Introduction
The ovaries are characterized by the occurrence of
neoplasms with diverse clinical, morphological and histological
features, and their pre-operative evaluation is considered to
greatly contribute to the diagnostic approach and further
management of these tumors (1). In
the majority of cases (80%), ovarian tumors are benign and
typically occur in young women between the ages of 20 and 45 years.
The most common benign ovarian neoplasms are epithelial tumors,
which are usually diagnosed in women of reproductive age. Malignant
ovarian neoplasms, which account for ~20% of cases, are more
commonly found in older women, between the ages of 40 and 65 years,
and are generally associated with a poor prognosis (2). A distinct category of epithelial
ovarian tumors are borderline malignant tumors, whose
characteristics fall between those of benign and malignant
categories (3).
Fibroma, thecoma and fibrothecoma are benign ovarian
stromal tumors characterized by the presence of fibroblastic
stromal cells and/or cells resembling luteinized theca cells
(4). Ovarian fibromas, first
described in 1983 by Young and Scully (5), are the most frequent solid ovarian
neoplasms and account for ~1 to 4.7% of ovarian tumors (6). They are usually unilateral, non-hormone
producing, and in most cases are diagnosed during the fifth to
sixth decade of life in peri-menopausal or menopausal women
(7). In some patients, ovarian
fibromas, particularly when large, can lead to severe
complications, such as torsion of the ipsilateral adnexa,
necessitating immediate surgical intervention (6).
The present study describes a rare case of torsion
of a large ovarian fibroma in a woman of reproductive age, which
did not manifest with the expected intensity of torsion; it rather
mimicked several clinical, biochemical and imaging features of a
solid ovarian carcinoma. The aim of the present case report was to
highlight this uncommon manifestation, explore its differential
diagnosis from malignancy and provide a brief review of the current
diagnostic and treatment algorithms for this condition, in order to
assist clinicians encountering similar conditions in their
practice.
Case report
A 48-year-old woman with a history of four full-term
vaginal deliveries, presented to the Emergency Department of the
General Hospital of Trikala, Trikala, Greece, with a 1-week history
of low-grade fever and abdominal pain. The pain was located in the
lower abdomen, radiating mainly to the right iliac fossa. It was of
mild intensity, continuous in nature, and accompanied by nausea and
a mild sensation of abdominal distension. The pain was not
associated with vomiting or diarrhea. The low-grade fever
reportedly began ~2 days following the onset of the abdominal pain.
The patient had an elevated body mass index (29.3) and a regular
menstrual cycle. She had not visited a gynecologist in the past 18
years, following her last childbirth. Her medical history included
hypothyroidism and arterial hypertension, both of which were
well-controlled with medication. The patient also reported having
undergone an appendectomy ~20 years prior.
Upon a clinical examination, her body temperature
was found to be 37.7˚C, and her blood pressure and pulse rate were
within normal range (125/75 mmHg and 85 beats/min, respectively).
Palpation of the abdomen revealed mild tenderness, particularly in
the right iliac fossa, without any signs of peritoneal irritation.
The levels of inflammatory markers were found to be slightly
elevated, as were the levels of tumor markers (Table I). The findings from the transvaginal
and transabdominal ultrasound were inconclusive. A subsequent
computed tomography (CT) scan revealed a large, well-circumscribed
solid mass with thick walls, located between the rectosigmoid
colon, the large bowel and the uterus, without contrast enhancement
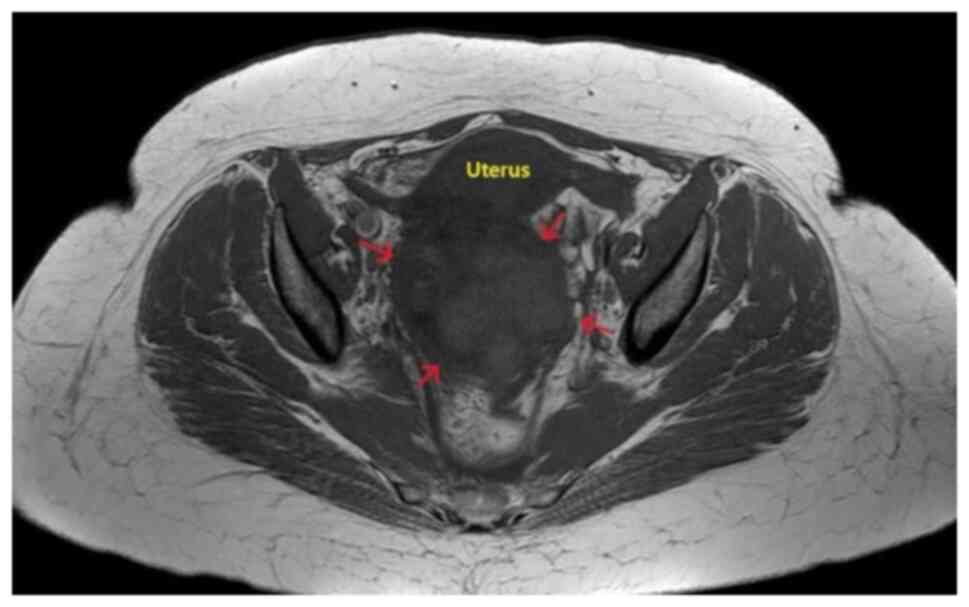
of its interior, but with wall and septal enhancement. Magnetic
resonance imaging (MRI) of the right adnexal region demonstrated a
large heterogeneous lesion measuring ~10x8.5 cm, with cystic and
necrotic areas inside, as well as regions of intermediate-to-high
signal intensity on T1 and low signal on T2 sequences (Fig. 1). The left ovary appeared normal.
Additionally, there was diffuse fat stranding in the pelvic cavity,
free fluid collection, and the presence of multiple mildly enlarged
para-aortic and iliac lymph nodes. All investigations were
inconclusive as regards the presence or absence of malignancy.
 | Table ILaboratory tests of the patient upon
arrival at the emergency department and during hospitalization. |
Table I
Laboratory tests of the patient upon
arrival at the emergency department and during hospitalization.
| Laboratory tests | Day of arrival at the
ED | 1st Day of
hospitalization | 3rd Day of
hospitalization | 5th Day of
hospitalization | 1st Post-operative
day | 2nd Post-operative
day | 4th Post-operative
day | 1st Post-operative
month | Normal laboratory
values |
|---|
| Ht | 37.4% | 35.6% | 34.3% | 33.9% | 30.1% | 29.2% | 30.7% | - | 37.7-49.7% |
| Hb | 12.9 g/dl | 11.9 g/dl | 11.1 g/dl | 10.9 g/dl | 9.9 g/dl | 9.3 g/dl | 10.1 g/dl | - | 11.8-17.8 gr/dl |
| PLT |
239x103/ml |
224x103/ml | 213
x103/ml |
210x103/ml |
201x103/ml |
205x103/ml |
217x103/ml | - |
150-350x103/ml |
| WBC |
17.8x103/ml |
15.3x103/ml | 14.1
x103/ml |
13.7x103/ml |
22.4x103/ml |
14.1x103/ml |
9.4x103/ml | - |
4-10.8x103/ml |
| NEUT | 84.4% | 84.1% | 83.2% | 81.9% | 92.9% | 84.1% | 73.2% | - | 40-75% |
| CRP | 25.70 mg/dl | 26.99 mg/dl | 22.55 mg/dl | 19.95 mg/dl | 19.91 mg/dl | 10.32 mg/dl | 4.37 mg/dl | - | <0.7 mg/dl |
| APTT | 30.4 sec | 30.9 sec | 31.8 sec | 33.9 sec | 32.8 sec | 30.7 sec | 29.8 sec | - | 24.0-35.0 sec |
| INR | 1.25 | 1.27 | 1.28 | 1.37 | 1.41 | 1.25 | 1.17 | - | 0.8-1.2 |
| FIB | 421 mg/dl | 437 mg/dl | 447 mg/dl | 565 mg/dl | 513 mg/dl | 491 mg/dl | 373 mg/dl | - | 200-400 mg/dl |
| Glu | 112 mg/dl | 85 mg/dl | 91 mg/dl | 85 mg/dl | 91 mg/dl | 85 mg/dl | 84 mg/dl | - | 75-115 mg/dl |
| Cr | 0.62 mg/dl | 0.56 mg/dl | 0.63 mg/dl | 0.66 mg/dl | 0.67 mg/dl | 0.63 mg/dl | 0.51 mg/dl | - | 0.40-1.10 mg/dl |
| Κ+ | 4.25 mmol/l | 4.66 mmol/l | 4.61 mmol/l | 4.32 mg/dl | 4.21 mg/dl | 4.11 mg/dl | 4.09 mg/dl | - | 3.5-5.1 mmol/l |
| Να+ | 136.5 mmol/l | 139.2 mmol/l | 138.1 mmol/l | 139.1 mmol/l | 138.9 mmol/l | 141.2 mmol/l | 141.4 mmol/l | - | 136-145 mmol/l |
| TBIL | 0.60 mg/dl | 0.48 mg/dl | - | - | 0.51 mg/dl | - | - | - | 0.3-1.2 mg/dl |
| DBIL | 0.07 mg/dl | 0.12 mg/dl | - | - | 0.11 mg/dl | - | - | - | 0.0-0.5 mg/dl |
| INBIL | 0.27 mg/dl | 0.31 mg/dl | - | - | 0.35 mg/dl | - | - | - | 0.0-0.7 mg/dl |
| SGOT | 19 IU/l | 17 IU/l | - | - | 18 IU/l | - | - | - | 5-33 IU/l |
| SGPT | 18 IU/l | 15 IU/l | - | - | 19 IU/l | - | - | - | 10-37 IU/l |
| AMY | 21 IU/l | 22 IU/l | - | - | 21 IU/l | - | - | - | 30-118 IU/l |
| CEA | 5.1 ng/ml | - | - | - | - | - | - | 0.8 ng/ml | <5 ng/ml |
| CA125 | 82.6 U/ml | - | - | - | - | - | - | 7 U/ml | ≤35 U/ml |
| CA15-3 | 31.4 U/ml | - | - | - | - | - | - | 12.4 U/ml | 0.0-31.3 U/ml |
| CA19-9 | 40.7 U/ml | - | - | - | - | - | - | 3.3 U/ml | 0.0-37 U/ml |
The combination of imaging findings, persistent
clinical symptoms and the continued elevation of the levels of
inflammatory markers despite intravenous treatment with antibiotics
[cefoxitin (Mefoxil®) at a dose of 2 g every 8 h and
metronidazole (Flagyl®) 500 mg three times a day], led
to the decision to perform a laparotomy, without having excluded
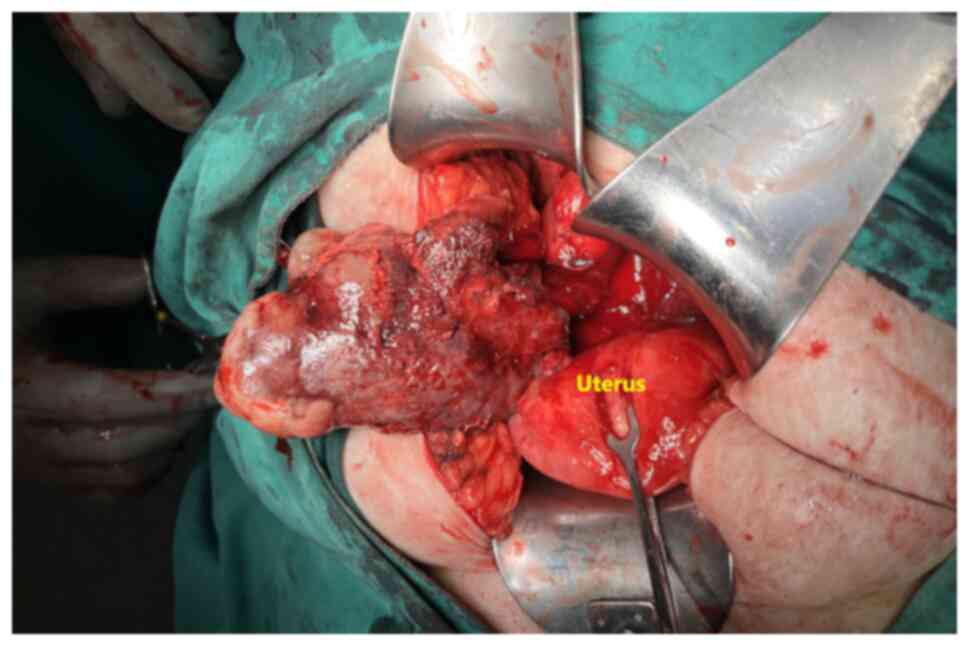
the diagnosis of solid ovarian cancer. Intraoperatively, a solid
ovarian mass with torsion and marked inflammation was identified
(Fig. 2). A frozen section indicated
a benign tumor; however, this did not allow for definitive tumor
classification. A total hysterectomy with bilateral
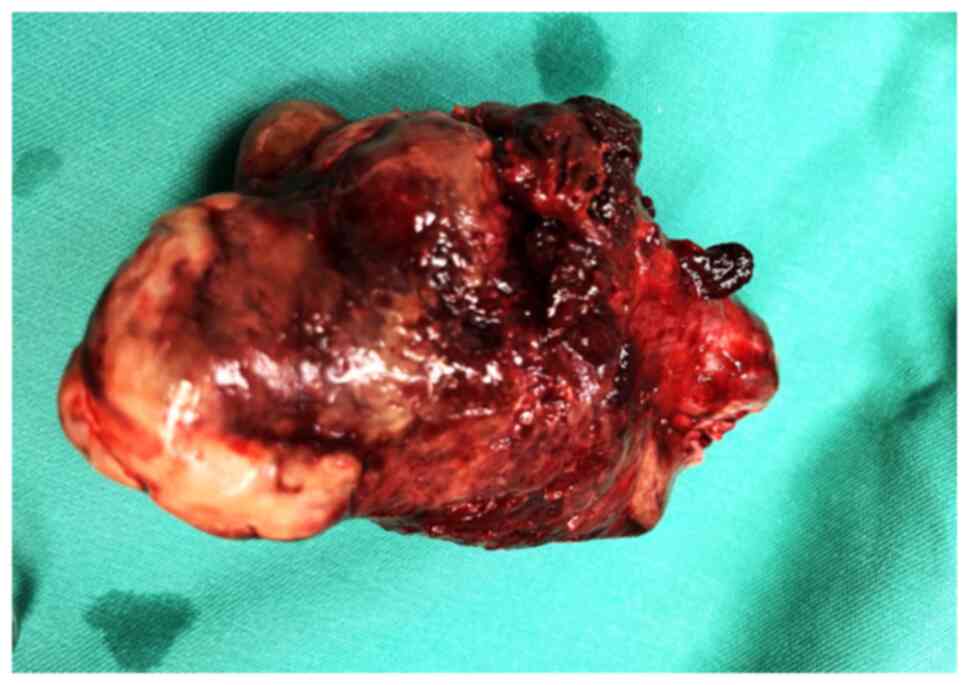
salpingo-oophorectomy was performed. A macroscopic histological
examination revealed a solid ovarian mass measuring 11x8x6.5 cm
with a lobulated brown outer surface. Sectioning of the mass
revealed a firm, elastic texture with areas of hemorrhage, findings
consistent with an ovarian fibroma (Fig.
3).
The specimens were subsequently sent for
histopathological assessment at the laboratory of the hospital. As
per the routine protocol, the specimens were embedded in paraffin
cubes and 5-µm-thick sections were obtained for the analysis. A
buffered, 10% formalin solution was utilized as a fixative medium,
for 36 h at room temperature. Hematoxylin and eosin 0.5% alcohol
(Diachel A.E.) staining was used, at room temperature with a 12-min
duration. All microscopic examinations were performed using a LEICA
DM2000 optical microscope (Leica Microsystems GmbH). The
histological examination of the surgical specimen confirmed the
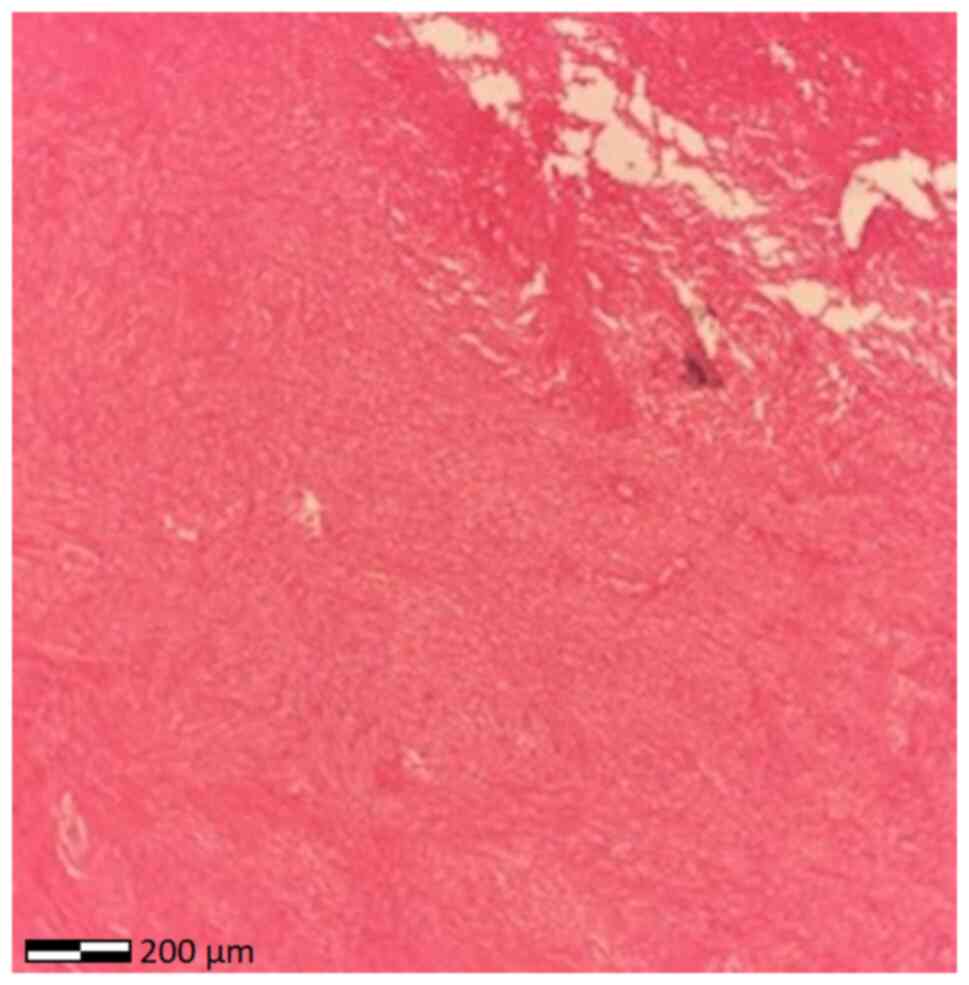
diagnosis of pedunculated submucosal uterine leiomyoma (Fig. 3). A microscopic examination revealed
vascular congestion, hemorrhagic infiltration and ischemic necrosis
of the ovarian tumor, indicative of adnexal torsion (Fig. 4).
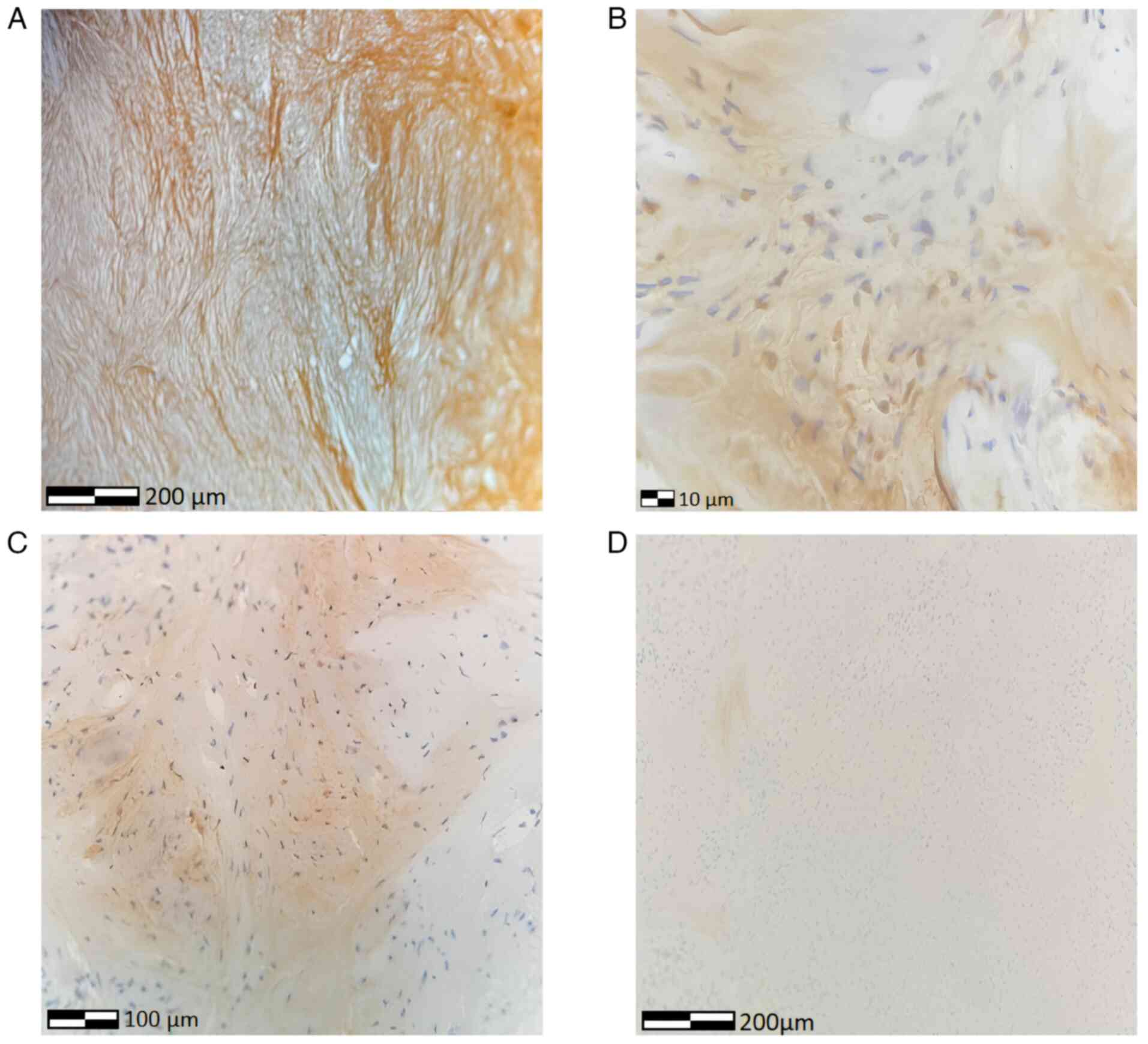
In addition, an immunohistochemical analysis was
performed. The sections used were 4-µm-thick, were
paraffin-embedded and were dewaxed for 40 min at 70˚C. The analysis
was performed using the automated BOND-LEICA system (Leica
Biosystems). The sections were placed sequentially in BOND Dewax
solution, 100% v/v ethanol solution and BOND wash solution. For
reticulin staining, the Reticulin Stain kit (cat. no. 25094,
Polysciences) was used in accordance with the manufacturer's
instructions. Oxidizer solution (1% potassium permanganate,
Reticulin Stain kit, cat. no. 25094, Polysciences) was applied for
5 min at room temperature and subsequently the slices were rinsed
in distilled water twice for 1 min at a time. The same procedure
(solution bath and rinsing) was performed with a
decolorizer/reducer solution (1% oxalic acid, Reticulin Stain kit,
cat. no. 25094, Polysciences) and sensitizer solution (2.5% ferric
ammonium sulfate, Reticulin Stain kit, cat. no. 25094,
Polysciences). Finally, the slices were ready for silver
impregnation, via a bath in a silver working solution (10% silver
nitrate, 30% ammonium hydroxide and 3% sodium hydroxide, Reticulin
Stain kit, cat. no. 25094, Polysciences) for 20 min and subsequent
rinsing as described above. The slices were bathed in a developer
solution (10% formalin) for 4 min, rinsed, bathed in a fixing
solution (5% sodium thiosulphate) for 2 min at room temperature,
rinsed and counterstained with (Reticulin Stain kit, cat. no.
25094, Polysciences) for 5 min at room temperature, before being
rinsed, dehydrated in graded alcohols and mounted for microscopy
(see below).
For antigen retrieval, BOND proprietary Heat Induced
Epitope Retrieval (HIER) solution was used for 20 min in 100˚C and
pH 8. The block peroxide kit (Bond; Leica Biosystems) was
subsequently used for 5 min. For WT1, the anti-WT1 antibody (cat.
no. AMAb91842, Atlas Antibodies) was used at a 1:1,200 dilution.
For inhibin, the 27331-1-AP antibody (cat. no. Ag25999, Proteintech
Group, Inc.) was used at a 1:800 dilution. For calretinin, the
82811-1-RR antibody (cat. no. Ag2924, Proteintech Group, Inc.) was
used at a 1:400 dilution. For all antibodies, a duration of
incubation of 30-60 min was used at 37˚C. Subsequently,
a secondary detection kit polymer (Bond; Leica Biosystems) was used
for a duration of 10 min with a post-primary (rabbit anti-mouse)
step followed by the polymer anti-rabbit antibody (DS9800, Bond;
Leica Biosystems), HRP-conjugated at room temperature for 8 min for
WT1 antibody and polymer anti-rabbit antibody (DS9800, Bond; Leica
Biosystems), HRP-conjugated at room temperature for 8 min for
inhibin and calretinin. All secondary antibodies were ready-to-use
and required no dilution. The DAB kit (Bond; Leica Biosystems) was
also used for 10 min to facilitate visualization. Hematoxylin was
applied for 5 min as a counterstain at room temperature and the
sections were dehydrated, mounted and cover-slipped. The resulting
slides were examined under a LEICA DM2000 optical microscope (Leica
Microsystems GmbH), at a magnification of x40, x100 and x400.
Immunohistochemical analysis confirmed the diagnosis of ovarian
fibroma (Fig. 5).
The post-operative course of the patient was
uneventful (Table I), and the
patient was discharged on the 4th day post-operatively day. At 1
month following surgery, the tumor marker levels were within normal
limits.
Discussion
The present study describes a case of ovarian
fibroma torsion with manifestations resembling ovarian malignancy.
The clinical diagnosis of twisted ovarian fibromas is challenging,
as they can mimic those of malignant ovarian tumors or degenerating
uterine leiomyomas (8). The sudden
onset of acute abdominal pain, accompanied by discomfort, severe
nausea and multiple episodes of vomiting, constitutes the primary
clinical feature commonly observed in patients with torsion of a
large ovarian fibroma (9). In the
patient described herein, the symptoms were considerably milder,
with low-intensity abdominal pain for 12 days, not associated with
signs of peritoneal irritation. The patient did not report any
vomiting; instead, the main accompanying symptom of the abdominal
pain was low-grade fever. Based on these clinical findings, the
further evaluation of the patient with advanced imaging was
warranted, rather than proceeding directly to emergency surgery,
which is typically indicated in cases of clear indications of
adnexal torsion and necrosis. Torsion, ischemia, and necrosis of
the adnexa represent an emergency condition requiring immediate
intervention due to the high risk of reactive peritonitis and
ischemic gangrene (10). The lack of
acute, worsening symptoms in the patient in the present study,
necessitated the inclusion of a malignant ovarian mass in the
differential diagnosis.
Beyond the unconventional clinical manifestations,
the imaging findings were also far from definitive in the case in
the present study. Ultrasonographic findings of ovarian fibromas
are generally non-specific, as was the case in the patient
described herein. It is estimated that transvaginal ultrasonography
has a sensitivity, specificity and accuracy of 97, 46 and 68%,
respectively, for the detection of solid adnexal masses (11). Doppler ultrasound imaging of the
pelvis is currently considered particularly useful in the
evaluation of adnexal torsion, being able to distinguish areas of
reduced perfusion; however, such findings may be caused by both
ischemia due to torsion and areas of necrosis within the tumor, as
was the case in the patient in the present study (12). A CT scan cannot reliably
differentiate ovarian fibromas from other solid ovarian masses,
given its lacking visualization capabilities as regards soft
tissues (12). The midline location
of the ovarian mass, deviation of the uterus toward the affected
ovary, and the presence of varying degrees of ascitic fluid are
imaging findings that support the diagnosis of adnexal torsion
(12). MRI is considered a
second-line diagnostic tool, with substantial imaging capabilities
for soft tissue lesions. Despite this fact, it is important to note
that the pre-operative differentiation of ovarian fibromas from
subserosal pedunculated uterine leiomyomas or solid malignant
ovarian tumors remains difficult, even if an MRI is used (8). In the patient described herein, neither
ultrasonography, nor CT, nor MRI could pre-operatively establish a
diagnosis of a twisted ovarian fibroma or definitively
differentiate it from solid ovarian cancer.
The differential diagnosis of ovarian fibroma, with
or without torsion, from solid ovarian cancer is challenging, if
based solely on clinical symptoms and conventional imaging, as
established in the present case report. Recent data however,
suggest that convolutional neural networks based on MRI may greatly
aid in the non-invasive preoperative differentiation of these
tumors (13). This advanced
technique is capable of accurately identifying the nature of the
mass (ovarian fibroma vs. solid ovarian carcinoma), thereby guiding
appropriate treatment strategies (13). This utility would be even more
helpful in rare cases of unilateral ovarian fibroma with ascites
and pleural effusion, or in bilateral presentations with ascitic
fluid, where differentiating it from Demons-Meigs syndrome or
metastatic ovarian tumors pre-operatively would be of even greater
clinical significance.
An accurate diagnosis is crucial to avoid
mismanagement, which can result in increased morbidity and
mortality rates (14-16).
In cases such as the one described in the present study, in the
absence of clear pre-operative diagnosis, a histopathological
analysis is the only method that can be used to reach a definitive
conclusion, using intra-operative frozen sections. Frozen sections
can assist in confirming or eliminating the presence of malignancy
and can thus guide intra- and post-operative treatment accordingly,
as was the case in the present study. However, frozen sections
should not constitute the only diagnostic investigation or be
entirely relied upon for surgical decision-making, as they are
associated with certain limitations (17). In particular, sampling errors,
including poor biopsy site selection and poor assessment of cell
infiltration; technical errors, including freezing artifacts and
poor staining; and interpretive errors, due to tumor heterogeneity
and uncertainty, indicate that frozen sections should not be
considered infallible and render proper communication and
coordination between surgeon and pathologist of vital importance
(17). This is even more pronounced
in cases where metastatic ovarian tumors originating from primary
malignancies, typically of the gastrointestinal tract or breast,
coexist with benign ovarian tumors such as fibromas, thecomas and
fibrothecomas, posing severe diagnostic challenges, even with the
utilization of frozen sections (18). Olaofe et al (19) reported a unique case of a Krukenberg
tumor arising within an ovarian fibroma, where diagnosis was
particularly difficult due to histological similarities between
Krukenberg cells and ovarian stromal cells, particularly when
present in limited foci. In the case described herein, although
only a single tumor component was present, the frozen section was
only able to exclude malignancy and could not provide any
information regarding histological type or classification of the
neoplasm, once more confirming the limitations of solely relying on
this technique.
Finally, the utility of tumor markers in the
diagnosis of ovarian fibromas should be discussed. Although rare,
ovarian fibromas associated with elevated serum CA-125 levels
should be included in the differential diagnosis with epithelial
ovarian carcinoma, not only in post-menopausal women, but also in
women of reproductive age (20). In
the patient in the present study, the borderline elevated CA-125
levels led to the suspicion of malignancy; however, combined with
the mild abdominal pain, persistent low-grade fever and elevated
inflammatory markers, they may also be attributed to inflammatory
conditions with ischemia and necrosis. Similarly, the borderline
enlargement of multiple para-aortic and iliac lymph nodes, and the
reported presence of reactive pelvic fluid collections may be
attributed to either an inflammatory or malignant etiology, further
contributing to the diagnostic dilemma between a twisted ovarian
fibroma and solid ovarian carcinoma. Ultimately, definitive
diagnosis was made via a scheduled surgical intervention.
The management of a twisted ovarian fibroma is
surgical, either via laparotomy or laparoscopy. A laparoscopic
approach is reserved for young patients with exophytic ovarian
fibroma and minimal risk of intraperitoneal tumor dissemination
(21). In the event that the damage
to the twisted adnexa is reversible and the patient is of
reproductive age with a desire for future fertility, the excision
of the fibroma or, if necessary, unilateral salpingo-oophorectomy
following intraoperative frozen section analysis is considered the
treatment of choice (20,21). A total hysterectomy with bilateral
salpingo-oophorectomy is indicated in older patients (22). In the patient in the present study, a
total abdominal hysterectomy with bilateral salpingo-oophorectomy
was performed. The patient expressed a lack of desire for future
childbearing; thus, the spread of inflammation from the twisted
adnexa to the uterus, and particularly the inconclusive
intraoperative histological assessment of a presumably benign tumor
requiring multiple permanent sections for definitive diagnosis,
were the reasons for opting for total hysterectomy rather than
adnexectomy.
In conclusion, ovarian fibromas are the most common
solid ovarian tumors. Torsion of a large ovarian fibroma is a rare,
yet severe complication that typically requires prompt surgical
intervention. In the patient in the present study, the mild and
non-alarming progression of the disease deviated from expected
clinical manifestations and necessitated a complete preoperative
work-up and the performance of a scheduled total abdominal
hysterectomy with bilateral salpingectomy and oophorectomy. The
solid nature of ovarian fibromas, their atypical clinical and
imaging features, and their potential association with ascites and
elevated serum CA-125 levels necessitate thorough differential
diagnosis in order to eliminate the possibility of solid ovarian
malignancy. Although the analysis of intraoperative frozen sections
may suggest a likely benign tumor, definitive classification of the
ovarian mass requires multiple permanent histological sections.
Only following the surgical removal of the tumor and performing an
immunohistochemical analysis can a definitive diagnosis of ovarian
fibroma be established.
Acknowledgements
The authors would like to express their appreciation
to Mrs. Mousia Maria and Mrs. Simopoulou Evangelia, physicians of
the Pathology Department of the General Hospital of Trikala
(Trikala, Greece), for providing and interpreting the
histopathological slides.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
All authors (ET, AT, EX, IRA, AZ and IT)
participated in the preparation of the manuscript. ET, AT, EX and
AZ participated in the design of the study, in the literature
search, and in the writing of the manuscript. IRA was involved in
the provision of study materials (such as blood tests, imaging) or
patient data, patient care, data collection and aggregation, data
analysis and interpretation, and in the writing of the manuscript.
IT was involved in the conception and design of the study, in
administrative support, in the provision of study materials (such
as blood tests, imaging) or patient data, in patient care, in data
collection and analysis, and in manuscript writing. ET, AT, EX,
IRA, AZ and IT confirm the authenticity of all the raw data, and
agree to be accountable for all aspects of the work, so that any
questions relating to research integrity or scientific accuracy in
any part of the study are appropriately investigated and resolved.
All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present case report was carried out in
accordance with the Declaration of Helsinki. The patient provided
written informed consent to participate in the present study.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mehra P, Aditi S, Prasad KM and Bariar NK:
Histomorphological analysis of ovarian neoplasms according to the
2020 WHO classification of ovarian tumors: A distribution pattern
in a tertiary care center. Cureus. 15(e38273)2023.PubMed/NCBI View Article : Google Scholar
|
|
2
|
McCluggage WG, Singh N and Gilks CB: Key
changes to the World Health Organization (WHO) classification of
female genital tumours introduced in the 5th edition (2020).
Histopathology. 80:762–778. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hauptmann S, Friedrich K, Redline R and
Avril S: Ovarian borderline tumors in the 2014 WHO classification:
Evolving concepts and diagnostic criteria. Virchows Arch.
470:125–142. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Flissate F, Bensrhir I, Mahfoud H, Lakhdar
A, Baidada A and Sassi S: Fibrothecoma a rare ovarian tumor: A case
report. Int J Surg Case Rep. 120(109771)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Young RH and Scully RE: Ovarian stromal
tumors with minor sex cord elements: A report of seven cases. Int J
Gynecol Pathol. 2:227–234. 1983.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Chechia A, Attia L, Temime RB, Makhlouf T
and Koubaa A: Incidence, clinical analysis, and management of
ovarian fibromas and fibrothecomas. Am J Obstet Gynecol.
199:473.e1–e4. 2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Parrado RH, Batten M, Smith M and McDuffie
LA: Ovarian fibrothecoma in an adolescent: a case report. J Pediatr
Surg Case Rep. 95(102678)2023.
|
|
8
|
Abdelazim IA, Abu-Faza M, Abdelrazek K,
Amer OO, Shikanova S and Zhurabekova G: Ovarian fibroma commonly
misdiagnosed as uterine leiomyoma. Gynecol Minim Invasive Ther.
9:36–38. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Parwate NS, Patel SM, Arora R and Gupta M:
Ovarian fibroma: A clinico-pathological study of 23 cases with
review of literature. J Obstet Gynaecol India. 66:460–465.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Chang-Patel EJ, Palacios-Helgeson LK and
Gould CH: Adnexal torsion: A review of diagnosis and management
strategies. Curr Opin Obstet Gynecol. 34:196–203. 2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Komatsu T, Konishi I, Mandai M, Togashi K,
Kawakami S, Konishi J and Mori T: Adnexal masses: Transvaginal US
and gadolinium-enhanced MR imaging assessment of intratumoral
structure. Radiology. 198:109–115. 1996.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chang HC, Bhatt S and Dogra VS: Pearls and
pitfalls in diagnosis of ovarian torsion. Radiographics.
28:1355–1368. 2008.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Zheng Y, Wang H, Weng T, Li Q and Guo L:
Application of convolutional neural network for differentiating
ovarian thecoma-fibroma and solid ovarian cancer based on MRI. Acta
Radiol. 65:860–868. 2024.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Guelzim Y, Bennasser A, Marrakchi S,
Houssaini AS, Idoubba S, Boujida I, Jahid A, Allali N, Chat L and
Haddad SE: Demons-Meigs syndrome caused by a giant ovarian fibroma:
A case report. Radiol Case Rep. 19:2585–2589. 2024.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Mohamad R, Al Laham O, Albrijawy R, Sallom
M, Merhij A and Almousa M: A case report of bilateral benign
ovarian fibrothecoma coincidental with ascites: An unconventional
co-occurrence. Ann Med Surg (Lond). 85:3739–3743. 2023.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Strobel SL, Jenison EL, Van Kooten JM,
Kitts AN and Britton AJ: Triple negative lobular breast carcinoma
metastatic to an ovarian fibrothecoma. J Histotechnol. 43:200–203.
2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jaafar H: Intra-operative frozen section
consultation: Concepts, applications and limitations. Malays J Med
Sci. 13:4–12. 2006.PubMed/NCBI
|
|
18
|
Wan J, Feng Z, Shi J and Li Q: Metastatic
breast carcinoma and Krukenberg tumor from signet-ring cell gastric
cancer. Asian J Surg. 46:2984–2986. 2023.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Olaofe OO, Betiku OA, Okongwu CC,
Adefidipe AA and Soremekun AI: Krukenberg tumour in a 46-year-old
black African woman with a background of ovarian fibroma-A case
report. BMC Womens Health. 24(566)2024.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Thanasa A, Thanasa E, Kamaretsos E,
Paraoulakis I, Ziogas AC, Kontogeorgis G, Grapsidi V, Gerokostas
EE, Kontochristos V and Thanasas I: Surgical treatment of a rare
case of ovarian fibroma associated with elevated CA125 levels in a
patient of reproductive age: A case report. Cureus.
15(e34097)2023.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Son CE, Choi JS, Lee JH, Jeon SW, Hong JH
and Bae JW: Laparoscopic surgical management and clinical
characteristics of ovarian fibromas. JSLS. 15:16–20.
2011.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Erekson EA, Martin DK and Ratner ES:
Oophorectomy: The debate between ovarian conservation and elective
oophorectomy. Menopause. 20:110–114. 2013.PubMed/NCBI View Article : Google Scholar
|