Introduction
Cerebral vasospasm (CV) or delayed cerebral ischemia
(DCI) occurs in 30-40% of patients with aneurysmal subarachnoid
hemorrhage (aSAH) (1). However,
despite the use of various therapeutic procedures, 16-65% of these
patients develop ischemia (1-4).
The identification of CV (clinically or with
angiography) in the early stages of SAH can be complex and
challenging (2,3). Although 40-70% of patients exhibit
substantial arterial narrowing (on a Doppler ultrasound or in
angiography), only 20-30% of these patients present with DCI
(2,3). Intra-arterial digital subtraction
angiography (DSA) is effective as a screening device for patients
whose symptoms and clinical findings are consistent with focal
cerebral ischemia (CI) (5). However,
when analyzing the global vasculature with DSA, the detailed
delineation of the calf vessels may not be accomplished when
several stenoses are present and constitute an invasive method.
Computed tomography (CT) can illustrate the extent to which tissue
is irreversibly damaged (the ischemic core) (6-8),
and it indicates that reperfusion therapy may not be necessary or
may even be harmful when the ischemic core is large or the
perfusion is damaged to a great extent (9,10). By
contrast, CT perfusion (CTP) can identify damages not recognized by
other methods and may be beneficial for assessing CI related to SAH
(11). CTP can be used in daily
practice or it can be used as a separate diagnostic tool without
the need for magnetic resonance imaging data to predict the
outcomes of patients with SAH (12,13).
Various devices are employed to enhance cerebral blood flow (CBF)
in patients with SAH who develop CV or DCI. For example,
intra-aortic balloon counterpulsation, hyperdynamic therapy,
intra-arterial and intrathecal drug infusion, as well as novel
experimental techniques, such as endovascular treatment and various
drugs or their combinations, may be helpful if treatment commences
early. However, in the case that a CV does not appear or treatment
begins too late, CI may occur even with optimal management
(14). Phosphodiesterase-V (PDE-V)
is a regulatory enzyme of the endothelial nitric oxide synthase
(eNOS)/nitric oxide (NO)/cyclic guanosine monophosphate (cGMP)
pathway (15,16). The inhibition of this pathway mainly
through sildenafil (a PDE-V inhibitor) in patients with vasospasm
due to spontaneous SAH has been found to improve flow velocity on a
transcranial Doppler (17). At the
same time, animal and patient studies have revealed reduced blood
levels of endothelin-1 (18-21).
In addition, studies on patients with cardiovascular diseases have
proven that sildenafil is safe to administer (22-24).
However, to date, to the best of our knowledge, no extensive data
are available to confirm the positive effects of sildenafil in
patients with vasospasm due to SAH from a ruptured aneurysm.
In this respect, the present retrospective cohort
study was performed evaluate the utility of sildenafil following
its intravenous or oral administration in preventing DCI that
develops due to vasospasm in patients with aSAH.
Patients and methods
Study design and patient
population
The present retrospective cohort study analyzed
patients diagnosed with spontaneous SAH/aSAH (34 of the 42 patients
were diagnosed with spontaneous SAH/aSAH). The Institutional Review
Board (IRB) of Nicosia General Hospital, Cyprus approved the study
(IRB no. EEBK EΠ 2021.02.158). The study was in line with the
Declaration of Helsinki in 1995 (as revised in Edinburgh 2000).
Written informed was obtained from all patients for publication of
their data.
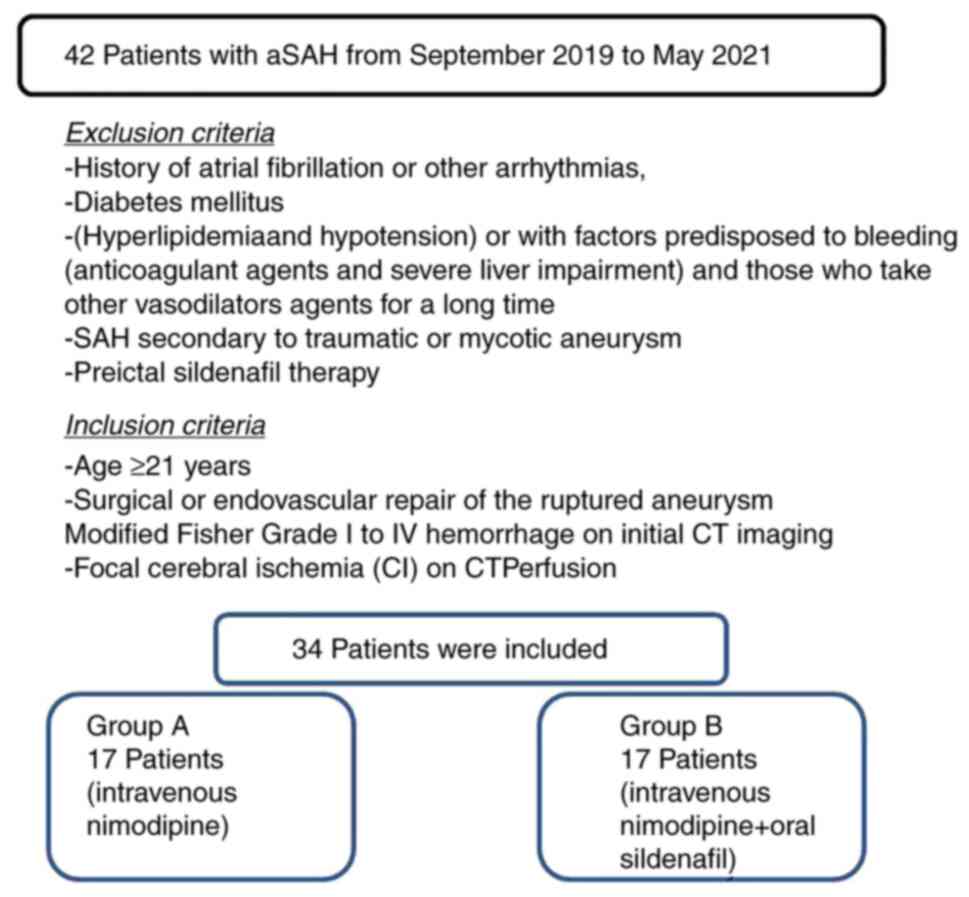
Inclusion criteria
The inclusion criteria were the following: An age
≥21 years, surgical or endovascular repair of the ruptured
aneurysm, a Modified Fisher grade of I to IV hemorrhage on initial
CT imaging, and evidence of CI on CTP. The patients were divided
into two groups, namely group A, which included patients treated
with only intravenous nimodipine, and group B, which included those
who received intravenous nimodipine together with sildenafil using
a dose escalation scheme (high dose of 20 mg or bioequivalent to a
40 mg oral dose). All individuals received nimodipine at 60 mg
every 4 h with close monitoring (including patients' heartbeat,
breathing rate, temperature, oxygen saturation and blood pressure)
for 21 days. These groups were identified based on age, sex, CT
findings, Glasgow Coma Scale (GCS) during intubation and
neurosurgical intervention as factors influencing patient
outcomes.
Exclusion criteria
Patients were excluded if they exhibited factors
predisposed to CI, apart from vasospasm (i.e., those with a history
of atrial fibrillation or other arrhythmias, diabetes mellitus,
hyperlipidemia and hypotension) or if they exhibited factors
predisposed to bleeding (anticoagulant agents and severe liver
impairment) and those who were taking any other vasodilators agents
for a long period of time, SAH secondary to traumatic or mycotic
aneurysm and preictal sildenafil therapy (Fig. 1). All participants had a follow-up
for 30 days or until the day of discharge from the hospital.
Patient outcomes were evaluated at 30 days using a CT scan, and a
complete neurological examination and a GCS assessment were
performed. The clinical outcome was categorized according to the
presence of neurological or radiological evidence as normal,
adverse or mortality.
Radiological CV or CI assessment
During the 3rd to the 6th day following the SAH, CTP
was performed in all the participants to identify a quantifiable
index of CI after CV, given that angiographically detectable
cerebral artery constriction is most commonly present 3-10 days
after the onset of the condition. The cerebral blood volume (CBV)
and CBF values were documented and assessed after receiving two
contiguous 10-mm slices placed at the anatomical point of the basal
ganglia with similar angulation as for native CT. A bolus of 50 ml
non-ionic contrast medium (Imeron 400, Bracco Imaging Deutschland
GmbH) accompanied by 30 ml saline was then infused using a power
injector at a flow rate of 4 ml/sec. Subsequently, 40 captures were
obtained at each slice level at a rate of two images per second
(120 kV, 110 mAs, 512x512 matrix). CTP color maps were
qualitatively assessed using a visual grading scale, and CTP
parameters were established utilizing software platforms (Perfusion
CT, Siemens). A positive visual measurement was recorded for
side-to-side apparent bilateral abnormalities, suggesting a decline
in CBF, CBV and mean transit time (MTT), which were related to the
central volume principle: CBF=CBV/MTT (2,25). CBV
was determined in milliliters of blood per 100 g of the brain and
was established as the volume of blood flow for a certain amount of
brain tissue (2,26). MTT was determined as the average time
required for blood to move through a particular brain volume and
was calculated in seconds (2).
Statistical analysis
Statistical analyses were performed using the
Statistical Package for the Social Sciences (SPSS 11; SPSS, Inc.).
The normality of the distribution of variables was assessed using
the Shapiro-Wilk test. Categorical variables were compared between
groups using Fisher's exact test and continuous data were compared
with the Mann-Whitney U test. Receiver operating characteristic
(ROC) analysis was presented to reveal the implementation of TCD or
CTP indicators in recognition of unfavorable outcomes. A P-value
<0.05 was considered to indicate a statistically significant
difference.
Results
In total, 34 of the 42 patients diagnosed with
spontaneous SAH/aSAH were enrolled in the present study. A total of
17 patients were included in group A and 17 patients were included
in group B. Of the 34 patients included, 18 were males (52.9%), and
the median age was 54.4 years. Of these patients, 18 (52.9%) had
undergone surgery, and 16 (47.1%) had an endovascular procedure.
The baseline characteristics of the study participants and CTP data
are presented in Table I. All
patients had a regular follow-up for 1 month.
 | Table IBaseline characteristics of the
patients included in the present study. |
Table I
Baseline characteristics of the
patients included in the present study.
| Parameters | All patients, n=34
(100%) | Group A, n=17
(50%) | Group B, n=17
(50%) | P-value |
|---|
| Age, years | 54.4±18 | 56.0±16 | 52.8±20 | 0.679 |
| Sex (male), n
(%) | 18 (52.9) | 10 (29.4) | 8 (23.5) | 0.170 |
| GCS at
admission | 13.1±2 | 12.6±2 | 13.7±1 | 0.201 |
| Procedure, n
(%) | | | | |
|
Surgical | 18 (52.9) | 10 (29.4) | 8 (23.5) | 0.492 |
|
Endovascular | 16 (47.1) | 7 (20.5) | 9 (26.4) | |
| MAP | | | | |
|
% Reduction
from baseline | 7.4±7 | 6.7±7 | 8.2±8 | 0.742 |
|
Duration,
min | 7.7±11 | 6.0±10 | 9.4±13 | 0.440 |
| Hunt and Hess
grade, n (%) | | | | |
|
I | 8 (23.5) | 3 (8.8) | 5 (14.7) | 0.419 |
|
II | 15 (44.1) | 4 (11.7) | 11 (32.3) | 0.016 |
|
III | 7 (20.5) | 6 (17.6) | 1 (2.9) | 0.034 |
|
IV | 3 (8.8) | 3 (8.8) | 0 (0) | 0.070 |
|
V | 1 (2.9) | 1 (2.9) | 0 (0) | 0.310 |
| Modified Fisher
grade, n (%) | | | | |
|
I | 8 (23.5) | 3 (8.8) | 5 (14.7) | 0.419 |
|
II | 16 (47.0) | 5 (14.7) | 11 (32.3) | 0.039 |
|
III | 7 (20.5) | 6 (17.6) | 1 (2.9) | 0.034 |
|
IV | 3 (8.8) | 3 (8.8) | 0 (0) | 0.070 |
| Aneurysm location,
n (%) | | | | |
|
ACoA | 6 (17.6) | 3 (8.8) | 3 (8.8) | NS |
|
MCA | 12 (35.2) | 4 (11.7) | 8 (23.5) | 0.151 |
|
PICA | 2 (5.8) | 1 (2.9) | 1 (2.9) | NS |
|
Pcom | 5 (14.7) | 3 (8.8) | 2 (5.8) | 0.628 |
|
ICA | 9 (26.4) | 6 (17.6) | 3 (8.8) | 0.244 |
| CT perfusion (white
matter) parameters | | | | |
|
CBFmean ± SD
(mlblood/100 gtissue) | 19.4±11 | 24.0±7 | 14.7±12 | 0.011 |
|
CBVmean ± SD
(mlblood/100 gtissue) | 1.4±1 | 1.6±0. | 1.2±1 | 0.042 |
|
MMTmean ± SD
(sec) | 4.3±1.5 | 4.6±1 | 3.9±1 | 0.055 |
Univariate analysis revealed that there was a
statistically significant difference in the mean values of CBF, CBV
and MTT between the participants who developed adverse ischemic
events and between those who did not develop adverse ischemic
events (P<0.05, Table II).
Overall, there was a statistically significant difference in the
number of patients who developed an ischemic event at 1 month in
group B compared with those of group A (P<0.05, Table II).
| Table IIUnivariate analysis (outcome,
ischemic event at 1 month). |
Table II
Univariate analysis (outcome,
ischemic event at 1 month).
| Parameter | Patients with
ischemic event, n=14 (41.1%) | Patients without
ischemic event, n=20 (58.9%) | P-value |
|---|
| Groups, n (%) | | | |
|
Group A | 14 (41.1) | 3 (8.8) | 0.001 |
|
Group B | 0 (0) | 17(50) | 0.001 |
| Age, years | 58.1±15 | 51.8±20 | 0.336 |
| Sex (male),
n(%) | 10 (29.4) | 8 (23.5) | 0.161 |
| GCS at
admission | 12.1±2 | 13.9±1 | 0.011 |
| Procedure, n
(%) | | | |
|
Surgical | 10 (29.4) | 8 (23.5) | 0.071 |
|
Endovascular | 4 (11.7) | 12 (35.2) | |
| MAP | | | |
|
% Reduction
from baseline | 4.7±3 | 9.4±8 | 0.388 |
|
Duration,
min | 3.1±4 | 11.0±14 | 0.181 |
| Hunt and Hess
grade, n (%) | | | |
|
I | 1 (2.9) | 7 (20.5) | 0.059 |
|
II | 3 (8.8) | 12 (35.2) | 0.026 |
|
III | 6 (17.6) | 1 (2.9) | 0.007 |
|
IV | 3 (8.8) | 0 (0) | 0.030 |
|
V | 1 (2.9) | 0 (0) | 0.225 |
| Modified Fisher
grade, n (%) | | | |
|
I | 1 (2.9) | 7 (20.5) | 0.059 |
|
II | 4 (11.7) | 12 (35.2) | 0.071 |
|
III | 6 (17.6) | 1 (2.9) | 0.007 |
|
IV | 3 (8.8) | 0 (0) | 0.030 |
| Aneurysm
location | | | |
|
ACoA | 3 (8.8) | 3 (8.8) | 0.628 |
|
MCA | 2 (5.8) | 10 (29.4) | 0.032 |
|
PICA | 1 (2.9) | 1 (2.9) | 0.794 |
|
Pcom | 2 (5.8) | 3 (8.8) | 0.954 |
|
ICA | 6 (17.6) | 3 (8.8) | 0.070 |
| CT perfusion (white
matter) parameters | | | |
|
CBFmean ± SD
(mlblood/100 gtissue) | 26.6±4 | 14.3±11 | 0.001 |
|
CBVmean ± SD
(mlblood/100 gtissue) | 1.8±0. | 1.1±1 | 0.005 |
|
MMTmean± SD
(sec) | 4.9±1 | 3.8±1 | 0.001 |
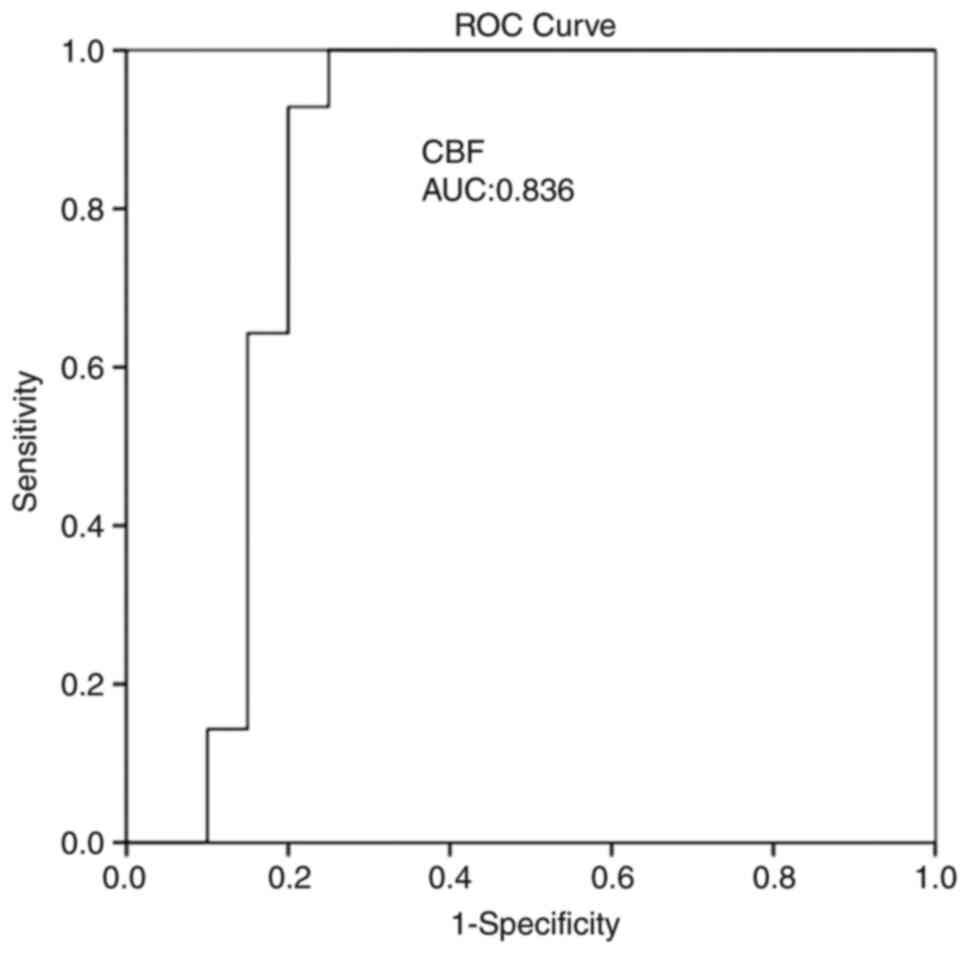
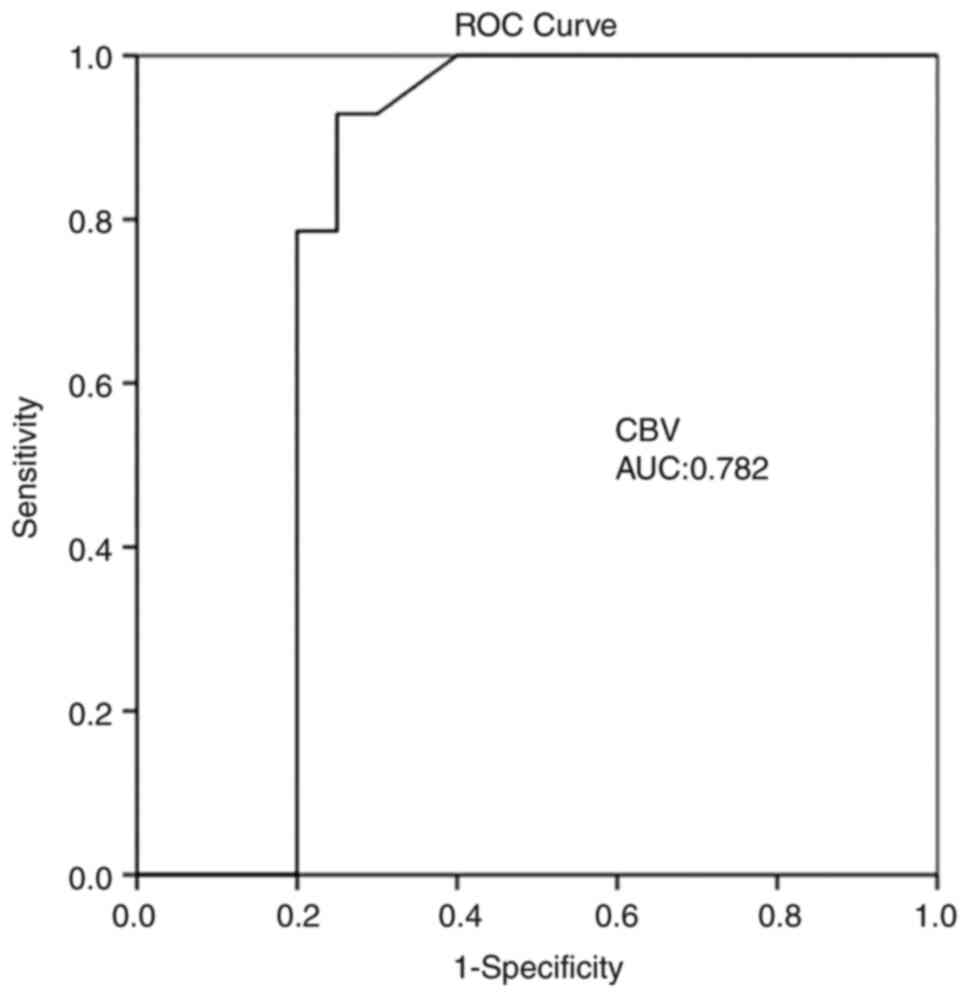
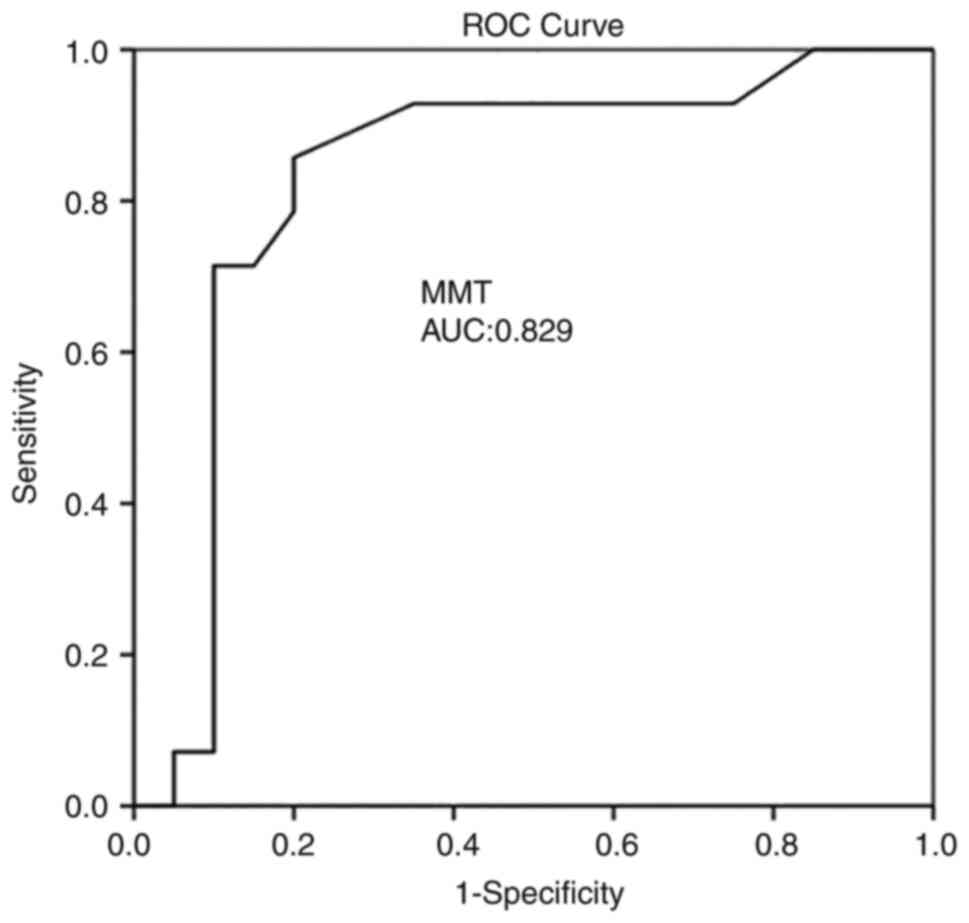
Multivariate analysis (Table III) revealed that CBF was an
independent factor in detecting an ischemic event at 1 month
(P=0.004). ROC analysis demonstrated that, among the CTP variables,
a CBF value <18.35 ml/100 g/min with 92.9% sensitivity and 80%
specificity and an MTT value >3.7 sec with 85.7% sensitivity and
80% specificity exhibited the optimal performance to diagnose
adverse ischemic events at 1 month, as evaluated by an area under
the curve standard error [AUC (SE)] of [0.83 (0.07)] and [0.82
(0.07)] (P=0.001, respectively; Table
IV and Fig. 2, Fig. 3 and Fig.
4).
| Table IIIMultivariate analysis (outcome,
ischemic event at 1 month). |
Table III
Multivariate analysis (outcome,
ischemic event at 1 month).
| | 95% CI for
Exp(B) |
|---|
| Parameter | P-value | Exp(B) | Lower | Upper |
|---|
| CBFmean ± SD
(mlblood/100 gtissue) | 0.004 | 1.395 | 1.109 | 1.754 |
| CBVmean ± SD
(mlblood/100 gtissue) | 0.028 | 0.079 | 0.008 | 0.758 |
| MMTmean ± SD
(sec) | 0.125 | 2.479 | 0.778 | 7.900 |
| Table IVROC analysis. |
Table IV
ROC analysis.
| | 95% CI | |
|---|
| Parameters | Area | Std Error | Lower | Upper | P-value |
|---|
| CBFmean ± SD
(mlblood/100 gtissue) | 0.836 | 0.077 | 0.684 | 0.988 | 0.001 |
| CBVmean ±S D
(mlblood/100 gtissue) | 0.782 | 0.089 | 0.608 | 0.957 | 0.006 |
| MMTmean ± SD
(sec) | 0.829 | 0.079 | 0.673 | 0.984 | 0.001 |
Discussion
The results of the present study suggest that using
sildenafil, intravenously or by oral administration may be helpful
for the prevention of DCI that develops due to vasospasm in
patients with SAH following an aneurysm rupture. In addition, CTP,
obtainable in everyday practice, provides valuable details
regarding SAH-associated CV. Certainly, CTP, mainly CBF and MTT,
can identify patients who have developed delayed unfavorable
ischemic incidents. Thus, sildenafil constitutes a very promising
therapy for the management of SAH. DSA is the gold standard for
identifying CV and different cerebrovascular entities (2,27,28).
However, the fact that the procedure is invasive and the radiation
exposure require careful patient selection and preclude widespread
use (29). Therefore, CTP is
currently the most commonly used and studied imaging technique
(2,28). A range of cut-off values associated
with DCI have been mentioned, counting an MTT value >5.0-6.4 sec
or a local CBF value <25-40 ml/100 g/min (2,30). In
the present study, a CBF value <18.35 ml/100 g/min with 92.9%
sensitivity and 80% specificity, and an MTT value >3.7 sec with
85.7% sensitivity and 80% specificity exhibited the optimal
performance in diagnosing adverse ischemic events at 1 month, as
evaluated using an AUC (SE). The present study examined two groups
of patients, depending on sildenafil therapy uptake. At a 1-month
follow-up, patients in group B (treated with a combination of
nimodipine and sildenafil) exhibited clinical outcomes without
ischemic damage in CTP. By contrast, the patients in group A
(treated only with nimodipine) exhibited unfavorable clinical
outcomes with ischemic damage in CTP.
Vasospasm following aSAH is a multifactored
mechanism and the standard of choice is the mainstay for preventing
calcium channel blocker nimodipine (31-34).
Furthermore, previous studies have indicated that not only
angiographic vasospasm, but also a disrupted microcirculation due
to microvascular constriction, micro-thrombosis, impaired
autoregulation, cortical spreading ischemia and blood-brain barrier
disruption may contribute to the development of DCI (35,36).
However, therapeutic strategies for vasospasm, refractory to
endovascular or microsurgical intervention are still under
investigation. Although it has been demonstrated that microsurgical
treatment may be helpful for vasospasms (37), others have justified the effects of
endovascular intervention as rescue therapy for severe vasospasm on
the clinical, as well as the radiological outcomes of patients with
aSAH (38). For this reason, the
present study was designed using, as a control group, those
patients that were treated with the mainstay of prevention, namely
the calcium channel blocker, nimodipine, to avoid bias. In
addition, it was better to include both endovascular and
microsurgical management as the results may would be more clear and
more related to the reality.
According to certain studies, sildenafil can cause
unacceptable hypotension in the patient population with aSAH, and
may thus be associated with unfavorable clinical outcomes (38-40).
However, the present study demonstrated that the blood pressure
profile was acceptable at a dose of 20 mg without evidence of a
prolonged adverse effect or any statistically significant
difference between groups (Tables I
and II). In addition, while there
was a 7.4% mean reduction in mean arterial pressure from baseline
levels, this was transient, lasting an average of 6.0 min until it
returned to baseline levels. The literature has well documented
that the upregulation of the eNOS/NO/cGMP pathway, a component of
the development of SAH-induced CV, can improve the clinical
outcomes and DCI (41-46).
Thus, researchers have administered PDEV inhibitors, such as
sildenafil to inhibit SAH-induced DCI. Theoretically, the mechanism
through which sildenafil, as a PDE-V inhibitor, utilizes its
positive vascular results has been in its capacity to increase
intracellular cGMP levels in vascular smooth muscle cells and
regulate vascular tone (47). In
addition, when CBF to a region reduces to ischemic levels,
sildenafil, similar to other orally active PDE5 inhibitors, such as
vardenafil, has exhibited the capability to decrease the extent of
the infarct and promote recovery by supporting the vasculature in
hypoxic areas (48,49). The findings of the present study
demonstrate that sildenafil may ‘reverse’ CV and the development of
CI.
However, the present study has certain limitations.
First, it was a small, single-center study. Therefore, firm
conclusions regarding the role of sildenafil in the management of
SAH cannot be reached. In addition, as vasospasm following aSAH is
a multifactorial mechanism, its role as a rescue therapy for
vasospasm, refractory to endovascular or microsurgical intervention
is not yet clear. Thus the present study did not distinguish the
causes of DCI as it would be impossible, and for this reason, the
present study was designed, using as a control group, those
patients that were treated with the mainstay of prevention, namely
with the calcium channel blocker, nimodipine, to avoid bias. In
addition, in the present study, there were a few patients with Hunt
and Hess grade IV or V; thus, the development of CV may not have
been severe. However, this may be a basis for a future, more
extensive clinical studies.
In conclusion, the present study demonstrates that
the use of intravenous or oral sildenafil may be helpful for the
prevention of DCI that develops due to vasospasm in patients with
aSAH. In addition, CTP, mainly CBF and MTT, obtainable in everyday
practice, provides valuable details regarding SAH-associated CV.
This sequence, along with the evidence of preclinical data in SAH
studies and the favorable effects of sildenafil in the treatment of
other entities related to vascular endothelium dysfunction,
provides a strong justification for more extensive prospective
clinical investigations into its efficacy for the prevention of
SAH-related DCI.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
GF, AAF and VEG conceptualized the study. KF, VEG,
AAF, PP, IT, NT, DAS, VT, NM and KT made a substantial contribution
to the analysis and interpretation of the data, and wrote and
prepared the draft of the manuscript. EL was the radiologist who
examined the patients and analyzed the radiological data. VEG and
GF analyzed the data and provided critical revisions. GF and KF
confirm the authenticity of all the data. All authors contributed
to manuscript revision and have read and approved the final version
of the manuscript.
Ethics approval and consent to
participate
The Institutional Review Board (IRB) of Nicosia
General Hospital, Cyprus approved the study (IRB no. EEBK EΠ
2021.02.158). The study was in line with the Declaration of
Helsinki in 1995 (as revised in Edinburgh 2000). Written informed
was obtained from all included patients for the publication of
their data.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cossu G, Messerer M, Oddo M and Daniel RT:
To look beyond vasospasm in aneurysmal subarachnoid haemorrhage.
Biomed Res Int. 2014(628597)2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Fotakopoulos G, Makris D, Kotlia P,
Kapsalaki E, Papanikolaou J, Georgiadis I, Zakynthinos E and
Fountas K: The value of computed tomography perfusion &
transcranial Doppler in early diagnosis of cerebral vasospasm in
aneurysmal & traumatic subarachnoid hemorrhage. Future Sci OA.
4(FSO313)2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ko NU, Rajendran P, Kim H, Rutkowski M,
Pawlikowska L, Kwok PY, Higashida RT, Lawton MT, Smith WS, Zaroff
JG and Young WL: Endothelial nitric oxide synthase polymorphism
(-786T->C) and increased risk of angiographic vasospasm after
aneurysmal subarachnoid hemorrhage. Stroke. 39:1103–1018.
2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Dumont AS, Dumont RJ, Chow MM, Lin CL,
Calisaneller T, Ley KF, Kassell NF and Lee KS: Cerebral vasospasm
after subarachnoid hemorrhage: Putative role of inflammation.
Neurosurgery. 53:123–135. 2003.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Foley WD, Smith DF, Milde MW, Lawson TL,
Towne JB and Bandyk DF: Intravenous DSA examination of patients
with suspected cerebral ischemia. Radiology. 151:651–659.
1984.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Muir KW, Baird-Gunning J, Walker L, Baird
T, McCormick M and Coutts SB: Can the ischemic penumbra be
identified on noncontrast CT of acute stroke? Stroke. 38:2485–2490.
2007.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Murphy BD, Fox AJ, Lee DH, Sahlas DJ,
Black SE, Hogan MJ, Coutts SB, Demchuk AM, Goyal M, Aviv RI, et al:
Identification of penumbra and infarct in acute ischemic stroke
using computed tomography perfusion-derived blood flow and blood
volume measurements. Stroke. 37:1771–177. 2006.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wintermark M and Warach SJ: Acute stroke
imaging research roadmap II and international survey of acute
stroke imaging capabilities: We need your help! AJNR Am J
Neuroradiol. 34(1671)2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Campbell BC, Christensen S, Butcher KS,
Gordon I, Parsons MW, Desmond PM, Barber PA, Levi CR, Bladin CF, De
Silva DA, et al: Regional very low cerebral blood volume predicts
hemorrhagic transformation better than diffusion-weighted imaging
volume and thresholded apparent diffusion coefficient in acute
ischemic stroke. Stroke. 41:82–88. 2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Yassi N, Parsons MW, Christensen S, Sharma
G, Bivard A, Donnan GA, Levi CR, Desmond PM, Davis SM and Campbell
BC: Prediction of poststroke hemorrhagic transformation using
computed tomography perfusion. Stroke. 44:3039–3043.
2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Provenzale JM, Shah K, Patel U and McCrory
DC: Systematic review of CT and MR perfusion imaging for assessment
of acute cerebrovascular disease. AJNR Am J Neuroradiol.
29:1476–1482. 2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Derex L, Nighoghossian N, Hermier M,
Adeleine P, Berthezène Y, Philippeau F, Honnorat J, Froment JC and
Trouillas P: Influence of pretreatment MRI parameters on clinical
outcome, recanalization and infarct size in 49 stroke patients
treated by intravenous tissue plasminogen activator. J Neurol Sci.
225:3–9. 2004.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Parsons MW, Barber PA, Chalk J, Darby DG,
Rose S, Desmond PM, Gerraty RP, Tress BM, Wright PM, Donnan GA and
Davis SM: Diffusion- and perfusionweighted MRI response to
thrombolysis in stroke. Ann Neurol. 51:28–37. 2002.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Francoeur CL and Mayer SA: Management of
delayed cerebral ischemia after subarachnoid hemorrhage. Crit Care.
20(277)2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Friebe A and Koesling D: Regulation of
nitric oxide-sensitive guanylyl cyclase. Circ Res. 93:96–105.
2003.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ghofrani HA, Osterloh IH and Grimminger F:
Sildenafil: From angina to erectile dysfunction to pulmonary
hypertension and beyond. Nat Rev Drug Discov. 5:689–702.
2006.PubMed/NCBI View
Article : Google Scholar
|
|
17
|
Mukherjee KK, Singh SK, Khosla VK,
Mohindra S and Salunke P: Safety and efficacy of sildenafil citrate
in reversal of cerebral vasospasm: A feasibility study. Surg Neurol
Int. 3(3)2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Das A, Xi L and Kukreja RC:
Phosphodiesterase-5 inhibitor sildenafil preconditions adult
cardiac myocytes against necrosis and apoptosis. Essential role of
nitric oxide signaling. J Biol Chem. 280:12944–12955.
2005.PubMed/NCBI View Article : Google Scholar
|
|
19
|
García-Cardoso J, Vela R, Mahillo E,
Mateos-Cáceres PJ, Modrego J, Macaya C and López-Farré AJ:
Increased cyclic guanosine monophosphate production and endothelial
nitric oxide synthase level in mononuclear cells from sildenafil
citrate-treated patients with erectile dysfunction. Int J Impot
Res. 22:68–76. 2010.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Gebska MA, Stevenson BK, Hemnes AR,
Bivalacqua TJ, Haile A, Hesketh GG, Murray CI, Zaiman AL, Halushka
MK, Krongkaew N, et al: Phosphodiesterase-5A (PDE5A) is localized
to the endothelial caveolae and modulates NOS3 activity. Cardiovasc
Res. 90:353–363. 2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Konstantinopoulos A, Giannitsas K,
Athanasopoulos A, Spathas D and Perimenis P: The impact of daily
sildenafil on levels of soluble molecular markers of endothelial
function in plasma in patients with erectile dysfunction. Expert
Opin Pharmacother. 10:155–1560. 2009.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Abbott D, Comby P, Charuel C, Graepel P,
Hanton G, Leblanc B, Lodola A, Longeart L, Paulus G, Peters C and
Stadler J: Preclinical safety profile of sildenafil. Int J Impot
Res. 16:498–504. 2004.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Conti CR, Pepine CJ and Sweeney M:
Efficacy and safety of sildenafil citrate in the treatment of
erectile dysfunction in patients with ischemic heart disease. Am J
Cardiol. 83:29C–34C. 1999.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Fox KM, Thadani U, Ma PT, Nash SD, Keating
Z, Czorniak MA, Gillies H and Keltai M: CAESAR I (Clinical American
and European Studies of Angina and Revascularization)
investigators. Sildenafil citrate does not reduce exercise
tolerance in men with erectile dysfunction and chronic stable
angina. Eur Heart J. 24:2206–2212. 2003.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Meier P and Zierler KL: On the theory of
the indicator-dilution method for measurement of blood flow and
volume. J Appl Physiol. 6:731–744. 1954.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Konstas AA, Goldmakher GV, Lee TY and Lev
MH: Theoretic basis and technical implementations of CT perfusion
in acute ischemic stroke, part 1: Theoretic basis. AJNR Am J
Neuroradiol. 30:662–668. 2009.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Yao GE, Li Q, Jiang XJ, Liu J, Li JL,
Zhang LL, Li LL, Zhang J and Xie P: Vasospasm after subarachnoid
hemorrhage: A 3D rotational angiography study. Acta Neurochir
Suppl. 110:221–225. 2011.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Cremers CH, van der Schaaf IC, Wensink E,
Greving JP, Rinkel GJ, Velthuis BK and Vergouwen MD: CT perfusion
and delayed cerebral ischemia in aneurysmal subarachnoid
hemorrhage: A systematic review and meta-analysis. J Cereb Blood
Flow Metab. 34:200–207. 2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kunze E, Pham M, Raslan F, Stetter C, Lee
JY, Solymosi L, Ernestus RI, Vince GH and Westermaier T: Value of
perfusion CT, transcranial doppler sonography, and neurological
examination to detect delayed vasospasm after aneurysmal
subarachnoid hemorrhage. Radiol Res Pract.
2012(231206)2012.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sanelli PC, Ugorec I, Johnson CE, Tan J,
Segal AZ, Fink M, Heier LA, Tsiouris AJ, Comunale JP, John M, et
al: Using quantitative CT perfusion for evaluation of delayed
cerebral ischemia following aneurysmal subarachnoid hemorrhage.
AJNR Am J Neuroradiol. 32:2047–2053. 2011.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Levati A, Solaini C and Boselli L:
Prevention and treatment of vasospasm. J Neurosurg Sci Mar. 42 (1
Suppl 1):S27–S31. 1998.PubMed/NCBI
|
|
32
|
Hansen D, Hannemann L, Specht M and
Schaffartzik W: Cerebral vasospasm following aneurysmal
subarachnoid hemorrhage. Therapeutic value of treatment with
calcium antagonists, hypervolemic hemodilution and induced arterial
hypertension. Anaesthesist. 44:219–229. 1995.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
33
|
Grotenhuis JA and Bettag W: Prevention of
symptomatic vasospasm after SAH by constant venous infusion of
nimodipine. Neurol Res. 8:243–249. 1986.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Hänggi D, Beseoglu K, Turowski B and
Steiger HJ: Feasibility and safety of intrathecal nimodipine on
posthaemorrhagic cerebral vasospasm refractory to medical and
endovascular therapy. Clin Neurol Neurosurg. 110:784–790.
2008.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Geraghty JR and Testai FD: Delayed
cerebral ischemia after subarachnoid hemorrhage: Beyond vasospasm
and towards a multifactorial pathophysiology. Curr Atheroscler Rep.
19(50)2017.PubMed/NCBI View Article : Google Scholar
|
|
|
Maruhashi T and Higashi Y: An overview of
pharmacotherapy for cerebral vasospasm and delayed cerebral
ischemia after subarachnoid hemorrhage. Expert Opin Pharmacother.
22:1601–1614. 2021.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Ba Y, Zhang C, Huang J, Hua X, Cui T, Zhao
S and Gao G: Microsurgical clipping vs. arterial embolization in
the treatment of ruptured anterior circulation aneurysms. Am J
Transl Res. 13:8040–8048. 2021.PubMed/NCBI
|
|
37
|
Mielke D, Döring K, Behme D, Psychogios
MN, Rohde V and Malinova V: The impact of endovascular rescue
therapy on the clinical and radiological outcome after aneurysmal
subarachnoid hemorrhage: A safe and effective treatment option for
hemodynamically relevant vasospasm? Front Neurol.
13(838456)2022.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Atalay B, Caner H, Cekinmez M, Ozen O,
Celasun B and Altinors N: Systemic administration of
phosphodiesterase V inhibitor, sildenafil citrate, for attenuation
of cerebral vasospasm after experimental subarachnoid hemorrhage.
Neurosurgery. 59:1102–1107. 2006.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Adiga A, Edriss H and Nugent K:
Intracranial aneurysm and sildenafil. Proc (Bayl Univ Med Cent).
29:178–1780. 2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Gokce C, Gulsen S, Yilmaz C, Guven G,
Caner H and Altinors N: The effect of the sildenafil citrate on
cerebral vasospasm and apoptosis following experimental
subarachnoid hemorrhage in rats. J Neurosurg Sci. 54:29–37.
2010.PubMed/NCBI
|
|
41
|
Edwards DH, Byrne JV and Griffith TM: The
effect of chronic subarachnoid hemorrhage on basal
endothelium-derived relaxing factor activity in intrathecal
cerebral arteries. J Neurosurg. 76:830–837. 1992.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Inoha S, Inamura T, Ikezaki K, Nakamizo A,
Amano T and Fukui M: Type V phosphodiesterase expression in
cerebral arteries with vasospasm after subarachnoid hemorrhage in a
canine model. Neurol Res. 24:607–612. 2002.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Kasuya H, Weir BK, Nakane M, Pollock JS,
Johns L, Marton LS and Stefansson K: Nitric oxide synthase and
guanylate cyclase levels in canine basilar artery after
subarachnoid hemorrhage. J Neurosurg. 82:250–255. 1995.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Kim P, Schini VB, Sundt TM Jr and
Vanhoutte PM: Reduced production of cGMP underlies the loss of
endothelium-dependent relaxations in the canine basilar artery
after subarachnoid hemorrhage. Circ Res. 70:248–256.
1992.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Thomas JE and Rosenwasser RH: Reversal of
severe cerebral vasospasm in three patients after aneurysmal
subarachnoid hemorrhage: Initial observations regarding the use of
intraventricular sodium nitroprusside in humans. Neurosurgery.
44:48–58. 1999.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Vellimana AK, Milner E, Azad TD, Harries
MD, Zhou ML, Gidday JM, Han BH and Zipfel GJ: Endothelial nitric
oxide synthase mediates endogenous protection against subarachnoid
hemorrhage-induced cerebral vasospasm. Stroke. 42:776–782.
2011.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Han BH, Vellimana AK, Zhou ML, Milner E
and Zipfel GJ: Phosphodiesterase 5 inhibition attenuates cerebral
vasospasm and improves functional recovery after experimental
subarachnoid hemorrhage. Neurosurgery. 70:178–187. 2012.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Sahara M, Sata M, Morita T, Nakajima T,
Hirata Y and Nagai R: A phosphodiesterase-5 inhibitor vardenafil
enhances angiogenesis through a protein kinase G-dependent
hypoxia-inducible factor-1/vascular endothelial growth factor
pathway. Arterioscler Thromb Vasc Biol. 30:1315–1324.
2010.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Zhang L, Zhang RL, Wang Y, Zhang C, Zhang
ZG, Meng H and Chopp M: Functional recovery in aged and young rats
after embolic stroke: Treatment with a phosphodiesterase type 5
inhibitor. Stroke. 36:847–852. 2005.PubMed/NCBI View Article : Google Scholar
|