Introduction
Esophageal cancer (EC) is the sixth major leading
cause of cancer-related mortality. Almost half of the cases may
already have metastasis at the time of presentation (1). It is mainly divided into two subtypes,
including squamous cell carcinoma (SCC) and adenocarcinoma (ADC)
(2). Esophageal ADC is associated
with a poor survival rate and prognosis. However, at an early
stage, its cure rate is ~50% following surgical resection (3,4). EC
frequently spreads to the liver, lungs, bones and brain. However,
subcutaneous and soft tissue metastases are uncommon (5,6). The
incidence of subcutaneous metastasis originating from EC ranges
from 0.7 to 9%, and only a few reports have been published to date
(1,3,5-7).
The risk factors for this type of metastasis remain ambiguous
(3,7,8). The
most common sites of subcutaneous metastasis from EC include the
neck, scalp and face. Chest wall involvement is a very rare
phenomenon (3). The majority of
malignant tumors on the chest wall are metastasized from the
cancers of surrounding organs (9).
The present study describes a rare case of
gastroesophageal ADC that metastasized to the chest wall, invading
the fourth anterior rib.
Case report
Patient information
A 70-year-old female presented to the Cardiothoracic
Department at Smart Health Tower (Sulaimani, Iraq), complaining of
acute chest pain after 4 months of undergoing an Ivor-Lewis
esophagectomy for gastroesophageal ADC.
Diagnostic assessment of the previous
presentation
An endoscopic examination revealed an esophageal
mass just above the gastroesophageal junction with evidence of
bleeding. A computed tomography (CT) scan of the chest and abdomen
revealed a lower esophageal tumor with local pathological lymph
nodes without esophageal obstruction or other organ invasions. A
biopsy specimen was obtained and histopathological examination
(conducted at another institution) confirmed a gastroesophageal
ADC. Immunohistochemistry was positive for CDX2 and negative for
HER2 and TTF1 (data not shown; conducted at another institution).
The patient received four cycles of neoadjuvant chemotherapy and
then underwent an Ivor-Lewis surgery.
Clinical findings and diagnostic
assessment
The physical examination of the patient did not
reveal any notable findings.
At 4 months following the surgical resection of
gastroesophageal ADC, the patient was referred to the
Cardiothoracic Department at Smart Health Tower complaining of
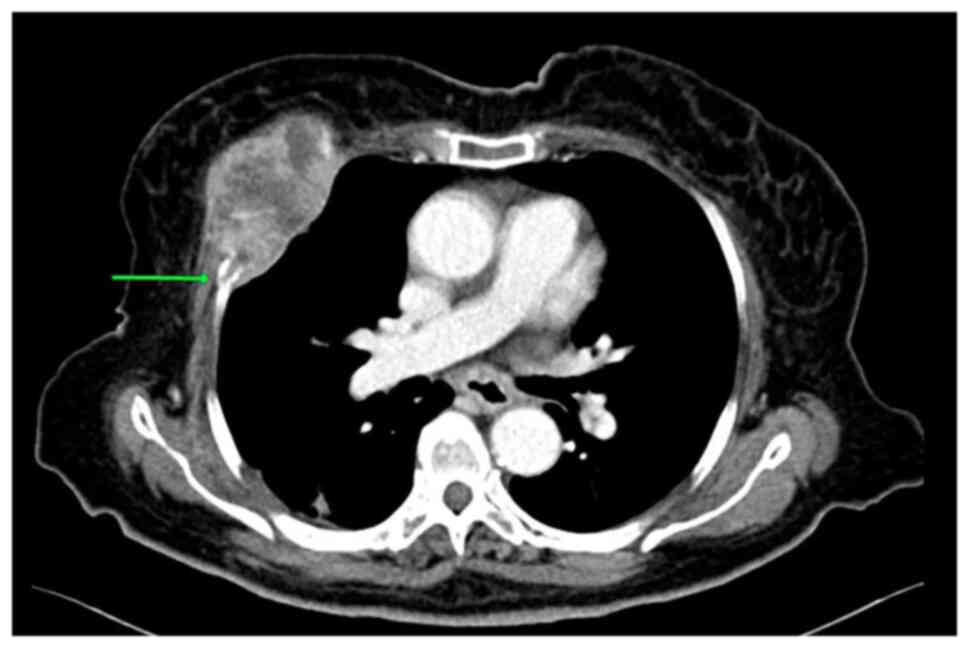
acute chest pain. A chest ultrasound (US) revealed a solid
hypoechoic mass (87x63x51 mm) on the right side of the chest,
lateral to the sternum, located ~12 mm under the skin. A
contrast-enhanced CT scan of the chest revealed a destructive mass
on the right anterior fourth rib (7.5x5 cm; Fig. 1). A fine needle aspiration (FNA) was
conducted and this revealed a metastatic moderately differentiated
ADC to the chest wall. A fluorodeoxyglucose (FDG)-positron emission
tomography (PET)/CT scan revealed a large FDG avid deposit on the
right side of the chest wall. The mediastinal lymph nodes exhibited
internal calcification and were suspicious as infected lymph nodes.
The lymph nodes exhibited a lack of uptake in the PET scan; they
had calcification and were thus diagnosed as reactionary lymph
nodes to the previous infection.
Therapeutic intervention
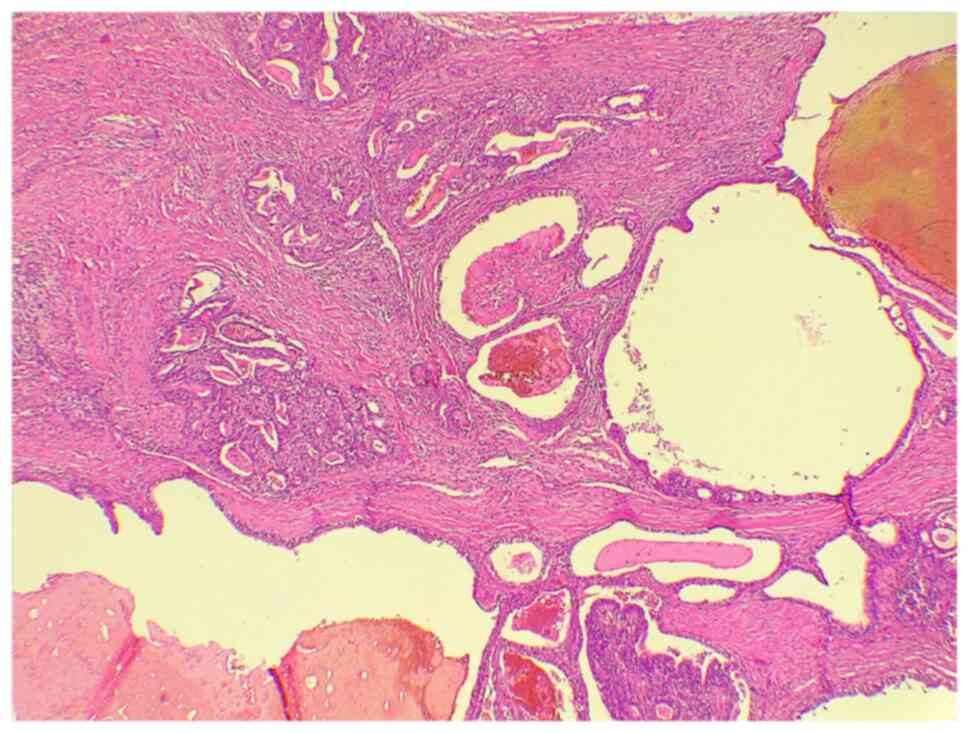
The patient underwent a chest wall resection and
reconstruction. Under general anesthesia, a right-side anterior
chest incision was made and the second, third and fourth ribs were
resected with overlying soft tissues, including the pectoralis
muscle and overlying skin. A sample was sent for histopathological
analysis and a gastroesophageal ADC metastasizing to the chest wall
was confirmed (Fig. 2).
Follow-up
The post-operative period was uneventful and the
patient received Myogesic (six tablets) per day for 20 days
(2x3).
Discussion
EC is one of the most common causes of
cancer-related mortality worldwide. The possibility of metastasis
during the presentation of the primary cancer is up to 50%. Despite
the fact that both types of EC (SCC and ADC) can respond to
chemotherapy, the survival rate is low and is dependent on the
disease stage. The 5-year survival rates of patients range between
95% at the early stages of the disease and 10-15% at stage III. The
median survival rate in metastatic cases has been reported to be
<1 year (1). This type of cancer
predominately arises between the ages of 60 and 70 years (5). EC metastasis to visceral organs, such
as the liver and lungs is common, while subcutaneous metastasis is
estimated to be <10% (1,6,10). It is
most likely asymptomatic, although it can also cause acute pain
(11).
Although they are very rare, subcutaneous metastatic
lesions can develop from both types of EC, and their incidence
typically relates to the prevalence of the primary cancer.
Esophageal ADC is more frequent among Caucasian males in contrast
to esophageal SCC, which is more common among Caucasian females,
Asians and individuals of African origin (3). Males have been mentioned as the
dominant sex in cases of EC metastasis to unusual sites (2). In the esophagus, the most commonly
involved regions are the lower and distal parts (12). In addition, it has been noted that
tumors growing in the lower third of the esophagus, particularly
ADC, have a higher risk of distant metastasis (16.7%) than those
growing in the upper and middle third (~6%) (7). The case presented herein was a female
in her 70s, who presented with acute chest pain following an Ivor
Lewis esophagectomy for gastroesophageal ADC. In line with the
findings of a previous study (7),
the ADC developed in the lower part of the esophagus just above the
gastroesophageal junction.
EC can metastasize to subcutaneous tissues of
various locations and the most common ones are the neck, scalp and
face. However, its metastasis to the back, axillary regions and
chest wall is exceedingly uncommon (1,3). Datta
et al (3) reported three
cases of subcutaneous metastasis from esophageal ADC; two of them
metastasized to the skin and scalp, and the third case involved the
chest wall. They also stated that subcutaneous metastasis can occur
in a variable time interval, such as in the early stage of the
disease or later (3). Riley and Wah
(13) also reported a case of skull
and skin metastasis in a patient who experienced an esophageal ADC
resection 4 years prior. The lesion was first suspected to be a
post-traumatic hematoma (13).
Another study discussed an incident of scalp metastasis from an
esophageal ADC following a total esophagogastrectomy (14). In the current literature, at least to
the best of our knowledge, the occurrence of chest wall metastasis
from esophageal ADC has rarely been reported (13). Before Datta et al (3), Lindenmann et al (15) reported a chest wall metastasis from
esophageal ADC in a 59-year-old male following 18 months of
transhiatal esophagectomy and two-field lymphadenectomy. The case
presented with thoracic pain and the tumor metastasized to the
right ventrolateral area of the chest wall under the right pectoral
muscle (15). Furthermore,
Gogalniceanu et al (1)
described a case of chest wall metastasis that appeared as a back
lump that was noticed during the diagnosis of an esophageal ADC.
Tunio et al (11) added
another case to the literature that involved the right posterior
chest wall and developed after 9 months of primary cancer
management.
Generally, there are two common assumptions
regarding chest wall metastasis from EC. The first one states that
this metastasis can occur due to the implantation of the carcinoma
during resection of the tumor and it is known as ‘implantation
metastases’. The latter supports the notion of tumor cell
dissemination along the esophageal lymphatic and hematogenous
systems (15). In the case presented
herein, chest wall metastasis was found 4 months following the
surgical resection, in a manner that the condition presented with
chest pain. The metastasis involved the right anterior of the chest
wall, lateral to the sternum and invaded the anterior fourth rib,
which is a rare finding. As regards the mechanism of metastasis,
the case in the present study supports the second assumption and
was considered to be caused by hematogenous dissemination.
Several particular points have been proposed for the
improved diagnosis of chest wall metastasis. An extensive physical
examination appears to be necessary in all patients who have been
affected by a known cancer with repeated clinical assessments
during the period of treatment and follow-up. In addition,
multi-modality assessments need to be performed in patients with
EC, such as a CT scan, PET scan, oesophago-gastro-duodenoscopy,
endoscopic US, laparoscopy and biopsy of any chest wall lesion, in
order to better consider the disease stage and prevent unnecessary
intervention (1). Using US is
essential to determine whether a lesion is solid or cystic, and it
also demonstrates any relation of the lesion to surrounding
structures (13). When a suspicious
mass is identified on a US, CT and magnetic resonance imaging can
be used as additional diagnostic approaches to provide further
information about the nature of the lesion and its association with
the adjacent structures (13). The
combination of FDG PET and CT can accurately identify soft tissue
masses originating in unusual locations (2). In the case of the present study, a
chest US revealed a solid hypoechoic mass on the right side of the
chest lateral to the sternum. A contrast-enhanced CT scan of the
chest revealed a mass on the right anterior fourth rib. FNA
revealed a metastatic ADC to the chest wall.
The survival rate of patients with subcutaneous
metastatic tumors can be <1 year following diagnosis due to a
poor prognosis. Commonly, the aim of treatment is palliation
through tumor resection in addition to chemoradiotherapy (3). Systemic therapy may have a high failure
rate in the treatment of such poor prognostic diseases, and
Lindenmann et al (15)
mentioned total resection of chest wall metastasis as the treatment
of choice. The patient in the present study underwent chest wall
resection and reconstruction, in which the second, third and fourth
ribs were resected with overlying soft tissues. Histopathological
analysis confirmed chest wall metastasis from previously managed
gastroesophageal ADC.
In conclusion, chest wall metastasis from EC,
invading the ribs is an extremely rare incident. However, its
likelihood of occurrence should not be neglected, and proper
clinical assessment and follow-up are mandatory following the
treatment of primary cancer.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RA was the oncologist who managed the case. OHGH,
DAI and FHK were the major contributors to the conception of the
study, and surgeons who managed the case. HOA and FHK were involved
in the literature review and in the writing of the manuscript, as
well as in data analysis and interpretation. BAAw, BAAb, DH, HHKA
and BJM were involved in the literature review, in the design of
the study, in the revision of the manuscript and in the collection
and processing of the images. BAAw and DAI confirm the authenticity
of all the raw data. SHT was the radiologist who performed the
assessment. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient's family described in the present study for the inclusion
of her data in the study.
Patient consent for publication
Written informed consent was obtained from the
patient's family described in the present study for the publication
of her data and any related images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gogalniceanu P, Jarral OA, Purkayastha S,
Aggarwal R and Zacharakis E: Chest wall metastasis from oesophageal
adenocarcinoma: A rare presentation. Updates Surg. 63:223–226.
2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mendiola VL and Willis M: Esophageal
adenocarcinoma with extensive metastasis to unexpected sites: A
case report. Case Rep Oncol. 11:742–750. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Datta S, Muñoz-Largacha JA, Li L, Zhao GQ
and Litle VR: Subcutaneous metastases from early stage esophageal
adenocarcinoma case report. Int J Surg Case Rep. 29:108–112.
2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Rice TW, Adelstein DJ, Zuccaro G, Falk GW
and Goldblum JR: Advances in the treatment of esophageal carcinoma.
Gastroenterologist. 5:278–294. 1997.PubMed/NCBI
|
|
5
|
Balukrishna S, Jennifer P and Viswanathan
PN: Solitary subcutaneous metastasis from squamous cell carcinoma
of the esophagus: A case report and brief review of literature. J
Gastrointest Cancer. 42:269–271. 2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hsu KF, Lee SC, Ho CL, Jin JS, Chang YM
and Tzao C: Abdominal subcutaneous metastasis from esophageal
squamous cell carcinoma. J Med Sci. 29:217–219. 2009.
|
|
7
|
Nguyen D, Siraj S, Ngu C, Bennett G and
Pranavan G: An unusual case of oesophageal adenocarcinoma
presenting with subcutaneous metastases. J Gastrointest Cancer. 45
(Suppl 1):S175–S177. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kapoor J, Basu S and Menon S: Subcutaneous
metastasis in esophageal carcinoma detected by FDG-PET Imaging.
Indian J Cancer. 46:354–355. 2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Saijo H, Kitamura Y, Takenaka H, Kudo S,
Yokoo K, Hirohashi Y and Takahashi H: Occult thyroid follicular
carcinoma diagnosed as metastasis to the chest wall. Intern Med.
56:2033–2037. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Quint LE, Hepburn LM, Francis IR, Whyte RI
and Orringer MB: Incidence and distribution of distant metastases
from newly diagnosed esophageal carcinoma. Cancer. 76:1120–1125.
1995.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tunio MA, AlAsiri M and Riaz K:
Adenocarcinoma of oesophagus metastasising to the subcutaneous soft
tissue. Arab J Gastroenterol. 14:133–134. 2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Thrift AP: The epidemic of oesophageal
carcinoma: Where are we now? Cancer Epidemiol. 41:88–95.
2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Riley S and Wah T: Cutaneous metastasis of
esophageal adenocarcinoma with an unusual presentation. J Clin
Ultrasound. 35:289–292. 2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Park JM, Kim DS, Oh SH, Kwon YS and Lee
KH: A case of esophageal adenocarcinoma metastasized to the scalp.
Ann Dermatol. 21:164–167. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lindenmann J, Matzi V, Porubsky C, Maier A
and Smolle-Juettner FM: Complete resection of an isolated chest
wall metastasis from esophageal carcinoma after transhiatal
esophagectomy and gastric pull-up at one and a half-year follow-up.
J Thorac Oncol. 2:773–776. 2007.PubMed/NCBI View Article : Google Scholar
|