arch Phys Med Rehabil.
83:308–316. 2002.PubMed/NCBI View Article : Google Scholar
|