Introduction
One of the most frequent pathology in
Otorhinolaryngology practice is chronic rhinosinusitis (CRS), which
in the United States, affects 14% of the population, associated
with an increasing incidence of allergic rhinitis. CRS has a
considerable social and economic burden due mainly to frequent
visits to primary care facilities, as well as to an increase in the
use of pharmaceutical products (1). The quality of life index of patients
CRS, measured by bodily pain and social functioning is
significantly lower than that of patients with angina, congestive
heart failure, chronic obstructive pulmonary disease or even back
pain (2). Even if CRS is a highly
prevalent disease, there is a paucity of accurate epidemiological
data, as compared to available data on the diagnosis, microbiology
and treatment of the condition (3).
CRS is a chronic inflammatory disease which affects
the nasal cavities and paranasal sinuses; however, under this term
are likewise grouped a heterogeneous group of diseases, which have
different etiologies and pathological mechanisms (4). The CRS milieu can act as a reservoir
of bacteria (5) that may cause
other respiratory infections, such as laryngitis, tracheitis,
bronchitis and pneumonia (6), as
well as distant surgical site-like infections (7) and even invasive infections in rare
cases (8). The diagnosis of CRS is
usually clinical and straightforward and is based upon criteria
established by the American Academy of Otorhinolaryngology: The
presence of two or more significant symptoms (anterior or posterior
rhinorrhea, nasal obstruction/congestion, hyposmia/anosmia and
facial pain/pressure) which last for >12 weeks, confirmed by the
results of nasal endoscopy and/or a CT scan (1).
There are two types of CRS: CRS with nasal polyps
(CRSwNP) and CRS without nasal polyps (CRSsNP) (9). Different molecular mechanisms are
involved in the formation of nasal polyps. The genetic alterations
include the mutation and differential expression of the ras family
of genes (10). Expression
analyses have revealed the downregulation of wild-type B-Raf
proto-oncogene serine/threonine kinase (BRAF) (11) and the increased expression of
angiogenic markers, such as vascular endothelial growth factor A
(VEGFA) or transforming growth factor β1 (TGF-β1) (12). Another mechanism for the formation
of nasal polyps is infection with viruses, such as human herpes
virus or human papillomavirus (13). A previous histological study
demonstrated a significantly high proportion of tissue eosinophilia
in CRS, most prominently in patients with CRSwNP (14).
B lymphocytes are a key constituent of the adaptive
immune response and play important roles in various inflammatory
disorders (15–18). Although the most well-known role of
B lymphocytes is to produce antibodies that can contribute to
disease pathogenesis, B cells can also act as antigen-presenting
cells or regulatory cells by producing a large array of cytokines
that influence the inflammatory response. Recently, it was
demonstrated that the expression of TNF B cell-activating factor
(BAFF) is greatly increased in the nasal polyps of patients with
CRSwNP (16). Furthermore, several
histopathological studies have demonstrated increased levels of
immunoglobulins IgG, IgE and IgA in the sinuses of patients with
CRS (19–22).
As far as T cells are concerned, our understanding
of their activity in the nasal mucosa is based on extrapolation,
using cell cultures as a starting point, that can be obtained from
brushed nasal epithelial cells (23,24).
There are also studies on biopsies from nasal polyps showing the
role of cytokines, such as tumor necrosis factor-α (TNF-α)
(25) or other cytokines (26). Dendritic cells (DCs) serve as the
primary antigen-presenting cells (APCs) in the process of the nasal
immune response and consequently, they present antigens to naive T
lymphocytes (27).
CD45 is a protein tyrosine phosphatase (PTP), that
is expressed by hematopoietic cells, with the exception of
platelets and mature erythrocytes. PTP is encoded by the PTPRC gene
located on chromosome 1. Furthermore, CD45 plays important roles in
T cell receptor (TCR) and B cell receptor (BCR) signal
transduction. CD45 isoforms are specific to the activation and
maturation state of the cells. There are 3 isoforms of CD45: B220
expressed on B lymphocytes, CD45 RA expressed on naive T
lymphocytes and CD45 RO expressed on activated and memory T
lymphocytes (28).
CD20 is considered a pan-antigen for B lymphocytes,
expressed on mature B cells, but not on active plasmocytes
(18). CD20 is a membrane
non-glycosylated phosphoprotein of 33–37 kDa which contains three
hydrophobic regions that are embedded in the cell membranes.
Additional amino and carboxyl long ends are localized
intracellularly with only a portion of the molecule exposed
extracellularly. This antigen is involved in the modulation of B
cells, proliferation and differentiation. The CD20 antigen is
expressed early in the development of pre-B cells, supposedly even
before the cytoplasmic expression of alpha chains whereas it is not
detected in plasma cells. This antigen is not expressed by
monocytes, erythrocytes and mesenchymal cells (29).
Major producers of interleukin (IL)-13 and IL-5 are
the group 2 innate lymphoid cells (ILC2s) (30,31).
These cells are involved in the Th2 type inflammatory response and
mediate among other processes, intestinal immunity to helminths,
the hyperreactivity of the airways and asthmatic bronchial
obstruction (32,33).
The treatment of CRS is based on corticosteroids,
antibiotics and endoscopic sinus surgery. However, the application
of these treatments does not induce a significant change in the
evolution of the disease, the need for surgery or in the prevention
of recurrences (34–36). Clearly the pathogenesis of CRS and
factors that promote mucosal inflammation requires a deeper
understood in order to develop novel diagnostic and therapeutic
tools or strategies.
On the basis of the above-mentioned aspects, the
present study, which analyzes fragments of nasal polyps surgically
resected from patients with CRSwNP, proposes the assessment of B
lymphocytes [using activated T cells (ATC) armed with CD20
antibody] and T lymphocytes (using ATC armed with anti-CD3
antibody), the presence of CD45+ cells (the leukocyte
common antigen) and the evaluation of vasculature of nasal polyp
(CD34+ cells) to assess the inflammatory infiltrate of
nasal polyps.
Materials and methods
Patients and samples
Fragments of the polyps removed from 127 patients
with CRSwNP who underwent surgery at the Otorhinolaryngology Clinic
of Clinical County Emergency Hospital of Craiova, Romania, between
January and July, 2018 were histologically analyzed. We used the
histologically normal areas of the extracted surgical piece as a
control normal mucosa. The access of the database with patient
demographic and clinical electronic records for the purpose of this
study was approved by the Ethics Committee of Clinical County
Emergency Hospital of Craiova, Romania. As we are a teaching
hospital, all patients admitted to our hospital signed a written
consent by which they agreed that their medical data could be used
in scientific studies.
In order for patients to be included in this study,
compliance to certain criteria was necessary, including the
following: i) A symptomatology that lasted for >12 weeks,
without complete resolution: Nasal obstruction, muco-purulent nasal
discharge, hyposmia or anosmia, headaches with exacerbations
secondary to bacterial infections. ii) Different changes in the
region of the middle meatus, such as edema or polyps, observed upon
the endoscopic examination of nasal cavities.
The biological material was surgically obtained,
under general anesthesia, and analyzed at the Laboratory of
Pathology, Emergency County Hospital, Craiova, Romania. The tissues
were fixed in 10% buffered formalin, for 24 h. For
histopathological analysis, the sections were then embedded in
paraffin and stained with hematoxylin and eosin (H&E; Sanimed
SA, Bucharest, Romania). Serial sections (3-4-µm-thick) were cut
from paraffin blocks (automated rotating microtome Leica RM2255),
and placed on lamellas treated with poly-L-Lysine (Sigma-Aldrich,
Munich, Germany) and allowed to dry at laboratory temperature for
12 h. At room temperature, the slides were treated with Mayer
hematoxylin for 3 min, washed, differentiated for 10 sec in
alcohol-hydrochloric acid solution, washed again, stained with
eosin solution for 15 sec, dehydrated in 3 baths of alcohol (60
degrees, 96 degrees and finally absolute alcohol) and clarified in
3 toluene baths. Finally the slides were mounted using Canada balm
(Sigma-Aldrich).
Immunohistochemistry
For immunohistochemistry, the paraffin sections with
the same thickness as mentioned above (3–4 µm) were attached on to
electrostatically treated slides, deparaffinized in xylene at 58°C
for 1 h, then 2 more times for 10 min at room temperature, fixed in
cold acetone (4°C) for 5 min and then let to air-dry at room
temperature for 30 min. Immunohistochemistry was carried out using
soluble labeled streptavidin biotin (LSAB)/horseradish peroxidase
(HRP) complexes. Streptavidin is an avidin tetrameric analog with a
60-kDa molecular weight, extracted from Streptomyces
avidinii bacterium, able to bind easier to the molecules of
biotin. The affinity of streptavidin for biotin is 10-fold greater,
which leads to an intense specific detection and amplification of
antigen-antibody links. We used the Dako LSAB 2 System HRP kit
(Universal DAKO Labeled Streptavidin Biotin 2 System Horseradish
Peroxidase), as previously described (37). The sections were incubated in
peroxidase blocking solution (hydrogen peroxide 3%) for 10 min at
room temperature and rinsed with phosphate-buffered saline (PBS).
The slides were pre-treated in order to reveal the antigen by
microwaves and were incubated in a wet room contact with primary
antibody for about 1 hour at room temperature. goat anti-rabbit IgG
(h+l) secondary antibody (cat. no. 31820; Thermo Fisher Scientific,
San Frascisco, CA, USA) was added and the slides were incubated at
room temperature for 30 min. After washing in clean water, the
slides were incubated with streptavidin peroxidase at room
temperature for 10 min. The chromogen-substrate
[3,3′-diaminobenzidine (DAB)] was added in a dark room and once the
brown color appeared, the slides were submerged in water for
stopping and then stained with hematoxylin for 3 min. The slides
were dehydrated through 95% ethanol for 2 min and 2 times in 100%
ethanol for 3 min. Finally, the sections were mounted in Canada
balm (cat. no. C1795; Sigma-Aldrich).
In the immunohistochemical analysis, we used
concentrated antibodies from Thermo Fisher Scientific as follows:
CD20 mouse IgG monoclonal antibody (HI47), PE (cat. no.
MHCD2004-4), CD3 mouse IgG monoclonal antibody (S4.1) (cat. no.
Q10484), CD45 mouse IgG monoclonal antibody (HI30), pacific orange
(cat. no. MHCD4530TR) and CD34 mouse IgG monoclonal antibody
(BI-3C5) (cat. no. 07-3403). In order to obtain optimal dilution,
the antibodies were weak in the PBS-azide solution.
The immunohistochemical staining visualized the
investigated antigens using DAB chromogen, which caused a brown
precipitate (cell nucleus was stained light blue by hematoxylin).
Immunohistochemical staining was evaluated by a 4-grade system,
according to the model established by the European Organization for
Research and Treatment of Cancer-Gynaecological Cancer Cooperative
Group in 1997 (38), as follows:
Absent (−), weak intensity (+), moderate intensity (++) and strong
immunostaining (+++). After immunostaining was carried out, we
assessed the number of cells per 20X field by examining 20 fields
for each slide. The results were expressed as cells/field.
Statistical analysis
All numerical data are expressed as the median
(interquartile range). For sex data, we used the one-sample Z-test
to determine whether the proportion of males differed significantly
from 50% for each age group (in other words if there was a
significant difference between the proportion of males and
females). For count data we used 2×2 or 2×3 Chi-squared tests. To
determine differences between multiple groups, we used the
non-parametric Wilcoxon test, as some distribution data were skewed
and we had a low number of hyperplastic polyps, followed by the
post-hoc Mann-Whitney test with the Holm-Sidak adjustment for
multiple comparisons. The statistical significance level was set at
0.05.
Results
Demographic data
There were no significant differences in sex
distribution among patients in the specific age groups with the
exception of the 11–20-year age category, which exhibited a
significantly higher precedence of males (male:female ratio,
2.07:1; Table I).
 | Table I.Age and sex distribution of patients
with nasal polyposis. |
Table I.
Age and sex distribution of patients
with nasal polyposis.
| Age | Male | Female | Male:female
ratio | Total, n (%) | P-value |
|---|
| 0–10 years | 3 | 3 | 1.00:1 | 6 (4.72) | 0.999 |
| 11–20 years | 31 | 15 | 2.07:1 | 46 (36.22) | 0.018 |
| 21–30 years | 13 | 11 | 1.18:1 | 24 (18.90) | 0.683 |
| 31–40 years | 12 | 5 | 2.40:1 | 17 (13.38) | 0.089 |
| 41–50 years | 9 | 5 | 1.80:1 | 14 (11.02) | 0.2849 |
| 51–60 years | 13 | 7 | 1.86:1 | 20 (15.75) | 0.180 |
| Total | 81 | 46 | 1.76:1 | 127 | <0.001 |
Histopathological changes
We classified the histopathological changes of the
nasal polyps according to the Davidsson and Hellquist
classification (39). We examined
127 nasal polyps that were classified as follows: Allergic polyps
(with eosinophilic infiltrate), 69 cases (54.33%); fibro
inflammatory polyps, 47 cases (37.01%); and hyperplastic polyps
with marked hyperplasia of the seromucous glands, 11 cases (8.67%).
The allergic and fibro-inflammatory polyps were mostly ulcerated,
whereas the hyperplastic polyps were mostly non-ulcerated (Table II).
| Table II.The pathological types and nature of
the surface epithelium in nasal polyps. |
Table II.
The pathological types and nature of
the surface epithelium in nasal polyps.
|
| Ulceration | Histological
type |
|---|
|
|
|
|
|---|
| Histological
type | Non-ulcerated
(n=11) | Ulcerated
(n=116) | P-value | Pseudostratified
ciliated columnar epithelium (n=108) | Squamous epithelium
(n=12) | Transitional
epithelium (n=7) | P-value | Pseudostratified
vs. squamous | Pseudostratified
vs. transitional | Squamous vs.
transitional |
|---|
| Allergic polyps
(n=69) | 3 (4.35%) | 66 (95.65%) | 0.059 | 58 (84.06%) | 8 (11.59%) | 3 (4.35%) | <0.001 | 0.007 | 0.003 | 0.042 |
| Fibro-inflammatory
polyps (n=47) | 0 (0%) | 47 (100%) | 0.008 | 43 (91.48%) | 2 (4.26%) | 2 (4.26%) | <0.001 | 0.007 | 0.007 | 0.539 |
| Hyperplastic polyps
(n=11) | 8 (72.73%) | 3 (26.27%) | <0.001 | 7 (63.64%) | 2 (18.18%) | 2 (18.18%) | 0.025 | 0.035 | 0.035 | 0.539 |
We observed the following histopathological changes:
The structure of the epithelium was evidenced by collagenous
subjacent stroma with mixed areas, sometimes associated with
hyaline zones. The pseudostratified columnar epithelium
predominated in all types of polyps, but was more frequent in
fibro-inflammatory polyps (91.48%). In all types of polyps, we also
observed a diffuse underlayer or periglandular lymphoplasmacytic
infiltrate composed predominantly from T lymphocytes and
eosinophils. The histopathological changes suggest the chronic
inflammation of the sinus mucosa, diffusely distributed in allergic
polyps and with nodular distribution in fibro-inflammatory
polyps.
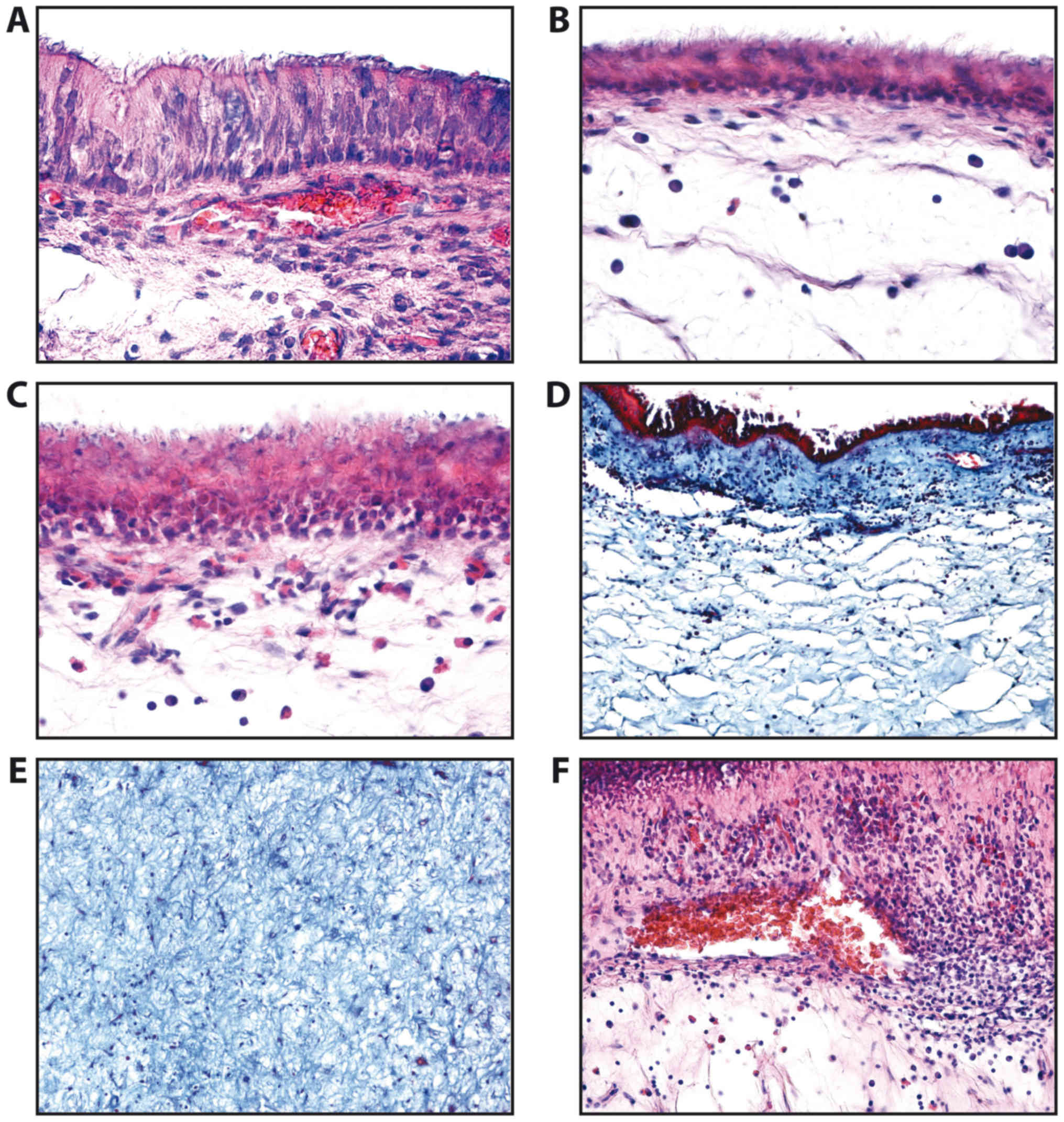
In this study, we identified normal epithelium
composed of tall cells (Fig. 1A),
atrophic epithelium (Fig. 1B),
squamous metaplasia of the epithelium (Fig. 1C) with the chorion moderately
infiltrated with lymphocytes, plasma cells and sometimes
eosinophils. The lamina propria and stromal polyp appeared in many
fibrous and spongy areas (Fig. 1D and
E). Areas with vascular congestion and abundant inflammatory
infiltrate were also detected (Fig.
1F). The basal membrane often appeared thickened.
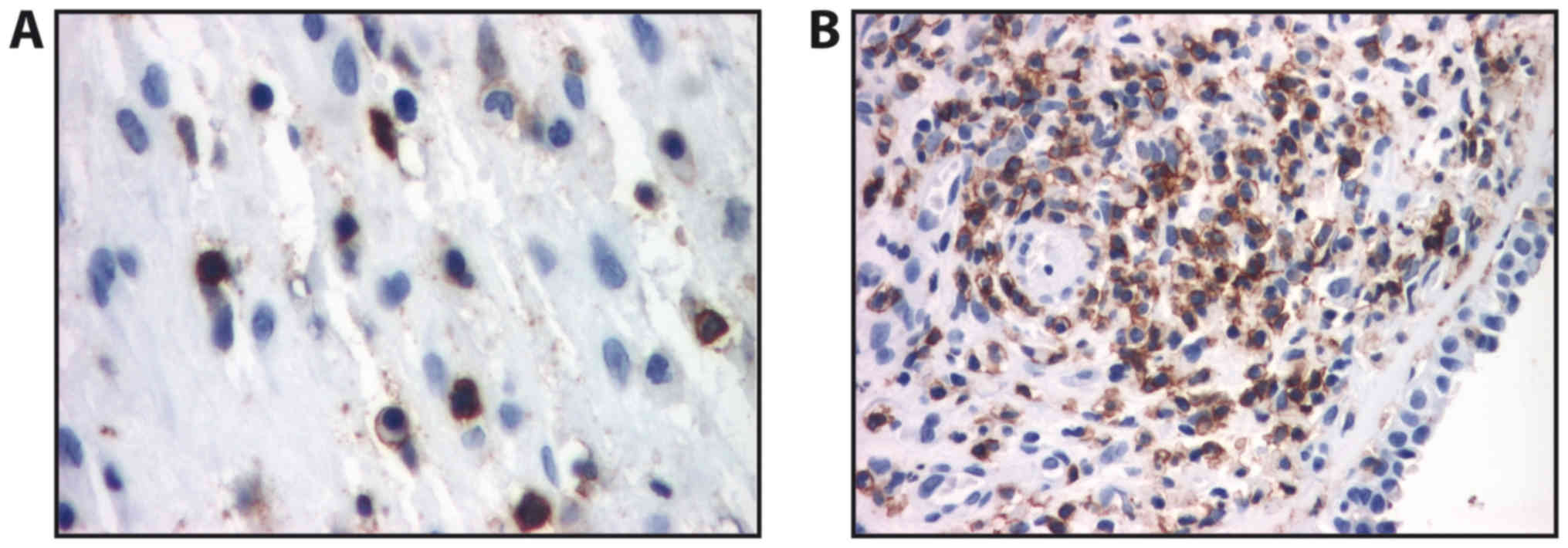
Analysis of immunostaining
In allergic polyps, immunostaining for CD45RO
revealed a diffuse localization of activated and memory T
lymphocytes, which presented distinct immunostaining at the cell
membrane (Fig. 2A). In
fibro-inflammatory polyps, CD45RO staining revealed numerous
activated T lymphocytes with distinct immunostaining at the
membrane level; however, we also observed an underlayer with mostly
periglandular arrangement. In some cases, the infiltrate formed
lymphoid follicles (Fig. 2B). The
activated and memory T lymphocytes (CD45RO+) were most
abundant in allergic polyps followed by fibro-inflammatory polyps
and hyperplastic polyps (Table
III), the differences between the immunostaining level between
the polyp types were all significant (P<0.05).
| Table III.Distribution of eosinophils, T
lymphocytes (CD3+), B lymphocytes (CD20+),
CD34+ cells and CD34+ vessels in different
types of polyps. |
Table III.
Distribution of eosinophils, T
lymphocytes (CD3+), B lymphocytes (CD20+),
CD34+ cells and CD34+ vessels in different
types of polyps.
|
| Allergic polyps
(n=69) | Fibro-inflammatory
polyps (n=47) | Hyperplastic polyps
(n=11) | Group
difference | Allergic vs.
fibro-inflammatory | Allergic vs.
hyperplastic | Fibro-inflammatory
vs. hyperplastic |
|---|
|
|
|
|
|
|
|
|
|
|---|
| Parameter | Median (IQR) | Median (IQR) | Median (IQR) | P-value | P-value | P-value | P-value |
|---|
| Eosinophils | 128.3 | 3.4 | 0 | <0.001 | <0.001 | <0.001 | 0.007 |
| (cells/20X
field) | (81.5–181.6) | (0.64–8.2) | (0–0.4) |
|
|
|
|
| T lymphocytes
(CD3+) | 28.9 | 61.7 | 55.7 | <0.001 | <0.001 | <0.001 | 0.580 |
| (cells/20X
field) | (28.5–71.9) | (35.2–112.8) | (38.1–65.4) |
|
|
|
|
| Activated and
memory | 19.4 | 14.3 | 12.5 | <0.001 | <0.001 | <0.001 | 0.009 |
|
(CD45RO+) | (14.3–22.7) | (12.1–15.7) | (10.5–15.4) |
|
|
|
|
| T lymphocytes |
|
|
|
|
|
|
|
| (cells/20X
field) |
|
|
|
|
|
|
|
| B lymphocytes
(CD20+) | 12.9 | 33.4 | 22.3 | <0.001 | <0.001 | <0.001 | 0.054 |
| (cells/20X
field) | (10.5–23.4) | (14.7–38.2) | (12.5–33.1) |
|
|
|
|
| CD34+
cells/20X field | 14.3 | 42.7 | 28.2 | <0.001 | <0.001 | <0.001 | <0.001 |
|
| (12.1–17.8) | (36.5–48.9) | (24.1–30.5) |
|
|
|
|
| CD34+
vessels/0.5 mm2 | 60.3 | 190.3 | 127.1 | <0.001 | <0.001 | <0.001 | <0.001 |
|
| (55.8–62.4) | (170.7–211.9) | (117.1–132.5) |
|
|
|
|
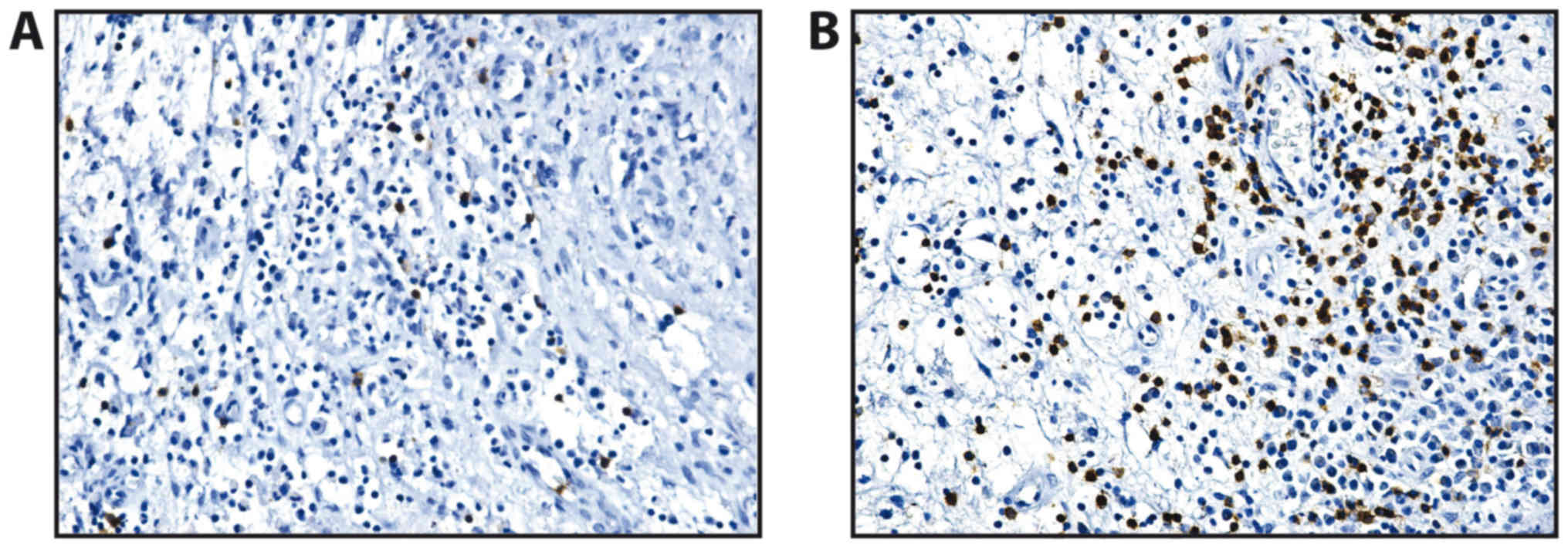
Anti-CD20 monoclonal antibody underlined a
continuous mark for B lymphocytes at the membrane level. In all the
polyps, the B lymphocytes were much less represented compared with
the population of T lymphocytes, that were diffusely present in the
polyp stroma (Fig. 3). We observed
an increase in the numbers of B lymphocytes in the
fibro-inflammatory polyps (Table
III).
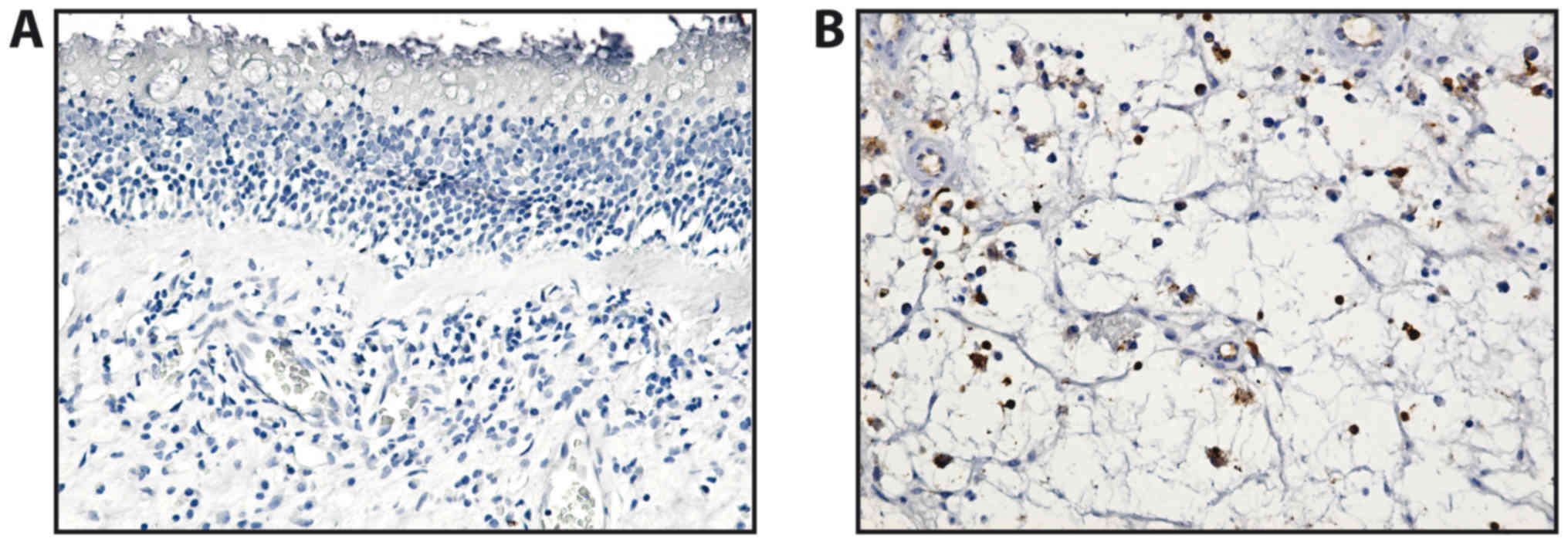
The T lymphocytes (CD3+) were barely
present in the lamina propria of the mucosal polyp and in the deep
stroma (Fig. 4). In the allergic
polyps, CD3 immunostaining revealed that the T lymphocytes
exhibited a diffuse distribution in the stroma of the analyzed
polyps. In general, T lymphocytes were much more numerous in the
fibro-inflammatory and hyperplastic polyps than in the allergic
ones (Table III).
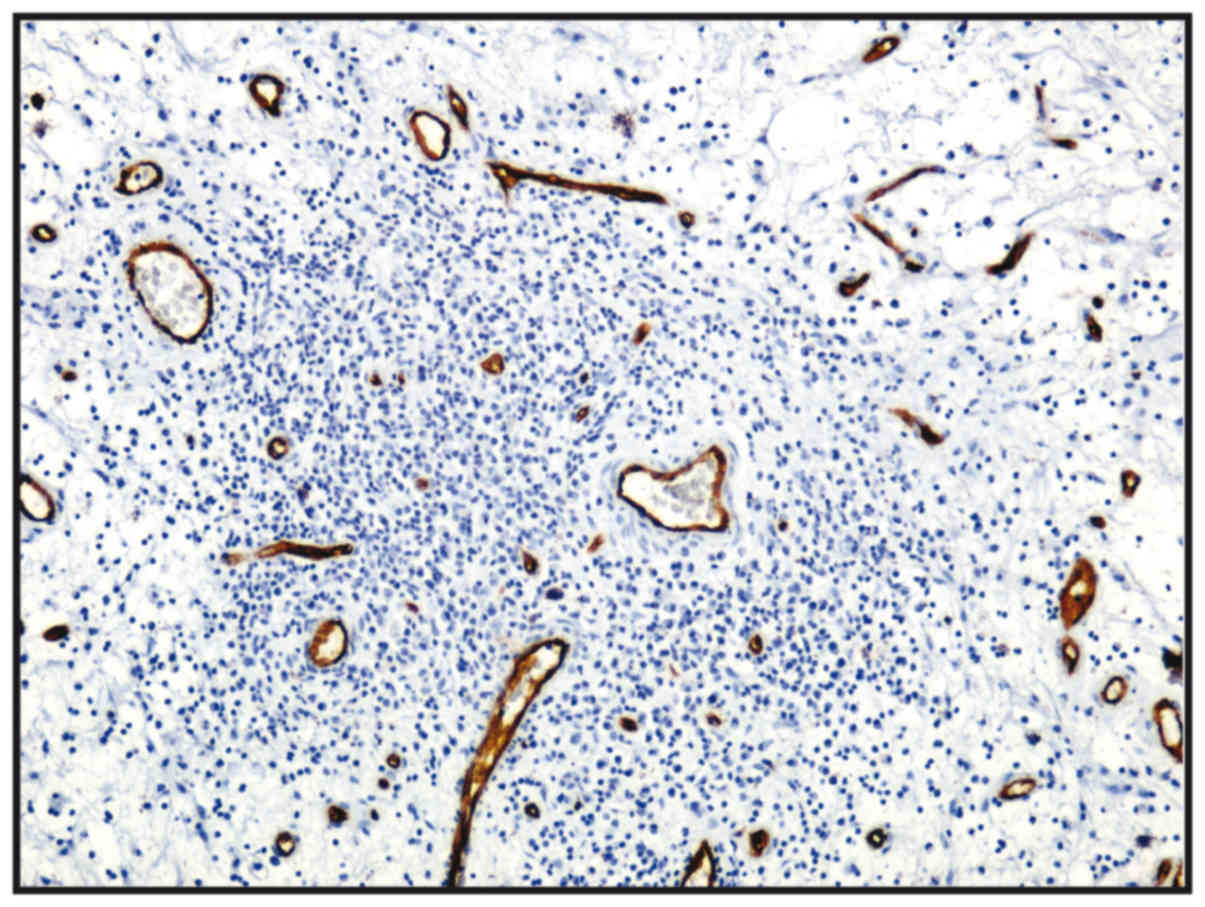
The microvasculature of all nasal polyps exhibited a
non-homogeneous distribution, with the most intensely vascular
areas being the areas of the lymphoid infiltration
(CD34+) (Table III
and Fig. 5).
Discussion
Although CRS is a common disease, commonly addressed
by the healthcare facilities, the pathology of the disease is
poorly understood and the therapeutic options are limited, which
results in a significant loss of the quality of life of the
affected patients and induces a substantial financial burden
(2,40). As regards the demographic data from
the present study, there was no significant difference between the
number of men and women with nasal polyps, as in other studies
(41), although the majority of
patients with nasal polyps were middle-aged, at around 40 years of
age. In this study, most polyps were from patients aged 11–20
years, as many parents turned to the hospital otorhinolaryngology
specialists for polypectomy. The higher male:female ratio in the
11–20 year old age group detected in this study is well in
accordance with that of another study (42). In addition, Vento et al
(43) identified a male:female
ratio of 2.4:1 and Diamantopoulos et al (44) determined a male:female ratio of
3.3:1.
The majority of nasal polyps that were resected were
of the allergic type (69 polyps), then of the fibro-inflammatory
type secondary to infection or other causes (47 polyps). In
addition, 11 polyps were classified as hyperplastic.
The histopathological findings of this study
revealed that ulceration was present in a high percentage of the
allergic and fibro-inflammatory polyps. A previous study on
African, Chinese and Caucasian populations demonstrated that 10–20%
of hyperplastic polyps were ulcerated as opposed to 75% of
fibro-inflammatory and allergic polyps (45). The study by Lathi et al that
included 112 Indian patients found that 62.5% from the polyps were
of the allergic type and 25% of the fibro-inflammatory type, that
is similar with our percentages of 54.33, 37.01 and 8.67%,
respectively (46). The high
percentage of ulceration may be due to trauma or mechanical
pressure of growing polyps inside nasal cavities.
In a separate study by Tripathi and Ranjan (47) performed on 119 polyp biopsies in
the pathology laboratory, it was shown that 79.1% of the polyps had
pseudostratified ciliated columnar epithelium, 18.8% had squamous
epithelium and 2.1% transitional epithelium. These findings were
confirmed in this study, which identified a pseudostratified
ciliated columnar epithelium in 84.06% of the allergic polyps,
whereas the squamous epithelium and transitional epithelium were
identified in 11.59 and 4.35% of the cases, respectively in these
polyp types. Moreover, in all types of polyps, significant
differences between the types of epithelium were detected in our
study in hyperplastic polyps (P=0.025) and highly significant
differences in allergic and fibroinflammatory polyps
(P<0.001).
The most important factors in the pathogenesis of
CRS are identified as both the chronic activation of a variety of
inflammatory cells such as B cells, a key component of the adaptive
immune response, as well as the defects in innate immunity
(19,48). A number of studies have focused on
B and T lymphocyte expression, as well as on the inflammatory
infiltrate in patients with CRS with or without nasal polyposis.
Thus, it has been noted that the number of CD3+ cells,
CD20+ cells and plasma cells in nasal polyps are
significantly higher compared to those in the middle turbinates
(49). The inflammatory infiltrate
and cell proliferation are associated with the presentation of
nasal polyps (50). It has been
observed that in patients with nasal polyposis associated with
cystic fibrosis, there is an increase in the number and activation
state of T lymphocytes and an increase in the number of plasma
cells. Furthermore, in nasal polyps, increased levels of
eosinophils, eosinophil cationic protein (ECP) and eotaxin compared
with CRS and controls were determined. Patients with CRS present
with Th1 polarization and an increase in IFN-γ and TGF-β levels,
with nasal polyps showing Th2 polarization/high IL-5 and IgE
(51).
In the study by Hulse et al (52), there was no significant difference
between the median number of CD20+ cells per high-power
field (hpf) in CRS tissues as compared with the controls. However,
we must take into account the known difficulty of measuring protein
expression by immunohistochemistry. A much better method for the
quantitative characterization of B cell populations is flow
cytometry. The utilization of this method has demonstrated a
significantly higher number of CD19+ B cells in CRSwNP
compared with healthy control subjects or CRSsNP patients (53).
The polyps present higher levels of BAFF that
correlates with an increased expression of CD20 (54), leading to the conclusion that B
lymphocytes found in polyp tissue favor a microenvironment for
activation, proliferation and differentiation (55). Furthermore, decreased apoptosis in
polyps from aspirin-sensitive patients and the eosinophilic
infiltration has been linked to an increased expression of
CD45RO+ activated/memory cells and to the clinical
features of the rhinosinusitis has been demonstrated (56). The number of CD45-positive cells is
higher in patients with CRSwNP compared to those with CRSsNP
(P<0.01). The number of CD45+ cells in nasal polyps
has been shown to increase >2-fold the total number of cells
(57).
In this study, in all types of polyps, continuous
marking for B lymphocytes at the membrane level was detected. The
underlayer or periglandular lymphoplasmacytic infiltrate was
composed predominantly from T lymphocytes and eosinophils with
diffuse disposition at the stroma level, as revealed by CD45 and
CD3 immunostaining.
The distribution of the microvasculature had a
nonhomogeneous distribution in nasal polyps as the most intensely
vascular area were lymphoid infiltration areas (CD34+).
The histopathological changes suggest the chronic inflammation of
sinus mucosa, diffusely distributed in allergic polyps and with
nodular distribution in fibro-inflammatory polyps. The number of B
lymphocytes was slightly greater in the fibro-inflammatory
polyps.
In conclusion, the findings of the present study
demonstrate that the inflammatory infiltrate in nasal polyps is
composed mainly from T cells and eosinophils in all types of
polyposis. We observed a diffuse distribution in the allergic
polyps and nodular distribution in the fibro-inflammatory polyps,
and also a hyperplasia of the seromucous glands. The number of B
lymphocytes was slightly increased in the fibro-inflammatory
polyps. Further studies are required in order to fully understand
the pathology of CRS and to find novel therapeutic options.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the current
study are included in this published article or are available from
the corresponding author upon reasonable request.
Authors' contributions
All the authors were involved in conceiving and
designing the study. MM, AC and GMu contributed to sample
collection. MM, DA, AC and GMi collected the data. OZ, GMi
performed the statistical analysis. DC, AOD, GT and OZ drafted and
wrote the manuscript. DC, AOD, DAS, GT and AMT gave advice on the
experimental design, interpreted the results and critically revised
the manuscript. All authors have read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
The access of the database for the purpose of this
study was approved by the Ethics Committee of Clinical County
Emergency Hospital of Craiova, Romania. As we are a teaching
hospital, all patients admitted to our hospital signed a written
consent by which they agree that their medical data can be used in
scientific studies.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this
article.
References
|
1
|
Jankowski R, Rumeau C, Gallet P and Nguyen
DT: Nasal polyposis (or chronic olfactory rhinitis). Eur Ann
Otorhinolaryngol Head Neck Dis. 135:191–196. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Khairuddin NK, Salina H, Gendeh BS, Wan
Hamizan AK and Lund VJ: Quality of life and recurrence of disease
in patients with eosinophilic and non-eosinophilic 1 chronic
rhinosinusitis with nasal polyposis. Med J Malaysia. 73:1–6.
2018.PubMed/NCBI
|
|
3
|
Fokkens WJ, Lund VJ, Mullol J, Bachert C,
Alobid I, Baroody F, Cohen N, Cervin A, Douglas R, Gevaert P, et
al: EPOS 2012: European position paper on rhinosinusitis and nasal
polyps 2012. A summary for otorhinolaryngologists. Rhinology.
50:1–12. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stevens WW, Schleimer RP, Chandra RK and
Peters AT: Biology of nasal polyposis. J Allergy Clin Immunol.
133:1503–1503.e1. 4–2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ungureanu A, Zlatian O, Mitroi G, Drocaş
A, Ţîrcă T, Călina D, Dehelean C, Docea AO, Izotov BN, Rakitskii
VN, et al: Staphylococcus aureus colonisation in patients from a
primary regional hospital. Mol Med Rep. 16:8771–8780. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Calina D, Rosu L, Rosu AF, Ianosi G,
Ianosi S, Zlatian O, Mitrut R, Docea AO, Rogoveanu O and Mitrut P:
Etiological diagnosis and pharmacotherapeutic management of
parapneumonic pleurisy. Farmacia. 64:946–952. 2016.
|
|
7
|
Călina D, Docea AO, Rosu L, Zlatian O,
Rosu AF, Anghelina F, Rogoveanu O, Arsene AL, Nicolae AC, Drăgoi
CM, et al: Antimicrobial resistance development following surgical
site infections. Mol Med Rep. 15:681–688. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zlatian O, Balasoiu AT, Balasoiu M,
Cristea O, Docea AO, Mitrut R, Spandidos DA, Tsatsakis AM, Bancescu
G and Calina D: Antimicrobial resistance in bacterial pathogens
among hospitalised patients with severe invasive infections. Exp
Ther Med. 16:4499–4510. 2018.PubMed/NCBI
|
|
9
|
Dennis SK, Lam K and Luong A: A Review of
classification schemes for chronic rhinosinusitis with nasal
polyposis endotypes. Laryngoscope Investig Otolaryngol. 1:130–134.
2016. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zaravinos A, Bizakis J, Soufla G,
Sourvinos G and Spandidos DA: Mutations and differential expression
of the ras family genes in human nasal polyposis. Int J Oncol.
31:1051–1059. 2007.PubMed/NCBI
|
|
11
|
Zaravinos A, Bizakis J and Spandidos DA:
RKIP and BRAF aberrations in human nasal polyps and the adjacent
turbinate mucosae. Cancer Lett. 264:288–298. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zaravinos A, Soufla G, Bizakis J and
Spandidos DA: Expression analysis of VEGFA, FGF2, TGFbeta1, EGF and
IGF1 in human nasal polyposis. Oncol Rep. 19:385–391.
2008.PubMed/NCBI
|
|
13
|
Zaravinos A, Bizakis J and Spandidos DA:
Prevalence of human papilloma virus and human herpes virus types
1–7 in human nasal polyposis. J Med Virol. 81:1613–1619. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gitomer SA, Fountain CR, Kingdom TT, Getz
AE, Sillau SH, Katial RK and Ramakrishnan VR: Clinical examination
of tissue eosinophilia in patients with chronic rhinosinusitis and
nasal polyposis. Otolaryngol Head Neck Surg. 155:173–178. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Koennecke M, Pries R and Wollenberg B:
Regulatory dysfunctions in nasal polyposis. HNO. 66:290–295.
2018.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ickrath P, Kleinsasser N, Ding X, Ginzkey
C, Beyersdorf N, Kerkau T, Hagen R and Hackenberg S: Impact and
modulations of peripheral and edaphic B cell subpopulations in
chronic rhinosinusitis with nasal polyposis. Clin Exp
Otorhinolaryngol. 11:133–140. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wongratanacheewin S: Significant role of
cytokines and signaling pathway in rheumatoid arthritis, nasal
polyposis and human airway smooth muscle cells. Asian Pac J Allergy
Immunol. 31:1–2. 2013.PubMed/NCBI
|
|
18
|
Chin D and Harvey RJ: Nasal polyposis: An
inflammatory condition requiring effective anti-inflammatory
treatment. Curr Opin Otolaryngol Head Neck Surg. 21:23–30. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tan BK, Peters AT, Schleimer RP and Hulse
KE: Pathogenic and protective roles of B cells and antibodies in
patients with chronic rhinosinusitis. J Allergy Clin Immunol.
141:1553–1560. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen JB, James LK, Davies AM, Wu YB,
Rimmer J, Lund VJ, Chen JH, McDonnell JM, Chan YC, Hutchins GH, et
al: Antibodies and superantibodies in patients with chronic
rhinosinusitis with nasal polyps. J Allergy Clin Immunol.
139:1195–1204 e1111. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pratt E, Collins AM, Sewell WA and Harvey
RJ: Antigen selection in IgE antibodies from individuals with
chronic rhinosinusitis with nasal polyps. Am J Rhinol Allergy.
24:416–421. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gonçalves C, Pinaffi JV, Carvalho JF,
Pinna FR, Constantino GT, Voegels RL, Bueno C, Bonfá E and Viana
VS: Antineutrophil cytoplasmic antibodies in chronic rhinosinusitis
may be a marker of undisclosed vasculitis. Am J Rhinol. 21:691–694.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Brewington JJ, Filbrandt ET, LaRosa FJ
III, Moncivaiz JD, Ostmann AJ, Strecker LM and Clancy JP: Brushed
nasal epithelial cells are a surrogate for bronchial epithelial
CFTR studies. JCI Insight. 3:32018. View Article : Google Scholar
|
|
24
|
Bridges MA: Culture of airway epithelial
cells collected by a nasal brushing technique. In Vitro Cell Dev
Biol Anim. 33:82–83. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bradding P, Mediwake R, Feather IH, Madden
J, Church MK, Holgate ST and Howarth PH: TNF alpha is localized to
nasal mucosal mast cells and is released in acute allergic
rhinitis. Clin Exp Allergy. 25:406–415. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Boita M, Bucca C, Riva G, Heffler E and
Rolla G: Release of type 2 cytokines by epithelial cells of nasal
polyps. J Immunol Res. 2016:26432972016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jacobi HH, Liang Y, Tingsgaard PK, Larsen
PL, Poulsen LK, Skov PS, Haak-Frendscho M, Niles AL and Johansson
O: Dendritic mast cells in the human nasal mucosa. Lab Invest.
78:1179–1184. 1998.PubMed/NCBI
|
|
28
|
Rheinländer A, Schraven B and Bommhardt U:
CD45 in human physiology and clinical medicine. Immunol Lett.
196:22–32. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Casan JM, Wong J, Northcott MJ and Opat S:
Anti-CD20 monoclonal antibodies: Reviewing a revolution. Hum Vaccin
Immunother. Aug 10–2018.(Epub ahead of print). doi:
10.1080/21645515.2018.1508624. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
No authors listed, . Abstracts of The
International Symposium of Recent Update in Rhinosinusitis and
Nasal Polyposis. Med J Malaysia. 71 (Suppl 2):1–35. 2016.
|
|
31
|
Moro K, Yamada T, Tanabe M, Takeuchi T,
Ikawa T, Kawamoto H, Furusawa J, Ohtani M, Fujii H and Koyasu S:
Innate production of T(H)2 cytokines by adipose tissue-associated
c-Kit(+)Sca-1(+) lymphoid cells. Nature. 463:540–544. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Halim TY, Krauss RH, Sun AC and Takei F:
Lung natural helper cells are a critical source of Th2 cell-type
cytokines in protease allergen-induced airway inflammation.
Immunity. 36:451–463. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yasuda K, Muto T, Kawagoe T, Matsumoto M,
Sasaki Y, Matsushita K, Taki Y, Futatsugi-Yumikura S, Tsutsui H,
Ishii KJ, et al: Contribution of IL-33-activated type II innate
lymphoid cells to pulmonary eosinophilia in intestinal
nematode-infected mice. Proc Natl Acad Sci USA. 109:3451–3456.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kang SH, Dalcin PT, Piltcher OB and
Migliavacca RO: Chronic rhinosinusitis and nasal polyposis in
cystic fibrosis: Update on diagnosis and treatment. J Bras Pneumol.
41:65–76. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bachert C, Zhang L and Gevaert P: Current
and future treatment options for adult chronic rhinosinusitis:
Focus on nasal polyposis. J Allergy Clin Immunol. 136:1431–1440.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Csomor P, Sziklai I and Karosi T: Effects
of intranasal steroid treatment on the presence of biofilms in
non-allergic patients with chronic rhinosinusitis with nasal
polyposis. Eur Arch Otorhinolaryngol. 271:1057–1065. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mitroi M, Căpitănescu A, Georgescu CV,
Mogoantă CA, Popescu C, Georgescu M, Mitroi G and Ioniţă E:
Expression pattern of CK7 and CK20 in nasal polyps, at patients
with chronic rhinosinusitis with nasal polyposis. Rom J Morphol
Embryol. 52 (Suppl 3):1051–1057. 2011.PubMed/NCBI
|
|
38
|
van Diest PJ, van Dam P, Henzen-Logmans
SC, Berns E, van der Burg ME, Green J and Vergote I; European
Organization for Research and Treatment of Cancer-Gynaecological
Cancer Cooperative Group, : A scoring system for
immunohistochemical staining: Consensus report of the task force
for basic research of the EORTC-GCCG. J Clin Pathol. 50:801–804.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Davidsson A and Hellquist HB: The
so-called ‘allergic’ nasal polyp. ORL J Otorhinolaryngol Relat
Spec. 55:30–35. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Aboud SK, Husain S and Gendeh BS:
Evaluation on quality of life in patients with nasal polyposis
managed with optimal medical therapy. Allergy Rhinol (Providence).
5:2–8. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Cortesina G, Cardarelli L, Riontino E,
Majore L, Ragona R and Bussi M: Multi-center study of recurrent
nasal sinus polyposis: Prognostic factors and possibility of
prophylaxis. Acta Otorhinolaryngol Ital. 19:315–324. 1999.(In
Italian). PubMed/NCBI
|
|
42
|
Settipane GA: Epidemiology of nasal
polyps. Allergy Asthma Proc. 17:231–236. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Vento SI, Wolff CH, Salven PJ, Hytönen ML,
Ertama LO and Malmberg CH: Vascular permeability factor/vascular
endothelial growth factor in nasal polyps. Acta Otolaryngol Suppl.
543:170–174. 2000.PubMed/NCBI
|
|
44
|
Diamantopoulos II, Jones NS and Lowe J:
All nasal polyps need histological examination: An audit-based
appraisal of clinical practice. J Laryngol Otol. 114:755–759. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lacroix JS, Zheng CG, Goytom SH, Landis B,
Szalay-Quinodoz I and Malis DD: Histological comparison of nasal
polyposis in black African, Chinese and Caucasian patients.
Rhinology. 40:118–121. 2002.PubMed/NCBI
|
|
46
|
Lathi A, Syed MM, Kalakoti P, Qutub D and
Kishve SP: Clinico-pathological profile of sinonasal masses: A
study from a tertiary care hospital of India. Acta Otorhinolaryngol
Ital. 31:372–377. 2011.PubMed/NCBI
|
|
47
|
Tripathi P and Ranjan R: A comparative
study of histopathology of different types of nasal polyps:
Allergic, inflammatory and neoplastic. Ann Int Med Dent Res.
3:41–45. 2017.
|
|
48
|
Takeda K, Sakakibara S, Yamashita K,
Motooka D, Nakamura S, El Hussien MA, Katayama J, Maeda Y, Nakata
M, Hamada S, et al: Allergic conversion of protective mucosal
immunity against nasal bacteria in patients with chronic
rhinosinusitis with nasal polyposis. J Allergy Clin Immunol. Jul
25–2018.(Epub ahead of print). doi: 10.1016/j.jaci.2018.07.006.
|
|
49
|
Wang X, Guo J, Zhang H, Tao G, Han D, Zhu
X, Fan E and Li Y: Roles of CD43, CD20 and local IgE in the
pathogenesis of nasal polyps. Zhonghua Er Bi Yan Hou Ke Za Zhi.
36:333–334. 2001.(In Chinese). PubMed/NCBI
|
|
50
|
Wu X, Wang LF and Zang YH: Expression of
CD68 CD45RO CD20 and proliferating cell nuclear antigen in nasal
polyps. Zhonghua Er Bi Yan Hou Ke Za Zhi. 38:187–190. 2003.(In
Chinese). PubMed/NCBI
|
|
51
|
Sobol SE, Christodoulopoulos P, Manoukian
JJ, Hauber HP, Frenkiel S, Desrosiers M, Fukakusa M, Schloss MD and
Hamid Q: Cytokine profile of chronic sinusitis in patients with
cystic fibrosis. Arch Otolaryngol Head Neck Surg. 128:1295–1298.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Hulse KE, Norton JE, Suh L, Zhong Q,
Mahdavinia M, Simon P, Kern RC, Conley DB, Chandra RK, Tan BK, et
al: Chronic rhinosinusitis with nasal polyps is characterized by
B-cell inflammation and EBV-induced protein 2 expression. J Allergy
Clin Immunol. 131:1075–83, 1083.e1-7. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Min JY, Hulse KE and Tan BK: B-cells and
antibody-mediated pathogenesis in chronic rhinosinusitis with nasal
polyps. Adv Otorhinolaryngol. 79:48–57. 2016.PubMed/NCBI
|
|
54
|
Yoon YH, Jin J, Kwon KR, Kim SH, Rha KS
and Kim YM: The role of B cell Activating Factor (BAFF) expression
on pathogenesis of nasal polyp in chronic rhinosinusitis with nasal
polyposis. Rhinology. 52:390–396. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Hulse KE: Immune mechanisms of chronic
rhinosinusitis. Curr Allergy Asthma Rep. 16:12016. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Chen D, Chen L and Xiao L: The progress
study of tumor suppressor gene and apoptosis gene in nasal polyps.
Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 29:2099–2102.
2015.(In Chinese). PubMed/NCBI
|
|
57
|
Kowalski ML, Grzegorczyk J, Pawliczak R,
Kornatowski T, Wagrowska-Danilewicz M and Danilewicz M: Decreased
apoptosis and distinct profile of infiltrating cells in the nasal
polyps of patients with aspirin hypersensitivity. Allergy.
57:493–500. 2002. View Article : Google Scholar : PubMed/NCBI
|