Introduction
Hypertensive disorders of pregnancy (HDP) are one of
the major causes of maternal mortality around the world. Routine
prenatal care decreases the morbidity rate of the
pregnancy-specific seizure disorder, eclampsia; however, the rate
of preeclampsia, a common and major complication causing
significant maternal and fetal morbidity and mortality worldwide
(1), remains largely unchanged in
China.
A great deal of effort has been directed at the
identification of HDP etiology and pathogenesis; however, there is
no specific biomarker or test ready for clinical use to make early
diagnosis and predict severity, although there are some encouraging
findings (2). Based on a century
of research into HDP, there is increased understanding of this
disease; however, the complete etiology and pathogenesis remain
unclear because the causes of HDP are not independent and specific
biomarkers and methods are limited. Therefore, identifying a useful
measure to make early diagnosis and estimate the severity of HDP is
currently an important research hot spot in obstetrics.
Following the development of proteomics, new
approaches, including comparative differential proteomics, can
provide reliable data with accurate quantitation and good
reproducibility. At present there are various novel differential
proteomics analysis methods, among which difference gel
electrophoresis (DIGE) technology is one of the most popular, as it
has high-resolution, inherited from two-dimensional gel
electrophoresis (2-DE), and has high reproducibility, high
sensitivity, high throughput capability and high dynamic range.
DIGE is a method that can label protein samples with different
fluorescent dyes prior to 2-DE, and can separate up to three
different protein samples at the same time in one two-dimensional
gel (3,4). The internal standard is used to match
the protein patterns across gels; thus, negating the problem of
inter-gel variation, a common issue with 2-DE (4). Recently, this technology has
exhibited important value for early diagnosis of malignant tumors,
including nasopharyngeal carcinoma, breast cancer, gastric cancer,
liver cancer, autoimmune disease and infectious diseases, with
specificity and sensitivity up to 90% (5). This technology has also been used to
investigate obstetrical diseases (6). Based on differential proteome
analysis of fetal accessory (including placenta, membrane,
umbilical cord and amniotic fluid) and maternal body fluids,
including placenta, amniotic fluid, blood, cerebrospinal fluid and
urine, it is possible to investigate the molecular biology of
pregnancy and its complications. By comparing the differential
proteome of normal pregnancy and those with obstetrical
complications, certain potential specific molecular biomarkers may
be identified.
Urine is the final metabolic product of blood
following glomerular filtration and renal tubule resorption; thus,
the change of its composition, quantity and characteristics can
reflect the information of urinary system diseases, and even the
metabolic condition of the whole body. Though the American College
of Obstetricians and Gynecologists no longer consider proteinuria
as a diagnostic criteria for preeclampsia (7), the quantity and quality of the
protein changes in urine may still be associated with preeclampsia;
therefore, the current study aimed to determine the differences in
protein content between the urine of patients with HDP and normal
pregnancy using a technology platform based on DIGE, matrix
assisted laser desorption ionization-time of flight/time of flight
mass spectrometry (MALDI TOF/TOF) and bioinformatics analysis.
Subsequently, the content changes of identified proteins in the
patient urine were validated using ELISA.
Materials and methods
Materials
Cyanine (Cy) 2, Cy3, Cy5, Tris,
3-[(3-cholamidopropyl)dimethylammonio]-1-propanesulfonate,
tetramethylethylenediamine, dithiothreitol (DTT), EDTA,
dimethylformamide, Ettan™ 2-D Quant Kit, Ettan™ 2-D Clean-up Kit
were obtained from GE Healthcare (Chicago, IL, USA).
Trichloroacetic acid, trifluoroacetic acid and
cyano-4-hydroxycinnamic acid were purchased from Sigma-Aldrich
(Merck KGaA, Darmstadt, Germany). Human prostaglandin-H2
D-isomerase (L-PGDS; cat. no. RD191113100R) and perlecan (cat. no.
DPSG10) ELISA kits were from BioVendor-Laboratorni Medicina A.S.
(Brno, Czech Republic).
Sample preparation
Urine samples were collected from 10 patients with
gestational hypertension (Group G), 10 patients with mild
preeclampsia (Group M), 10 patients with severe preeclampsia (Group
S) and 10 normal pregnancies (Group N) admitted to the Department
of Obstetrics, Shenzhen Maternity and Child Healthcare Hospital
Affiliated to Southern Medical University (Shenzhen, China) between
September 2013 and December 2013, (aged 26–41). Written informed
consent was obtained from all study participants and ethical
approval for this study was obtained from the local research ethics
committee of Southern Medical University. Gestational hypertension
is diagnosed by BP ≥140/90 mmHg first appearing during pregnancy
and returning to normal 12 weeks postpartum without proteinuria.
Mild preeclampsia is diagnosed by BP ≥140/90 mmHg after 20
gestational weeks and urinary albumin ≥0.3 g/24 h or (+). The
diagnosis criteria of severe preeclampsia includes BP ≥160/110 mmHg
and urinary albumin ≥5 g/24 h or (++), serum creatinine level ≥106
µmol/l, blood platelet <100×109/l, elevated lactate
dehydrogenase, elevated transaminase, persistent headache or visual
disorder, persistent upper abdomen discomfort and fetal growth
restriction. Women with a history of hypertension, renal disease,
heart disease, liver disease, diabetes, severe anemia, malignant
tumor and rheumatic disease were excluded. The clinical data from
these 40 cases are presented Table
I. A total of 10 urine samples were mixed into one sample
separately and then ultrafiltration and centrifugation were
performed to obtain the urine protein sample. Ettan™ 2-D Clean-up
kit and Ettan™ 2-D Quant kit were used to purify and quantify the
urine protein sample.
 | Table I.Patient clinical information. |
Table I.
Patient clinical information.
| Characteristic | Group N | Group G | Group M | Group S | F-value | P-value |
|---|
| Age (years) | 32.58±4.43 | 33.41±4.56 | 31.72±5.12 | 34.02±3.96 | 0.243 |
0.865 |
| Gravity | 2.38±1.27 | 2.58±1.13 | 2.43±1.21 | 2.41±1.34 | 0.026 |
0.994 |
| Parity | 0.68±0.26 | 0.75±0.17 | 0.73±0.21 | 0.67±0.25 | 0.147 | 0.93 |
| Gestational age
(days) | 277.75±18.27 | 274.36±20.15 | 269.56±22.35 | 265.84±20.75 | 0.329 |
0.804 |
Protein labeling with CyDye DIGE
fluor
Urine protein samples were labeled with Cy2, Cy3 and
Cy5 following dissolving in dimethylformamide. Typically, 50 µg
lysate was labeled with 400 pmol Cy3 and Cy5, while the same amount
of the pool standard that contained equal quantities of all the
samples was labeled with Cy2, namely the internal label. Each
sample was loaded on two gels labeled with Cy3 and Cy5 to achieve
statistical confidence. Prior to quenching with 1 µl 10 mM lysine
for 10 min on ice, the Cy dye was placed in the dark on ice for 30
min to acquire labeling reactions. These labeled samples were then
combined for 2-D DIGE analysis.
2-DE
2-DE was performed with Ettan™ IPGPhor and Ettan™
DALT Six electrophoresis units. Prior to SDS-PAGE, each strip was
equilibrated with 10 ml equilibration buffer A (6 M urea, 50 mM
Tris-HCL pH 8.8, 30% glycerol, 2% SDS, 10 mg/ml DTT) on a rocking
table for 15 min, followed by 10 ml equilibration of buffer B (6 M
urea, 50 mM Tris-HCL pH 8.8, 30% glycerol, 2% SDS, 25 mg/ml
iodoacetamide) for another 15 min. Then the trips were loaded and
run on 12% acrylamide isocratic Laemmli gels with running parameter
settings as constant power of 3 W per gel for 45 min, followed by
17 W per gel until the bromophenol blue dye front had run off the
bottom of the gels. Then, the Typhoon 9410 imager (GE Healthcare)
was used to visualize the labeled protein and match with DIGE
images with DeCyder 6.5 software (GE Healthcare) to identify the
spots of interest.
MALDI TOF/TOF and protein
identification
Protein spots of interest were excised using an
automatic Spot picker, and then the picked spots underwent in-gel
digestion, followed by analysis with ABI 4800 MALDI TOF/TOF mass
spectrometry (Applied Biosystems; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA). The mass spectral data were submitted to the
SWISSPROT database (www.uniprot.org/) using Mascot software (www.matrixscience.com). The proteins with
identification probabilities of >95% given by Mascot were
considered successfully identified and then received bioinformatics
analysis.
ELISA analysis
From the identified proteins, two were selected,
L-PGDS and perlecan, to be analyzed by ELISA to confirm the content
change in urine. Urine samples were collected from another 50
patients with gestational hypertension (Group G), 50 patients with
mild preeclampsia (Group M), 50 patients with severe preeclampsia
(Group S) and 50 normal pregnancies (Group N) admitted to
Department of Obstetrics, Shenzhen Maternity and Child Healthcare
Hospital Affiliated to Southern Medical University (Shenzhen,
China), between January 2014 and December 2014. Similarly, written
informed consent was obtained from all study participants and
ethical approval for this study was obtained from the local
research ethics committee of Shenzhen Hospital, Southern Medical
University (Shenzhen, China). The inclusion criteria were
consistent with the diagnosis criteria. Women with a history of
hypertension, renal disease, heart disease, liver disease,
diabetes, severe anemia, malignant tumor and rheumatic disease were
excluded. According to the kit (BioVendor-Laboratorni Medicina
A.S.), the urine concentration of L-PGDS and perlecan were
determined in all patients.
Statistical analysis
Data were presented as the mean ± standard
deviation. The one-way analysis of variance and further multiple
comparisons by Student-Newman-Keuls test were used for comparing
the L-PGDS and perlecan between Group N, G, N and M. SPSS (version
19.0; IBM Corp., Armonk, NY, USA) was used for statistical
analysis. P<0.05 was considered to indicate the statistically
significant difference.
Results
Results of 2-DE and mass
spectrometry
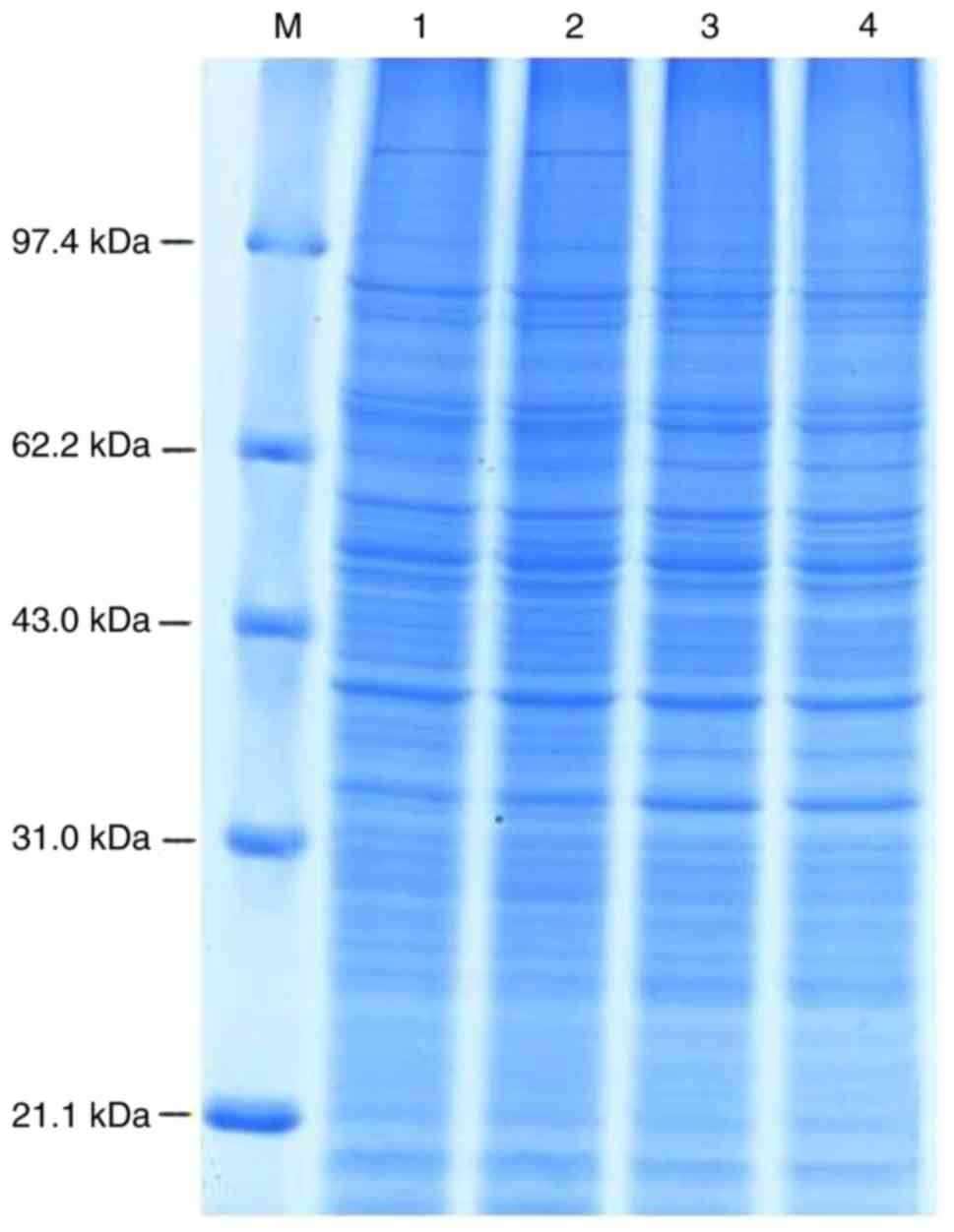
Total proteins were extracted from the urine of 10
patients with gestational hypertension, 10 patients with mild
preeclampsia, 10 patients with severe preeclampsia and 10 normal
pregnancies, and then 50 µg samples of the four groups subjected to
SDS-PAGE electrophoresis for accuracy (Fig. 1). The 2-DE images were obtained by
fluorescence scanning and analyzed using DeCyder software to
estimate the abundance of proteins in each sample objectively to
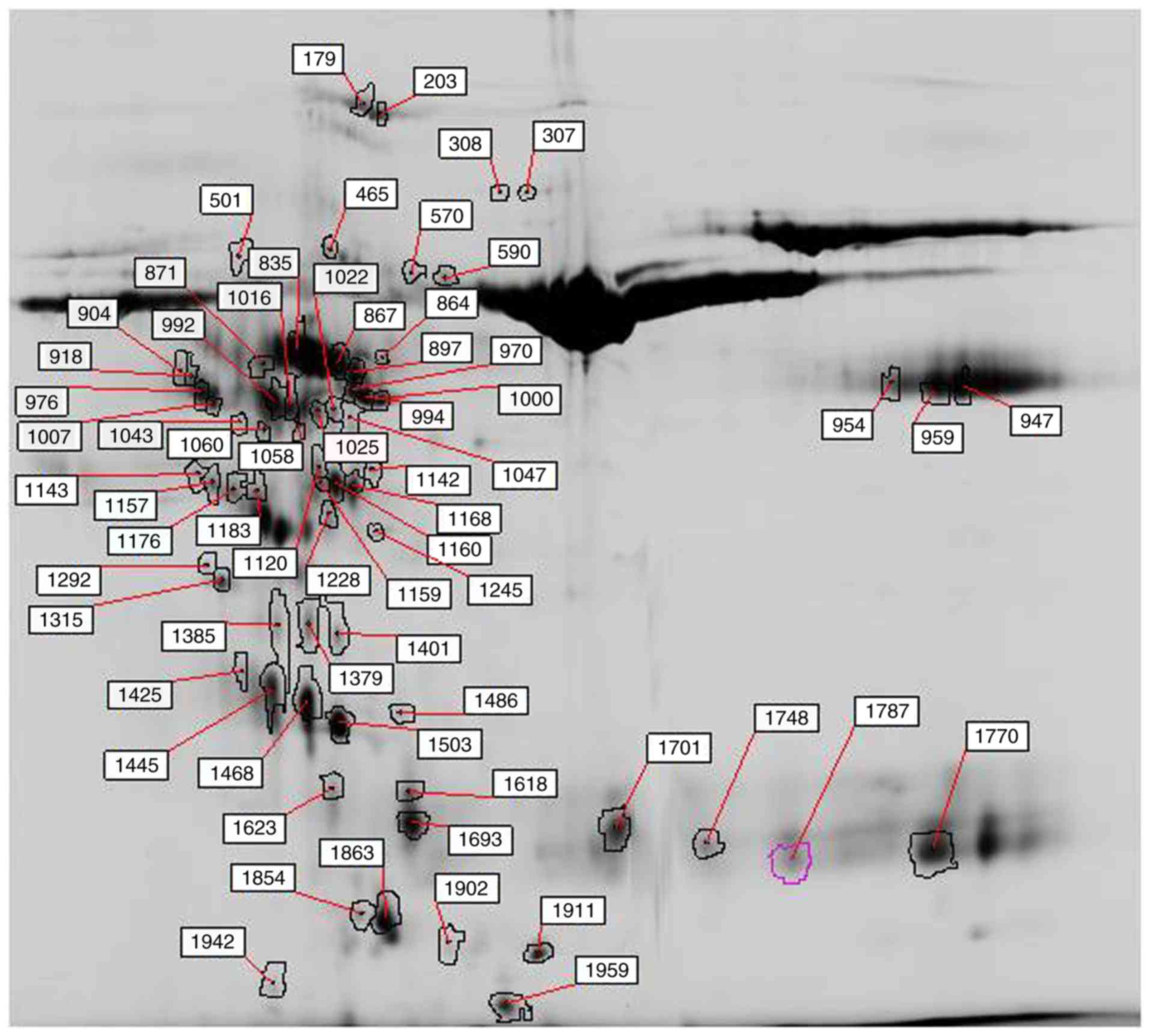
provide quantitative data. A filter threshold of 1.5 was set to
detect the protein spots of interest that had a significant change
among the four groups. Compared with the normal pregnancy group, 44
differential protein spots were identified, among which 22 were
upregulated and 22 were downregulated in the gestational
hypertension group, 15 were upregulated and 30 downregulated in the
mild preeclampsia group compared with the gestational hypertension
group. There were 45 differential protein spots when comparing the
severe preeclampsia group with the mild preeclampsia group, of
which 9 were upregulated and 36 were downregulated. On account of
some protein spots changing in all four groups, 65 differential
protein spots were analyzed in total (Fig. 2).
Following mass spectrometry analysis, 30
differential proteins were identified. Ceruloplasmin, Ig-γ-3 chain
C region and pancreatic α-amylase were all upregulated in
hypertensive disorders in pregnancy; however, hemopexin,
antithrombin-III, kininogen-1, α-2-HS-glycoprotein, vitamin
D-binding protein, actin cytoplasmic 2, apolipoprotein A-I and
chorionic somatomam-motropin hormone were all downregulated. For
α-1B-glycoprotein, cadherin-11, pregnancy-specific β-1-glycoprotein
11, gelsolin, inter-α-trypsin inhibitor heavy chain H4, keratin
type II cytoskeletal 2 epidermal, protein α-1-microglobulin/bikunin
precursor (AMBP), vesicular integral-membrane protein VIP36,
filamin-A-interacting protein 1, semenogelin-1, L-PGDS, Ig κ chain
V–III region WOL, perlecan, mannan-binding lectin serine protease
2, fibrinogen alpha chain and long palate, lung and nasal
epithelium carcinoma-associated protein 1 contents were higher in
gestational hypertension than in normal pregnancies, but lower in
mild and severe preeclampsia. By contrast, serum albumin and
α-1-antitrypsin were lower in gestational hypertension compared
with normal pregnancies, and higher in mild and severe
preeclampsia. No significant difference was observed in the
remaining protein, ganglioside GM2 activator, in the four groups.
The genes and functions of all these identified proteins are
presented in Table II.
| Table II.Functional analysis of differential
proteins. |
Table II.
Functional analysis of differential
proteins.
| Accession no. | Protein name | Gene name | Functions |
|---|
| P00450 | Ceruloplasmin | CP | Transfer Fe2+ into
Fe3+, play an important role in the iron transport in the
membrane |
| P02768 | Serum albumin | ALB | Regulate the osmotic
pressure of the blood |
| P04217 |
α-1B-glycoprotein | A1BG | Play a role in the
regulation of Cell recognition and cellular behaviour |
| P01009 | α-1-antitrypsin | SERPINA1 | Irreversible
inhibition of trypsin, chymotrypsin and fibrinolysin |
| P02790 | Hemopexin | HPX | Combine and transport
heme |
| P55287 | Cadherin-11 | CDH11 | A kind of
Calcium-depend cell protein and can differentiate Heterogeneous
cells |
| P01008 | Antithrombin-III | SERPINC1 | The most important
serine protease inhibitor in plasma |
| P01042 | Kininogen-1 | KNG1 | Play role in blood
clotting, inhibit platelet aggregation and increase blood vessel
permeability |
| P02765 |
α-2-HS-glycoprotein | AHSG | Stimulate the
endothocytic effect of cells and affect bone formation |
| P01860 | Ig-γ-3 chain C
region | IGHG3 | Participate in the
immune system |
| P04746 | Pancreatic
α-amylase | AMY2A | One kind of digestive
enzyme |
| P02774 | Vitamin D-binding
protein | GC | A multifunctional
protein that carries vitamin D and inhibits actin
polymerization |
| Q9UQ72 | Pregnancy-specific
β-1-glycoprotein 11 | PSG11 | A specific protein
involved in the pregnancy process that play role in the foetal
chromosomal abnormalities prenatal diagnosis and foetal growth
restriction |
| P06396 | Gelsolin | GSN | A calcium-regulated
actin, acting in the process of cilia formation |
| P63261 | Actin, cytoplasmic
2 | ACTG1 | A class of highly
conserved proteins present in a variety of motor cells |
| Q14624 | Inter-α-trypsin
inhibitor heavy chain H4 | ITIH4 | Acting in the acute
response period |
| P35908 | Keratin, type II
cytoskeletal 2 epidermal | KRT2 | Involved in the
keratinization process, and keratinocyte activation,
value-added |
| P02760 | Protein AMBP | AMBP | Include three
fragments: a1 microglobulin, a trypsin inhibitor light chain and
trypstatin |
| Q12907 | Vesicular
integral-membrane protein VIP36 | LMAN2 | Play role of
intracellular lectin in the early secretion and involved in
transporting polymer galactose |
| Q7Z7B0 | Filamin-A-interacting
protein 1 | FILIP1 | Involved in the role
of silk protein-A/F-actin axis, control of new cortical cells from
the beginning of the ventricle area |
| P04279 | Semenogelin-1 | SEMG1 | Involved in the
formation and ejaculation of gel matrix in epididymal
secretions |
| P41222 | Prostaglandin-H2
D-isomerase | PTGDS | Catalyses the
conversion of PGH2 to PGD2, a prostaglandin involved in smooth
muscle contraction/relaxation, and an inhibitor of platelet
aggregation |
| P01623 | Ig κ chain V–III
region WOL | – | Part of
immunoglobulin, involving in the immune system |
| P02647 | Apolipoprotein
A-I | APOA1 | Involved in the
reverse transport of cholesterol from the tissue to the liver |
| P01243 | Chorionic
somatomam-motropin hormone | CSH1 | Participate in
stimulating lactation, foetal growth and metabolism in
pregnancy |
| P98160 | Basement membrane
specific heparan sulfate proteoglycan core protein | HSPG2 | The complete
composition of the basement membrane, as a matrix appendage of
cells, plays an important role in vascularization |
| P17900 | Ganglioside GM2
activator | GM2A | Can regulate
phospholipid single chain and fatty acid, Can be combined with
ganglioside to stimulate ganglioside GM2 degradation |
| O00187 | Mannan-binding
lectin serine protease 2 | MASP2 | Serum proteins play
an important role in the activation of complement systems through
mannan-binding lectin serine protease 2 |
| P02671 | Fibrinogen α
chain | FGA | Fibrinogen has a
dual function: the monomer polymerization into fibrin, and act as a
cofactor in platelet aggregation |
| Q8TDL5 | Long palate, lung
and nasal epithelium carcinoma-associated protein1 | LPLUNC1 | By identifying and
removing pathogens, it may be a primary body of the human body
defence mechanism |
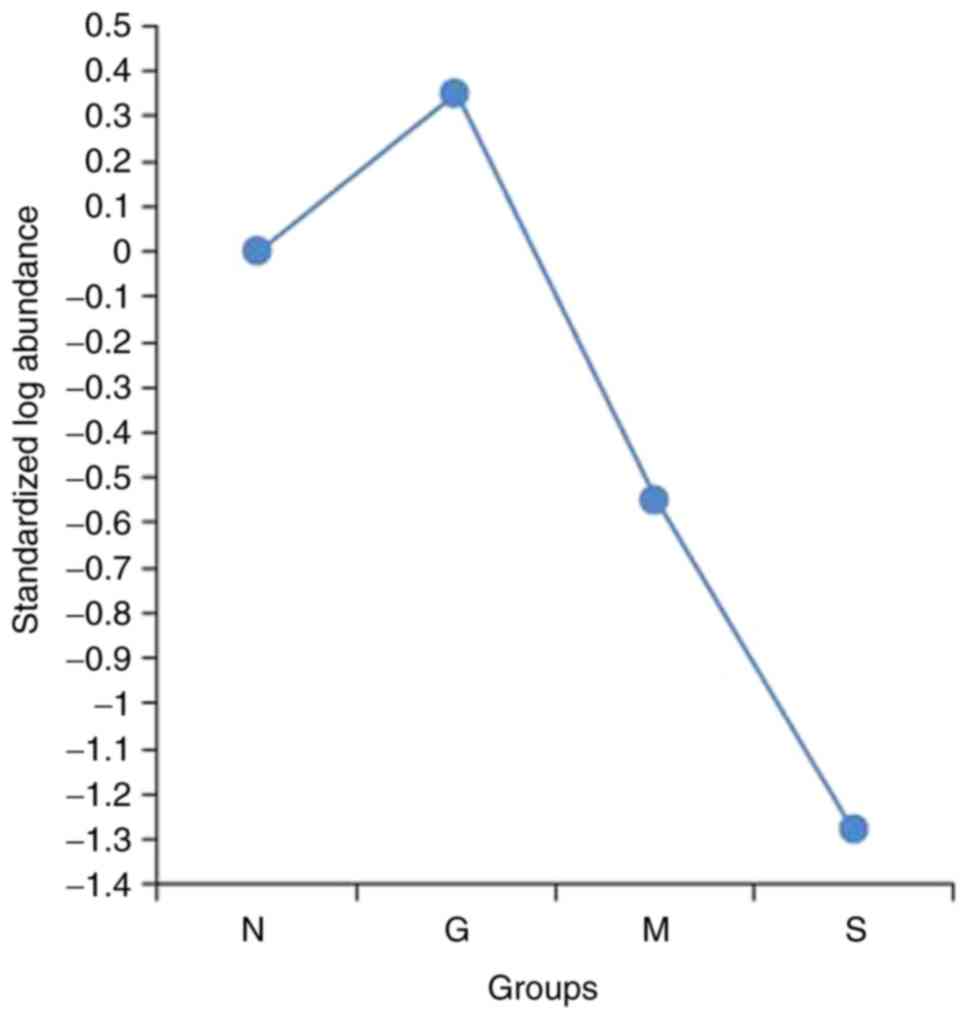
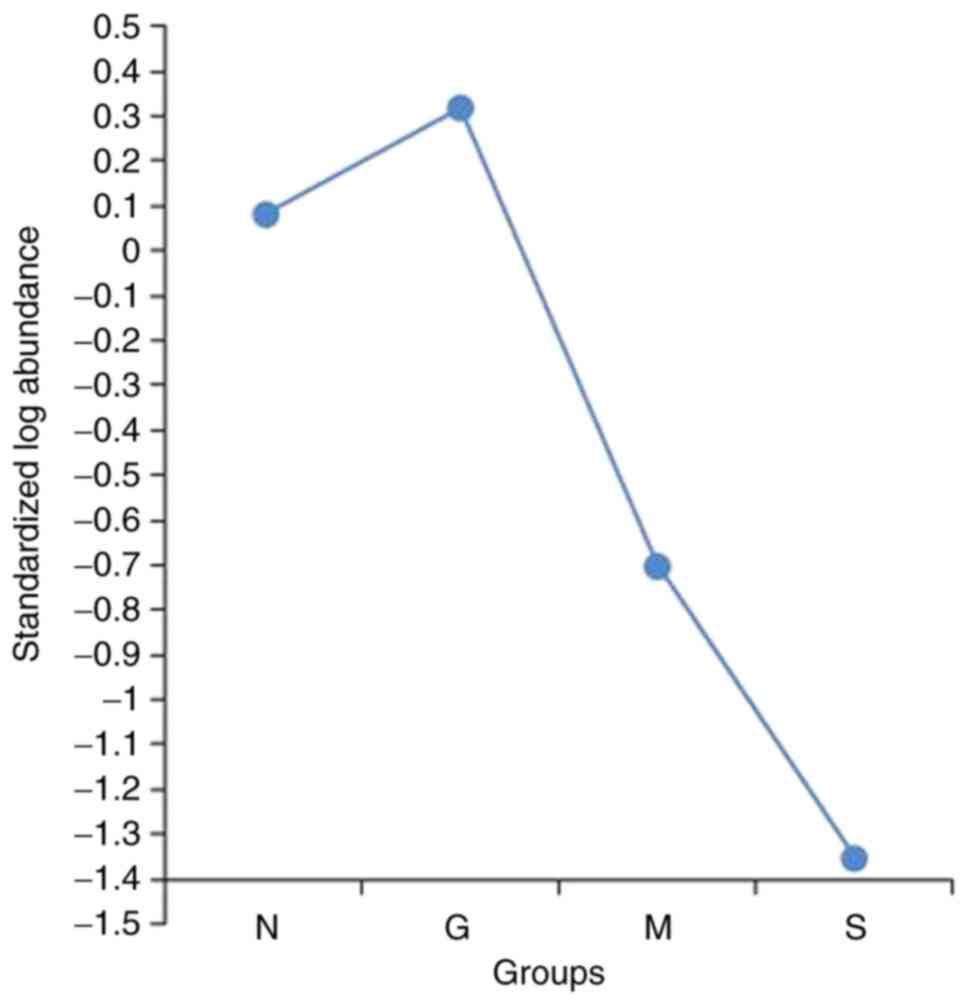
Using the DeCyder software, abundance curves of
these differential protein spots, no. 1,618 and no. 1,911, which
can reflect the state of renal function were simulated (Figs. 3 and 4). The abundance ratio of gestational
hypertension and normal pregnancies for spot no. 1,618 was 2.13,
and the ratio was 1.58 for spot no. 1911. However, for mild and
severe preeclampsia, the abundance curve exhibited reductions in
spot no. 1,618 and no. 1,911, with ratios of 0.26 and 0.16 in mild
preeclampsia, respectively, and 0.06 and 0.04 in severe
preeclampsia, respectively. According to mass spectrometry analysis
and database searching, spot no. 1,618 was confirmed as L-PGDS and
no. 1911 was perlecan. In consideration of their change trends, the
two proteins may have important effects in the genesis of
gestational hypertension and preeclampsia.
Results of ELISA
To validate the results regarding L-PGDS and
perlecan, ELISA was used for further confirmation in another 50
patients with gestational hypertension (Group G), 50 patients with
mild preeclampsia (Group M), 50 patients with severe preeclampsia
(Group S) and 50 normal pregnancies (Group N). When observing the
changes in L-PGDS, there was significant difference among the four
groups and further multiple comparisons indicated that there was no
variation between Group N (1.26±0.25 µg/ml) and Group G (1.32±0.16
µg/ml); however, the concentration of L-PGDS in Group M (0.94±0.23
µg/ml) and Group S (0.78±0.23 µg/ml) were significantly lower than
that of Group N and Group G (both P<0.001). When comparing Group
M with Group S, there were significantly lower levels in Group S
(P=0.023). Regarding the urine perlecan concentration, the results
illustrated a higher concentration in Group G (12.73±3.71 nmol/l;
P=0.036) and lower in Group M (8.02±1.66 nmol/l, P=0.006) and Group
S (6.63±1.39 nmol/l, P<0.001) compared with Group N (9.99±1.85
nmol/l). Similarly, perlecan was decreased in Group S compared with
Group M (P=0.039; Table
III).
| Table III.ELISA results of L-PGDS and perlecan
in the four patient groups. |
Table III.
ELISA results of L-PGDS and perlecan
in the four patient groups.
| Protein | Group N | Group G | Group M | Group S | F-value | P-value |
|---|
| L-PGDS (µg/ml) |
1.26±0.25a–c |
1.32±0.16b,c |
0.94±0.23c | 0.78±0.23 | 68.59 | <0.001 |
| Perlecan
(nmol/l) |
9.99±1.85b–d |
12.73±3.71b,c |
8.02±1.66c | 6.63±1.39 | 64.01 | <0.001 |
Discussion
With the development of DIGE and MALDI TOF/TOF
technologies, proteomic research has been widely used in the
post-genomics era, and can provide new opportunities to identify
the novel biomarkers for various important diseases, as it allows
for the large-scale investigation of proteins in complex biological
fluids and tissues in a high-throughput manner. The proteomic
studies of preeclampsia have predominantly focused on maternal
blood, placenta, amniotic fluid and trophoblast cells (3,4).
When comparing the levels the low molecular-weight protein in serum
from patients with preeclampsia in the early second trimester with
a control group, Anand et al (8) identified >60 potential biomarkers,
which when modeled in a 14 different multi-marker combinations
exhibited sensitivity and specificity of >90% for the early
detection of women at risk for preeclampsia. Another proteomic
study on preeclampsia indicated that C1s subcomponent and protein
AMBP were significantly overexpressed in the preeclamptic serum
(9), which may be useful in early
prediction.
Although urine is a good source of biomarkers, there
few studies have researched preeclampsia using urine samples and no
consistent results have been found (10). Carty et al (11) used a proteomic strategy to identify
urinary biomarkers that predict preeclampsia prior to the onset of
disease and screened out several biomarkers, including fibrinogen α
chain, collagen α chain and uromodulin fragments, which may
contribute to better prediction, monitoring and accurate diagnosis
of preeclampsia.
Proteinuria is used to distinguish between
gestational hypertension and preeclampsia; therefore, the quantity
and component changes of urine protein may have important role in
distinction of these two types of hypertensive disorders of
pregnancy (12,13). Differential proteins were examined
in the urine of patients with gestational hypertension, mild
preeclampsia, severe preeclampsia and normal pregnancies using DIGE
and mass spectrometry, and 30 differential proteins were
identified, among which α-1B-glycoprotein, cadherin-11,
pregnancy-specific β-1-glycoprotein 11, gelsolin, inter-α-trypsin
inhibitor heavy chain H4, keratin type II cytoskeletal 2 epidermal,
protein AMBP, vesicular integral-membrane protein VIP36,
filamin-A-interacting protein 1, semenogelin-1, mannan-binding
lectin serine protease 2, fibrinogen α chain and long palate, lung,
nasal epithelium carcinoma-associated protein 1, Ig κ chain V–III
region WOL, L-PGDS and perlecan were overexpressed in gestational
hypertension, and expression was reduced in patients with mild and
severe preeclampsia compared with that of normal pregnancies. All
these proteins have their own functions and may have certain
effects on the disease; information on their functions is presented
in Table III.
L-PGDS (β trace protein) has anionic charge, is of
smaller molecular weight than serum albumin (26,000 vs. 66,000 Da)
and catalyzes prostaglandin H2 conversion into prostaglandin D2.
L-PGDS is distributed in the central nervous system, visual system,
male genital system and cardiovascular system. L-PGDS is
synthesized in the choroid plexus or leptomeninges of the brain and
secreted steadily through cerebrospinal fluid into circulating
blood. Therefore it can be detected in cerebrospinal fluid, aqueous
fluid, blood plasma, urine and amnio fluid. As serum L-PGDS is
excreted through glomerular capillary walls, reduction in the
number of functioning glomeruli decreases the renal clearance of
L-PGDS and increases serum L-PGDS concentrations. Urinary L-PGDS
excretions may be more useful to predict the increased glomerular
permeability in an early stage of systemic diseases because of the
larger molecular weight and its anionic property (14,15).
In the current study, the concentration of urinary L-PGDS was
decreased in preeclampsia, particularly in severe preeclampsia,
indicating that the renal function was altered in these patients.
However, an opposing view can be found in which urinary L-PGDS
excretions are increased in patients with various forms of renal
diseases (16). Therefore, in the
future transgenic L-PGDS knock-out mouse models should be used to
verify its function in preeclampsia. Additionally, the product
produced by L-PGDS, prostaglandin D2, which inhibits platelet
aggregation and causes relaxation of vascular smooth muscle, may
have a role in the genesis of preeclampsia development (17).
Perlecan is a basement membrane-specific heparan
sulfate proteoglycan core protein and is one of the largest
proteoglycans, with a protein core of ~500 kDa that can be modified
by the addition of N-terminal heparan sulfate side chains. Perlecan
is particularly abundant in basement membrane and pericelluar
spaces, where it regulates diverse cellular processes, including
bone formation, inflammation, cardiac development and angiogenesis.
Located at the glomerular basement membrane and glomerular
endothelial surface layer, perlecan is the major component of the
filtration barrier and has an important role in maintaining renal
function. The N-terminal heparan sulfate side chains of perlecan
act as a reservoir for growth factors, which can promote
angiogenesis by presenting growth factors to their respective cell
surface receptors (18,19). By contrast, perlecan can inhibit
the autophagy of cells (18). The
result of the current study demonstrated that perlecan was
decreased in the urine of patients with preeclampsia compared with
normal pregnancies, and may indicate the existence of glomerular
filtration barrier injury resulting in proteinuria and renal
dysfunction, which supports previous research (20). The downregulated expression
perlecan in renal organ of different renal diseases and models
explains the pathogenesis of renal injury caused not only by
glomerular filtration barrier injury but also by the decrease of
angiogenesis and the increase of autophagy accompanied the decrease
of perlecan. All these evidence supported that perlecan may have
effect in the renal change of preeclampsia. Future work will likely
ensure this effect using gene knock-out model.
In conclusion, compared with normal pregnancies,
differential proteins were identified in the urine of patients with
gestational hypertension and preeclampsia. The identified proteins
may be good biomarkers for predicting and diagnosing the
hypertensive disorders in early pregnancy. L-PGDS and perlecan may
be involved in the genesis and development of renal injury in
preeclampsia. Further studies will be performed to investigate the
function of L-PGDS and perlecan in preeclampsia.
Acknowledgements
No applicable.
Funding
This study was funded by research project of
Shenzhen Health and Family Planning Commission (grant no.
201605011), Seedling Program of Shenzhen Hospital of Southern
Medical University (grant no. 2016MM09) and Natural Science
Foundation of China (grant no. 81701473).
Availability of data and materials
The datasets used or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HXG designed the study, performed the research,
analysed data and wrote the paper. YBZ performed research and
analyzed data. CPW performed research and wrote the paper. MZ
helped designed the study and checked the data. SWH performed
research and analyzed data.
Ethics approval and consent to
participate
Written informed consent was obtained from all study
participants and ethical approval for this study was obtained from
the local research ethics committee of Southern Medical
University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Roberts JM: Pregnancy related
hypertension. Maternal Fetal Medicine. Creasy RK and Resnik R:
(4th). W.B Saunders. (Philadelphia, PA). 833–872. 1998.
|
|
2
|
Frampton GK, Jones J, Rose M and Payne L:
Placental growth factor (alone or in combination with soluble
fms-like tyrosine kinase 1) as an aid to the assessment of women
with suspected pre-eclampsia: Systematic review and economic
analysis. Health Technol Assess. 20:1–160. 2016. View Article : Google Scholar
|
|
3
|
Pasquali M, Serchi T, Planchon S and
Renaut J: 2D-DIGE in proteomics. Methods Mol Biol. 1654:245–254.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Alban A, David SO, Bjorkesten L, Andersson
C, Sloge E, Lewis S and Currie I: A novel experimental design for
comparative two-dimensional gel analysis: Two-dimensional
difference gel electrophoresis incorporating a pooled internal
standard. Proteomics. 3:36–44. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wei YS, Zheng YH, Liang WB, Zhang JZ, Yang
ZH, Lv ML, Jia J and Zhang L: Identification of serum biomarkers
for nasopharyngeal carcinoma by proteomic analysis. Cancer.
112:544–551. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vuadens F, Benay C, Crettaz D, Gallot D,
Sapin V, Schneider P, Bienvenut WV, Lémery D, Quadroni M, Dastugue
B and Tissot JD: Identification of biologic markers of the
premature rupture of fetal membranes: Proteomic approach.
Proteomics. 3:1521–1525. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Roberts JM, August PA, Bakris G, Barton
JR, Bernstein IM, Druzin M, Gaiser RR, Granger JP, Jeyabalan A,
Johnson DD, et al: American College of Obstetricians and
Gynecologists; Task Force on Hypertension in Pregnancy.
Hypertension in pregnancy. Report of the American College of
Obstetricians and Gynecologists' Task Force on Hypertension in
Pregnancy. Obstet Gynecol. 122:1122–1131. 2013.PubMed/NCBI
|
|
8
|
Anand S, Bench Alvarez TM, Johnson WE,
Esplin MS, Merrell K, Porter TF and Graves SW: Serum biomarkers
predictive of pre-eclampsia. Biomark Med. 9:563–575. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim SM, Cho BK, Kang MJ, Norwitz ER, Lee
SM, Lee J, Park CW, Kim BJ, Jun JK, Park JS and Yi EC: Expression
changes of proteins associated with the development of preeclampsia
in maternal plasma: A case-control study. Proteomics. 16:1581–1589.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kolialexi A, Mavreli D, Tounta G, Mavrou A
and Papantoniou N: Urine proteomic studies in preeclampsia.
Proteomics Clin Appl. 9:501–506. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Carty DM, Siwy J, Brennand JE, Zürbig P,
Mullen W, Franke J, McCulloch JW, Roberts CT, North RA, Chappell
LC, et al: Urinary proteomics for prediction of preeclampsia.
Hypertension. 57:561–569. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Buhimschi IA, Zhao G, Funai E, Saade GR
and Buhimschi C: Proteomics analysis of urine in preeclampsia (PE):
A novel diagnosis for an old disease. Am J Obstet Gynecol.
193:S152005. View Article : Google Scholar
|
|
13
|
Blankley RT, Gaskell SJ, Whetton AD, Dive
C, Baker PN and Myers JE: A proof-of-principle gel-free proteomics
strategy for the identification of predictive biomarkers for the
onset of pre-eclampsia. BJOG. 116:1473–1480. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Uehara Y, Makino H, Seiki K and Urade Y;
L-PGDS Clinical Research Group of Kidney, : Urinary excretions of
lipocalin-type prostaglandin D synthase predict renal injury in
type-2 diabetes: A cross-sectional and prospective multicentre
study. Nephrol Dial Transplant. 24:475–482. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gerhardt T, Pöge U, Stoffel-Wagner B,
Klein B, Klehr HU, Sauerbruch T and Woitas RP: Serum levels of
beta-trace protein and its association to diuresis in haemodialysis
patients. Nephrol Dial Transplant. 23:309–314. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bacci MR, Cavallari MR, de Rozier-Alves
RM, Alves Bda C and Fonseca FL: The impact of
lipocalin-type-prostaglandin-D-synthase as a predictor of kidney
disease in patients with type 2 diabetes. Drug Des Devel Ther.
22:3179–3182. 2015.
|
|
17
|
Saito S, Tsuda H and Michimata T:
Prostaglandin D2 and reproduction. Am J Reprod Immunol. 47:295–302.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gubbiotti MA, Neill T and Iozzo RV: A
current view of perlecan in physiology and pathology: A mosaic of
functions. Matrix Biol. 57-58:285–298. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Smith S and Hassell JR: Focus on
molecules: Perlecan (HSPG2). Exp Eye Res. 83:471–472. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Conde-Knape K: Heparan sulfate
proteoglycans in experimental models of diabetes: A role for
perlecan in diabetes complications. Diabetes Metab Res Rev.
17:412–421. 2001. View
Article : Google Scholar : PubMed/NCBI
|