Introduction
Gastric cancer is the fourth most common type of
cancer and the second leading cause of cancer-related death
worldwide (1). Peritoneal
dissemination is a common finding and the most frequent site of
recurrence in gastric cancer; it is associated with a poor
prognosis even after curative resection (2–4). In
recent years, certain reports have focused on the efficacy of
chemotherapy for peritoneal dissemination (5–9).
Staging laparoscopy is currently the most sensitive method for
detecting peritoneal dissemination and minimising the possibility
of unnecessary laparotomy (10,11).
However, it is often extremely difficult to make a decision
regarding indications and timing in performing laparoscopy in
preoperative diagnosis and during postoperative monitoring.
Although computed tomography (CT) is a diagnostic modality for the
detection of peritoneal metastasis in conventional imaging study,
CT has a limited capacity for revealing peritoneal metastasis
unless the disease has progressed sufficiently to cause obstruction
of the intestinal, biliary or urinary tract (12–14).
High-speed spiral CT showed a sensitivity of only 47.4% in patients
with peritoneal dissemination of abdominal malignancies (15).
Therefore, it is necessary to identify an ideal
molecular marker with which to determine the optimum time for
staging laparoscopy so as not to retard chemotherapy due to the
inevitable delay in detection. Such a marker is expected to be less
invasive and easily monitored, for example by a simple blood test.
Carbohydrate antigen (CA) 125 has been investigated for putative
diagnostic value, but its utility as a screening marker is limited
due to its low sensitivity (16).
Peritoneal dissemination in gastric cancer is
characterised by abundant collagen deposition in the peritoneum
(17), resulting in various severe
complications such as ileus, hydronephrosis and obstructive
jaundice. The mechanism proposed for the formation of this
desmoplastic stroma is the apparent increase caused by the
accumulation of the preexisting matrix or synthesis by neoplastic
cells themselves. In the liver, extracellular matrix components,
the amino-terminal propeptide of procollagen type III (type III
procollagen) and type IV collagen are considered to be reliable
serum markers of active fibrogenesis and are used clinically to
assess the progression of fibrosis (18–20).
The present study was performed to investigate
whether the progression of peritoneal metastasis in gastric cancer
is accompanied by such changes in collagen-and basement
membrane-related metabolites in serum, as well as whether these
metabolites are useful in the diagnosis of disease progression in
clinical practice. The serum levels of type III procollagen and
type IV collagen were examined in gastric cancer patients with and
without peritoneal dissemination. Additionally type III procollagen
and IV collagen were compared to commonly accepted tumor markers,
such as carcinoembryonic antigen (CEA), CA19-9 and CA125. Findings
of this study showed that type IV collagen can be used as a serum
marker for peritoneal dissemination in gastric cancer.
Materials and methods
Patients and serum samples
Serum was obtained at the time of diagnosis with
informed consent according to our Institutional Review
Board-approved guidelines. A total of 117 serum samples were
obtained from patients with pathologically confirmed gastric
adenocarcinoma, all of whom underwent surgical treatment or
laparoscopic examination at the Department of Gastroenterological
Surgery of Kanazawa University Hospital between 2004 and 2008.
Inclusion criteria for the study involved patients
with a confirmed diagnosis of gastric adenocarcinoma and the
provision of written informed consent. Exclusion criteria included
inability to provide informed consent, patients with chronic
hepatitis or liver cirrhosis, to eliminate false-positive results,
and patients with other malignancies diagnosed or treated within
the last 5 years.
Of the 117 patients included in this study, 32
(27.3%) had peritoneal dissemination (17 male, 15 female; mean age
57 years, range 28–80). All of the patients underwent laparotomy
(n=7) or laparoscopic examination (n=25) to pathologically confirm
the peritoneal dissemination of gastric cancer. Based on the
laparotomy findings, 85 of the 117 patients (72.6%) had no
peritoneal dissemination. These patients were divided into two
groups based on pathological findings: 40 patients (34.1%) in the
advanced gastric cancer group (23 male, 17 female; mean age 68
years, range 47–78) and 45 patients (38.6%) in the early gastric
cancer group (22 male, 23 female; mean age 67 years, range 50–75).
Staging was carried out according to the classification of the
Japanese Endoscopic Society, in which the distribution of early
gastric cancer was defined as a T1 tumor (tumor invasion of mucosa
or submucosa) (21).
Samples were centrifuged after collection and stored
at −70°C until the assays were performed. The samples were labelled
with a unique identifier to protect the confidentiality of the
patients. None of the samples were thawed more than twice before
analysis.
Biochemical assays
CEA and CA19-9 levels were measured by a counting
immunoassay using a Ranream CEA kit (TOA Medical Electronics Co.,
Kobe, Japan) and a Ranream CA19-9 kit (Toray-Fuji Bionics, Tokyo,
Japan). CA125 analysis was performed using a Cobas Core CA125
enzyme-immunoassay analysis kit (Roche, Basel, Switzerland). The
serum type III procollagen level was determined using a commercial
RIA kit (Behringwerke AG, Marburg, Germany), and type IV collagen
concentration was determined by ELISA using a commercial kit (Fuji
Chemical Ind., Tokyo, Japan). Each sample was assessed in
triplicate. The cut-off values of CEA, CA19-9 and CA125 were set
according to the manufacturer’s instructions (6.5 ng/ml, 37 U/ml
and 35 U/ml, respectively).
Statistical methods
A comparison between the quantitative variables was
performed using the Mann-Whitney U test. The diagnostic accuracy of
each of the candidate biomarkers was evaluated using receiver
operating characteristic (ROC) curve analysis, which correlates
true and false-positive rates [sensitivity and (1 - specificity)].
In addition, the differences in the area under the curve (AUC)
values were determined. The optimal cut-off point for type IV
collagen was selected based on the ROC curve analysis. Sensitivity,
specificity, positive and negative predictive values were
calculated using a 2 × 2 table of the collected data. Multivariate
logistic regression for the odds ratio was used to assess the
simultaneous contribution of each covariate in the multivariate
analysis. In all analyses, P<0.05 was considered to be
statistically significant. Statistical analyses were carried out
using SPSS® v12.0 software.
Results
Serum levels of type III procollagen and
type IV collagen
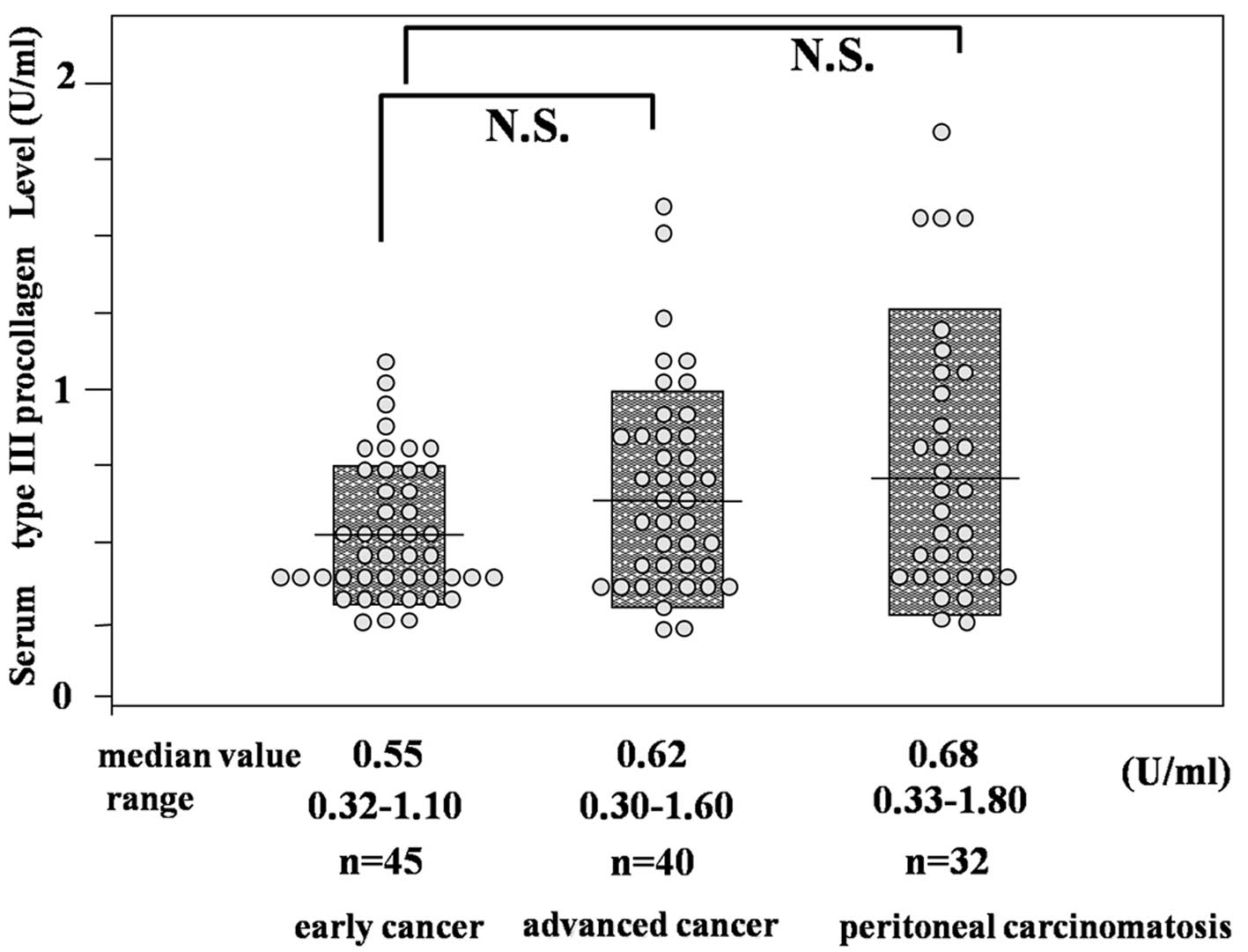
The median serum type III procollagen levels in the
early and advanced gastric cancer groups were 0.55 and 0.62 U/ml,
respectively. The corresponding value in patients with peritoneal
dissemination was 0.68 U/ml. No significant differences were noted
in the median serum type III procollagen levels among the three
groups (Fig. 1).
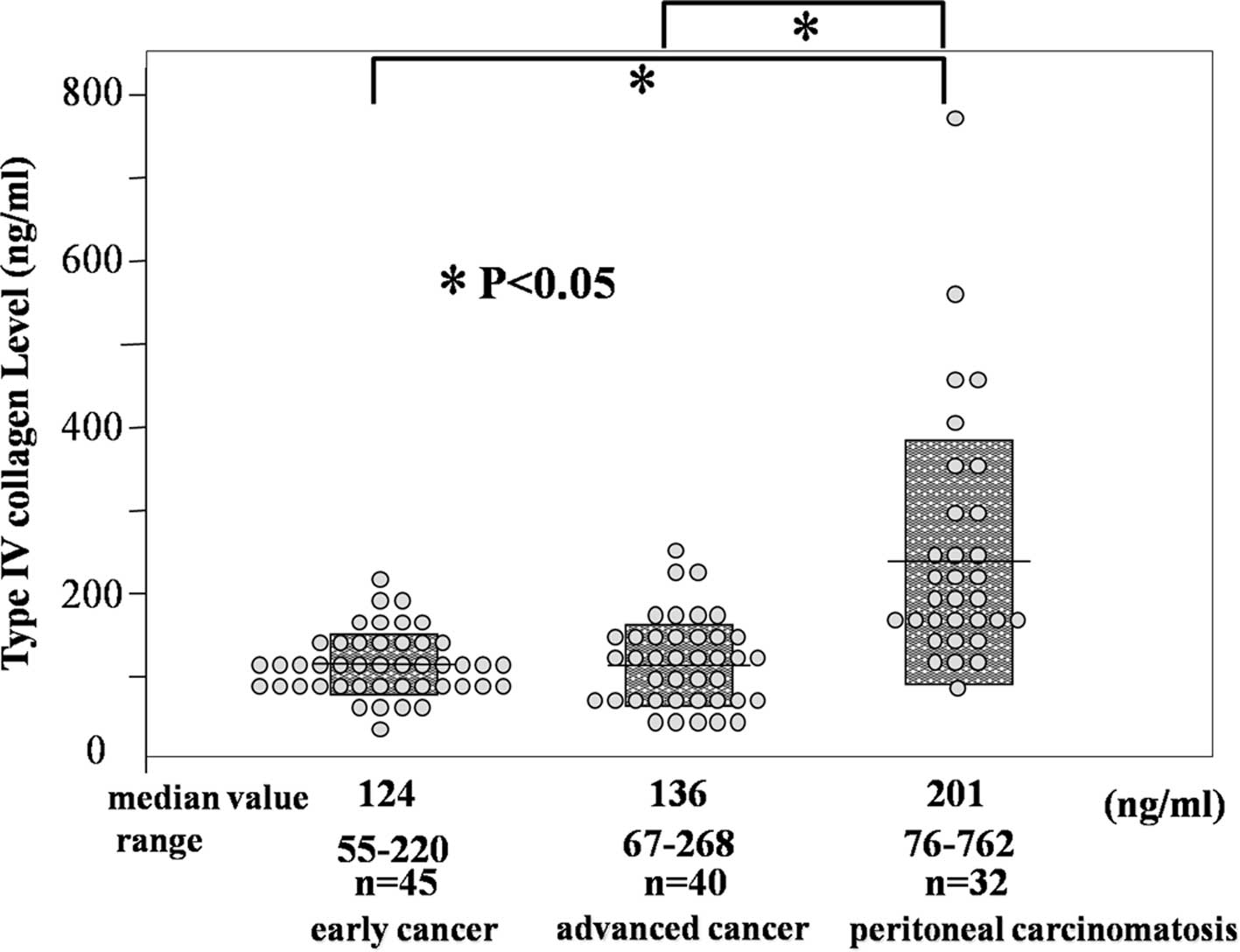
In contrast, the median serum type IV collagen level
was significantly higher in patients with peritoneal dissemination
(201 ng/ml) in comparison with the early gastric cancer patients
(124 ng/ml) and advanced gastric cancer patients (136 ng/ml)
(P<0.05) (Fig. 2).
ROC curve for the diagnosis of peritoneal
dissemination
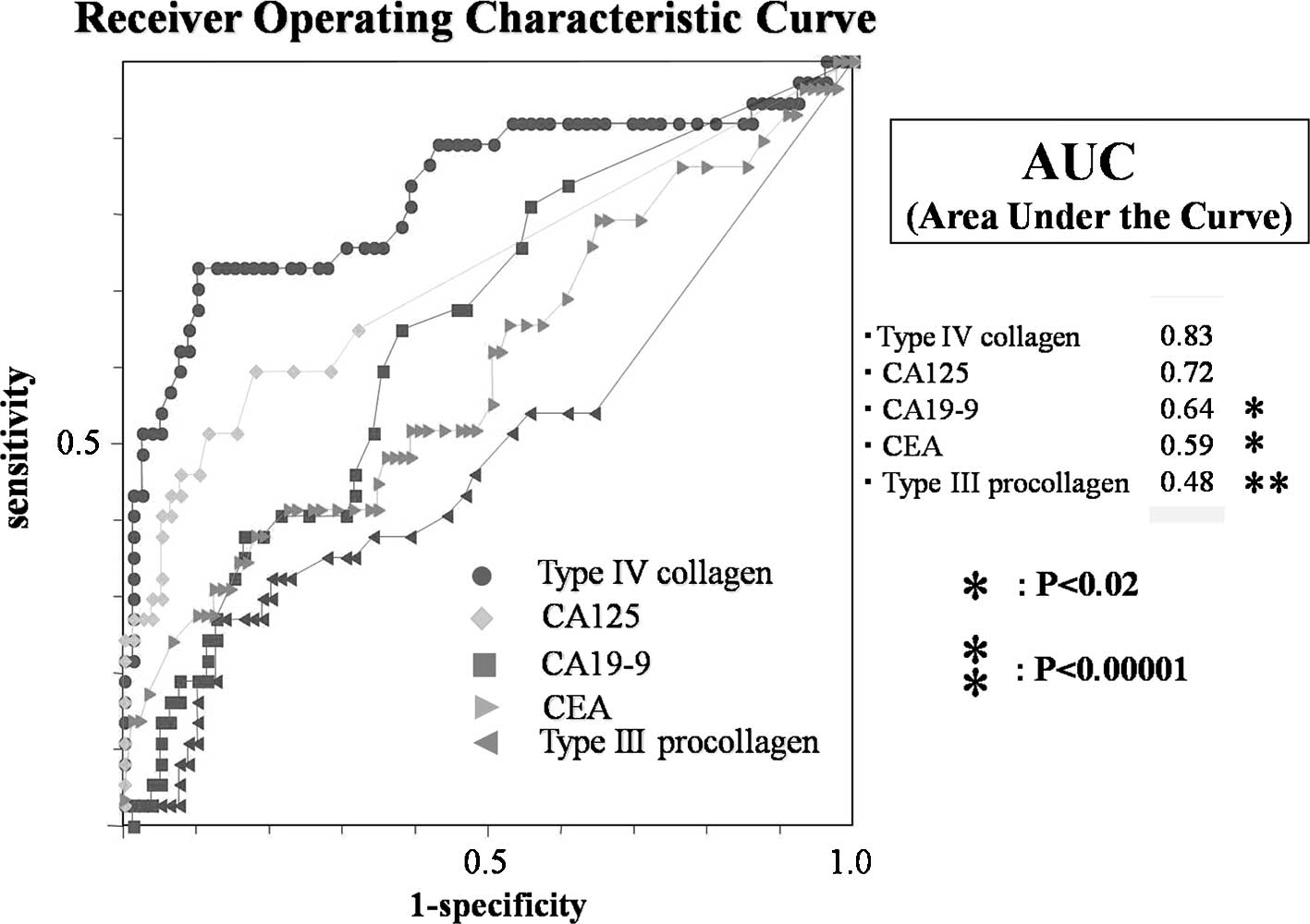
To evaluate the performance of type III procollagen
and IV collagen as a diagnostic test, ROC curves were generated as
shown in Fig. 3. The diagnostic
accuracy of the test is expressed by the AUC. Among the individual
markers, type IV collagen had the largest AUC (0.83), followed by
CA125 (0.72), CA19-9 (0.64), CEA (0.59) and type III procollagen
(0.48). Although no significant difference was found between the
AUC values of type IV collagen and CA125 (P=0.15), the AUC value of
type IV collagen was significantly higher than those of CA19-9, CEA
and type III procollagen (P<0.02–0.00001). These observations
suggested that type IV collagen is a more useful marker for
predicting peritoneal dissemination than type III procollagen.
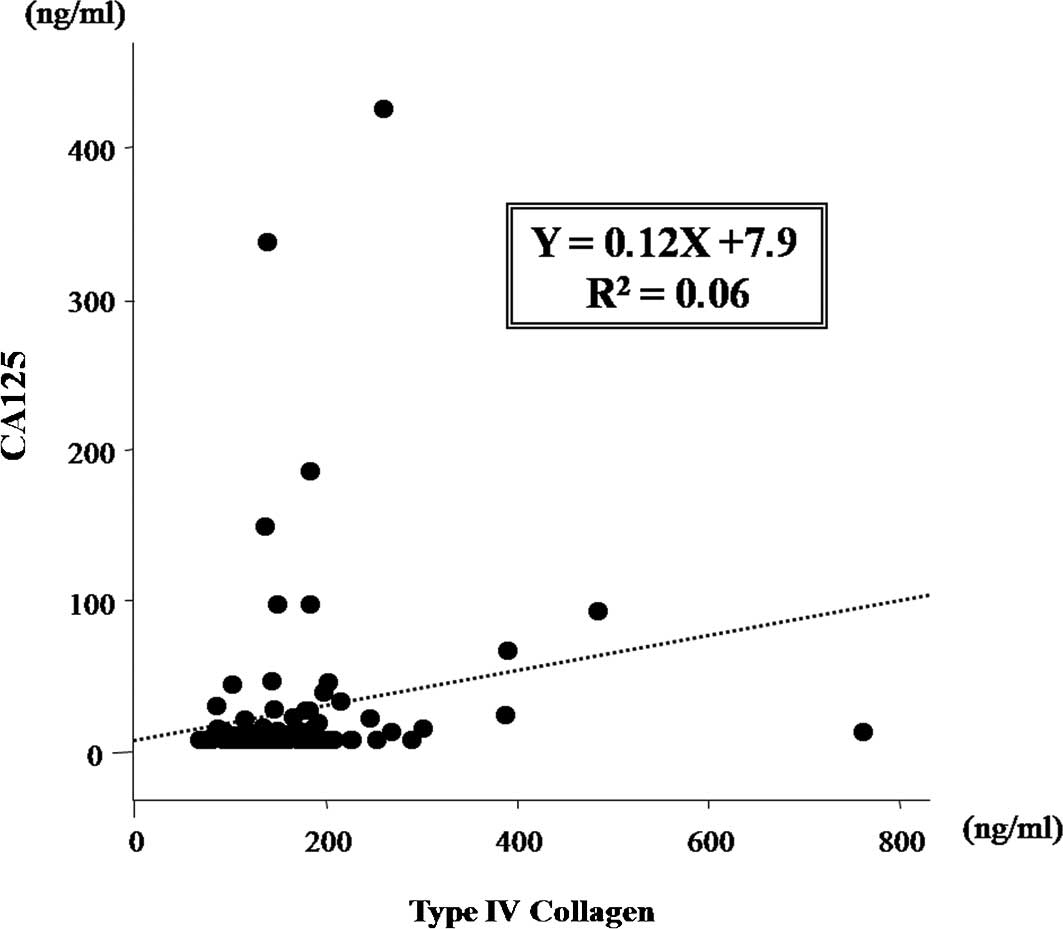
The correlation between the levels of type IV
collagen and CA125 was investigated. The data showed no correlation
between these markers with a coefficient (R2) of 0.06
(Fig. 4). This result suggested
that serum type IV collagen is useful as a serum marker for
peritoneal dissemination involving a different mechanism than that
responsible for the elevation of CA125.
The correlations between the levels of other markers
were also investigated, but no significant correlations were
observed (data not shown).
With regard to type IV collagen, the best compromise
between true and false positives was achieved by a threshold of
~170 ng/ml according to the ROC curve analysis.
Comparison of biomarkers for the
diagnosis of peritoneal dissemination
Table I shows the
performance of the biomarkers for the diagnosis of peritoneal
dissemination in gastric cancer. For type IV collagen, a cut-off
value of 170 ng/ml was used in this investigation. The sensitivity
of type IV collagen was much higher than that of the other markers.
The specificity and positive predictive values of CA125 were higher
than those of type IV collagen. The highest negative predictive
value was observed for type IV collagen. Type IV collagen, CA19-9
and CA125 significantly predicted peritoneal dissemination in the
univariate analyses. Based on multivariate logistic regression,
type IV collagen and CA125 independently predicted peritoneal
dissemination. The odds ratios for type IV collagen and CA125 were
15.667 (95% CI, 5.534–44.312) and 9.435 (95% CI, 1.765–50.459),
respectively (Table II).
 | Table IComparison of the diagnostic ability
of serum biomarkers for the diagnosis of peritoneal
dissemination. |
Table I
Comparison of the diagnostic ability
of serum biomarkers for the diagnosis of peritoneal
dissemination.
| Biomarker | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | OR | 95% CI | P-value |
|---|
| CEA | 27.03 | 87.34 | 50.00 | 71.88 | 2.56 | 0.98–6.69 | 0.05600 |
| CA19-9 | 21.62 | 92.41 | 57.14 | 71.57 | 3.36 | 1.11–10.06 | 0.03100 |
| CA125 | 29.73 | 94.94 | 73.33 | 74.26 | 7.93 | 3.74–9.21 | 0.00050 |
| Type IV collagen | 70.27 | 86.08 | 70.27 | 86.08 | 14.616 | 2.80–9.07 | <0.00001 |
| Table IIMultivariable logistic regression
analyses to predict peritoneal dissemination. |
Table II
Multivariable logistic regression
analyses to predict peritoneal dissemination.
| Biomarker | SD | P-value | OR | 95% CI |
|---|
| CA19-9 | 0.7805 | 0.8300 | 0.84 | 0.18–3.89 |
| CA125 | 0.8553 | 0.0086 | 9.43 | 1.76–50.45 |
| Type IV
collagen | 0.5306 | <0.0001 | 15.66 | 5.53–44.31 |
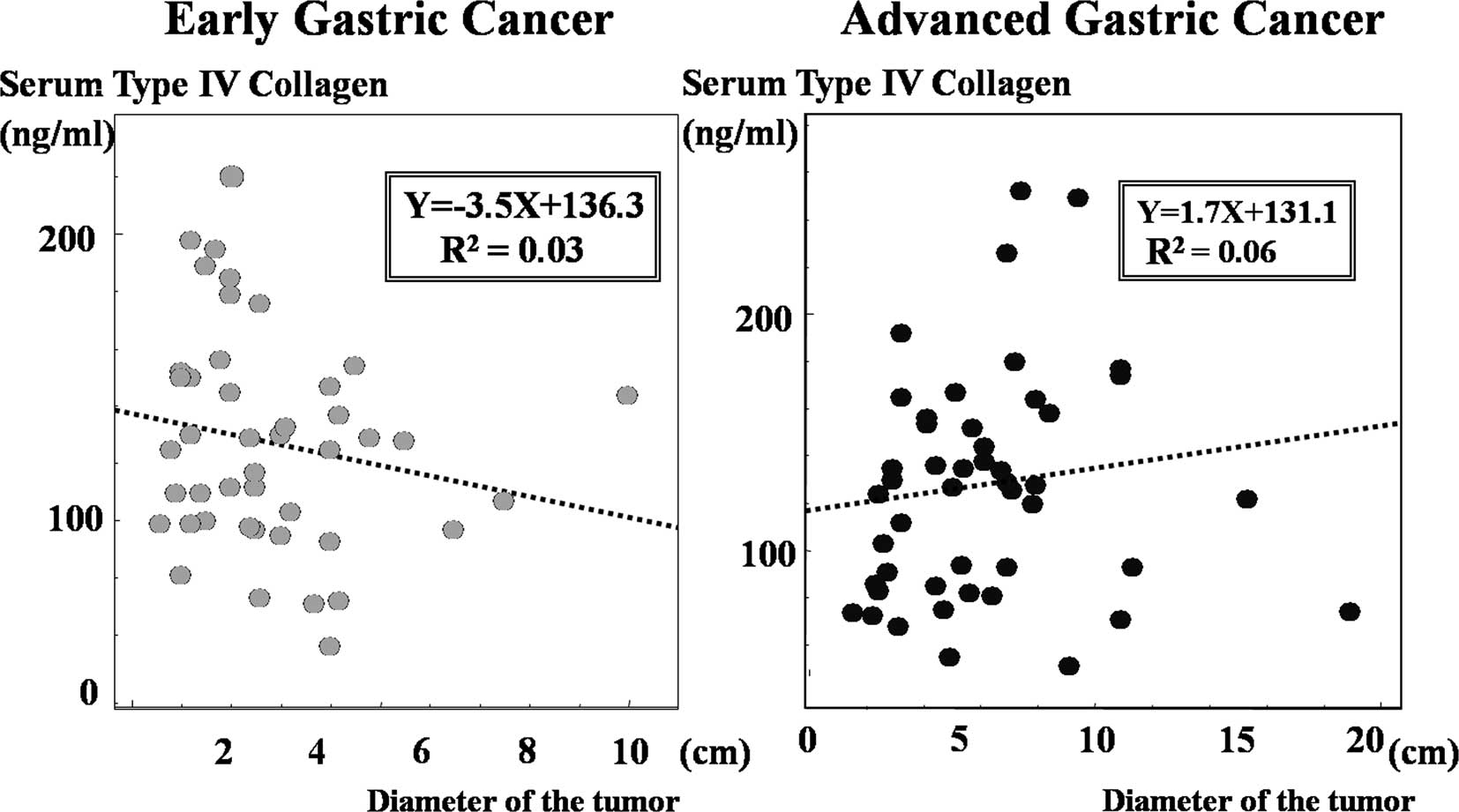
Association between type IV collagen and
the size of the primary tumor
The correlation between the size of the primary
tumor and serum type IV collagen levels in patients with early and
advanced gastric cancer was analysed. As shown in Fig. 5, no correlations were found between
the size of the primary tumor and serum type IV collagen levels
with coefficients (R2) of 0.03 in early gastric cancer
and 0.06 in advanced gastric cancer.
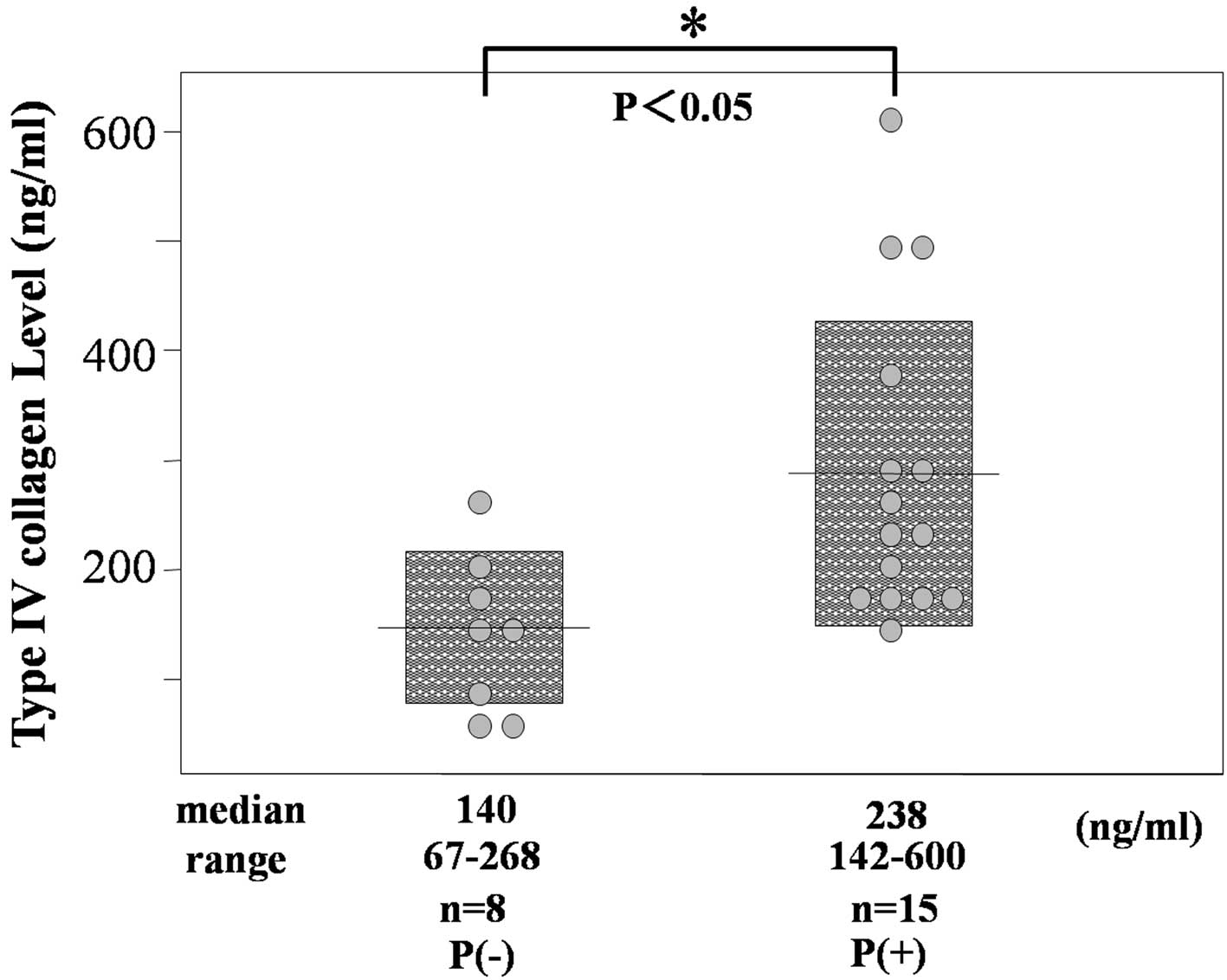
Type IV collagen in patients with
scirrhous gastric cancer
The serum type IV collagen levels were measured in
patients with scirrhous gastric carcinoma, which is characterised
by increased fibrous stroma in the primary tumor (n=3). As shown in
Fig. 6, the median serum type IV
collagen level in patients with peritoneal dissemination (238
ng/ml, 142–600 ng/ml) was significantly higher than in patients
without peritoneal dissemination (140 ng/ml, 67–268 ng/ml). The
results suggested that serum type IV collagen levels are closely
related to the process of peritoneal dissemination.
Discussion
Extracellular matrix components, particularly type
III procollagen and IV collagen, have been used as indirect
fibrogenesis markers in various chronic liver diseases, such as
haemochromatosis, viral hepatitis and alcoholic liver disease.
These components are reported to be useful indicators of collagen
matrix turnover in other diseases, such as interstitial pneumonia,
cardiomyopathy, diabetic nephropathy and systemic sclerosis which
are characterised by the accumulation of collagen in the organs
(22–25). Furthermore, elevation of the
extracellular matrix components in body fluid was confirmed in
patients with carcinomas, including stomach, lung, liver, colon and
breast (26–28). Akazawa et al reported that
the serum levels of type III procollagen in scirrhous gastric
cancer patients were elevated above normal values (29). Korenaga et al also reported
that type IV collagen levels in peritoneal lavage in patients with
peritoneal dissemination of gastric cancer were significantly
higher than patients without peritoneal dissemination (30). In the present study, the serum
levels of type IV collagen were significantly higher in patients
with than in those without peritoneal dissemination. No significant
differences were found in the serum type III procollagen levels
between the two groups of patients.
The most significant criterion for tumor markers is
the sensitivity/specificity diagram ROC curve (31). The area under the ROC curve
indicates the clinical usefulness of a tumor marker, and a larger
AUC corresponds to a more favorable tumor marker. In this study,
type IV collagen had the largest AUC of the individual markers. We
used a cut-off point of 170 ng/ml for type IV collagen in the ROC
analysis. The sensitivity and negative predictive values of type IV
collagen were much higher than those of other conventional markers,
but were lower than those of CA125. Multivariate analysis indicated
that the serum type IV collagen level was an independent predictive
factor for peritoneal dissemination. To the best of our knowledge,
this is the first study of serum type IV collagen elevation in
gastric cancer patients with peritoneal dissemination.
The present study showed that CA125 is more useful
than the conventional biomarkers CEA and CA19-9. Since no
significant correlation was noted between the serum levels of type
IV collagen and CA125 and these markers were independent predictive
factors in multivariate analysis, it is possible that a combination
assay with type IV collagen and CA125 may be more useful in the
improvement of diagnostic parameters for the detection of
peritoneal dissemination.
Subsequently, we investigated whether serum type IV
collagen levels were affected by fibrosis in the primary tumor. No
correlation was found between the size of the primary tumor and
serum type IV collagen levels. Moreover type IV collagen levels
were significantly higher in patients with than in those without
peritoneal dissemination, even in cases of scirrhous gastric
cancer, which is characterised pathologically by abundant fibrous
stroma. The results suggested that the elevation of serum type IV
collagen is not affected by the primary tumor, and may be a
specific predictor of peritoneal dissemination. Although the
precise mechanism remains unclear, we speculated that such changes
in type IV collagen in reaction to peritoneal dissemination result
from the destruction of the basement membrane in the peritoneum.
Type IV collagen is a significant component of the basement
membrane, a physical barrier that prevents cancer cells from
invading the underlying stroma (32,33).
Previous studies supported the importance of increased proteolytic
degradation of the extracellular matrix composed of interstitial
matrix and basement membrane in the process of tumor invasion and
metastasis (32–36).
Matrix metalloproteinases (MMPs) are a family of
highly conserved zinc-and calcium-dependent extracellular enzymes
involved in the modification of the extracellular matrix (34–36). A
number of studies demonstrated enhanced the tissue expression of
MMP2 and 9. These MMPs are known to degrade type IV collagen and
gelatine in the basement membrane in a number of malignant tumors
(37–39). With regard to peritoneal
dissemination, it was reported that the up-regulation of MMP2 in
ovarian cancer cells is critical for their adhesion to the
mesothelial lining of the peritoneum and omentum (40). In addition, Sun et al
reported that type IV collagenase (MMP2/9) activity was increased
in malignant ascites, including gastric cancer (41). Given these findings, it was
speculated that the presence of type IV collagen in serum is
related to the destruction of the basement membrane during the
process of metastasis. On the other hand, type III procollagen,
which is a type of fibrillar collagen, is present particularly in
tissues exhibiting elastic properties, such as skin and blood
vessels, and is identified in the fibrous stroma in the primary
tumors of gastric cancer (42). It
appears likely that type III procollagen is less affected by the
destruction of the basement membrane in this situation.
The present study suggested that an analysis of the
type IV collagen level improves diagnostic accuracy in cases of
peritoneal dissemination in gastric cancer. Laparoscopic
examination may be performed prior to chemotherapy in patients with
suspected peritoneal dissemination detected based on serum type IV
collagen level. Therefore, the appropriate treatment may be
selected to maximise the benefit of therapy at the time of
exploration. In conclusion, the serum type IV collagen level is a
potentially useful novel biomarker for the peritoneal dissemination
of gastric cancer. Studies in larger numbers of patients using
repeated measurements of type IV collagen should be performed in
order to evaluate the prognostic value of this procedure for
peritoneal dissemination in gastric cancer.
References
|
1
|
Parkin DM, Pisani P and Ferlay J: Global
cancer statistics. CA Cancer J Clin. 49:33–64. 1999. View Article : Google Scholar
|
|
2
|
Yamazaki H, Oshima A, Murakami R, Endoh S
and Ubukata T: A long-term follow-up study of patients with gastric
cancer detected by mass screening. Cancer. 63:613–617. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ikeguchi M, Yamamoto O and Kaibara N:
Management protocol for scirrhous gastric cancer. In Vivo.
18:577–580. 2004.PubMed/NCBI
|
|
4
|
Chen CY, Wu CW, Lo SS, Hsieh MC, Lui WY
and Shen KH: Peritoneal carcinomatosis and lymph node metastasis
are prognostic indicators in patients with Borrmann type IV gastric
carcinoma. Hepatogastroenterology. 49:874–877. 2002.PubMed/NCBI
|
|
5
|
Van Cutsem E, Moiseyenko VM, Tjulandin S,
Majlis A, Constenla M, Boni C, Rodrigues A, Fodor M, Chao Y, Voznyi
E, Risse ML and Ajani JA; V325 Study Group. Phase III study of
docetaxel and cisplatin plus fluorouracil compared with cisplatin
and fluorouracil as first-line therapy for advanced gastric cancer:
a report of the V325 Study Group. J Clin Oncol. 24:4991–4997.
2006.PubMed/NCBI
|
|
6
|
Glehen O, Mohamed F and Gilly FN:
Peritoneal carcinomatosis from digestive tract cancer: new
management by cytoreductive surgery and intraperitoneal
chemohyperthermia. Lancet Oncol. 5:219–228. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ishigami H, Kitayama J, Kaisaki S,
Hidemura A, Kato M, Otani K, Kamei T, Soma D, Miyato H, Yamashita H
and Nagawa H: Phase II study of weekly intravenous and
intraperitoneal paclitaxel combined with S-1 for advanced gastric
cancer with peritoneal metastasis. Ann Oncol. 21:67–70. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fushida S, Kinoshita J, Yagi Y, Funaki H,
Kinami S, Ninomiya I, Fujimura T, Nishimura G, Kayahara M and Ohta
T: Dual anti-cancer effects of weekly intraperitoneal docetaxel in
treatment of advanced gastric cancer patients with peritoneal
carcinomatosis: a feasibility and pharmacokinetic study. Oncol Rep.
19:1305–1310. 2008.
|
|
9
|
Yoshida K, Ninomiya M, Takakura N,
Hirabayashi N, Takiyama W, Sato Y, Todo S, Terashima M, Gotoh M,
Sakamoto J and Nishiyama M: Phase II study of docetaxel and S-1
combination therapy for advanced or recurrent gastric cancer. Clin
Cancer Res. 12:3402–3407. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Burke EC, Karpeh MS, Conlon KC and Brennan
MF: Laparoscopy in the management of gastric adenocarcinoma. Ann
Surg. 225:262–267. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gretschel S, Siegel R, Estévez-Schwarz L,
Hünerbein M, Schneider U and Schlag PM: Surgical strategies for
gastric cancer with synchronous peritoneal carcinomatosis. Br J
Surg. 93:1530–1535. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sendler A, Dittler HJ, Feussner H, Nekarda
H, Bollschweiler E, Fink U, Helmberger H, Höfler H and Siewert JR:
Preoperative staging of gastric cancer as precondition for
multimodal treatment. World J Surg. 19:501–508. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Davies J, Chalmers AG, Sue-Ling HM, May J,
Miller GV, Martin IG and Johnston D: Spiral computed tomography and
operative staging of gastric carcinoma: a comparison with
histopathological staging. Gut. 41:314–319. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Düx M, Richter GM, Hansmann J, Kuntz C and
Kauffmann GW: Helical hydro-CT for diagnosis and staging of gastric
carcinoma. J Comput Assist Tomogr. 23:913–922. 1999.PubMed/NCBI
|
|
15
|
Yang QM, Bando E, Kawamura T, Tsukiyama G,
Nemoto M, Yonemura Y and Furukawa H: The diagnostic value of PET-CT
for peritoneal dissemination of abdominal malignancies. Gan To
Kagaku Ryoho. 33:1817–1821. 2006.PubMed/NCBI
|
|
16
|
Nakata B, Hirakawa YS, Chung K, Kato Y,
Yamashita Y, Maeda K and Onoda N: Serum CA 125 level as a predictor
of peritoneal dissemination in patients with gastric carcinoma.
Cancer. 83:2488–2492. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yashiro M, Chung YS, Nishimura S, Inoue T
and Sowa M: Fibrosis in the peritoneum induced by scirrhous gastric
cancer cells may act as ‘soil’ for peritoneal dissemination.
Cancer. 77:1668–1675. 1996.PubMed/NCBI
|
|
18
|
Gabrielli GB and Corrocher R: Hepatic
fibrosis and its serum markers. Dig Dis. 9:303–316. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yamada S, Suou T, Kawasaki H and Yoshikawa
N: Clinical significance of serum 7S collagen in various liver
diseases. Clin Biochem. 25:467–470. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jeffers LJ, Coelho-Little ME, Cheinquer H,
Vargas C, Civantos F and Alvarez L: Procollagen-III peptide and
chronic viral C hepatitis. Am J Gastroenterol. 90:1437–1440.
1995.PubMed/NCBI
|
|
21
|
Japanese Research Society for Gastric
Cancer. The General Rules for the Gastric Cancer Study. 12th
edition. Kanehara Shuppan; Tokyo: 1993
|
|
22
|
Kasuga I, Yonemaru M, Kiyokawa H, Ichinose
Y and Toyama K: Clinical evaluation of serum type IV collagen 7S in
idiopathic pulmonary fibrosis. Respirology. 1:277–281. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sato Y, Kataoka K, Matsumori A, Sasayama
S, Yamada T and Ito H: Measuring serum aminoterminal type III
procollagen peptide, 7S domain of type IV collagen, and cardiac
troponin T in patients with idiopathic dilated cardiomyopathy and
secondary cardiomyopathy. Heart. 78:505–508. 1997. View Article : Google Scholar
|
|
24
|
Guseva NG, Anikina NV, Myllylä R, Risteli
L, Risteli J and Chochlova JV: Markers of collagen and basement
membrane metabolism in sera of patients with progressive systemic
sclerosis. Ann Rheum Dis. 50:481–486. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xu X, Wu Z, Zhou Q, Zhang Y and Wu D: The
role of determining the levels of serum collagen type IV in
diagnosing early diabetic nephropathy. Ren Fail. 24:747–753. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Katayama M, Hino F, Kamihagi K, Sekiguchi
K, Titani K and Kato I: Urinary fibronectin fragments (a potential
tumor marker) measured by immunoenzymometric assay with
domain-specific monoclonal antibodies. Clin Chem. 37:466–471.
1991.
|
|
27
|
Basso D, Belluco C, Mazza S, Greco E,
Della Rocca F, Pauletto P, Nitti D, Lise M and Plebani M:
Colorectal cancer metastatic phenotype stimulates production by
fibroblasts of N-terminal peptide of type III collagen: clinical
implications for prognosis. Clin Chim Acta. 312:135–142. 2001.
View Article : Google Scholar
|
|
28
|
Mazouni C, Arun B, André F, Ayers M,
Krishnamurthy S, Wang B, Hortobagyi GN, Buzdar AU and Pusztai L:
Collagen IV levels are elevated in the serum of patients with
primary breast cancer compared to healthy volunteers. Br J Cancer.
99:68–71. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Akazawa S, Fujiki T, Kanda Y, Kumai R and
Yoshida S: Diagnostic values of serum type III procollagen
N-terminal peptide in type IV gastric cancer. Gan To Kagaku Ryoho.
12:861–866. 1985.PubMed/NCBI
|
|
30
|
Korenaga D, Orita H, Maekawa S, Itasaka H,
Ikeda T and Sugimachi K: Peritoneal collagen type IV concentration
in adenocarcinoma of the gastrointestinal tract and its
relationship to histological differentiation, metastasis, and
survival. Surg Today. 28:780–786. 1998. View Article : Google Scholar
|
|
31
|
Baker SG: The central role of receiver
operating characteristic (ROC) curves in evaluating tests for the
early detection of cancer. J Natl Cancer Inst. 95:511–515. 2003.
View Article : Google Scholar
|
|
32
|
Martinez-Hernandez A and Amenta PS: The
basement membrane in pathology. Lab Invest. 48:656–677. 1983.
|
|
33
|
Liotta LA: Tumor invasion and metastases –
role of the extracellular matrix. Cancer Res. 46:1–7. 1986.
|
|
34
|
Meyer T and Hart IR: Mechanisms of tumor
metastasis. Eur J Cancer. 34:214–221. 1998. View Article : Google Scholar
|
|
35
|
Conway JG, Trexler SJ, Wakefield JA,
Marron BE, Emerson DL and Bickett DM: Effect of matrix
metalloproteinase inhibitors on tumor growth and spontaneous
metastasis. Clin Exp Metastasis. 14:115–124. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Heppner KJ, Matrisian LM, Jensen RA and
Rodgers WH: Expression of most matrix metalloproteinase family
members in breast cancer represents a tumor-induced host response.
Am J Pathol. 149:273–282. 1996.PubMed/NCBI
|
|
37
|
Mori M, Mimori K, Shiraishi T, Fujie T,
Baba K, Kusumoto H, Haraguchi M, Ueo H and Akiyoshi T: Analysis of
MT1-MMP and MMP2 expression in human gastric cancers. Int J Cancer.
74:316–321. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
De Mingo M, Morán A, Sánchez-Pernaute A,
Iniesta P, Díez-Valladares L, Pérez-Aguirre E, de Juan C,
García-Aranda C, Díaz-López A, García-Botella A, Martín-Antona E,
Benito M, Torres A and Balibrea JL: Expression of MMP-9 and TIMP-1
as prognostic markers in gastric carcinoma. Hepatogastroenterology.
54:315–319. 2007.PubMed/NCBI
|
|
39
|
Duffy MJ, Maguire TM, Hill A, McDermott E
and O’Higgins N: Metalloproteinases: role in breast carcinogenesis,
invasion and metastasis. Breast Cancer Res. 2:252–257. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kenny HA, Kaur S, Coussens LM and Lengyel
E: The initial steps of ovarian cancer cell metastasis are mediated
by MMP-2 cleavage of vitronectin and fibronectin. J Clin Invest.
118:1367–1379. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sun XM, Dong WG, Yu BP, Luo HS and Yu JP:
Detection of type IV collagenase activity in malignant ascites.
World J Gastroenterol. 9:2592–2595. 2003.PubMed/NCBI
|
|
42
|
Minamoto T, Ooi A, Okada Y, Mai M, Nagai Y
and Nakanishi I: Desmoplastic reaction of gastric carcinoma: a
light-and electron-microscopic immunohistochemical analysis using
collagen type-specific antibodies. Hum Pathol. 19:815–821. 1998.
View Article : Google Scholar
|