1. Introduction
Systemic lupus erythematosus (SLE) is a chronic,
autoimmune, connective tissue disease characterized by the loss of
immune tolerance, autoantibody production, immune-complex
deposition and multisystem inflammatory injury. It affects women
disproportionately and is most frequently diagnosed during the
reproductive years, thus necessitating pregnancy counseling and
pregnancy management integral components of longitudinal lupus care
(1-3).
Although pregnancy outcomes in SLE have improved substantially over
the past two decades, affected pregnancies still carry higher rates
of maternal morbidity, placental dysfunction and adverse neonatal
outcomes compared with pregnancies in the general population,
particularly in the presence of active disease, lupus nephritis and
antiphospholipid antibodies (4-6).
Accordingly, the modern approach to SLE in pregnancy extends beyond
flare management alone and requires preconception optimization,
individualized risk assessment, pregnancy-compatible disease
control, and coordinated surveillance by rheumatology,
maternal-fetal medicine, nephrology and neonatology teams when
indicated (7-9).
2. Pathogenesis of SLE
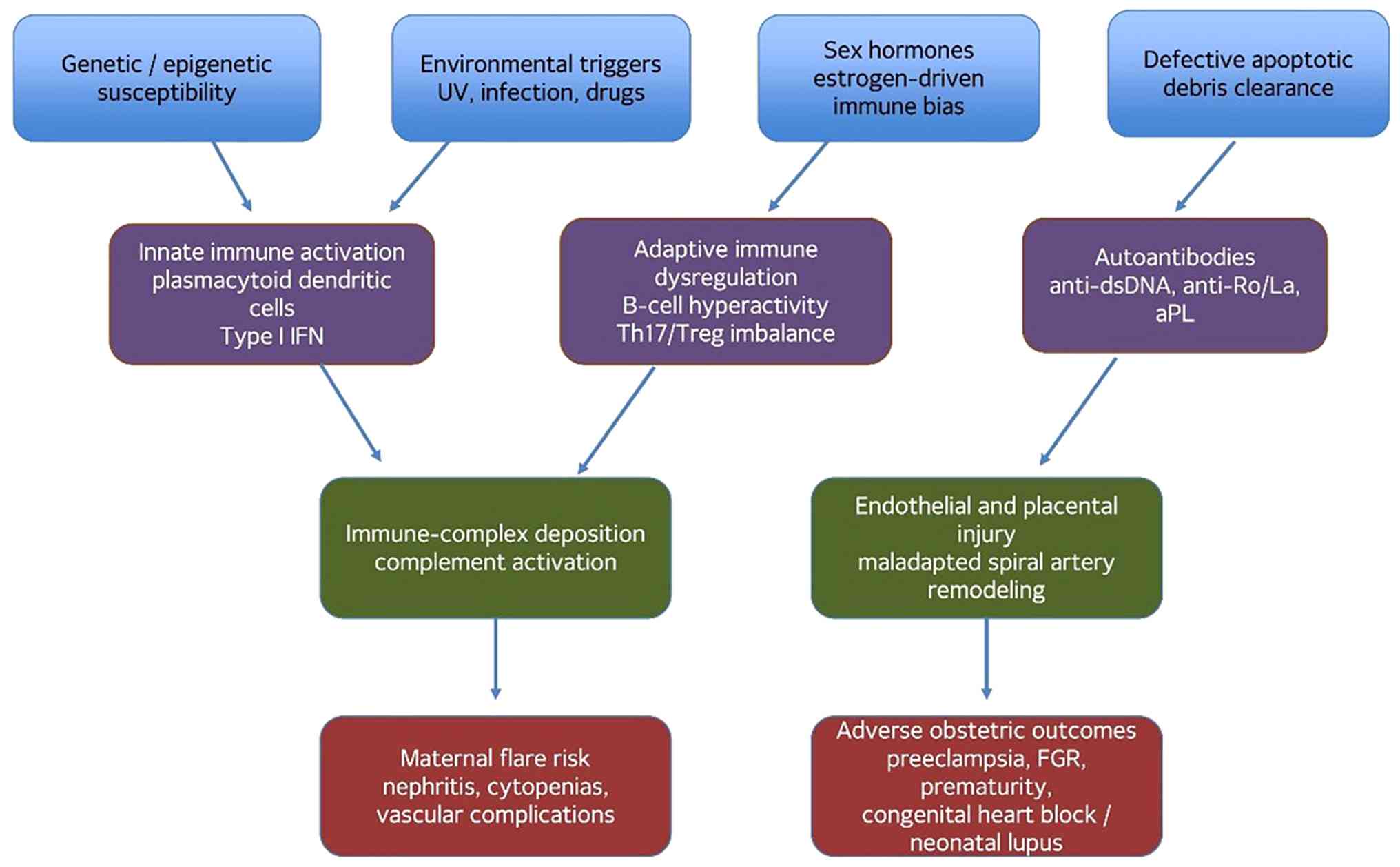
SLE develops through multilevel interactions among
genetic susceptibility, epigenetic dysregulation, sex-hormone
signaling, defective clearance of apoptotic debris, type I
interferon activation, aberrant B-cell and T-cell responses and
complement-mediated tissue injury. In genetically predisposed
individuals, environmental triggers, such as ultraviolet radiation,
viral exposure, cigarette smoke, and selected drugs increase
cellular stress and apoptosis. When apoptotic material is
inadequately cleared, nuclear antigens remain accessible to
antigen-presenting cells and autoreactive lymphocytes, facilitating
the generation of antinuclear, anti-double stranded DNA, anti-Sm
and antiphospholipid antibodies. The resulting immune complexes
activate complement, amplify plasmacytoid dendritic cell interferon
signaling, recruit inflammatory leukocytes, and produce end-organ
injury in the kidneys, skin, joints, hematologic compartment,
vasculature and central nervous system (10-13).
Pregnancy adds a distinct immunologic layer to this
process. Successful gestation requires finely regulated maternal
immune tolerance rather than generalized immunosuppression. Early
implantation and placentation rely on controlled innate immune
activation, decidual natural killer-cell remodeling,
trophoblast-maternal crosstalk and subsequent expansion of
regulatory T-cell pathways. In patients with SLE, these tolerance
mechanisms may be destabilized by pre-existing interferon pathway
activation, complement overactivity, endothelial dysfunction, and
persistent autoantibody production. A relative shift in T-cell
polarization, dysregulated Th17/Treg balance, enhanced B-cell
survival and heightened cytokine signaling may, in combination,
increase flare susceptibility, particularly when pregnancy begins
during a period of serologic or clinical activity (7,13-15).
These mechanisms are also directly relevant to
obstetric diseases. Type I interferon excess, antiphospholipid
antibodies, neutrophil extracellular trap formation, complement
activation, and placental vascular injury can impair spiral artery
remodeling and uteroplacental perfusion, thereby linking maternal
autoimmunity with preeclampsia, fetal growth restriction, preterm
birth and fetal loss. Thus, the pathobiology of SLE in pregnancy
should be understood not merely as baseline lupus occurring
coincidentally during gestation, but as a dynamic interaction
between systemic autoimmunity and the immunologic, vascular and
placental adaptations required for normal pregnancy (4,5,9,13,15,16).
The interaction between immune dysregulation, interferon signaling,
complement activation and placental vascular injury provides a
unifying framework linking systemic lupus erythematosus
pathobiology with adverse obstetric outcomes. The schematic diagram
presented in Fig. 1 highlights how
immune-complex formation and endothelial dysfunction converge on
placental insufficiency, thereby contributing to complications such
as preeclampsia, fetal growth restriction and preterm birth.
3. Effects of pregnancy on SLE
The effects of pregnancy on SLE activity are best
understood through the interplay between pre-pregnancy disease
control, medication continuation, serologic activity and prior
organ involvement rather than pregnancy alone. Contemporary cohorts
suggest that flare rates are substantially lower than historically
reported when conception occurs during remission or low disease
activity and hydroxychloroquine is continued; nevertheless,
pregnancy and the early postpartum period remain clinically
vulnerable windows, particularly for patients with lupus nephritis,
active serology, previous severe flares, or the withdrawal of
pregnancy-compatible therapy (4-6,16-20).
The assessment of activity during pregnancy should
be standardized whenever possible. The SLE Pregnancy Disease
Activity Index (SLEPDAI) was specifically developed to reduce
confounding by physiological gestational changes, and recent
prospective evidence supports the utility of the SLE disease
activity score (SLE-DAS) in early pregnancy as a predictor of
subsequent maternal flares, particularly as demonstrated in
first-trimester cohort analyses (18). In parallel, general disease activity
instruments, such as SLEDAI, BILAG-2004 and Physician Global
Assessment (PGA) remain useful when interpreted by clinicians
experienced in lupus and pregnancy, while the SLICC/ACR Damage
Index is relevant for defining cumulative organ injury and
long-term maternal risk rather than active inflammation per se
(8,18-22).
From a practical standpoint, these instruments should not replace
clinical judgment; however, they improve reproducibility,
longitudinal monitoring and communication across specialties.
A major clinical goal is the achievement of
remission or low disease activity prior to conception. A low lupus
disease activity state (LLDAS) and remission at conception have
been associated with fewer maternal flares and more favorable
obstetric outcomes, while first-trimester disease activity and
hypocomplementemia are associated with preterm birth, preeclampsia
and placental insufficiency (18-20,22).
Distinguishing the physiological changes of pregnancy from flare
remains challenging: Mild anemia, edema, fatigue and isolated
musculoskeletal discomfort may be gestational, whereas a falling
complement level relative to baseline, rising anti-dsDNA titers,
active urinary sediment, progressive proteinuria, thrombocytopenia,
or inflammatory rash/arthritis should prompt concern for active
disease. The postpartum period deserves equal attention as disease
activity often intensifies following delivery, particularly within
the first 6 months (16,19).
4. Pre-pregnancy counseling and
considerations
Pre-pregnancy counseling should be structured,
explicit and individualized as the strongest determinant of
pregnancy outcome in SLE is not the diagnosis alone, but the
disease state and treatment profile at conception. Counseling
should therefore move beyond a general warning that ‘complications
may occur’ and instead classify the patient into an obstetric-risk
framework based on current disease activity, cumulative organ
damage, antibody profile, renal history, cardiovascular status,
prior obstetric history and exposure to potentially teratogenic
agents (4,5,8,16,23).
The ideal candidate for conception is a patient
whose disease has been clinically quiescent or maintained at a low
disease activity for at least 6 months, with stable renal function,
controlled blood pressure, pregnancy-compatible medications and no
major recent flares. By contrast, conception during active
nephritis, uncontrolled hypertension, pulmonary hypertension,
advanced chronic kidney disease, severe heart failure, recent
stroke, or active thrombotic antiphospholipid syndrome (APS) is
associated with a substantially increased maternal and fetal risk,
and may justify the postponement of pregnancy until medical
optimization is achieved (5,7,8,16). Counseling should explicitly
differentiate modifiable risk from non-modifiable risk: Disease
control, medication reconciliation, aspirin/heparin planning and
the timing of conception are modifiable; prior severe nephritis and
chronic organ damage define baseline vulnerability.
Medication optimization is a central component of
pre-pregnancy care. Hydroxychloroquine should generally be
continued; prednisone should be minimized to the lowest effective
dose; azathioprine, tacrolimus and cyclosporine may be considered
when indicated; and known teratogens, such as mycophenolate,
methotrexate, cyclophosphamide and leflunomide require
discontinuation with appropriate washout and transition planning
prior to conception (8,9,15,24). In
addition, counseling should address aspirin prophylaxis,
anticoagulation when APS is present, anti-Ro/SSA and
anti-La/SSB-related fetal surveillance, and the need for
multidisciplinary care. Notably, modern data underscore that
pregnancy planning and medical readiness are associated with
improved reproductive outcomes than ill-timed conception during
active disease or teratogenic exposure (23). A structured preconception assessment
framework integrating disease activity, organ involvement, antibody
profile and medication status supports individualized risk
stratification and informed decision-making regarding pregnancy
timing (Table I).
 | Table IPreconception assessment framework
for pregnancy planning in women with systemic lupus
erythematosus. |
Table I
Preconception assessment framework
for pregnancy planning in women with systemic lupus
erythematosus.
| Domain | Preconception
assessment | Clinical
rationale |
|---|
| Disease
activity | Confirm remission
or low disease activity for at least 6 months; document recent
flare history and current symptom burden. | Active disease at
conception is strongly associated with maternal flare,
preeclampsia, prematurity and fetal loss. |
| Renal status | Serum creatinine,
urine protein quantification, urinary sediment, blood pressure, and
prior lupus nephritis phenotype. | Defines baseline
maternal risk and improves later differentiation between nephritis
flare and preeclampsia. |
| Antibody
profile | aPL profile,
anti-Ro/SSA, anti-La/SSB, anti-dsDNA, complement baseline. | Guides
anticoagulation strategy, fetal echocardiographic surveillance, and
inter-pretation of serologic change during pregnancy. |
| Medication
plan | Continue
pregnancy-compatible therapy; discontinue or switch teratogens with
documented washout and replacement plan. | Prevents avoidable
flare while minimizing embryotoxic or fetotoxic exposure. |
| Organ
damage/comorbidity | Pulmonary
hypertension, chronic kidney disease, heart failure, chronic
hypertension, prior thrombosis or stroke. | Identifies
pregnancies that should be delayed, co-managed intensively, or
occasionally discouraged. |
| Obstetric
history | Previous
miscarriage, fetal growth restriction, preeclampsia, preterm birth,
congenital heart block. | Determines
recurrence risk and the intensity of maternal-fetal
surveillance. |
5. Pre-pregnancy analyses in patients with
SLE
The pre-pregnancy evaluation in SLE should
distinguish between routine background lupus surveillance and
pregnancy-specific risk stratification. General SLE monitoring
includes complete blood count, renal profile, liver profile,
urinalysis, protein quantification, complement levels and
anti-dsDNA assessment; however, in the context of pregnancy
planning, these tests have a different purpose: They establish a
maternal baseline against which later gestational changes can be
interpreted and identify women at increased risk for flare,
nephritis recurrence, preeclampsia, placental dysfunction and fetal
compromise (8,16,21).
Pregnancy-specific evaluations should include, at
minimum, the confirmation of disease activity status; the
quantification of proteinuria and renal function; blood pressure
assessment; antiphospholipid antibody profiling; anti-Ro/SSA and
anti-La/SSB testing; medication review; and the targeted evaluation
of organ systems that materially alter pregnancy risk, particularly
the kidneys, cardiovascular system and lungs. Echocardiography is
appropriate when pulmonary hypertension, cardiomyopathy,
significant valvular disease, or prior cardiopulmonary symptoms are
suspected. Pulmonary function testing or thoracic imaging should be
reserved for women with respiratory symptoms or known parenchymal
disease rather than performed indiscriminately in all patients.
Likewise, thrombophilia-oriented planning should focus primarily on
APS rather than broad nonselective testing (5,7,8,16).
Baseline complement levels and anti-dsDNA titers are
particularly valuable as serial interpretation during pregnancy is
more informative than isolated absolute values. Similarly,
documenting preconception serum creatinine, urine protein excretion
and urinary sediment markedly improves later differentiation
between quiescent renal disease, lupus nephritis flare and
superimposed preeclampsia. For women with thyroid symptoms, prior
thyroid disease, or autoimmune clustering, thyroid function testing
is reasonable; however, thyroid studies should be presented as
selective adjuncts rather than mandatory lupus-specific pregnancy
biomarkers in all patients. This distinction improves conceptual
clarity and aligns the evaluation with practical clinical
decision-making (8,16,21).
Establishing a comprehensive maternal baseline through targeted
laboratory and clinical evaluation is essential for distinguishing
physiological gestational changes from pathological processes such
as lupus flare, nephritis, or preeclampsia (Table II).
| Table IIRecommended pre-pregnancy analyses
and their pregnancy-specific clinical utility in women with
systemic lupus erythematosus. |
Table II
Recommended pre-pregnancy analyses
and their pregnancy-specific clinical utility in women with
systemic lupus erythematosus.
| Analysis | Pregnancy-specific
use |
|---|
| Complete blood
count, creatinine, liver profile | Establishes
maternal baseline and identifies cytopenia, renal impairment, or
comorbidity relevant to pregnancy risk. |
| Urinalysis +
protein quantification | Essential for
documenting baseline renal involvement and later interpreting new
proteinuria. |
| Anti-dsDNA, C3,
C4 | Best interpreted
longitudinally; falling complement relative to baseline and rising
anti-dsDNA may support flare. |
| Antiphospholipid
antibody panel | Determines
antiphospholipid syndrome risk stratification and aspirin/heparin
planning. |
| Anti-Ro/SSA and
anti-La/SSB | Identifies
pregnancies requiring counseling about neonatal lupus and serial
fetal rhythm surveillance. |
| Targeted
echocardiography/pulmonary evaluation | Reserved for
suspected cardiopulmonary disease, pulmonary hypertension, or prior
organ involvement. |
| Medication
reconciliation | Ensures compatible
treatment, washout of teratogens, and clear pregnancy/lactation
planning. |
6. Contraceptives in patients with SLE
Contraception is relevant in patients with SLE as it
underpins safe pregnancy planning. Women with active disease,
recent flares, severe organ involvement, or current exposure to
teratogenic medications should be protected from unplanned
conception until disease control and medication transition have
been achieved. Accordingly, contraceptive counseling should be
framed as a component of reproductive safety and timing rather than
as a disconnected gynecologic topic (8,23).
Highly effective contraception is particularly
important for women taking mycophenolate, methotrexate,
cyclophosphamide, or other agents that may cause embryotoxicity or
fetotoxicity. Intrauterine devices, including copper and
levonorgestrel systems, are generally preferred due to their high
efficacy and minimal dependence on adherence, although the
thrombotic profile and antiphospholipid antibody status should be
considered when estrogen-containing methods are discussed. Combined
oral contraceptives may be acceptable in selected women with
stable, low-activity disease and without antiphospholipid
antibodies or a major risk of thrombosis, whereas progestin-only
options are often preferred when thrombosis risk is a concern
(8,16,25).
The essential clinical principle is that every woman
of reproductive age with SLE should have a documented reproductive
plan: Whether she desires pregnancy now, later, or not at all;
whether conception is medically advisable at the present time; and
which contraceptive strategy best aligns with her disease activity
and medications. This approach prevents high-risk pregnancies
during periods of medical instability and directly supports the
goal of well-timed conception (23).
7. Infertility in patients with SLE
Fertility in women with SLE is often described as
broadly preserved; yet, this statement may be misleading in
clinical practice. Subfertility in SLE may arise from
disease-related inflammation, chronic organ dysfunction, reduced
ovarian reserve, associated autoimmune endocrinopathies, sexual
dysfunction, psychosocial burden, delayed childbearing and
treatment-related gonadotoxicity. Therefore, the infertility
discussion should extend beyond the mere observation that
infertility ‘is not uncommon’ and instead outline a diagnostic and
management framework tailored to lupus (15,26-28).
The initial evaluation should mirror standard
infertility work-up, but with SLE-specific expansion. Core
assessment includes ovulatory history, ovarian reserve testing with
anti-Mullerian hormone and/or antral follicle count, thyroid
assessment when indicated, a review of menstrual function,
age-related fertility risk, partner-related factors and medication
exposure. Particular attention should be paid to cumulative
cyclophosphamide exposure, as gonadal toxicity is dose- and
age-dependent and remains one of the most critical iatrogenic
threats to fertility in SLE. Recent data support the use of
anti-Mullerian hormone and antral follicle count as clinically
useful markers of diminished ovarian reserve in this population,
even when menstrual cycles appear preserved (27). These markers are particularly useful
because cyclophosphamide-related ovarian injury may precede overt
menstrual disturbance, and contemporary reviews of fertility in SLE
recommend incorporating ovarian reserve testing into individualized
reproductive counseling (26,27).
Fertility preservation should be discussed prior to
the e of cyclophosphamide whenever feasible. Concurrent
gonadotropin-releasing hormone agonists may reduce the risk of
ovarian insufficiency and improve the odds of later pregnancy,
although they should be viewed as protective rather than fully
restorative. When disease severity permits, mycophenolate-based
nephritis regimens may reduce gonadotoxic exposure compared with
cyclophosphamide; however, this advantage is relevant to long-term
reproductive planning and not to pregnancy itself, as mycophenolate
is contraindicated during gestation (28). Assisted reproductive technologies may
be considered in carefully selected patients with quiescent
disease; however, stimulation protocols should be coordinated with
rheumatology and maternal-fetal medicine teams because estrogen
exposure, thrombosis risk, and antiphospholipid antibodies may
alter the safety profile. Anticoagulation and hydroxychloroquine
continuation may be necessary in selected patients undergoing
assisted reproduction (8,26,29).
8. Effects of SLE on pregnancy
The effects of SLE on pregnancy should be discussed
in pregnancy-specific terms rather than extrapolated from disease
behavior outside gestation. The principal determinants of adverse
outcomes are active disease at conception, lupus nephritis (current
or previous), antiphospholipid antibodies or antiphospholipid
syndrome, chronic hypertension, accumulated organ damage, and
anti-Ro/SSA or anti-La/SSB seropositivity. These factors do not
confer identical risk throughout gestation; rather, they influence
different maternal and placental pathways at different times in
pregnancy (4,5,8,16,30).
During the first trimester, active systemic
inflammation and antiphospholipid-mediated placental injury
increase the risks of implantation failure, miscarriage and early
pregnancy loss. In the second and third trimesters, placental
malperfusion, endothelial dysfunction, nephritis and maternal
vascular disease become increasingly relevant, translating into
preeclampsia, fetal growth restriction, medically indicated
prematurity, and stillbirth. Anti-Ro/SSA and anti-La/SSB antibodies
introduce a distinct fetal risk profile, especially congenital
heart block and neonatal lupus, which emerges during the
mid-trimester period of greatest transplacental antibody effect
(5,8,31-33).
Evidence-based counseling should therefore emphasize
timing and stratification. Women who conceive in remission or low
disease activity on pregnancy-compatible therapy usually have
substantially improved outcomes than those who conceive during
active disease or while receiving teratogens. Recent data confirm
that active disease, nephritis, and antiphospholipid antibodies are
among the most consistent predictors of adverse pregnancy outcomes,
while pregnancy planning and medical readiness remain modifiable
levers that clinicians can intervene upon before conception
(4,17,23,30).
This risk pattern is supported by systematic evidence identifying
lupus nephritis, antiphospholipid antibody positivity, and active
disease as recurrent predictors of fetal loss, preterm birth,
hypertensive disease, and fetal growth restriction (4,30).
9. Maternal complications associated with
SLE
Preeclampsia
Preeclampsia is one of the most critical maternal
complications associated with pregnancy in patients with SLE as it
is both more common and more difficult to diagnose than in the
general obstetric population. The risk further increases in the
presence of lupus nephritis, chronic hypertension, antiphospholipid
antibodies and active systemic inflammation. Previous research has
consistently identified nephritis and antiphospholipid positivity
as major risk amplifiers, supporting the concept that preeclampsia
in SLE often reflects overlapping endothelial, placental,
inflammatory, and renal pathology rather than an isolated obstetric
event (4,5,17,30,34,35).
Systematic reviews and meta-analyses specifically support lupus
nephritis and antiphospholipid antibody positivity as major
predictors of hypertensive disease and other adverse pregnancy
outcomes (4,36). Primary cohort and guideline-based
evidence further supports the contribution of chronic hypertension,
active inflammation and renal impairment to preeclampsia risk in
SLE (5,17,30,34,35).
Diagnostic differentiation from lupus nephritis
flare is a major clinical challenge as both conditions may present
with hypertension, proteinuria, thrombocytopenia and renal
dysfunction. Features favoring nephritis include active urinary
sediment, rising anti-dsDNA titers, hypocomplementemia relative to
baseline, and concomitant extra-renal lupus manifestations.
Features favoring preeclampsia include abrupt-onset hypertension
following mid-gestation, placental insufficiency and angiogenic
imbalance. Emerging evidence suggests that angiogenic biomarkers,
particularly soluble fms-like tyrosine kinase-1 (sFlt-1), placental
growth factor (PlGF) and the sFlt-1/PlGF ratio may serve as useful
adjuncts in distinguishing preeclampsia from active lupus
nephritis, although they should be interpreted within the broader
clinical context rather than used in isolation (29,36).
From a preventive standpoint, low-dose aspirin
should be initiated in women with SLE unless contraindicated,
ideally commencing by 12-16 weeks of gestation, and anticoagulation
should be added when obstetric or thrombotic APS is present
(8,16,37).
Hemolysis with elevated liver tests
and thrombocytopenia (HELLP)
HELLP syndrome represents a severe microangiopathic
and endothelial variant within the hypertensive disease spectrum of
pregnancy and may be particularly complex in women with SLE as
thrombocytopenia, hemolysis, transaminitis and renal impairment can
overlap with lupus flare, thrombotic microangiopathy, catastrophic
APS and active nephritis. In women with lupus who are pregnant,
HELLP should therefore trigger a structured differential diagnosis
rather than reflex attribution to preeclampsia alone (8,16,38).
Current evidence supports prompt multidisciplinary
assessment, serial maternal laboratory monitoring and fetal
evaluation, with delivery remaining the definitive management once
maternal or fetal instability is established. Complement
dysregulation has been implicated in severe disease phenotypes,
which is mechanistically relevant in SLE and antiphospholipid
syndrome, although complement-targeted therapy remains
investigational rather than standard care in this setting (38).
Lupus nephritis
Lupus nephritis is among the strongest predictors of
adverse maternal and fetal outcomes in pregnancy in patients with
SLE. Its importance lies not only in the presence of renal disease
itself, but also in the timing of activity, the degree of baseline
chronic damage, the burden of proteinuria, the coexistence of
hypertension and difficulty distinguishing renal flare from
superimposed preeclampsia. Women with active or recent nephritis
have higher rates of preeclampsia, preterm delivery, fetal growth
restriction and pregnancy loss than women with quiescent non-renal
disease (4,5,17,34,35,39).
The most favorable outcomes are observed when
pregnancy occurs after at least 6 months of renal quiescence, with
stable serum creatinine, controlled blood pressure and low
proteinuria. During pregnancy, worsening proteinuria alone is
insufficient to diagnose nephritis flare as gestational physiology
and preeclampsia can both alter urinary findings. Interpretation
should instead integrate urinary sediment, complement trends,
anti-dsDNA activity, blood pressure trajectory, extrarenal
manifestations and fetal/placental assessment. Angiogenic
biomarkers, particularly the sFlt-1/PlGF ratio, may add
discriminatory value when clinical uncertainty persists (29,36).
Management depends on severity and timing.
Hydroxychloroquine should be maintained; glucocorticoids are used
for flares; and pregnancy-compatible steroid-sparing agents, such
as azathioprine or calcineurin inhibitors may be required. Renal
biopsy during pregnancy is reserved for selected situations in
which the result would meaningfully alter management and procedural
risk is acceptable. More commonly, clinicians rely on integrated
clinical judgment and empiric treatment when the pretest
probability of active nephritis is high (8,16,24).
Obstetric APS and antiphospholipid
antibodies
Obstetric APS is a major modifier of pregnancy risk
in SLE and should be discussed not as an ancillary antibody
finding, but as a distinct placental-thrombotic phenotype.
Persistent lupus anticoagulant, anticardiolipin and anti-beta2
glycoprotein I antibodies are associated with recurrent early loss,
fetal death, placental insufficiency, severe preeclampsia and
prematurity. Among these markers, lupus anticoagulant remains the
strongest single laboratory predictor of poor pregnancy outcomes
(30,37,40).
Risk stratification should distinguish asymptomatic
antibody positivity from definite obstetric APS and thrombotic APS,
as management differs substantially across these categories. Women
with prior obstetric APS generally require low-dose aspirin plus
prophylactic heparin, whereas women with thrombotic APS usually
require therapeutic anticoagulation throughout pregnancy and the
postpartum period. Persistently positive antibodies without prior
events warrant individualized counseling and, in numerous centers,
low-dose aspirin-based prevention depending on the antibody profile
and overall risk context (8,16,30,37).
Sepsis
Infection deserves greater emphasis in pregnancy in
patients with SLE as it contributes materially to maternal
morbidity and may mimic flare, particularly when fever, cytopenia,
elevated inflammatory markers, or multiorgan dysfunction are
present. Pregnancy-related immune modulation, chronic
corticosteroid exposure, baseline immune dysregulation, nephritis
and the use of immunosuppressive therapy collectively increase
susceptibility to severe infection. Clinically, the challenge lies
in discriminating infection from active SLE, while avoiding delayed
antimicrobial therapy in unstable patients (5,7,16).
Hematological complications
Hematological complications in pregnancy in patients
with SLE extend beyond descriptive anemia and thrombocytopenia.
These abnormalities may reflect disease activity, medication
toxicity, iron deficiency, microangiopathy, hemolysis, APS, or
gestational physiology, and their prognostic significance depends
on context. Persistent thrombocytopenia, hemolysis, or pancytopenia
should prompt evaluation for flare, HELLP syndrome, thrombotic
microangiopathy, or infection rather than being attributed
automatically to uncomplicated gestation (5,8,16).
10. Placental disease in pregnancy in women
with SLE and fetal complications of SLE
Placental disease
Placental disease is central to the pathophysiology
of adverse obstetric outcomes in SLE. Rather than being viewed as a
passive end-organ victim, the placenta functions as a biologically
active interface where interferon signaling, complement activation,
antiphospholipid-mediated thrombosis, endothelial injury and
maladaptive spiral artery remodeling converge. Histopathological
analyses describe infarction, decidual vasculopathy, fibrin
deposition and impaired villous development, all of which are
compatible with chronic uteroplacental malperfusion (8,14,29,41).
This placental perspective helps explain why women
with even mildly active systemic disease may still experience fetal
growth restriction, preeclampsia and prematurity, particularly when
serologic activity or antiphospholipid antibodies are present. It
also underscores why fetal surveillance should be interpreted in
parallel with maternal biomarkers and blood pressure rather than as
a purely fetal issue.
Fetal complications of SLE
Fetal complications of SLE should be framed
according to the mechanism and timing. Early losses are more
closely linked to antiphospholipid-mediated implantation and
placental failure, whereas later complications are more often
driven by placental insufficiency, maternal vascular disease,
nephritis, hypertension and medically indicated preterm delivery.
Across recent syntheses, the most reproducible predictors of poor
fetal outcomes are active maternal disease, lupus nephritis,
antiphospholipid antibodies, chronic hypertension and prior adverse
pregnancy history (4,5,8,17,30).
Clinically, surveillance should be risk-adapted.
Serial fetal growth assessment, umbilical artery Doppler when
placental insufficiency is suspected, maternal blood pressure
monitoring, and targeted fetal echocardiography in anti-Ro/SSA- or
anti-La/SSB-positive pregnancies improve practical utility more
than broad descriptive statements about risk alone (8,16,21).
Neonatal lupus. Neonatal lupus is a passively
acquired autoimmune syndrome caused primarily by transplacental
transfer of maternal anti-Ro/SSA and anti-La/SSB antibodies, with
cardiac disease representing its most severe manifestation.
Cutaneous lesions, cytopenia, hepatobiliary abnormalities and
transient laboratory disturbances are often self-limited as
maternal antibodies clear. By contrast, congenital heart block is
usually irreversible and is associated with substantial morbidity,
frequently requiring pacemaker placement (31-33,42,43).
As risk is antibody-mediated rather than
disease-activity-mediated, even asymptomatic mothers with
anti-Ro/SSA or anti-La/SSB positivity require structured
surveillance. Current practice generally includes serial fetal
echocardiographic assessment during the period of highest risk for
conduction abnormalities, typically from ~16 to 26 weeks of
gestation, with some centers extending surveillance thereafter in
selected high-risk pregnancies. Hydroxychloroquine continuation is
particularly critical, as prospective data support a reduction in
recurrent congenital heart block among anti-SSA/Ro-positive
pregnancies exposed to hydroxychloroquine (33). Thus, neonatal lupus is not merely
defined entity, but as a condition requiring anticipatory
screening, counseling regarding recurrence risk and coordinated
fetal-cardiology follow-up. This recommendation is supported by
reviews of neonatal lupus pathogenesis and clinical cohorts
demonstrating the association between maternal anti-Ro/SSA or
anti-La/SSB antibodies and fetal conduction disease (31-33,42,43).
11. Puerperium
The puerperium is a high-risk transition period in
SLE. Hemodynamic shifts, postpartum inflammatory rebound,
medication changes, interrupted follow-up and the risk of
thrombosis, particularly in women with antiphospholipid antibodies
all contribute to maternal vulnerability. Postpartum care should
therefore be prespecified prior to delivery and include
thromboprophylaxis duration when indicated, blood pressure
follow-up, renal reassessment in women with nephritis or
preeclampsia, medication reconciliation for lactation, and early
rheumatology review as flares may emerge in the weeks to months
following delivery (8,16,44,45).
12. Medications for SLE during
pregnancy
Pharmacological management for SLE during pregnancy
should be presented according to therapeutic intent and
reproductive safety rather than as a list of isolated agents. The
central objective is to maintain maternal disease quiescence using
pregnancy-compatible therapy as uncontrolled lupus is consistently
more dangerous to both the mother and fetus than the majority of
approved medications used judiciously during gestation.
Accordingly, therapy should be stratified into: i) Medications
recommended to be continued; ii) medications that can be used when
clinically indicated; iii) medications that require discontinuation
prior to conception due to known teratogenicity or insufficient
safety data (8,9,15).
Corticosteroids
Glucocorticoids remain essential for the treatment
of lupus flares in pregnancy, and their role should be described
with greater therapeutic nuance. Non-fluorinated glucocorticoids
such as prednisone and prednisolone are preferred for maternal
disease as placental metabolism limits fetal exposure. They are
effective for arthritis, serositis, cutaneous disease and a number
of moderate flares; however, their prolonged or high-dose use
increases the risks of gestational diabetes, hypertension,
infection, preterm birth, osteoporosis, and possibly, growth
restriction; thus, the lowest effective dose should be used and
steroid-sparing therapy should be introduced when repeated
escalation is anticipated (8,16,46,47).
Fluorinated corticosteroids, such as dexamethasone
and betamethasone, cross the placenta more readily and are
therefore reserved for specific fetal indications rather than
routine maternal control. This distinction is particularly relevant
in the context of suspected fetal conduction disease, where
fluorinated steroids may be considered in selected early or
incomplete block scenarios after multidisciplinary discussion,
despite ongoing uncertainty in the evidence base (15,33,48).
Non-steroidal anti-inflammatory drugs
(NSAIDs)
NSAIDs may still play a role in the short-term
control of pain and serositis in selected patients, although their
use during pregnancy needs to be restricted by gestational age and
maternal-fetal context. They are generally avoided in the third
trimester due to the risk of ductus arteriosus constriction and
oligohydramnios, and caution is also warranted from 20 weeks onward
in light of fetal renal concerns highlighted by regulatory
agencies. Consequently, NSAIDs should not be portrayed as routine
background therapy in lupus pregnancy; instead, they are limited
adjuncts, while acetaminophen and disease-directed
anti-inflammatory control are often safer long-term strategies
(6,16,49).
Antithrombotic therapy
Antithrombotic therapy in pregnancy in patients with
SLE is primarily determined by antiphospholipid antibody status,
prior thrombosis and obstetric history. Low-dose aspirin is
recommended for the majority of pregnant women with SLE to reduce
the risk of preeclampsia, while heparin-based regimens are added
according to the APS phenotype. Warfarin is generally avoided
during organogenesis due to teratogenicity, although individualized
exceptions in highly selected mechanical-valve or
extreme-thrombotic-risk scenarios belong to specialist management
rather than routine lupus pregnancy care (8,16,37,50,51).
Immunomodulators
Hydroxychloroquine is the cornerstone maintenance
therapy used in pregnant patients with SLE and should, in the
majority of cases, be continued prior to conception, throughout
gestation and during lactation. It is associated with lower disease
activity and may reduce selected obstetric and neonatal
complications, including the recurrence of congenital heart block
in anti-SSA/Ro-positive pregnancies (6,6,33,52-54).
For this reason, drug discontinuation out of unfounded teratogenic
concern should be actively discouraged.
Azathioprine is among the preferred steroid-sparing
immunosuppressants in pregnancy when additional disease control is
needed, particularly for nephritis maintenance or persistent
systemic activity. Its use should be limited to accepted dosing
thresholds, although it is far better supported in pregnancy than
several alternative immunosuppressants (8,16,55,56).
Immunosuppressants
Mycophenolate mofetil, mycophenolic acid,
methotrexate and cyclophosphamide are contraindicated or strongly
avoided in pregnancy due to established embryotoxicity,
fetotoxicity, or gonadotoxicity. Their importance lies not only in
identifying them as unsafe agents, but also in emphasizing
preconception transition planning. Women receiving these therapies
require early counseling, reliable contraception and deliberate
conversion to pregnancy-compatible alternatives before conception
is attempted (8,16,57-59).
Calcineurin inhibitors on the other hand, such as
tacrolimus and cyclosporine, are increasingly recognized as useful
pregnancy-compatible options for selected patients with lupus
nephritis or steroid-dependent disease, whereas voclosporin,
despite efficacy in active lupus nephritis outside pregnancy, lacks
sufficient pregnancy safety data to recommend its use during
gestation. The appropriate framework is therefore: Established
calcineurin inhibitors may be considered in pregnancy when
indicated, and voclosporin is relevant primarily to pre-pregnancy
risk assessment and drug transition planning (24,60).
13. Biologics and emerging therapies
This section briefly discusses biologics and
emerging therapies to reflect current SLE therapeutics. Anifrolumab
is currently an approved treatment for moderate-to-severe SLE; some
women of reproductive age may present for preconception counseling
while receiving it. However, human pregnancy data remain
insufficient to recommend routine continuation during gestation;
thus, current practice generally favors transition to
better-characterized pregnancy-compatible regimens prior to
conception whenever disease control allows (61). Belimumab has a growing, yet still
incomplete pregnancy safety dataset and may be considered case by
case in refractory disease, whereas rituximab is usually reserved
for severe maternal indications in exceptional circumstances
(9,16). Optimizing pharmacological management
in SLE during pregnancy requires balancing maternal disease control
with fetal safety through the use of pregnancy-compatible therapies
and the avoidance of teratogenic agents (Table III).
| Table IIIMedication use in pregnancy for women
with systemic lupus erythematosus: Compatibility, restrictions and
clinical considerations. |
Table III
Medication use in pregnancy for women
with systemic lupus erythematosus: Compatibility, restrictions and
clinical considerations.
|
Medication/class | Pregnancy | Comment |
|---|
|
Hydroxychloroquine | Continue | Cornerstone
background therapy; associated with lower lupus activity and no
established teratogenic signal. |
|
Prednisone/prednisolone | Use if needed | Prefer lowest
effective dose; useful for flare control, but prolonged high-dose
use increases maternal complications. |
| Azathioprine | Compatible | Preferred
steroid-sparing option when additional control is required. |
|
Tacrolimus/cyclosporine | Compatible in
selected cases | Useful particularly
in nephritis or steroid-dependent disease; requires blood pressure
and renal monitoring. |
| Low-dose
aspirin | Recommended in most
pregnancies | Used to reduce
preeclampsia risk unless contraindicated. |
| Heparin | Use according to
antiphospholipid syndrome phenotype | Preferred
anticoagulant in pregnancy. |
| Non-steroidal
anti-inflammatory drugs | Limited/avoid in
late pregnancy | Short-term only in
selected situations; avoid in the third trimester and use caution
from 20 weeks onward. |
| Mycophenolate,
methotrexate, leflunomide |
Contraindicated | Require
discontinuation before conception. |
|
Cyclophosphamide |
Avoid/contraindicated except in
exceptional circumstances | Embryotoxic and
gonadotoxic; relevant mainly to preconception planning. |
| Voclosporin | Insufficient
pregnancy data | Important for
preconception medication review; not recommended routinely in
pregnancy. |
| Anifrolumab/JAK
inhibitors | Insufficient
pregnancy data | Should generally be
discontinued or switched before conception whenever feasible. |
Emerging classes such as Janus kinase inhibitors
should also be mentioned in the context of reproductive counseling.
Although these agents are not standard pregnancy therapies in SLE,
they are increasingly encountered in immune-mediated disease
management and are generally avoided in pregnancy due to limited
human safety evidence. Their relevance to the present review lies
in pre-pregnancy medication reconciliation, washout planning, and
risk communication rather than use during gestation itself. This
distinction improves the completeness and contemporary relevance of
the pharmacologic discussion without overstating pregnancy safety
data.
14. Conclusion
Pregnancy in women with SLE currently has a
substantially improved prognosis than in earlier decades; however,
favorable outcomes depend on one principle above all others:
Conception should occur during sustained remission or low disease
activity on pregnancy-compatible therapy. Across the current
evidence base, the most consistent drivers of adverse outcome are
active disease at conception, lupus nephritis, antiphospholipid
antibodies/APS, chronic organ damage and inadequate pre-pregnancy
optimization. Conversely, hydroxychloroquine continuation, aspirin
prophylaxis when appropriate, anticoagulation for APS, and
structured multidisciplinary surveillance meaningfully improve care
(4-6,8,16,17).
Clinically, pregnancy in patients with SLE should be
managed as a longitudinal pathway rather than an isolated
gestational episode. This pathway includes reproductive planning
and contraception during unsafe periods, rigorous pre-pregnancy
assessment, trimester-specific maternal-fetal monitoring, prompt
differentiation of flare from obstetric mimics such as
preeclampsia, and postpartum follow-up for thrombosis, renal
deterioration, hypertension, flares and medication-lactation
reconciliation. Remaining knowledge gaps include the optimal role
of biomarkers for nephritis vs. preeclampsia discrimination,
long-term outcomes following in utero exposure to novel
biologics and targeted therapies, and the refinement of
individualized fetal surveillance strategies in antibody-positive
pregnancies. Future research is warranted to focus on these
clinically unresolved areas to support more precise and safer
reproductive care for women with SLE.
Acknowledgements
The authors acknowledge the support of the
University of Medical Sciences and Technology and Almaarefa
University (Riyadh, Saudi Arabia) in facilitating this work. The
authors are grateful for their academic and institutional guidance.
This support consisted of academic mentorship, institutional
affiliation support, and administrative facilitation during
manuscript preparation; no financial support, materials, or
study-specific funding were provided.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
All authors (IO, AA, MA and SM) significantly
contributed to the development of the review article. IO was
involved in the study supervision and conceptualization, as well as
in the writing of the original draft of the manuscript and provided
critical revisions. AA was involved in the literature review, data
collection and initial manuscript drafting. SM was involved in
manuscript editing and quality assurance. MA was involved in the
review of the manuscript. All authors have read and approved of the
final manuscript. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, AI tools were
used to improve the readability and language of the manuscript or
to generate images, and subsequently, the authors revised and
edited the content produced by the AI tools as necessary, taking
full responsibility for the ultimate content of the present
manuscript.
References
|
1
|
Knight CL and Nelson-Piercy C: Management
of systemic lupus erythematosus during pregnancy: Challenges and
solutions. Open Access Rheumatol. 8:23–36. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ngo ST, Steyn FJ and McCombe PA: Gender
differences in autoimmune disease. Front Neuroendocr. 35:347–369.
2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Petri M: Pregnancy and systemic lupus
erythematosus. Best Pract Res Clin Obstet Gynaecol. 64:24–30.
2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Wind M, Fierro JJ, Bloemenkamp KWM, de
Leeuw K, Lely AT, Limper M, Sueters M, Teng YKO, Walter IJ and
Kooiman J: Pregnancy outcome predictors in systemic lupus
erythematosus: A systematic review and meta-analysis. Lancet
Rheumatol. 6:e667–e683. 2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Society for Maternal-Fetal Medicine
(SMFM). Electronic address: pubs@smfm.org. Silver R, Craigo S,
Porter F, Osmundson SS, Kuller JA and Norton ME: Society for
maternal-fetal medicine consult series #64: Systemic lupus
erythematosus in pregnancy. Am J Obstet Gynecol. 228:B41–B60.
2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Clowse MEB, Eudy AM, Balevic S,
Sanders-Schmidler G, Kosinski A, Fischer-Betz R, Gladman DD, Molad
Y, Nalli C, Mokbel A, et al: Hydroxychloroquine in the pregnancies
of women with lupus: A meta-analysis of individual participant
data. Lupus Sci Med. 9(e000651)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Gamba A, Zen M, Depascale R, Calligaro A,
Gatto M, Iaccarino L and Doria A: Modern management of pregnancy in
systemic lupus erythematosus: From prenatal counseling to
postpartum support. J Clin Med. 13(3454)2024.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sammaritano LR, Bermas BL, Chakravarty EE,
Chambers C, Clowse MEB, Lockshin MD, Marder W, Guyatt G, Branch DW,
Buyon J, et al: 2020 American College of Rheumatology guideline for
reproductive health in rheumatic diseases. Arthritis Rheumatol.
72:529–556. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dao KH and Bermas BL: Systemic lupus
erythematosus management in pregnancy. Int J Womens Health.
14:199–211. 2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fanouriakis A, Kostopoulou M, Andersen J,
Aringer M, Arnaud L, Bae SC, Boletis J, Bruce IN, Cervera R, Doria
A, et al: EULAR recommendations for the management of systemic
lupus erythematosus: 2023 update. Ann Rheum Dis. 83:15–29.
2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rubin RL: Drug-induced lupus. In: Wallace
DJ, Hahn BH, (eds.): Dubois' Lupus Erythematosus and Related
Syndromes. 9th edition. Elsevier, 2019.
|
|
12
|
Kim JW, Kim HA, Suh CH and Jung JY: Sex
hormones affect the pathogenesis and clinical characteristics of
systemic lupus erythematosus. Front Med (Lausanne).
9(906475)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Fanouriakis A, Tziolos N, Bertsias G and
Boumpas DT: Update on the diagnosis and management of systemic
lupus erythematosus. Ann Rheum Dis. 80:14–25. 2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Andreoli L, Chighizola CB, Iaccarino L,
Botta A, Gerosa M, Ramoni V, Tani C, Bermas B, Brucato A, Buyon J,
et al: Immunology of pregnancy and reproductive health in
autoimmune rheumatic diseases. Autoimmun Rev.
22(103259)2023.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Tarter L and Bermas BL: Expert perspective
on a clinical challenge: Lupus and pregnancy. Arthritis Rheumatol.
76:321–331. 2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kim JW, Jung JY, Kim HA, Yang JI, Kwak DW
and Suh CH: Lupus low disease activity state achievement is
important for reducing adverse outcomes in pregnant patients with
systemic lupus erythematosus. J Rheumatol. 48:707–716.
2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Tani C, Zucchi D, Haase I, Larosa M,
Crisafulli F, Strigini FAL, Monacci F, Elefante E, Mucke J, Choi
MY, et al: Are remission and low disease activity state ideal
targets for pregnancy planning in systemic lupus erythematosus? A
multicentre study. Rheumatology (Oxford). 60:5610–5619.
2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Larosa M, Costedoat-Chalumeau N,
Guettrot-Imbert G, Le Guern V, Morel N, Jesus D, Iaccarino L, Inês
L and Doria A: SLE-DAS in the first trimester of gestation predicts
maternal lupus flares later in pregnancy. Front Pharmacol.
12(660123)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Murata T, Kyozuka H, Fukuda T, Toba N,
Kanno A, Yasuda S, Yamaguchi A, Nomura Y, Kanno T, Migita K and
Fujimori K: Maternal disease activity and serological activity as
predictors of adverse pregnancy outcomes in women with systemic
lupus erythematosus: A retrospective chart review. Arch Gynecol
Obstet. 305:1177–1183. 2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sims CA, Eudy AM, Doss J, Rogers JL, Sadun
RE, Criscione-Schreiber L, Sun K and Clowse ME: The impact of
pregnancy planning and medical readiness on reproductive outcomes
in women with systemic lupus erythematosus. Lupus. 32:1666–1674.
2023.PubMed/NCBI View Article : Google Scholar
|
|
21
|
McDonald EG, Bissonette L, Ensworth S,
Dayan N, Clarke AE, Keeling S, Bernatsky S and Vinet E: Monitoring
of systemic lupus erythematosus pregnancies: A systematic
literature review. J Rheumatol. 45:1477–1490. 2028.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Morales-Martinez FA, Salas-Castro C,
García-Garza MR, Valdés-Martínez O, García-Luna SM, Garza-Elizondo
M, Vidal-Gutiérrez O, Saldívar-Rodríguez D and Sordia-Hernández LH:
Evaluation of the ovarian reserve in women with systemic lupus
erythematosus. J Fam Reprod Health. 15:38–44. 2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ejaz K, Abid D, Juneau P, Chu J and Hasni
S: Use of gonadotropin-releasing hormone agonists for ovarian
preservation in patients receiving cyclophosphamide for systemic
lupus erythematosus: A meta-analysis. Lupus. 31:1706–1713.
2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Morand EF, Furie R, Tanaka Y, Bruce IN,
Askanase AD, Richez C, Bae SC, Brohawn PZ, Pineda L, Berglind A, et
al: Trial of anifrolumab in active systemic lupus erythematosus. N
Engl J Med. 382:211–221. 2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Petri M, Kim MY, Kalunian KC, Grossman J,
Hahn BH, Sammaritano LR, Lockshin M, Merrill JT, Belmont HM,
Askanase AD, et al: Combined oral contraceptives in women with
systemic lupus erythematosus. N Engl J Med. 353:2550–2558.
2005.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Stamm B, Barbhaiya M, Siegel C, Lieber S,
Lockshin M and Sammaritano L: Infertility in systemic lupus
erythematosus: What rheumatologists need to know in a new age of
assisted reproductive technology. Lupus Sci Med.
9(e000840)2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Moyer A and Edens C: Impact of systemic
lupus erythematosus on conception: Insights into infertility,
fertility preservation, assisted reproductive technology, and
pregnancy outcomes. Semin Reprod Med. 42:209–227. 2024.PubMed/NCBI View Article : Google Scholar
|
|
28
|
de Jesus GR, Lacerda MI, Rodrigues BC, Dos
Santos FC, do Nascimento AP, Cristóvão Porto L, de Jesús NR, Levy
RA and Klumb EM: Soluble Flt-1, placental growth factor, and
vascular endothelial growth factor serum levels to differentiate
between active lupus nephritis during pregnancy and preeclampsia.
Arthritis Care Res Hoboken. 73:717–721. 2021.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Hirashima C, Ogoyama M, Abe M, Shiraishi
S, Sugase T, Niki T, Matsubara S and Ohkuchi A: Clinical usefulness
of serum levels of soluble fms-like tyrosine kinase 1/placental
growth factor ratio to rule out preeclampsia in women with
new-onset lupus nephritis during pregnancy. CEN Case Rep. 8:95–100.
2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Jiang Y, Tao M, Chen J, Luo L, You Q, Wu H
and Zhang N: Calcineurin inhibitors in the treatment of systemic
lupus erythematosus during pregnancy: A narrative review with
emphasis on efficacy and safety. Eur J Obstet Gynecol Reprod Biol.
294:148–15. 2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Gryka-Marton M, Szukiewicz D,
Teliga-Czajkowska J and Olesinska M: An overview of neonatal lupus
with anti-Ro characteristics. Int J Mol Sci.
22(9281)2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Garcia S and Campos-de-Carvalho AC:
Neonatal lupus syndrome: The heart as a target of the immune
system. Acad Bras Cienc. 72:83–89. 2007.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Izmirly P, Kim M, Friedman DM,
Costedoat-Chalumeau N, Clancy R, Copel JA, Phoon CKL, Cuneo BF,
Cohen RE, Robins K, et al: Hydroxychloroquine to prevent recurrent
congenital heart block in fetuses of anti-SSA/Ro-positive mothers.
J Am Coll Cardiol. 76:292–302. 2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Bremme K, Honkanen S, Gunnarsson I and
Chaireti R: The presence of lupus nephritis additionally increases
the risk of preeclampsia among pregnant women with systemic lupus
erythematosus. Lupus. 28:1013–1021. 2019.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Moroni G, Calatroni M and Ponticelli C:
The impact of preeclampsia in lupus nephritis. Expert Rev Clin
Immunol: May 10:1-13, 2022 doi: 10.1080/1744666X.2022.2074399 (Epub
ahead of print).
|
|
36
|
Huang J, Zhu Q, Wang B, Wang H, Xie Z, Zhu
X, Zhao T and Yang Z: Antiphospholipid antibodies and the risk of
adverse pregnancy outcomes in patients with systemic lupus
erythematosus: A systematic review and meta-analysis. Expert Rev
Clin Immunol. 20:793–801. 2024.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Tektonidou MG, Andreoli L, Limper M,
Amoura Z, Cervera R, Costedoat-Chalumeau N, Cuadrado MJ, Dörner T,
Ferrer-Oliveras R, Hambly K, et al: EULAR recommendations for the
management of antiphospholipid syndrome in adults. Ann Rheum Dis.
78:1296–1304. 2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Vaught AJ, Gavriilaki E, Hueppchen N,
Blakemore K, Yuan X, Seifert SM, York S and Brodsky RA: Direct
evidence of complement activation in HELLP syndrome: A link to
atypical hemolytic uremic syndrome. Exp Hematol. 44:990–998.
2016.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Smyth A, Oliveira GH, Lahr BD, Bailey KR,
Norby SM and Garovic VD: A systematic review and meta-analysis of
pregnancy outcomes in patients with systemic lupus erythematosus
and lupus nephritis. Clin J Am Soc Nephrol. 51:2060–2068.
2010.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Yelnik CM, Laskin CA, Porter TF, Branch
DW, Buyon JP, Guerra MM, Lockshin MD, Petri M, Merrill JT,
Sammaritano LR, et al: Lupus anticoagulant is the main predictor of
adverse pregnancy outcomes in aPL-positive patients: Validation of
PROMISSE study results. Lupus Sci Med. 3(e000131)2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Stone S, Pijnenborg R, Vercruysse L,
Poston R, Khamashta MA, Hunt BJ and Poston L: The placental bed in
pregnancies complicated by primary antiphospholipid syndrome.
Placenta. 27:457–467. 2006.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Di Ludovico A, Rinaldi M, Mainieri F, Di
Michele S, Girlando V, Ciarelli F, La Bella S, Chiarelli F,
Attanasi M, Mauro A, et al: Molecular mechanisms of fetal and
neonatal lupus: A narrative review of an autoimmune disease
transferal across the placenta. Int J Mol Sci.
25(5224)2024.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Lun Hon K and Leung AK: Neonatal lupus
erythematosus. Autoimmune Dis. 2012(301274)2012.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Andreoli L, Bertsias GK, Agmon-Levin N,
Brown S, Cervera R, Costedoat-Chalumeau N, Doria A, Fischer-Betz R,
Forger F, Moraes-Fontes MF, et al: EULAR recommendations for
women's health and the management of family planning, assisted
reproduction, pregnancy and menopause in patients with systemic
lupus erythematosus and/or antiphospholipid syndrome. Ann Rheum
Dis. 76:476–485. 2017.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Yamamoto Y and Aoki S: Systemic lupus
erythematosus: Strategies to improve pregnancy outcomes. Int J
Womens Health. 8:265–272. 2016.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Götestam Skorpen C, Hoeltzenbein M,
Tincani A, Fischer-Betz R, Elefant E, Chambers C, da Silva J,
Nelson-Piercy C, Cetin I, Costedoat-Chalumeau N, et al: The EULAR
points to consider for use of antirheumatic drugs before pregnancy
and during pregnancy and lactation. Ann Rheum Dis. 75:795–810.
2016.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Kemp MW, Newnham JP, Challis JG, Jobe AH
and Stock SJ: The clinical use of corticosteroids in pregnancy. Hum
Reprod Update. 22:240–259. 2016.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Lateef A and Petri M: Systemic lupus
erythematosus and pregnancy. Rheum Clin North Am. 43:215–226.
2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
US Food and Drug Administration: FDA
recommends avoiding use of NSAIDs in pregnancy at 20 weeks or later
because they can result in low amniotic fluid: NSAIDs may cause
rare kidney problems in unborn babies, 2020.
|
|
50
|
Di Prima FA, Valenti O, Hyseni E, Giorgio
E, Faraci M, Renda E, De Domenico R and Monte S: Antiphospholipid
syndrome during pregnancy: The state of the art. J Prenat Med.
5:41–53. 2011.PubMed/NCBI
|
|
51
|
Schreiber K and Hunt BJ: Managing
antiphospholipid syndrome in pregnancy. Thromb Res. 181 (Suppl
1):S41–S46. 2019.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Nori W, Akram NN and Al-Ani RM: Update on
hydroxychloroquine use in pregnancy. World J Exp Med. 13:99–101.
2023.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Hu Z, Gao R, Huang W, Wang H and Qin L:
Effect of hydroxychloroquine on lupus activity, preeclampsia and
intrauterine growth restriction in pregnant women with systemic
lupus erythematosus and/or antiphospholipid syndrome: A systematic
review and meta-analysis. J Clin Med. 12(485)2023.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Duan J, Ma D, Wen X, Guo Q, Gao J, Zhang
G, Xu K and Zhang L: Hydroxychloroquine prophylaxis for
preeclampsia, hypertension and prematurity in pregnant patients
with systemic lupus erythematosus: A meta-analysis. Lupus.
30:1163–1174. 2021.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Nørgård B, Pedersen L, Fonager K,
Rasmussen SN and Sørensen HT: Azathioprine, mercaptopurine and
birth outcome: A population-based cohort study. Aliment Pharmacol
Ther. 17:827–834. 2023.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Natekar A, Pupco A, Bozzo P and Koren G:
Safety of azathioprine use during pregnancy. Can Fam Physician.
57:1401–1402. 2011.PubMed/NCBI
|
|
57
|
Perez-Aytes A, Marin-Reina P, Boso V, Ledo
A, Carey JC and Vento M: Mycophenolate mofetil embryopathy: A newly
recognized teratogenic syndrome. Eur J Med Genet. 61:16–21.
2017.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Merlob P, Stahl B and Klinger G: Tetrada
of the possible mycophenolate mofetil embryopathy: A review. Reprod
Toxicol. 28:105–108. 2009.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Jackson P, Paquette L, Watiker V, Randolph
L, Ramanathan R and Seri I: Intrauterine exposure to mycophenolate
mofetil and multiple congenital anomalies in a newborn: Possible
teratogenic effect. Am J Med Genet A. 149A:1231–1236.
2009.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Zhu Q, Wang J, Sun Q, Xie Z, Li R, Yang Z,
Song Z, Yang K and Zhao T: Effect of hydroxychloroquine on
pregnancy outcome in patients with SLE: A systematic review and
meta-analysis. Lupus Sci Med. 11(e001239)2024.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Rovin BH, Teng YKO, Ginzler EM, Arriens C,
Caster DJ, Romero-Diaz J, Gibson K, Kaplan J, Lisk L, Navarra S, et
al: Efficacy and safety of voclosporin versus placebo for lupus
nephritis (AURORA 1): A double-blind, randomised, multicentre,
placebo-controlled, phase 3 trial. Lancet. 397:2070–2080.
2021.PubMed/NCBI View Article : Google Scholar
|