Introduction
Since the outbreak of coronavirus disease 2019
(COVID-19) in China (1), COVID-19
infection has spread worldwide, resulting in a pandemic. The
mortality rate of COVID-19 is, however, decreasing globally
(2–4). Although COVID-19 infection causes
systemic multi-organ damage, the main cause of death in COVID-19 is
considered to be acute respiratory failure due to alveolar
macrophage activation and inflammation (5). Patients with COVID-19 can be
classified into three types: mild, requiring no oxygen
administration; moderate, requiring oxygen administration; and
severe, requiring artificial respiration. It is estimated that
patients with severe disease-account for just under 10% of the
total number of cases of infection (2,6).
Therefore, it is extremely important to identify
risk factors for severe disease, so that those who are most likely
to develop severe disease can be treated with potent antiviral or
immunosuppressive therapies (3,7).
The risk factors for severe disease status reported to date include
advanced age, chronic obstructive pulmonary disease, diabetes,
dyslipidemia, hypertension, chronic kidney disease, malignancy,
obesity, smoking, and immunosuppression (8–11).
Furthermore, many studies have revealed that blood biomarkers,
including white blood cell (WBC) count, lymphocyte count, platelet
(Plt) count, albumin, aspartate aminotransferase (AST), alanine
aminotransferase (ALT), lactate dehydrogenase (LDH), C-reactive
protein (CRP), D-dimer, ferritin, interleukin-6, procalcitonin
(PCT) levels, and prothrombin time (PT) are closely related with
disease severity in patients with COVID-19 (12–25). We previously examined COVID-19
disease severity and specific biomarkers, and reported that these
markers, especially CRP, ferritin, PCT, albumin, and LDH are useful
for predicting the severity of the disease (26). We also showed that hemostatic
abnormalities are frequently observed in patients with severe
disease stage (26).
However, there is no clear blood biomarker that
predicts deterioration from non-severe to severe disease.
Therefore, we investigated the prognostic biomarkers of COVID-19
infection at certain time points and focused on identifying markers
that might be predictors of disease deterioration from among the
commonly available blood biomarkers. We believe such markers will
help improve prognosis by allowing earlier intervention.
Materials and methods
Subjects
The subjects of this retrospective observational
study were 255 patients who were admitted to Mie General Medical
Center between April 2019 and September 2021 with COVID-19
infection. A section of the patients in the present study were
evaluated in a previous study (26). Of the 255 patients, 54 patients
were excluded because of the need for oxygen administration due to
underlying diseases or an unknown clinical course due to their
early transfer to other hospitals. The diagnosis of COVID-19
infection was based on positive results of real-time PCR (RT-PCR)
or antigen quantification tests using nasopharyngeal swabs.
We classified patients into two groups: those who
need oxygen therapy at the time of admission as the severe group,
and those who did not need oxygen as the non-severe group. Each
group was further subdivided into an improved group and a
deteriorated group. The study endpoint was defined as exacerbation
before discharge from the hospital, defined as the appearance of
oxygen demand in the non-severe group, and conversion to a
high-flow system or death in the severe group.
Treatment
All treatments basically followed the best treatment
at the moment. Both, patients with suspected or confirmed mild
disease without evidence of hypoxia or pneumonia as well as
asymptomatic patients, were treated symptomatically. The antiviral
agent, favipiravir, remdesivir, was administered to patients with
pneumonia. In severe cases, general symptom management and
supportive care with standard thromboprophylaxis were performed,
and patients who continued to deteriorate despite standard oxygen
therapy were given advanced respiratory therapy, such as high-flow
therapy or artificial oxygen/ventilatory support. Systemic
corticosteroid therapy, an IL-6 inhibitor and/or a Janus kinase
(JAK) inhibitor, was used according to the patient's status
(3,4).
Methods
Basically, blood biomarkers were examined as early
as possible after admission in all the subjects. Biomarkers
included WBC count, neutrophil count, lymphocyte count, hemoglobin
(Hb), Plt count, AST, ALT, LDH, creatinine, CRP, PCT, KL-6,
Presepsin (PSP), and D-dimer. WBC count, Hb, neutrophil count, and
lymphocyte count were measured using a fully automated blood cell
counter XN-3000 (Sysmex Co., Kobe, Japan). AST, ALT, LDH,
creatinine, and CRP were measured using LaboFit AST, LaboFit ALT,
CicaFit LD-IFCC (Kanto Chemical Co., Inc., Tokyo, Japan),
Signasu-auto CRE (Shino-Test Co., Tokyo, Japan, and CRP-LT, Japan)
and CRP-Latex X2 (Denka Co., Niigata, Japan) using Labospect006
(Hitachi High-Tech Co., Tokyo, Japan), respectively. PCT was
measured by Elecsys® BRAHMS PCT (Roche Diagnostics K.K.,
Tokyo, Japan) using a Cobas 8000 e602 (Roche Diagnostics K.K.,
Tokyo, Japan). KL-6 was measured by Lumipulse Presto II using
Lumipulse Presto KL-6 (Sekisui Medical Co., Ltd., Tokyo, Japan);
PSP was measured by STACIA CLEIA Presepsin (LSI Medience Co.,
Tokyo, Japan). D-dimer was measured by an automatic coagulation
analyzer CS-5100 (Sysmex Co., Kobe, Japan) with LIAS AUTO D-dimer
Neo (Sysmex Co., Kobe, Japan). The result of each test was
considered 0 if it was less than the sensitivity level of the
test.
Statistical analysis
Data are expressed as medians. An unpaired t-test
was used to evaluate differences in biomarkers in each group. In
addition, correlation coefficient analysis was performed; ROC
analysis was used to calculate the threshold to discriminate
between the improved subgroup and deteriorated subgroup, and cutoff
values were calculated. Multivariate analysis was also performed by
logistic regression analyses. Covariates for multivariate
regression were selected according to a significance level of less
than 0.2 in the univariate model using a stepwise method. Values of
P<0.05 were considered to indicate statistical significance. All
statistical analyses were performed using BellCurve for Excel
(version 3.23; Social Survey Research Information Co., Ltd.).
The study was conducted with the approval of the Mie
General Medical Center Ethics Committee (No 2020-44). All study
procedures were performed in accordance with the 1975 Declaration
of Helsinki (revised in 1983) on human rights and
experimentation.
Results
Comparison of biomarker levels between
the non-severe and severe groups
A total of 201 patients (median age 48 years, 105
males and 96 females) were included in the analysis. Of these, 125
were in the non-severe group and 76 in the severe group. The
patients in the severe group were significantly older than those in
the non-severe group (54 vs. 44 years, P<0.05) and included a
higher proportion of males (M/F; 53/23 vs. 52/73, P<0.05). In
terms of blood biomarkers, neutrophil count (P<0.001), AST
(P<0.001), ALT (P=0.005), LDH (P<0.001), Cre (P=0.002), CRP
(P<0.001), KL-6 (P<0.001), PCT (P<0.001), PSP
(P<0.001), and D-dimer levels (P=0.024) were significantly
higher in the severe group, while lymphocyte (P<0.001) and Plt
count (P=0.013) were significantly lower than those in the
non-severe group, although WBC (P=0.061) count and Hb level
(P=0.223) were not different (Fig.
1A-N).
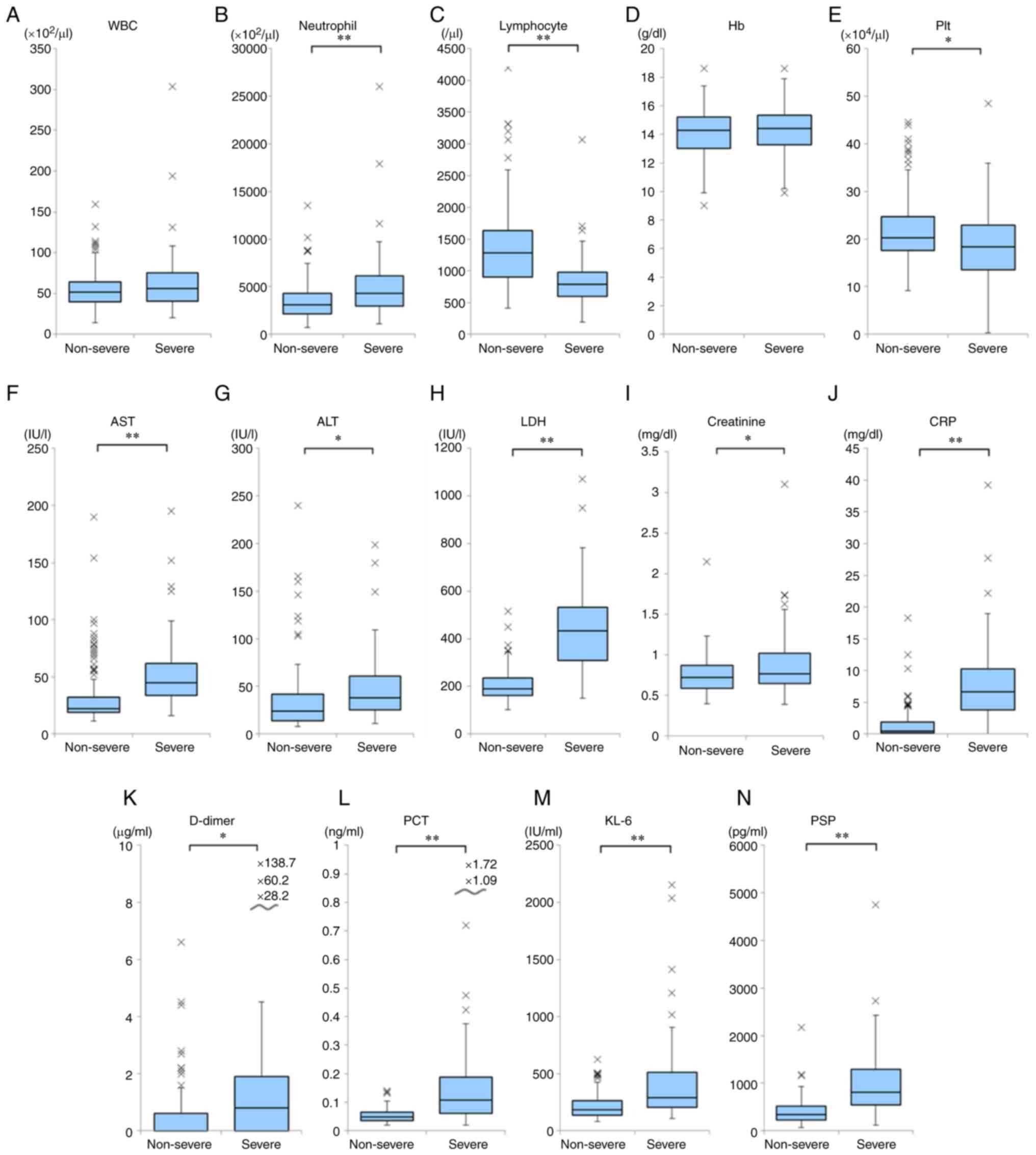 | Figure 1.Distribution of each biomarkers in
severe and non-severe groups. (A) WBC, (B) neutrophil, (C)
lymphocyte, (D) Hb, (E) platelet, (F) AST, (G) ALT, (H) LDH, (I)
creatinine, (J) CRP, (K) D-dimer, (L) PCT, (M) KL-6 and (N) PSP are
shown in severe and non-severe groups. *P<0.05, **P<0.001.
WBC, white blood cell; AST, aspartate aminotransferase; ALT,
alanine aminotransferase; LDH, lactate dehydrogenase; CRP,
C-reactive protein; PCT, procalcitonin; KL-6, sialylated
carbohydrate antigen KL-6; PSP, presepsin. |
Comparison of biomarker levels between
the improved and deteriorated groups
To examine the predictors of disease severity in
each group, each group was further divided into improved and
deteriorated groups (Table I).
There were no significant differences in age, sex, or BMI between
the improved and deteriorated subgroups of either the non-severe or
severe group. In the non-severe group, CRP (P=0.002) and LDH
(P=0.002) were significantly higher in the deteriorated subgroup
than in the improved subgroup. In the severe group, WBC count
(P=0.047), neutrophil count (P=0.039) and PSP (P=0.035) were
significantly higher in the deteriorated subgroup, and Plt count
(P=0.044) was significantly lower than in the improved subgroup
(Table II).
 | Table I.Demographic characteristics of
non-severe improved group, non-severe deteriorated group, severe
improved group and severe deteriorated group. |
Table I.
Demographic characteristics of
non-severe improved group, non-severe deteriorated group, severe
improved group and severe deteriorated group.
| Characteristic | Non-severe improved
group | Non-severe
deteriorated group | Severe improved
group | Severe deteriorated
group |
|---|
| n | 111 | 14 | 54 | 22 |
| Male, n | 46 | 6 | 38 | 15 |
| Female, n | 65 | 8 | 16 | 7 |
| Age, years
(range) | 43 (14–88) | 56 (27–85) | 51 (29–82) | 60 (22–91) |
| BMI,
kg/m2 (range) | 23.4
(13.7–42.1) | 25.7
(13.1–36.3) | 27.6 (19.6–48) | 25.2 (17.8–42) |
| Table II.Initial laboratory findings of
patients with COVID-19. |
Table II.
Initial laboratory findings of
patients with COVID-19.
| Variable | Non-severe improved
group | Non-severe
deteriorated group | Severe improved
group | Severe deteriorated
group |
|---|
| WBC
(×102/µl) | 54.3 (14–159) | 62.2 (31–132) | 57.9 (20–131) | 77.5a (27–304) |
| Neutrophil
(/µl) | 3,408.7
(727–13,499) | 4,419.4
(1,603–10,158) | 4,581.0
(1,094–11,659) |
6,471.8a
(1,685–26,022) |
| Lymphocyte
(/µl) | 1,393.7
(416–4,275) | 1,226.1
(482–3,313) | 814.7
(192–1,711) | 867.1
(200–3,070) |
| Hb (g/dl) | 14.1
(9.0–18.6) | 13.9
(10.8–17.4) | 14.4
(10.2–18.6) | 14.2
(9.9–17.9) |
| Plt
(×104/µl) | 21.9
(9.2–43.9) | 21.8
(10.4–44.6) | 20.3
(3.5–48.5) | 16.3a (0.3–28.4) |
| AST (IU/l) | 31.1 (11–190) | 40.6 (16–97) | 47.6 (17–152) | 60.5 (16–195) |
| ALT (IU/l) | 33.1 (8–240) | 44.9 (9–160) | 48.9 (11–180) | 49.5 (13–199) |
| LDH (IU/l) | 202.3
(102–517) | 265.6b (162–451) | 428.6
(174–949) | 491.0
(150–1,071) |
| Creatinine
(mg/dl) | 0.74
(0.4-2.15) | 0.77
(0.51-1.08) | 0.83
(0.42-3.10) | 1.00
(0.39-1.74) |
| CRP (mg/dl) | 1.19
(0.01-18.283) | 3.59b (0.083-12.458) | 7.83
(0.038-27.756) | 8.84
(1.046-39.193) |
| D-dimer
(µg/ml) | 0.51 (0–6.6) | 0.47 (0–2.2) | 2.77 (0–60.2) | 8.71 (0–138.7) |
| PCT (ng/ml) | 0.05
(0.00–0.13) | 0.07
(0.02–0.10) | 0.15
(0.02–1.09) | 0.25
(0.03–1.72) |
| KL-6 (IU/ml) | 213.5 (96–627) | 262.2 (79–501) | 419.9
(124–2,154) | 442.0
(105–2,036) |
| PSP (pg/ml) | 395.8
(78–2,171) | 519.9 (73–830) | 872.9
(117–2,421) |
1,240.7a
(373–4,752) |
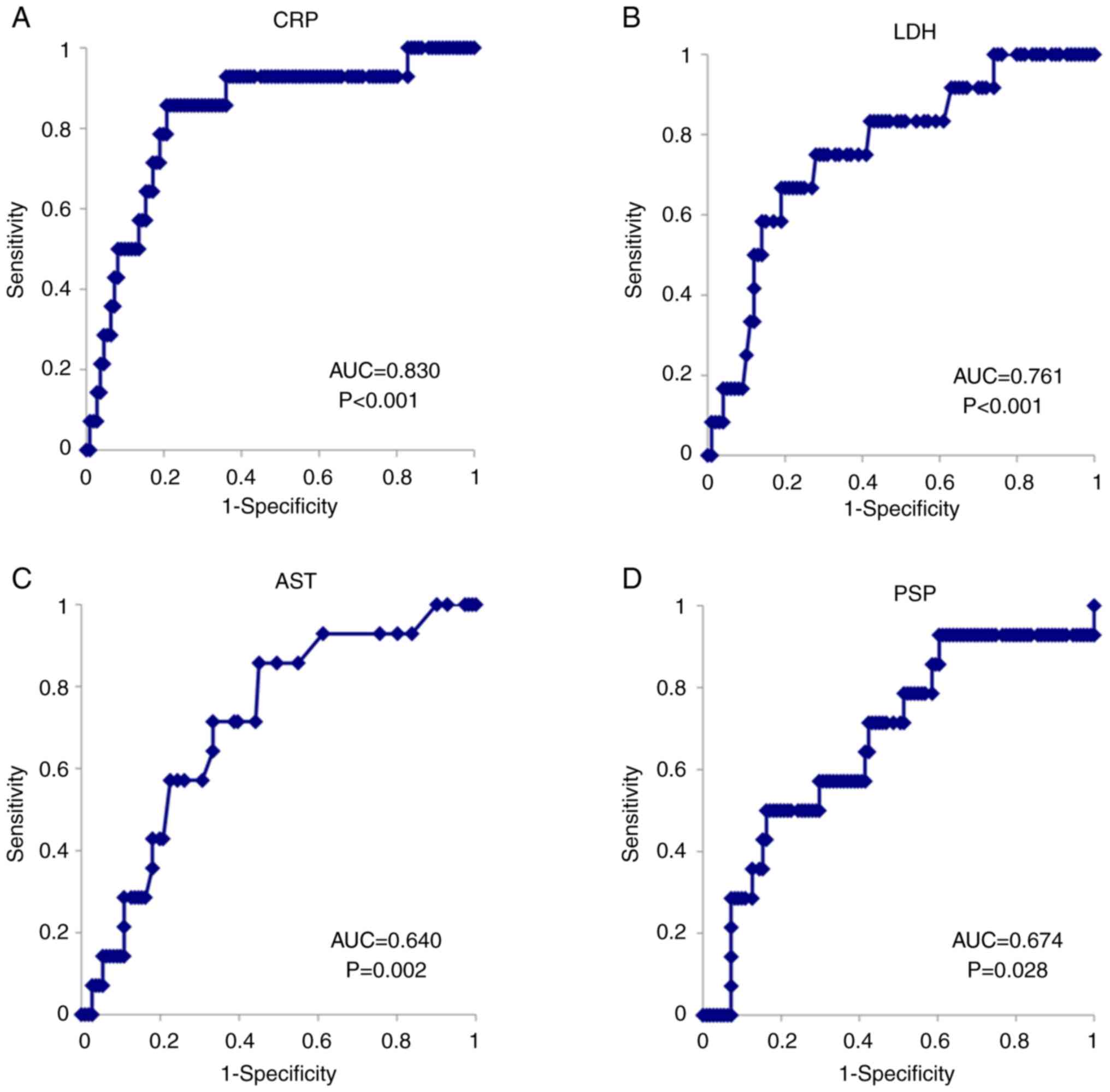
Next, the ability of each marker to predict between
improvement and deterioration was examined using ROC analysis. ROC
analysis revealed that CRP (AUC=0.830), LDH (AUC=0.761), AST
(AUC=0.709), PCT (AUC=0.696), PSP (AUC=0.674), and ALT (AUC=0.640)
had relatively good discriminatory ability in the non-severe group.
Lymphocyte count (AUC=0.589), D-dimer (AUC=0.510), and KL-6
(AUC=0.547) were not good predictive markers of severe disease
(Table III; Fig. 2A and B).
| Table III.ROC curve of non-severe improved
group vs. non-severe deteriorated group. |
Table III.
ROC curve of non-severe improved
group vs. non-severe deteriorated group.
| Variable | Cutoff value | Sensitivity
(%) | Odds ratio | AUC | P-value |
|---|
| WBC |
71×102/µl | 35.7 | 2.381 | 0.517 | 0.858 |
| Neutrophil | 4,941.6 /µl | 35.7 | 3.299 | 0.572 | 0.404 |
| Lymphocyte | 1,165.5 /µl | 57.1 | 1.687 | 0.589 | 0.253 |
| Hb | 13.2 g/dl | 42.9 | 2.025 | 0.519 | 0.845 |
| Plt |
18.6×104/µl | 57.1 | 2.895 | 0.549 | 0.569 |
| AST | 27 IU/l | 71.4 | 5.000 | 0.709 | 0.002 |
| ALT | 26 IU/l | 64.3 | 2.640 | 0.640 | 0.078 |
| LDH | 216 IU/l | 75.0 | 7.714 | 0.761 | <0.001 |
| Creatinine | 0.85 mg/dl | 50.0 | 2.581 | 0.576 | 0.361 |
| CRP | 1.61 mg/dl | 85.7 | 22.957 | 0.830 | <0.001 |
| D-dimer | 0 mg/dl | 66.7 | 1.176 | 0.510 | 0.917 |
| PCT | 0.062 ng/ml | 75.0 | 9.000 | 0.696 | 0.085 |
| KL-6 | 220 IU/ml | 50.0 | 1.816 | 0.547 | 0.647 |
| PSP | 369 pg/ml | 71.4 | 3.404 | 0.674 | 0.028 |
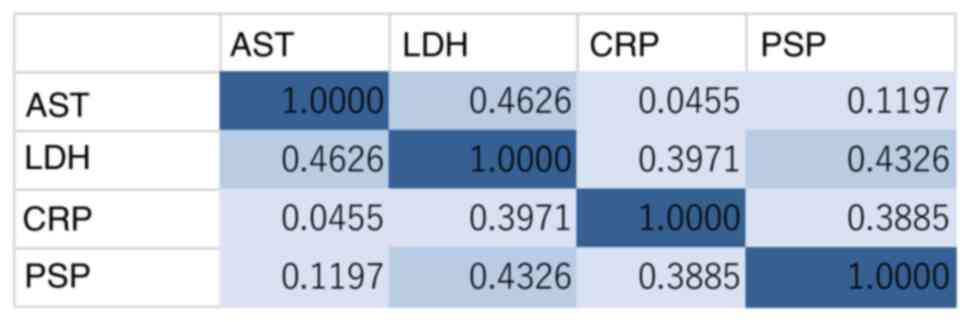
Statistical superiority in predicting prognosis was
observed only for CRP (P<0.001), LDH (P<0.001), AST
(P=0.002), and PSP (P=0.028). Spearman's rank correlation
coefficient showed a weak correlation between AST and LDH and
between LDH and PSP (Fig. 3).
Stepwise logistic regression analysis of the non-severe group
identified only CRP as a significant predictor of disease severity
(odds ratio 41.45, 95% confidence interval: 4.91-349.24,
P<0.001).
Further, in the severe group, ROC analysis of
laboratory values showed relatively high accuracy for creatinine
(AUC=0.646), PCT (AUC=0.644), Plt (AUC=0.630), and PSP (AUC=0.604),
although the values did not reach statistical significance.
Lymphocyte count (AUC=0.510), D-dimer (AUC=0.531), and KL-6
(AUC=0.516) at the time of admission were not predictive markers of
deterioration adequately in the severe group (Table IV).
| Table IV.ROC curve of severe improved group
vs. severe deteriorated group. |
Table IV.
ROC curve of severe improved group
vs. severe deteriorated group.
| Variable | Cutoff value | Sensitivity
(%) | Odds ratio | AUC | P-value |
|---|
| WBC |
54×102/µl | 63.6 | 1.625 | 0.574 | 0.323 |
| Neutrophil | 5,715.9/µl | 40.9 | 1.800 | 0.575 | 0.328 |
| Lymphocyte | 739.2/µl | 68.2 | 1.990 | 0.510 | 0.892 |
| Hb | 14.6 g/dl | 68.2 | 1.590 | 0.513 | 0.856 |
| Plt |
17.2×104/µl | 59.1 | 2.270 | 0.630 | 0.057 |
| AST | 44 IU/l | 59.1 | 1.444 | 0.544 | 0.576 |
| ALT | 32 IU/l | 50.0 | 2.000 | 0.532 | 0.671 |
| LDH | 476 IU/l | 54.5 | 2.471 | 0.580 | 0.334 |
| Creatinine | 0.9 mg/dl | 54.5 | 2.850 | 0.646 | 0.055 |
| CRP | 7.039 mg/dl | 63.6 | 2.359 | 0.540 | 0.572 |
| D-dimer | 0 mg/dl | 38.9 | 2.430 | 0.531 | 0.717 |
| PCT | 0.149 ng/ml | 68.4 | 6.139 | 0.644 | 0.069 |
| KL-6 | 231 IU/ml | 75.0 | 2.111 | 0.516 | 0.839 |
| PSP | 1,044 pg/ml | 50.0 | 2.857 | 0.604 | 0.177 |
Discussion
Identification of clinical and laboratory predictors
of disease progression toward severe or critical status is
extremely important for clinicians to be able to treat patients
appropriately and save their lives. In this study, we found several
biomarkers related to hematology, sepsis, inflammation, blood
coagulation, hepatic function, and renal function that were
significantly different between the non-severe and severe groups.
These results were consistent with previous reports. Several
meta-analyses have shown that many biomarkers are involved in
severe patients, including neutrophil, lymphocyte, monocyte, and
eosinophil counts, Hb, Plt count, albumin, serum sodium, AST, ALT,
blood urea nitrogen (BUN), creatinine, CRP, PCT, LDH, D-dimer,
glucose levels, and have demonstrated significantly different
levels of these markers between non-severe and severe patients,
suggesting that systemic disorders or organ failure, in addition to
respiratory failure and coagulation abnormalities, are prominent in
the severe stage of this infection (12,15–20,27).
We previously reported that patients' backgrounds,
including their median age and sex, hypertension, hyperlipidemia,
and diabetes mellitus are related to the severity of COVID-19
infection. We also reported that levels of CRP, ferritin, PCT,
albumin, HbA1c, and LDH are useful markers of severity, and that
hemostatic abnormalities are frequently observed in patients in a
severe disease stage (26).
In fact, these markers are critically important for
evaluating the patient's condition, including the occurrence of
complications and disease severity. However, it is not well
elucidated whether these biomarkers can predict the prognosis of
patients. Therefore, we divided patients in both the severe and
non-severe groups into two further groups each, the improved and
deteriorated subgroups. We found that in the non-severe group, four
markers, CRP, LDH, AST, and PSP have significant potential as
prognostic markers. Multivariate analysis demonstrated that CRP is
the most useful predictive marker for prognosis among them.
However, we cloud not identify potential markers of prognosis in
the severe group. CRP is a type of protein produced by the liver,
and its production is induced by various inflammatory cytokines,
such as IL-6, and hence, it serves as an early marker of infection
and inflammation (27). Many
studies also suggested the usefulness of CRP in diagnosing disease
severity (13,23,28–32), and the same results were obtained
in this study. Our logistic regression analysis clearly
demonstrated the effectiveness of CRP as a marker for diagnosing
severity and predicting disease progression in non-severe COVID-19
patients, who consisted primarily of those infected with the delta
variant, in Japan. Using ROC analysis in the early stage of
COVID-19 infection, a previous study showed that CRP might be a
valuable marker for predicting disease in non-severe COVID-19
patients (28), which is
consistent with our data. Therefore, these results suggest that
non-severe COVID-19 patients with high CRP levels should be
adequately followed and treated for the early detection of severe
manifestations and for establishing a therapeutic strategy, even if
their general condition or respiratory function do not meet the
standard for the severe group.
A previous study also listed PSP as a biomarker of
prognostic significance (33).
PSP, also known as soluble cluster of differentiation (CD) 14
subtype, is a small peptide generated from soluble CD14, and is
known to be a regulatory factor that modulates immune responses
through interaction with T and B cells, which is released into the
blood when monocytes are activated by the recognition of
lipopolysaccharides (LPS) from several infectious agents. PSP is an
early marker of mortality and reportedly shows better prognostic
performance than PCT. Hence, it has been proposed as a useful
marker in risk stratification strategies in patients with sepsis
(12,34,35). Furthermore, it was recently
demonstrated that PSP plays a role as a biomarker in providing
prognostic information, such as duration of hospitalization, even
in COVID-19 patients. Our results, showing the high prognostic
value of PSP in non-severe COVID-19 patients, suggest that PSP
might be a highly sensitive indicator of immunological reactions
against infectious antigens in the early stage of COVID-19
infection, and might predict subsequent disease progression.
However, in our study results, since PSP showed only a weak
correlation with CRP, we believe it is worthwhile to measure both
PSP and CRP.
We also found that the liver-related markers, AST
and LDH, could predict prognosis in non-severe COVID-19 patients.
Many liver-related biomarker abnormalities have been reported as
being associated with COVID-19, such as total bilirubin, AST, ALT,
γ-GTP, LDH, and low albumin levels. Many meta-analyses revealed
that some of these biomarkers (AST/ALT, γ-GTP, LDH) exhibit
significantly elevated levels in severe cases, and that high levels
of AST and LDH were more likely to be observed in severe cases
(17,18,20). However, since our study did not
consider patients with liver disease, further research is needed to
separately evaluate patients with liver disease in greater
detail.
According to previous reports, COVID-19-infected
livers exhibit several pathological changes such as extensive
apoptosis and binuclear hepatocytes, steatosis, lobular necrosis,
inflammation of the portal area, and congestion of hepatic sinuses
with micro thrombosis (36–38). Therefore, the underlying
mechanisms of liver injury in COVID-19 cases might include a
virus-induced cytopathic effect, immune-mediated inflammation by
cytokine storm, sepsis-related liver injury, hepatic sinus
congestion related to thrombosis, drug-induced liver injury, or
pre-existing liver disease. Based on these considerations, liver
disfunction might reflect an abnormal physiological condition in
COVID-19 infection and a worse clinical course. More mechanistic
understanding of liver injury with COVID-19 infection is critically
important in clinical management practices for patients with
hepatic injury.
Despite the potential markers of disease progression
in non-severe COVID-19 cases mentioned above, our study failed to
identify any biomarker that could predict the prognosis in severe
cases, although mean PSP, neutrophil count and, Plt count were
statistically significantly higher in the severe deteriorated
subgroup than the severe improved subgroup. These results suggest
that in severe cases, since various markers are already elevated
due to pneumonia and multiple organ failure, it is difficult to
predict the prognosis based on these markers alone.
Our results suggest that the monitoring of
inflammatory markers as well as liver-related markers, might serve
as an early warning system for progression to severe COVID-19.
Simultaneously monitoring CRP and PSP values might allow early
detection of lung disease, and might reduce over-prescription of
anti-viral agents or anti-inflammatory drugs for patients who do
not need them, and trigger early multidisciplinary therapy to
prevent sepsis and other severe conditions.
This study has several limitations. First, although
we followed the guidelines, treatment modalities changed during
this study period, and in some cases the duration of treatment and
the drugs used differed, even though the severity of COVID-19 was
the same, which may have affected the course of the disease.
Second, the retrospective study design and lack of standardization
of the available documents, such as for patients' backgrounds or
therapeutic interventions, could have led to selection bias. Third,
the sample sizes were relatively small for an accurate assessment
of risk factors. Finally, the data in this study were obtained from
a single center in Japan, which could potentially limit the
generalizability of the findings.
In conclusion, this analysis provides important
evidence for the prediction of prognosis in non-severe COVID-19
cases based on laboratory test results at the time of admission and
might facilitate efficient resource allocation in the era of
scarcity of available resources, including for hospitalization.
CRP, LDH, AST, and PSP are the most reliable markers
to determine the prognosis of patients with non-severe COVID-19.
Future methodologically well-designed studies conducted on other
populations will be needed to establish appropriate strategies for
treating patients with different severities of COVID-19
infection.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HW and KS conceived the study. YI and SF designed
the methodology. KI, MK, KN, KeY, SH, YS, HMik, HG, KH, YNa, HMiz,
ToK, YT, SK, TaK, YNi, DS, TT, YI, IM, AY, HW and SF curated the
data. SF, YI and SK confirm the authenticity of all the raw data.
SF wrote the original draft preparation. KS reviewed and edited the
manuscript. KI, MK, KN, KeY, SH, YS, HMik, HG, KH, YNa, HMiz, ToK,
YT, SK, TaK, YNi, DS, TT, YI, IM, AY, KT, KoY, HW and SF performed
the investigations. KS supervised. All authors read and approved
the final version of the manuscript.
Ethics approval and consent to
participate
The study was conducted with the approval of the Mie
General Medical Center Ethics Committee (approval no. 2020-44).
Opt-out method was performed for the participation in the
study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu
Y, Zhang L, Fan G, Xu J, Gu X, et al: Clinical features of patients
infected with 2019 novel coronavirus in Wuhan, China. Lancet.
395:497–506. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jiang F, Deng L, Zhang L, Cai Y, Cheung CW
and Xia Z: Review of the clinical characteristics of coronavirus
disease 2019 (COVID-19). J Gen Intern Med. 35:1545–1549. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gavriatopoulou M, Ntanasis-Stathopoulos I,
Korompoki E, Fotiou D, Migkou M, Tzanninis IG, Psaltopoulou T,
Kastritis E, Terpos E and Dimopoulos MA: Emerging treatment
strategies for COVID-19 infection. Clin Exp Med. 21:167–179. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
World Health Organization (WHO), . WHO
Coronavirus (COVID-19) Dashboard. WHO; Geneva: 2017, https://covid19.who.int/June 17–2022
|
|
5
|
Machhi J, Herskovitz J, Senan AM, Dutta D,
Nath B, Oleynikov MD, Blomberg WR, Meigs DD, Hasan M, Patel M, et
al: The natural history, pathobiology, and clinical manifestations
of SARS-CoV-2 infections. J Neuroimmune Pharmacol. 15:359–386.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
National Institutes of Health, . COVID-19
Treatment Guidelines: Clinical Spectrum of SARS-CoV-2 Infection.
https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/June
17–2022
|
|
7
|
World Health Organization (WHO), .
Therapeutics and COVID-19: living guideline. https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2022.4June
17–2022
|
|
8
|
Cheng Y, Luo R, Wang K, Zhang M, Wang Z,
Dong L, Li J, Yao Y, Ge S and Xu G: Kidney disease is associated
with in-hospital death of patients with COVID-19. Kidney Int.
97:829–838. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Suardi LR, Pallotto C, Esperti S, Tazzioli
E, Baragli F, Salomoni E, Botta A, Frigieri FC, Pazzi M, Stera C,
et al: Risk factors for non-invasive/invasive ventilatory support
in patients with COVID-19 pneumonia: A retrospective study within a
multidisciplinary approach. Int J Infect Dis. 100:258–263. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ustun GK, Keskin A, Aci R, Erdem MA and
Ari M: Association between Hb A1c and severity of COVID-19
patients. Hemoglobin. 45:124–128. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
British Medical Journal Best Practice, .
Coronavirus disease 2019 (COVID-19): Epidemiology. Coronavirus
disease. 2019.https://bestpractice.bmj.com/topics/en-gb/3000201/epidemiologyJune
17–2022
|
|
12
|
Wu J, Hu L, Zhang G, Wu F and He T:
Accuracy of presepsin in sepsis diagnosis: A systematic review and
meta-analysis. PLoS One. 10:e01330572015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kermali M, Khalsa RK, Pillai K, Ismail Z
and Harky A: The role of biomarkers in diagnosis of COVID-19-A
systematic review. Life Sci. 254:1177882020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pan F, Yang L, Li Y, Liang B, Li L, Ye T,
Li L, Liu D, Gui S, Hu Y and Zheng C: Factors associated with death
outcome in patients with severe coronavirus disease-19 (COVID-19):
A case-control study. Int J Med Sci. 17:1281–1292. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Soraya GV and Ulhaq ZS: Crucial laboratory
parameters in COVID-19 diagnosis and prognosis: An updated
meta-analysis. Med Clin (Barc). 155:143–151. 2020.(In English,
Spanish). View Article : Google Scholar
|
|
16
|
Li J, He X, Yuan Y, Zhang W, Li X, Zhang
Y, Li S, Guan C, Gao Z and Dong G: Meta-analysis investigating the
relationship between clinical features, outcomes, and severity of
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
pneumonia. Am J Infect Control. 49:82–89. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ghahramani S, Tabrizi R, Lankarani KB,
Kashani SMA, Rezaei S, Zeidi N, Akbari M, Heydari ST, Akbari H,
Nowrouzi-Sohrabi P and Ahmadizar F: Laboratory features of severe
vs. non-severe COVID-19 patients in Asian populations: A systematic
review and meta-analysis. Eur J Med Res. 25:302020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ou M, Zhu J, Ji P, Li H, Zhong Z, Li B,
Pang J, Zhang J and Zheng X: Risk factors of severe cases with
COVID-19: A meta-analysis. Epidemiol Infect. 148:e1752020.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Elshazli RM, Toraih EA, Elgaml A,
El-Mowafy M, El-Mesery M, Amin MN, Hussein MH, Killackey MT, Fawzy
MS and Kandil E: Diagnostic and prognostic value of hematological
and immunological markers in COVID-19 infection: A meta-analysis of
6320 patients. PLoS One. 15:e02381602020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Danwang C, Endomba FT, Nkeck JR, Wouna
DLA, Robert A and Noubiap JJ: A meta-analysis of potential
biomarkers associated with severity of coronavirus disease 2019
(COVID-19). Biomark Res. 8:372020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Paparella D, Colucci M, Squiccimarro E,
Raimondo P, De Palma F, Ranieri P, Mariggiò MA and Grasso S:
Clotting abnormalities in critically ill COVID-19 patients are
inconsistent with overt disseminated intravascular coagulation.
Thromb Res. 196:272–275. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mehta AA, Haridas N, Belgundi P and Jose
WM: A systematic review of clinical and laboratory parameters
associated with increased severity among COVID-19 patients.
Diabetes Metab Syndr. 15:535–541. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yitbarek GY, Ayehu GW, Asnakew S, Ayele
FY, Gare MB, Mulu AT, Dagnaw FT and Melesie BD: The role of
C-reactive protein in predicting the severity of COVID-19 disease:
A systematic review. SAGE Open Med. 9:205031212110507552021.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bivona G, Agnello L and Ciaccio M:
Biomarkers for prognosis and treatment response in COVID-19
patients. Ann Lab Med. 41:540–548. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Adachi M, Murakami M, Yoneoka D, Kawashima
T, Hashizume M, Sakamoto H, Eguchi A, Ghaznavi C, Gilmour S, Kaneko
S, et al: Factors associated with the risk perception of COVID-19
infection and severe illness: A cross-sectional study in Japan. SSM
Popul Health. 18:1011052022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yamamoto A, Wada H, Ichikawa Y, Mizuno H,
Tomida M, Masuda J, Makino K, Kodama S, Yoshida M, Fukui S, et al:
Evaluation of biomarkers of severity in patients with COVID-19
infection. J Clin Med. 10:37752021. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Huang I, Pranata R, Lim MA, Oehadian A and
Alisjahbana B: C-reactive protein, procalcitonin, D-dimer, and
ferritin in severe coronavirus disease-2019: A meta-analysis. Ther
Adv Respir Dis. 14:17534666209371752020. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang G, Wu C, Zhang Q, Wu F, Yu B, Lv J,
Li Y, Li T, Zhang S, Wu C, et al: C-reactive protein level may
predict the risk of COVID-19 aggravation. Open Forum Infect Dis.
7:ofaa1532020. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ali N: Elevated level of C-reactive
protein may be an early marker to predict risk for severity of
COVID-19. J Med Virol. 92:2409–2411. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ji P, Zhu J, Zhong Z, Li H, Pang J, Li B
and Zhang J: Association of elevated inflammatory markers and
severe COVID-19: A meta-analysis. Medicine (Baltimore).
99:e233152020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Stringer D, Braude P, Myint PK, Evans L,
Collins JT, Verduri A, Quinn TJ, Vilches-Moraga A, Stechman MJ,
Pearce L, et al: The role of C-reactive protein as a prognostic
marker in COVID-19. Int J Epidemiol. 50:420–429. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Smilowitz NR, Kunichoff D, Garshick M,
Shah B, Pillinger M, Hochman JS and Berger JS: C-reactive protein
and clinical outcomes in patients with COVID-19. Eur Heart J.
42:2270–2279. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zaninotto M, Mion MM, Cosma C, Rinaldi D
and Plebani M: Presepsin in risk stratification of SARS-CoV-2
patients. Clin Chim Acta. 507:161–163. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Endo S, Suzuki Y, Takahashi G, Shozushima
T, Ishikura H, Murai A, Nishida T, Irie Y, Miura M, Iguchi H, et
al: Usefulness of presepsin in the diagnosis of sepsis in a
multicenter prospective study. J Infect Chemother. 18:891–897.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Masson S, Caironi P, Spanuth E, Thomae R,
Panigada M, Sangiorgi G, Fumagalli R, Mauri T, Isgrò S, Fanizza C,
et al: Presepsin (soluble CD14 subtype) and procalcitonin levels
for mortality prediction in sepsis: Data from the Albumin Italian
outcome sepsis trial. Crit Care. 18:R62014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Fan Z, Chen L, Li J, Cheng X, Yang J, Tian
C, Zhang Y, Huang S, Liu Z and Cheng J: Clinical features of
COVID-19-related liver functional abnormality. Clin Gastroenterol
Hepatol. 18:1561–1566. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wang Y, Liu S, Liu H, Li W, Lin F, Jiang
L, Li X, Xu P, Zhang L, Zhao L, et al: SARS-CoV-2 infection of the
liver directly contributes to hepatic impairment in patients with
COVID-19. J Hepatol. 73:807–816. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Li J and Fan JG: Characteristics and
mechanism of liver injury in 2019 coronavirus disease. J Clin
Transl Hepatol. 8:13–17. 2020. View Article : Google Scholar : PubMed/NCBI
|