Introduction
Oral submucous fibrosis (OSMF) is a chronic disease
of uncertain origin that has a gradual and harmful effect on the
mucous membranes of various regions within the oral cavity.
Furthermore, it can sporadically spread to the pharynx and
esophagus and, on rare occasions, even to the larynx. It is
characterized by a sub-epithelial inflammatory reaction followed by
progressive fibrosis, leading to trismus and epithelial atrophy
(1). It is commonly observed in
individuals who are 20-35 years of age, and mostly in India and
Southeast Asia (prevalence rate, 2.26%), where it is commonly
associated with the use of areca nuts (2).
The etiology of the disease is exceedingly
intricate, and none of the therapeutic approaches employed to date
have yielded adequate outcomes. The management of patients with
OSMF is dependent on the extent of disease progression and its
clinical manifestations. In the initial phases, the cessation of
deleterious habits and the administration of nutritional
supplements (multivitamins) are implemented. During the
intermediate stages, a conservative approach is adopted which
entails intralesional injections in conjunction with medical
therapy. Surgical intervention is imperative in the advanced stages
of the disease (3). The chief
concern of affected patient is invariably the reduction in mouth
opening (trismus) and associated discomfort with the consumption of
food due to the burning sensation. However, the main concern of
clinicians is the potential of the disease for malignant
transformation (1).
The main goal of treatments for OSMF is to reduce
the associated burning sensation and trismus. This can be achieved
by therapy with intralesional injections of placental extract,
hyaluronidase and corticosteroids. These treatments have been used
alone or in combination in previous studies (4-8).
However, it should be noted that, to the best of our knowledge,
none of the studies published to date have considered the inclusion
of a control group. Moreover, it is worth mentioning that only two
studies have undertaken a brief follow-up examination spanning a
period of 9 months (5,6). Furthermore, it is important to
highlight that only two studies have been conducted with a sample
size of 60 patients, but utilize only two medications and no
follow-up was performed (7,8). Therefore, the present study was
undertaken in an aim to compare the therapeutic outcomes of
patients with OSMF treated with an intralesional injection of
placental extract, hyaluronidase combined with dexamethasone, and
placental extract combined with hyaluronidase and dexamethasone, in
comparison to a control group. In addition, the present study
analyzed the loss of mouth opening 1 year following the cessation
of treatment. The null hypothesis posited in the present study
suggests that there is no disparity in the therapeutic effects of
the three modalities in patients with OSMF.
Patients and methods
Study overview
A single-center, parallel-group, randomized
controlled trial (RCT) with a 1:1:1:1 allocation ratio (40 patients
in each group) was conducted at the Department of Oral Surgery,
Jawahar Medical Foundation's ACPM Dental College, Dhule, India
between March, 2022 and September, 2023. The patients presented
with trismus, a blanched, white marble-like appearance of the oral
mucosa, palpable fibrous bands, sunken cheeks, difficulty in eating
and a mild to moderate burning sensation. A detailed history of the
use of areca nuts, tobacco and its related products, as well as the
consumption of alcohol, and hot and spicy food was obtained from
the participants. Patients who were willing to participate were
examined thoroughly by a senior oral surgeon for the presence of
clinical symptoms, and the confirmation of OSMF was performed by a
histopathological examination. The study was conducted according to
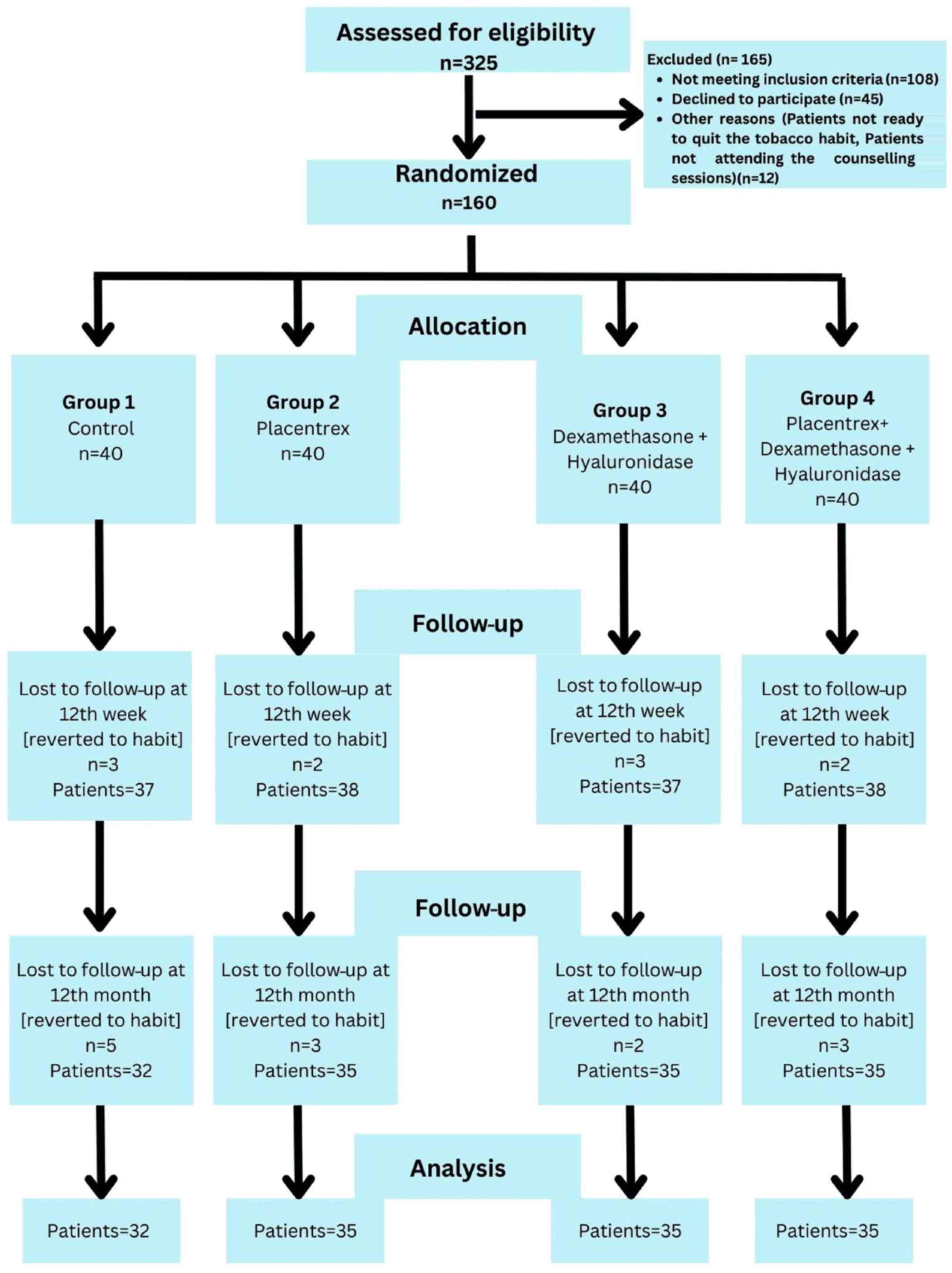
the principles of the Declaration of Helsinki. The present RCT was
conducted according to the Consolidated Standards of Reporting
Trials (CONSORT) guidelines, which are designed to improve the
reporting of parallel-group randomized controlled trials (9) as shown in Fig. 1. This trial was registered at the
Clinical Trial Registry of India at www.ctri.nic.in (CTRI/2022/01/061403; https://ctri.nic.in/Clinicaltrials/pmaindet2.php?EncHid=OTY1NDk=&Enc=&userName=).
Ethical considerations
The present study was approved by the Institutional
Ethical Committee of Jawahar Medical Foundation Annasaheb Chudaman
Patil Memorial Dental College (EC/NEW/INST/2022/2959/2022/63).
Written informed consent was obtained from all the patients after
explaining the outcomes and potential complications of the
procedure. The control group signed the consent forms stating that
they did not wish to receive treatment for intra-lesional
injections and therefore, patients in the control group were
provided with oral supplements for OSMF, such as antioxidants (OSMF
Vita, Sterlife Biotec), 0.1% triamcinolone oromucosal paste
(Turbocort, Indoco Remedies Ltd.), and 0.15% benzydamine mouthwash
(B-mine, Dupen Laboratories Pvt. Ltd.), along with regular mouth
opening exercises.
Sample size calculation
The sample size was calculated using G*Power
statistical software (Ver. 3.1 Franz Faul, Universität Kiel, Kiel,
Germany). The sample size was calculated from a previous study with
a type I error of 0.05, power of 80%, and an effect size of 0.3;
the resulting sample size was 15 for each group (4). The present study was conducted with 40
patients in each group, considering a 10% dropout rate and
increasing the power of the study to 90%.
Study population
A total of 325 patients with OSMF were screened
based on the eligibility criteria, and 160 patients were selected
for inclusion in the study based on the inclusion and exclusion
criteria. Patients diagnosed with grade 2 and grade 3 OSMF, as
evidenced from their results of the detailed clinical and
histopathological examination, according to the classification
protocol described in the study by Passi et al (10), were included in the study.
Patients previously treated for OSMF; patients who
had grade 1 and 4 OSMF; those who were allergic to placental
extracts, steroids and hyaluronidase; those who did not give their
consent; those with syndromic or systemic disease with mouth
ulcers; those who had undergone radiotherapy sessions leading to
oral ulcers; and those who had a previous history of major surgery
in the oral cavity or carcinoma of the oral cavity were excluded
from the study.
Routine hematological examinations, such as complete
blood count, clotting analysis, serum electrolyte assessment,
erythrocyte sedimentation rate (ESR), vitamin B12 levels, human
immunodeficiency virus detection and hepatitis B surface antigen
evaluation were conducted during the initial visit of the
patients.
The 160 patients with grade 2 and 3 OSMF who were
included in the study (Fig. 1) were
divided into four groups as follows: Group 1, 40 patients who did
not agree to receive intralesional injections, and were therefore
administered oral medication for OSMF; group 2, 40 patients who
received an intralesional injection of 2 ml placental extracts
(Placentrex, Albert David Pharmaceuticals Ltd.), mixed with 1 ml of
2% lignocaine; group 3, 40 patients who received an injection of
1,500 IU of 1 ml hyaluronidase (Hynidase, Shreya Pharmaceuticals
Ltd.), with 1 ml dexamethasone (Decadron, Wockhardt Ltd.), mixed
with 1 ml of 2% lignocaine; group 4, 40 patients who received a
combination of the drugs in the aforementioned two groups (2 ml
placental extracts, 1 ml hyaluronidase, 1 ml dexamethasone and 1 ml
of 2% lignocaine).
Randomization was exclusively performed for the
experimental groups, while the control group, due to ethical
considerations, comprised individuals who declined the
intra-lesional injection treatment. A computerized random number
generator was used to generate a sequence lacking a particular
pattern (Stat-Trek program; https://stattrek.com/). A total of 120 non-transparent
envelopes (for only the experimental groups) were meticulously
assembled and placed in a bowl. These envelopes were methodically
assigned a code and securely sealed by a separate researcher who
was not involved in the patient selection. Each participant in the
experimental group was instructed to select an envelope.
Subsequently, each participant was allocated an intervention in
accordance with the selected envelope.
The present study was an open-label study in which
the patients in the control group and the oral surgeon who treated
the patients could not be blinded. In the context of an open-label
investigation, it is desirable for the evaluation of the results to
be concealed, if feasible. Consequently, the statistician was
unaware of the allocation of the individuals to their respective
groups. Given the ethical considerations, it was not possible to
conceal the control group. To minimize any potential bias in the
evaluation process, the patients participating in the experimental
groups were not made aware of the specific pharmacological agent
employed for the intra-lesional injections.
Procedure
Patients were actively discouraged (through
preliminary counseling session) from consuming areca nut and
tobacco products, alcohol, and hot and spicy foods, which are
strongly associated with the development of the condition under
consideration. Furthermore, the patients were advised to adopt a
well-balanced diet. Moreover, meticulous efforts were made to
eliminate any potential sources of infection and irritation within
the oral cavity, such as the enameloplasty of sharp cusps, thus
ensuring a comprehensive approach for the management of the
condition. The patients were provided with oral prophylaxis, which
involved thorough cleaning and the maintenance of oral hygiene to
mitigate the risk of further complications. Repeated counseling
sessions were conducted with the patients to motivate them to leave
the habit of using tobacco products, alcohol, and hot and spicy
foods. Following a thorough assessment after a period of 8 weeks,
the patients were required to provide assurance that they had
successfully refrained from engaging in deleterious habits as
instructed, and based on their compliance, further management and
treatment were continued.
Drugs were introduced into the submucosal layer at
the affected site, mainly in the retromolar area (area of maximum
fibrosis), using an insulin syringe and needle, with the aim of
mitigating the development of fibrotic tissue that can result from
repeated injections. The patients were instructed to abstain from
rinsing their oral cavity for a minimum of 1 h subsequent to
receiving the aforementioned trio of submucosal injections. The
inclusion of lignocaine was intended to alleviate irritation and
enhance the drug distribution. The injections were administered
bi-weekly for a period of 3 months. All patients were also
administered SM fibro tablets (Warren Pharmaceuticals, Pvt. Ltd.)
containing zinc, selenium, copper, β-carotene, α-lipoic acid,
vitamin E and lycopene, to be taken twice daily for 1 year. The
patients were also instructed to perform mouth opening exercises
regularly with ice cream sticks five times a day, to perform
massages with 0.1% triamcinolone oromucosal paste (Turbocort,
Indoco Remedies Ltd.) twice daily and to rinse with benzydamine
0.15% mouthwash (B-mine Dupen Laboratories Pvt. Ltd.) for 1 year
(11). All patients were followed-up
at monthly visits, and repeated reminders were sent to their mobile
phones to remind them to follow the prescription diligently and
refrain from using areca nuts, tobacco products, alcohol, and hot
and spicy foods.
The primary outcome of the study was to assess the
improvement in mouth opening with the intervention compared to the
control group. Measurements of mouth opening in millimeters were
conducted using a disposable measuring scale. Interincisal mouth
opening was determined by measuring the distance between the
mesioincisal angle of the upper central incisor and the
mesioincisal angle of the lower central incisor. A standardized
protocol was followed for all cases of OSMF (12). The secondary outcome was the
assessment of the improvement in the burning sensation felt by the
patients. A five-point Likert numeric scale was used to assess the
burning sensation (0, indicated no burning sensation; 1, indicated
a mild burning sensation; 2, indicated a moderate burning
sensation; 3, indicated a severe burning sensation; and 4,
indicated an extreme burning sensation) (13). All measurements were obtained at
baseline, and at the 4th, 8th and 12th week, and 12 months
following intervention, as described in previous studies (4,6,7).
Statistical analysis
The collected data were statistically analyzed by
the descriptive analysis of mean, range and standard deviation
using SPSS software version 22 (IBM Corp.). The Shapiro-Wilk test
was used to examine the normality of the data. For normally
distributed data, parametric tests, such as one-way ANOVA were used
for inter-group comparisons of the interincisal distance between
the groups, and repeated ANOVA was used for intra-group
comparisons, followed by post-hoc analysis using Tukey's test. For
data which were not normally distributed, non-parametric tests,
such as the Kruskal-Wallis test, was used for inter- and
intra-group comparisons of burning sensation between the groups,
followed by post-hoc analysis using Dunn's test. A value of
<0.05 was considered to indicate a statistically significant
difference.
Results
The baseline characteristics of the groups are
presented in Table I. All groups
exhibited non-significant differences as regards the demographic
characteristics of the patients, such as age, sex distribution, and
patients with grade 2 and 3 OSMF, which nullified the confounding
bias due to these factors (P>0.05). The number of patients with
grade 2 OSMF was greater than that of those with grade 3 OSMF. All
the males were mostly tobacco chewers, and few were betal quid
chewers (88%, 12% respectively), whereas all the females were betal
quid chewers. In total, 55% of the patients complained of the
presence of a white patch in their mouth, 88% complained of reduced
mouth opening, and 11% complained of a burning sensation. The
routine blood investigations yielded results which were within the
normal range in the majority of the patients (96%); only 5 patients
had an iron deficiency (mean value, 42±10.5 µg/dl), 3 patients had
an increased ESR (23.15±3.5 mm/h) and 4 patients had a vitamin B12
deficiency (mean value, 225.12±23.12 pg/ml). Although the study
initially enrolled 40 patients, a subset of patients was ultimately
excluded from the analysis at the conclusion of the 1-year
follow-up period. This exclusion was due to their resumption of the
habit of consuming areca nut or tobacco products, as well as to
their discontinuation of treatment attendance, despite repeated
reminders and counseling efforts.
 | Table IDemographic data and habits and
complaints of the patients included in the study groups. |
Table I
Demographic data and habits and
complaints of the patients included in the study groups.
| Demographics
(n=137) |
|---|
| Characteristic | Group 1 (n=32) | Group 2 (n=35) | Group 3 (n=35) | Group 4 (n=35) | P-value |
|---|
| No. of patients with
grade 2 OSMF | 21 (65%) | 22 (62.8%) | 21 (60%) | 22 (62.8%) | 0.971 (NS) |
| No. of patients with
grade 3 OSMF | 11 (35%) | 13 (37.2%) | 14 (40%) | 13 (37.8%) | |
| Average age, years,
mean ± SD | 33.1±3.2 | 34.2±2.7 | 32.6±3.8 | 34.6±2.1 | 0.053 (NS) |
| Males | 22 (69%) | 20 (57%) | 25 (71%) | 26 (74%) | 0.07 (NS) |
| Females | 10 (31%) | 15 (43%) | 10 (29%) | 9 (27%) | |
| Habits (n=137) |
| Type of habit | Group 1 (n=32) | Group 2 (n=35) | Group 3 (n=35) | Group 4 (n=35) | Total ratio (%) |
| Tobacco (M/F) | 20/00 | 16/00 | 23/00 | 23/00 | 82/00 (88/00%) |
| Betel quid (M/F) | 02/10 | 04/15 | 02/10 | 03/09 | 11/44 (12/100%) |
| Patient complaints
(n=137) |
| Type of
complaint | Group 1 (n=32) | Group 2 (n=35) | Group 3 (n=35) | Group 4 (n=35) | Total ratio (%) |
| White patch | 15 | 20 | 19 | 21 | 75 (55%) |
| Reduced mouth
opening | 25 | 32 | 31 | 32 | 120 (88%) |
| Burning
sensation | 03 | 04 | 03 | 05 | 15 (11%) |
| Blood profiles
(n=137) |
| Blood parameter | Group 1 (n=32) | Group 2 (n=35) | Group 3 (n=35) | Group 4 (n=35) | Total ratio (%) |
| Increased ESR | 0 | 1 | 1 | 1 | 3 (2%) |
| Low serum iron | 1 | 2 | 2 | 0 | 5 (3.5%) |
| Low vitamin B12 | 0 | 1 | 2 | 1 | 4 (3%) |
Statistically significant differences were noted
between the groups for improvement in mouth opening and burning
sensation, and therefore, the null hypothesis was rejected. The
mean mouth opening increased in all groups, with highly
statistically significant differences observed in the experimental
groups (P<0.001) and non-significant differences were noted in
the control group (P=0.067), from baseline to the end of the
follow-up period at 1 year. There was a gradual increase in mouth
opening in all groups from baseline to the 12th week of treatment,
although this relapsed by the end of 1year. A maximum increase of
7.30±0.80 mm was noted in group 4, followed by 5.94±0.84 mm in
group 2, 5.11±0.92 mm in group 3, and least in the control group
(group 1) of 0.37±0.16 mm, from baseline to the end of 12th week.
No significant differences were observed between the groups at
baseline. This indicated that all groups were comparable at
baseline with similar mouth opening, which nullified the
confounding bias due to variable differences in the groups at
baseline (P=0.85). The maximum increase in mouth opening was noted
at the 12th week in group 4, followed by group 2, and the lowest in
the control group. The maximum relapse of 1.62±0.45 mm was observed
in group 2, followed by 0.52±0.83 mm relapse in group 3, and a
minimum relapse of 0.20±0.08 mm was observed in group 4, as shown
in Table II.
| Table IIComparison of mean mouth opening (in
mm) at different time intervals in the study groups using
ANOVA. |
Table II
Comparison of mean mouth opening (in
mm) at different time intervals in the study groups using
ANOVA.
| | Baseline (mean ±
SD) | 4th week (mean ±
SD) | 8th week (mean ±
SD) | 12th week (mean ±
SD) | 12th month (mean ±
SD) | ANOVA between
intervals (P-value) |
|---|
| Group 1 | 22.18±1.44 | 22.44±1.53 | 22.58±1.67 | 22.54±1.47 | 22.74±1.32 | 0.067 |
| Group 2 | 22.08±1.51 | 24.80±1.68 | 27.01±1.83 | 28.03±1.83 | 26.41±1.78 | 0.001b |
| Group 3 | 22.15±1.35 | 24.04±1.39 | 25.84±1.58 | 27.26±1.59 | 26.76±1.54 | 0.001b |
| Group 4 | 22.32±1.36 | 25.40±1.61 | 27.79±1.73 | 29.62±1.88 | 29.33±1.65 | 0.001b |
| ANOVA between
groups (P-value) | 0.85 | 0.02a | 0.003a | 0.001b | 0.001b | |
Upon further comparison of the groups by post-hoc
analysis at the 12th week, it was noted that non-significant
differences were observed between groups 2 and 3 as regards the
increase in mouth opening, whereas statistically significant
differences were found between the control group and the
experimental groups, as shown in Table
III.
| Table IIIIntragroup analysis of mean mouth
opening at the 12th week in the different study groups using
Tukey's post-hoc analysis. |
Table III
Intragroup analysis of mean mouth
opening at the 12th week in the different study groups using
Tukey's post-hoc analysis.
| Intragroup
comparison | P-value |
|---|
| Group 1 vs. group
2 | 0.0001b |
| Group 1 vs. group
3 | 0.0001b |
| Group 1 vs. group
4 | 0.0001b |
| Group 2 vs. group
3 | 0.131 |
| Group 2 vs. group
4 | 0.01a |
| Group 3 vs. group
4 | 0.0001b |
Groups 1, 2 and 3 exhibited no improvement in
burning sensation at 1 month of treatment, and thereafter,
exhibited a decrease until 1 year of follow-up. Group 4 exhibited a
decrease in burning sensation from baseline until 1 year of
follow-up. At baseline, all groups were similar, with no
significant differences, which nullified the confounding bias of
variable differences in the groups. The maximum reduction in
burning sensation was observed in group 4, followed by groups 3 and
2, and the least reduction was observed in the control group, as
shown in Table IV. Post-hoc
analysis using Dunn's test at the 12th week of follow-up revealed
that the patients in whom placental extract injection was
administered exhibited non-significant differences in the reduction
of burning sensation when compared to patients in whom a mixture of
dexamethasone and hyaluronidase was administered. However,
intralesional injections of medications significantly reduced the
burning sensation compared with the control group, as shown in
Table V.
| Table IVComparison of the mean scores of
burning sensation at the different time intervals in study groups
using the Kruskal-Wallis test. |
Table IV
Comparison of the mean scores of
burning sensation at the different time intervals in study groups
using the Kruskal-Wallis test.
| Groups | Baseline (mean ±
SD) | 4th week (mean ±
SD) | 8th week (mean ±
SD) | 12th week (mean ±
SD) | 12th month (mean ±
SD) | Kruskal-Wallis test
between time intervals (P-value) |
|---|
| Group 1 | 3.09±0.68 | 3.09±0.68 | 2.62±0.66 | 2.15±0.44 | 1.34±0.65 | 0.001b |
| Group 2 | 3.11±0.63 | 3.11±0.63 | 2.28±0.45 | 1.25±0.44 | 0.82±0.61 | 0.001b |
| Group 3 | 3.20±0.63 | 3.20±0.63 | 2.31±0.47 | 1.45±0.50 | 0.45±0.50 | 0.001b |
| Group 4 | 3.37±0.59 | 2.37±0.59 | 1.42±0.50 | 0.42±0.50 | 0.22±0.42 | 0.001b |
| Kruskal-Wallis
between groups (P-value) | 0.272 (NS) | 0.001b | 0.001b | 0.001b | 0.001b | |
| Table VIntragroup analysis of the mean
scores of burning sensation at the 12th week in the different study
groups using Dunn's post-hoc test. |
Table V
Intragroup analysis of the mean
scores of burning sensation at the 12th week in the different study
groups using Dunn's post-hoc test.
| Intragroup
comparison | P-value |
|---|
| Group 1 vs. group
2 | 0.01a |
| Group 1 vs. group
3 | 0.001b |
| Group 1 vs. group
4 | 0.001b |
| Group 2 vs. group
3 | 0.12 (NS) |
| Group 2 vs. group
4 | 0.01a |
| Group 3 vs. group
4 | 0.01a |
Discussion
OSMF is highly prevalent among the Indian
population. Given its potential for premalignancy (5.6%) and the
severity of clinical manifestations, numerous studies have been
conducted by various authors to investigate different facets of
this condition, such as scleroderma, including its etiology,
pathogenesis and treatment. However, the precise etiology and
pathogenesis of OSMF remain unclear (1-3).
Chewing areca nuts is the most prevalent causal factor for OSMF.
The predominant practice involves placing a betel quid in the
vestibule for various durations of time and frequencies. The
continuous interaction between betel quid and the oral mucosa leads
to the absorption and metabolic processing of quid alkaloids and
flavonoids. These components, along with their metabolites, act as
persistent sources of irritation in the oral mucosa. Furthermore,
the inclusion of coarse fibers in betel quid results in mechanical
irritation of the oral mucosa. The resulting microtrauma caused by
the ongoing friction of these coarse fibers from the areca nut
facilitates the diffusion of betel quid alkaloids and flavonoids
into the connective tissue beneath the epithelium, leading to
infiltration of inflammatory cells into the juxta-epithelial region
(3).
In the present study, the majority of the males were
tobacco chewers (88%), and all the females were betel quid chewers;
similar findings were observed in a study conducted on Indian
females (3). The history of habits
ranged from a minimum of 2 to 5 years in the majority of patients,
which depicts the slow, progressive nature of OSMF (2). Patients chew tobacco or betel quid to
4-5 times per day. The chief complaint of the patients was a
reduction in mouth opening (88%), and some patients complained of a
mild to moderate burning sensation (11%).
The initial symptoms of OSMF are a burning
sensation, pain and ulceration, which are predominantly observed in
patients with grade 1 OSMF. In the present study, as the included
patients had grade 2 and 3 OSMF, it was revealed that the majority
of the patients had a mild to moderate burning sensation (63% of
the patients had grade 2 OSMF, and 37% of the patients had grade 3
OSMF). This may be due to the presence of a maximum number of
degranulated mast cells in the initial stages of OSMF, which
decreases as the stage of OSMF progresses (14). With the advancing stage of OSMF,
fibrosis increases in the underlying connective tissues, leading to
reduced mouth opening. The majority of the patients had reduced
mouth opening and fibrosis with blanching of the oral mucosa. This
may be due to an increase in collagen synthesis as a result of the
active components of betel nuts. Recently, exosomes originating
from mesenchymal stem cells obtained from human adipose tissue have
demonstrated the ability to enhance the proliferative and migratory
capabilities of myofibroblasts, while also impeding the deposition
of collagen and the process of trans-differentiation in
vitro. Exosomes regulate the TGF-β pathway within
myofibroblasts and exhibit antifibrotic properties, rendering them
a potentially favorable therapeutic modality for treating OSMF
(15).
In the present study, few patients with OSMF had an
increased ESR, iron and vitamin B12 deficiency, as also observed in
a previous study (16). OSMF can be
identified as a collagen metabolic disorder that arises from the
excess production of extensively interconnected insoluble collagen
type I. Collagen hydroxylation requires the presence of ferrous
iron and ascorbic acid. The utilization of iron in the
hydroxylation of proline and lysine results in a reduction in serum
iron levels, which further leads to a decrease in vascularity and
facilitating fibrosis (17). Iron
and Vitamin B12 deficiencies arise mainly due to impaired food
intake, resulting from ulceration and a burning sensation in the
initial stages of OSMF, leading to an impairment in the
inflammatory reparative response of the lamina propria, which
ultimately leads to the progression of OSMF (18). Therefore, patients with an iron or
Vitamin B12 deficiency were administered supplements apart from
other prescribed interventions.
In the present study, the local administration of
placental extracts led to a significant improvement in mouth
opening by 5.94±0.84 mm after 12 weeks of treatment, but relapsed
by 1.62±0.45 mm after 1 year follow-up. These findings are
consistent with those of previous studies (6,13).
Placental extracts contain growth factors (TGF, FGF and VEGF) that
can reduce inflammation and inhibit platelet aggregation. The
activity of placental extract primarily involves the stimulation of
biogenesis, and its application is based on the principles of
tissue therapy. According to this hypothesis, tissues undergo a
process of biogenic adaptation, resulting in the generation of
substances necessary for their sustenance and vitality through
biogenic stimulation (13).
In the present study, the injection of dexamethasone
and hyaluronidase resulted in improvement of mouth opening by
5.11±0.92 mm after 12 weeks of treatment. Although it was not
significantly different from the placental extract group, a relapse
of 0.52±0.83 mm only was noted after 1 year of follow-up, which was
less than that in the placental extract group (1.62±0.45 mm). The
improvement in the burning sensation was also greater than that in
the control group. These findings are consistent with those of
previous studies (4,5,8).
However, these findings contradict those of Kisave et al
(7) who reported a statistically
significant improvement in mouth opening by hydrocortisone,
compared to placentrex. The disparity in the results may be due to
the differences in methodology. Dexamethasone plays a crucial role
in the suppression of the immune system by reducing the activity
and volume of the lymphatic system. By inhibiting the migration of
polymorphonuclear leukocytes and reversing capillary permeability,
it effectively diminishes inflammatory components and burning
sensations in patients with OSMF. As a corticosteroid for
intralesional injections, it demonstrates superior local potency, a
prolonged duration of action and minimal systemic absorption.
Steroids contribute to the initial alleviation of symptoms in
patients with limited mouth opening by clearing juxta-epithelial
inflammation and promoting collagen formation (19). Hyaluronidase is an enzyme that
diminishes the density of the ground substance and consequently
augments the permeability of tissues to injected corticosteroids.
It stimulates the hydrolysis of hyaluronic acid, a major component
of tissue cement, which hinders the dispersion of fluids through
tissues. Furthermore, it facilitates the dispersion and
assimilation of injection locally (20).
The present study indicated that the combination of
placental extracts, dexamethasone and hyaluronidase led to a
maximum improvement of 7.30±0.80 mm in mouth opening, with a
minimum relapse of 0.20±0.08 mm after 1 year of follow-up. The
maximum improvement in burning sensation was also observed in this
group (group 4). This may be due to the synergistic effects of
various drugs used in combination. These findings are in agreement
with those of the study by Shrinivas et al (21); however, Shrinivas et al
(21) did not compare this
combination with single drugs. The research conducted by Borle and
Borle (22) hypothesized that the
administration of different drugs through intralesional injections
contributes to intensified fibrosis and significant trismus. The
deteriorating effect of submucosal injections on this condition may
be attributed to the repeated penetration of the needle into the
soft tissues at various locations, clinical irritation caused by
the injected drugs, and the progressive nature of the disease
(22). To the best of our knowledge,
there is a lack of published literature offering a universally
accepted protocol and recommending an optimal pharmacological
regimen for the treatment of OSMF. For patients with OSMF who are
at the advanced stages of the disease and are undergoing complex
surgical procedures, alternative options exist, such as the
utilization of scalpel blades, electrocautery and laser therapy
(23).
In the present study, the control group, who was
administered oral medications, along with mouth opening exercises,
also exhibited an improvement in signs and symptoms. Although the
difference was not significant, it was less prominent when compared
with the treatment with the intralesional injections of various
drugs. The use of antioxidants containing lycopene can counteract
the detrimental impact of free radicals via physical and chemical
means, thereby safeguarding cellular constituents against
impairment caused by highly reactive oxygen species. However, the
efficacy of lycopene as a standalone therapeutic agent has been
found to be suboptimal compared with combination therapies in terms
of enhancing mouth opening (11).
Previous research has shown a significant improvement in mouth
opening with mouth exercises, which was not observed in the present
study (24). This may be due to the
non-performance of mouth-opening exercises regularly by patients
despite repeated reminders.
The previous systematic review conducted by More
et al (25) demonstrated that
a comprehensive treatment approach involving the use of nutritional
supplements and intralesional injection therapy was efficacious in
the management of OSMF, as observed in the present study. However,
it is imperative to investigate newer and more sophisticated
approaches for the direct administration of therapeutic agents into
affected areas to address the tendency towards fibrosis.
The present study had certain limitations, which
should be mentioned. Sex differences could not be evaluated in the
present study, as the disease was predominantly observed in the
male population. As the investigation was performed on individuals
from rural communities who had limited financial resources, mouth
opening exercises were executed using traditional ice-cream sticks
instead of mouth-exercising devices. Additionally, this particular
study was conducted as a single-center study owing to ethical and
financial constraints. It should be noted that the occurrence of
fibrosis resulting from repeated intra-lesional injections,
although not proven, was not assessed in the present study.
Therefore, further long-term, multicenter, randomized controlled
trials with long-term follow-up periods are warranted.
In conclusion, although there is no single treatment
modality for the successful treatment of OSMF, the present study
found that the intralesional injection of combination drugs, such
as 2 ml placental extracts, 1 ml hyaluronidase, 1 ml dexamethasone,
mixed with 1 ml of 2% lignocaine, along with SM fibro tablets twice
daily, mouth opening exercises, massaging with 0.1% triamcinolone
oromucosal paste twice daily and rinsing with benzydamine 0.15%
mouthwash, is highly effective in improving mouth opening and the
burning sensation in patients with grade 2 and 3 OSMF. A minimal
relapse of 0.2 mm was observed after 1 year of follow-up. Future
research is required however, to focus on conducting extensive
clinical trials and longitudinal studies to validate the safety and
efficacy of this treatment approach. In addition, it is crucial to
focus on preventive measures by educating young individuals on the
disease and on the risks of using tobacco products and betel
quid.
Acknowledgements
The authors acknowledge Dr Manish Sharma, Professor
at the Department of Oral Pathology at Jawahar Medical Foundation's
ACPM Dental College (Dhule, India) for providing guidance with the
statistical analysis.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
JG conceived and supervised the study, and was also
involved in the acquisition of cases, and in reviewing the
manuscript. SI was involved in the acquisition of cases, performing
treatment and in reviewing the manuscript. CP was involved in
performing treatment, and in the interpretation of the burning
sensation and trismus of the patients. UB was involved in reviewing
the literature for related studies, in the statistical analysis,
and in reviewing the manuscript. JJ was involved in the selection
of cases, and in the drafting and reviewing of the manuscript. KP
was involved in the selection of cases, in the interpretation of
data and in reviewing the manuscript. All authors have read and
approved the final manuscript. JG and SI confirm the authenticity
of all the raw data.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Ethical Committee of Jawahar Medical Foundation Annasaheb Chudaman
Patil memorial Dental College (EC/NEW/INST/2022/2959/2022/63).
Written informed consent was obtained from all patients for
participation in the present study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Singh P, Mittal R, Chandak S, Bhondey A,
Rathi A and Chandwani M: Prevalence of oral submucous fibrosis in
children of rural areas of Nagpur, Maharashtra, India. Int J Prev
Clinic Dent Res. 3:243–245. 2016.
|
|
2
|
Venkatesh R, Shah PH, More CB and Patil
DJ: Insight into history of Areca nut and oral submucous fibrosis:
A narrative review. Indian J Hist. Sci. 57:87–90. 2022.
|
|
3
|
Hande AH, Chaudhary MS, Gawande MN,
Gadbail AR, Zade PR, Bajaj S, Patil SK and Tekade S: Oral submucous
fibrosis: An enigmatic morpho-insight. J Cancer Res Ther.
15:463–469. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Shah PH, Venkatesh R, More CB and
Vassandacoumara V: Comparison of therapeutic efficacy of placental
extract with dexamethasone and hyaluronic acid with dexamethasone
for oral submucous fibrosis-A retrospective analysis. J Clin Diagn
Res. 10:ZC63–ZC66. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
James L, Shetty A, Rishi D and Abraham M:
Management of oral submucous fibrosis with injection of
hyaluronidase and dexamethasone in grade III oral submucous
fibrosis: A retrospective study. J Int Oral Health. 7:82–85.
2015.PubMed/NCBI
|
|
6
|
Reddy CN, Belaldavar BP and Havaldar RR:
study of efficacy of intraoral submucosal injections of
corticosteroids and placentrex in the management of oral submucous
fibrosis. Indian J Otolaryngol Head Neck Surg. 74 (Suppl
2):S1996–S2001. 2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kisave P, Shekhar V, Babu PS, Hussaini
SWU, Bhanot R, Kumar A and Tiwari RVC: The study of placentrex and
hydrocortisone as an adjunct treatment in oral submucous fibrosis.
J Family Med Prim Care. 9:2469–2474. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Naik SM, Appaji MK, Ravishankara S,
Goutham MK, Devi NP, Mushannavar AS and Naik SS: Comparative study
of intralesional triamcinolone acetonide and hyaluronidasevs
placental extract in 60 Cases of oral submucous fibrosis. Int J
Head Neck Surg. 3:59–65. 2012.
|
|
9
|
Hariton E and Locascio JJ: Randomised
controlled trials- the gold standard for effectiveness research:
Study design: Randomised controlled trials. BJOG.
125(1716)2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Passi D, Bhanot P, Kacker D, Chahal D,
Atri M and Panwar Y: Oral submucous fibrosis: Newer proposed
classification with critical updates in pathogenesis and management
strategies. Natl J Maxillofac Surg. 8:89–94. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rai A, Shrivastava PK, Kumar A, Kumar A,
Prasad K, Shakeel S and Ul Haque Z: Comparative effectiveness of
medicinal interventions for oral submucous fibrosis: A network
meta-analysis. J Stomatol Oral Maxillofac Surg.
124(101423)2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Sharma SR, Chavan S, Karjodkar FR, Sansare
K, Bharathi S and Singh S: Correlation of Clinical features in oral
submucous fibrosis: A 9-year retrospective study. Ethiop J Health
Sci. 32:137–44. 2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Zuali L, Mohiyuddin SMA, A S, Mohammadi K
and Paul I: Comparison between clinical outcome of intralesional
human placental extract alone and topical application of placental
extract gel after fibrotomy in oral submucous fibrosis. Cureus.
15(e40105)2023.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gupta S, Sharma M, Banerjee S, Holikatti
K, Kamble P and Goyal JV: The immunolocalization of mast cells in
the pathology of oral submucous fibrosis. Cureus.
15(e40069)2023.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Shao Z, Xu J, Xu X, Wang X, Zhou Y, Li Y
and Li K: Exosomes derived from human adipose mesenchymal stem
cells inhibits fibrosis and treats oral submucous fibrosis via the
miR-181a-5p/Smad2 Axis. Tissue Eng Regen Med. 21:123–135.
2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Abidullah M, Gaddikeri K, Anjum B,
Vairagare S, Tarani K and Seethamsetty S: Evaluation of
hematological profile in oral submucous fibrosis. Cureus.
14(e21926)2022.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Bhattacharya PT, Khaitan T, Sarkar SB and
Sinha R: Oral submucous fibrosis secondary to iron deficiency
anemia: A case report, etiopathogenesis and management. J Nutr
Health Aging. 20:205–208. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Xu H, Lyu FY, Song JY, Xu YM, Jiang EH,
Shang ZJ, Chen LL and Xu Z: Research achievements of oral submucous
fibrosis: Progress and prospect. Biomed Res Int.
2021(6631856)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Singh DT, Padshetty S, Shreen S, Begum N,
Vishwakarma SK and Khan AA: Injection placental in the management
of oral submucous fibrosis. Int J Mod Sci Eng Technol. 2:23–30.
2015.
|
|
20
|
Tilakaratne WM, Ekanayaka RP, Herath M,
Jayasinghe RD, Sitheeque M and Amarasinghe H: Intralesional
corticosteroids as a treatment for restricted mouth opening in oral
submucous fibrosis. Oral Surg Oral Med Oral Pathol Oral Radiol.
122:224–231. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Shrinivas , Shushma G and Kantly R:
Management of oral submucous fibrosis by combined oral medication
and intralesional injection: A treatment strategy. MedPulse-Int J
Dent. 7:1–5. 2018.
|
|
22
|
Borle RM and Borle SR: Management of oral
submucous fibrosis: A conservative approach. J Oral Maxillofac
Surg. 49:788–791. 1991.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Shen YW, Shih YH, Fuh LJ and Shieh TM:
Oral submucous fibrosis: A review on biomarkers, pathogenic
mechanisms, and treatments. Int J Mol Sci. 21(7231)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Gondivkar SM, Gadbail AR, Sarode SC,
Gondivkar RS, Patil S, Gaikwad RN and Yuwanati M: Clinical efficacy
of mouth exercising devices in oral submucous fibrosis: A
systematic review. J Oral Biol Craniofac Res. 10:315–320.
2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
More CB, Jatti Patil D and Rao NR:
Medicinal management of oral submucous fibrosis in the past
decade-A systematic review. J Oral Biol Craniofac Res. 10:552–568.
2020.PubMed/NCBI View Article : Google Scholar
|