Introduction
Colorectal carcinoma is one of the leading causes of
cancer-related death in Western Europe and the US (1). Post-surgical TNM staging is a
prognostic factor that is able to predict the clinical course of
this neoplasia, with 5-year survival rates decreasing concomitantly
to stage (2,3). For this reason, TNM staging is taken
into consideration in the therapeutic protocols applied to
colorectal cancer patients. Thus, stage I colorectal carcinoma is
treated by surgery alone, with adjuvant chemotherapy being the
choice of treatment in order to improve the survival of patients
affected by higher stage carcinomas. Nevertheless, in certain
instances TNM staging appears only to express the anatomic extent
of the neoplasia with no evidence of correlation with patient
survival (4). At present,
histoprognostic factors able to predict progression-free and
overall survival of colorectal cancer in order to select patients
for adjuvant therapies are not available. Thus, factors predicting
progression risk, in addition to the currently used
clinicalpathological staging system, are required.
Neutrophil gelatinase-associated lipocalin (NGAL) is
also known as NRL (neu-related lipocalin), oncogene 24p3,
uterocalin and lipocalin 2. It is a 25-kDa protein that is stored
in the granules of human neutrophils (5). Additionally, it belongs to the
lipocalin family which consists of more than 50 members, all of
which are characterized by the ability to bind and transport small
lipophilic substances (6). NGAL was
shown to be involved in iron trafficking (7) and to increase the cytoplasmic levels
of this mineral (8) by capturing
and transporting the iron particles to the inner cell following
interaction with specific membrane receptors (24p3, megalin). Its
role in the delivery of iron to the cells underlies the multiple
effects attributed to NGAL. Since it is released by activated
neutrophils, this protein is involved in the iron depletion
strategy exploited in immune defense against bacterial pathogens
(9). Furthermore, NGAL appears to
be involved in the growth, development and differentiation of a
number of human tissues, as early as in the embryo, via its
regulation of iron-responsive genes which are crucial in the
differentiation of primordial cells (10,11).
Since NGAL synthesis is induced by factors promoting
the development of neoplasias (6,11,12),
it was suggested that this protein plays a role in the
carcinogenesis and progression of human tumors (11). Accordingly, its overexpression has
been found in various types of cancer, including colorectal
(13–16). The role of NGAL in colorectal cancer
progression (18) is evident due to
the existence of a significant association between a high NGAL mRNA
quantity and nodal metastases or advanced stage of this neoplasia
(17). In addition, the induction
of NGAL overexpression has been shown to decrease cell-cell
adhesion, enhance cell-matrix attachment and increase cell motility
and in vitro invasion in colorectal cancer cell lines
(18). Subsequently, this study
aimed to evaluate whether progression-free survival may differ on
the basis of NGAL expression in colorectal cancer and whether this
expression is a predictor of disease progression in this
neoplasia.
Materials and methods
Materials
A total of 64 consecutive cases of surgically
resected colorectal carcinomas, procured from an equal number of
patients (29 female and 35 male patients; age range 36–89 years;
mean age 68.09±12.19), were obtained from the files of the
Department of Human Pathology of the University of Messina, Italy.
None of the patients had received pre-operative chemotherapy for
their neoplasia or had colonic carcinoma in situ. Complete
tumor resection had been achieved in all cases (R0). A total of 41
cases were located at the left colon (including rectum and sigma),
while 23 were located at the right colon (including caecum,
ascendant and transversus). Histological grade was established
according to the World Health Organization classification system
criteria; specifically, 24 cases were grade 1, 36 grade 2, while 4
cases were grade 3. Of all patients at the time of diagnosis, 20
had lymph nodes and 12 had liver metastases, with 5 of the latter
being submitted to surgical resection for their metastases.
Follow-up data, including information regarding progression-free
survival, were available in all 64 cases. None of the patients with
stage I cancer had been treated with adjuvant chemotherapy, while 3
out of 11 patients with stage II colorectal cancer had received
chemotherapy (5-fluorouracil plus folinic acid) as had all the
patients with stage III or IV cancers.
Methods
All 64 cases were formalin-fixed and
paraffin-embedded. For each case, 4-μm sections were cut from the
corresponding paraffin block for subsequent immunohistochemical
study.
Briefly, the endogenous peroxidase activity was
blocked with 0.1% H2O2 in methanol for 20
min. Normal sheep serum was then applied for 30 min to prevent
non-specific adherence of serum proteins. Sections were
sequentially incubated at 4°C overnight with the primary antibody
against NGAL (Santa Cruz Biotechnology, Santa Cruz, CA, USA;
1:100). The bound primary antibody was visualized using the Dako
EnVision peroxidase detection system (Dako Cytomation, Glostrup,
Denmark), according to the manufacturer’s instructions. For
immunostaining, the sections were incubated in the dark for 10 min
with 3,3′-diaminobenzidine tetra hydrochloride (Sigma Chemical Co.,
St. Louis, MO, USA), with the amount of 100 mg in 200 ml 0.03%
hydrogen peroxide in phosphate-buffered saline (PBS). Nuclear
counterstaining was performed by Mayer’s haemalum. The binding
specificity was assessed by omitting the primary antiserum or
replacing it with normal rabbit serum or PBS (pH 7.4). Proximal
tubules within samples of normal renal parenchyma were used as
positive controls for the immunoreactions (15,19).
Assessment of the immunostained section was
performed by two independent pathologists, who were blinded to the
clinicopathological data. NGAL expression was based on the presence
of cytoplasmic and membranous staining. The intensity of staining
(IS) was graded as negative (0), weak (1), moderate (2) and strong
(3). The area of staining positivity (ASP), recorded as a
percentage of neoplastic positive cells, was assessed using the
values: 0 (<10%), 1 (11–25%), 2 (26–50%), 3 (51–75%) and 4
(>75%), according to the procedure previously described
(16,21). An intensity distribution (ID) score
was then generated for each case by multiplying the values of IS
and ASP. Cases with an ID score of 0 were considered to be negative
for NGAL.
For the statistical analyses, samples were
subdivided into negative and positive tumors, according to the
median NGAL ID score, which was 0. Moreover, when only positive
cases were considered, low (ID score 1–2) and high (ID score >2)
NGAL expression was defined on the basis of the median ID score of
this subgroup (median ID score 2).
Statistical analysis
Fisher’s exact and Chi-square tests were performed
to assess the statistical correlations between NGAL expression and
various clinicopathological characteristics, such as age, gender or
the site, histological grade, depth of infiltration (T), presence
of nodal (N) or distant metastases (M), as well as tumor stage.
Progression-free survival was assessed by the
Kaplan-Meier method, with the date of primary surgery as the entry
data. The end point was characterized as the length of survival to
recurrent (local or distant) disease. The Mantel-Cox log-rank test
was applied to assess the strength of association between survival
time and each of the patient characteristics (age, gender,
chemotherapeutic treatment, site, histological grade, TNM stage and
NGAL immunoexpression of the tumor) as a single variable.
Concomitantly, a multivariate analysis (Cox regression model) was
utilised to determine the independent effect of each significant
variable.
P<0.05 was considered to be statistically
significant. Data were analysed using the SPSS package version
6.1.3 (SPSS Inc., Chicago, IL, USA).
Results
Table I shows the
clinicopathological and immunohistochemical data related to the 64
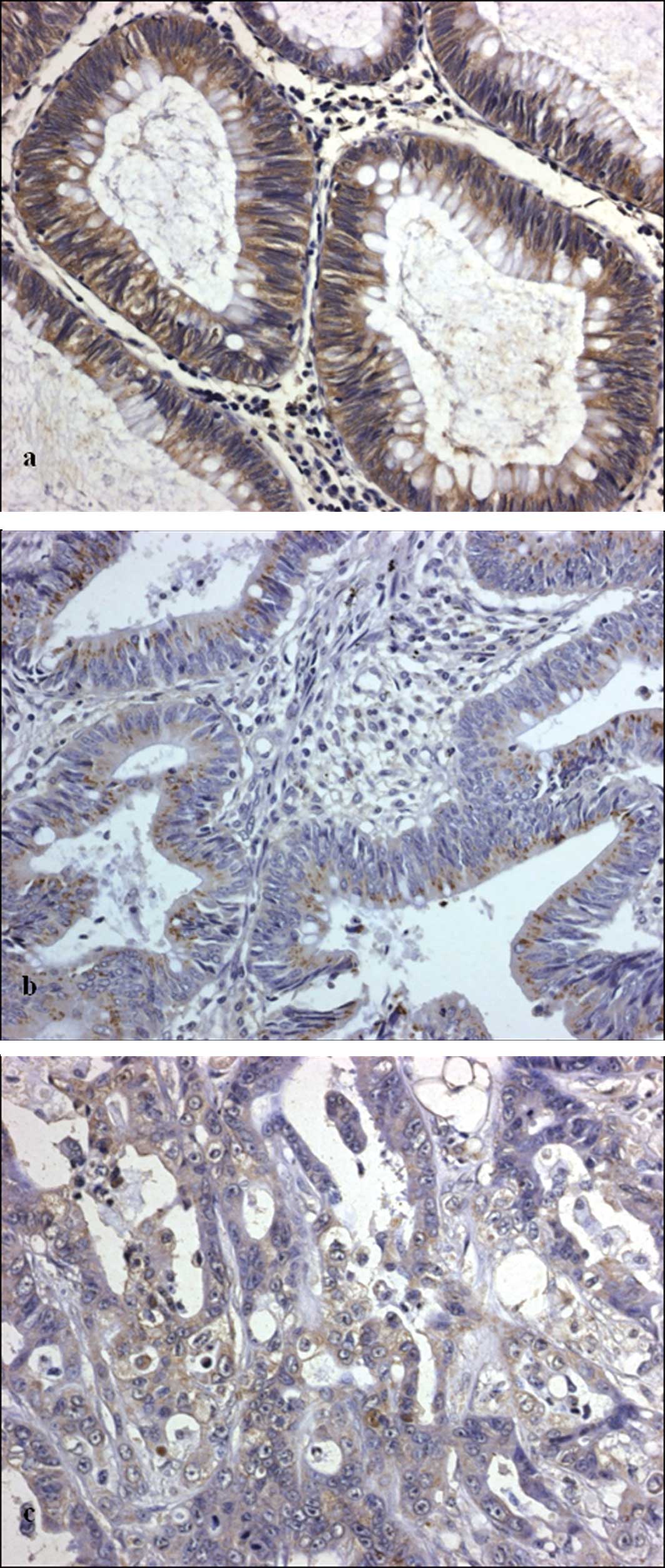
analyzed colorectal carcinomas. NGAL immunoexpression was found in
24 cases with variable ID scores. Immunostaining was present within
the cytoplasm of the neoplastic cells (Fig. 1), whereas no immunolabelling was
evident in the normal epithelium adjacent to the tumor. In
addition, in positive cases immunoreactivity was always evident at
the invasive front of the neoplasm.
 | Table IClinico-pathological characteristics
and NGAL immunohistochemical expression in 64 colorectal
carcinomas. |
Table I
Clinico-pathological characteristics
and NGAL immunohistochemical expression in 64 colorectal
carcinomas.
| Case | Age | Gender | Site | Grade | T | N | M | Stage | NGAL ID score | Recurrence | Progression-free
survival | Chemotherapy |
|---|
| 1 | 63 | M | Left colon | 3 | 2 | 0 | 0 | 1 | 0 | None | 106 | None |
| 2 | 76 | F | Right colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 105 | None |
| 3 | 86 | F | Left colon | 1 | 1 | 0 | 0 | 1 | 1 | None | 62 | None |
| 4 | 62 | M | Left colon | 1 | 2 | 0 | 0 | 1 | 0 | None | 96 | None |
| 5 | 58 | M | Left colon | 1 | 2 | 0 | 0 | 1 | 0 | None | 116 | None |
| 6 | 71 | M | Right colon | 1 | 2 | 0 | 0 | 1 | 0 | None | 88 | None |
| 7 | 55 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 74 | None |
| 8 | 75 | M | Right colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 86 | None |
| 9 | 62 | M | Right colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 65 | None |
| 10 | 79 | F | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 78 | None |
| 11 | 83 | F | Right colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 75 | None |
| 12 | 61 | F | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 61 | None |
| 13 | 62 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 2 | None | 89 | None |
| 14 | 76 | F | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 90 | None |
| 15 | 64 | F | Left colon | 2 | 2 | 0 | 0 | 1 | 2 | None | 90 | None |
| 16 | 70 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 82 | None |
| 17 | 79 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 93 | None |
| 18 | 63 | F | Right colon | 3 | 2 | 0 | 0 | 1 | 0 | None | 77 | None |
| 19 | 74 | M | Right colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 98 | None |
| 20 | 85 | F | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 65 | None |
| 21 | 53 | F | Right colon | 2 | 2 | 0 | 0 | 1 | 1 | None | 110 | None |
| 22 | 65 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 106 | None |
| 23 | 86 | M | Right colon | 2 | 1 | 0 | 0 | 1 | 0 | None | 112 | None |
| 24 | 69 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 117 | None |
| 25 | 66 | F | Right colon | 1 | 2 | 0 | 0 | 1 | 1 | Distant | 48 | None |
| 26 | 89 | F | Right colon | 1 | 2 | 0 | 0 | 1 | 2 | Distant | 30 | None |
| 27 | 71 | F | Right colon | 2 | 2 | 0 | 0 | 1 | 1 | Distant | 32 | None |
| 28 | 72 | M | Left colon | 2 | 2 | 0 | 0 | 1 | 0 | None | 106 | None |
| 29 | 47 | M | Right colon | 3 | 3 | 0 | 0 | 2 | 4 | Distant | 22 | None |
| 30 | 71 | M | Right colon | 2 | 4 | 0 | 0 | 2 | 0 | None | 84 | Yes |
| 31 | 81 | F | Right colon | 2 | 3 | 0 | 0 | 2 | 0 | None | 44 | None |
| 32 | 65 | M | Left colon | 2 | 4 | 0 | 0 | 2 | 2 | Local | 54 | None |
| 33 | 76 | M | Left colon | 3 | 3 | 0 | 0 | 2 | 0 | Distant | 32 | None |
| 34 | 37 | F | Left colon | 1 | 4 | 0 | 0 | 2 | 0 | None | 61 | Yes |
| 35 | 54 | F | Left colon | 2 | 4 | 0 | 0 | 2 | 1 | Distant | 20 | Yes |
| 36 | 86 | M | Left colon | 2 | 3 | 0 | 0 | 2 | 0 | Distant | 10 | None |
| 37 | 52 | F | Left colon | 2 | 3 | 0 | 0 | 2 | 1 | None | 60 | None |
| 38 | 82 | M | Left colon | 2 | 3 | 0 | 0 | 2 | 0 | Distant | 10 | None |
| 39 | 76 | M | Left colon | 2 | 3 | 0 | 0 | 2 | 4 | None | 35 | None |
| 40 | 64 | M | Right colon | 1 | 3 | 1 | 0 | 3 | 0 | Distant | 30 | Yes |
| 41 | 71 | F | Left colon | 2 | 2 | 1 | 0 | 3 | 0 | Distant | 12 | Yes |
| 42 | 88 | F | Left colon | 1 | 3 | 1 | 0 | 3 | 4 | Distant | 46 | Yes |
| 43 | 71 | M | Right colon | 2 | 3 | 1 | 0 | 3 | 0 | Distant | 58 | Yes |
| 44 | 63 | F | Left colon | 2 | 3 | 1 | 0 | 3 | 2 | None | 26 | Yes |
| 45 | 81 | F | Right colon | 1 | 2 | 1 | 0 | 3 | 1 | Distant | 34 | Yes |
| 46 | 36 | F | Left colon | 1 | 4 | 1 | 0 | 3 | 0 | None | 61 | Yes |
| 47 | 73 | M | Left colon | 1 | 4 | 1 | 0 | 3 | 1 | None | 76 | Yes |
| 48 | 68 | F | Left colon | 1 | 3 | 1 | 0 | 3 | 0 | None | 95 | Yes |
| 49 | 75 | M | Left colon | 3 | 4 | 1 | 0 | 3 | 0 | Distant | 20 | Yes |
| 50 | 46 | F | Right colon | 2 | 2 | 1 | 0 | 3 | 2 | Distant | 14 | Yes |
| 51 | 80 | M | Left colon | 2 | 2 | 1 | 0 | 3 | 1 | None | 78 | Yes |
| 52 | 75 | M | Left colon | 2 | 4 | 1 | 0 | 3 | 0 | Distant | 36 | Yes |
| 53 | 61 | M | Right colon | 1 | 4 | 1 | 1 | 4 | 2 | Distant | 25 | Yes |
| 54 | 77 | M | Left colon | 1 | 3 | 0 | 1 | 4 | 0 | Distant | 36 | Yes |
| 55 | 50 | F | Left colon | 1 | 4 | 1 | 1 | 4 | 0 | Distant | 24 | Yes |
| 56 | 63 | F | Left colon | 2 | 4 | 0 | 1 | 4 | 1 | Distant | 4 | Yes |
| 57 | 73 | M | Right colon | 2 | 3 | 1 | 1 | 4 | 0 | Distant | 14 | Yes |
| 58 | 78 | F | Left colon | 2 | 4 | 0 | 1 | 4 | 4 | None | 61 | Yes |
| 59 | 71 | F | Left colon | 2 | 3 | 1 | 1 | 4 | 1 | Distant | 29 | Yes |
| 60 | 62 | M | Left colon | 2 | 2 | 1 | 1 | 4 | 3 | None | 106 | Yes |
| 61 | 68 | M | Left colon | 2 | 3 | 1 | 1 | 4 | 0 | None | 80 | Yes |
| 62 | 42 | F | Left colon | 2 | 4 | 0 | 1 | 4 | 0 | None | 104 | Yes |
| 63 | 60 | M | Right colon | 3 | 4 | 1 | 1 | 4 | 0 | None | 76 | Yes |
| 64 | 60 | M | Right colon | 1 | 2 | 0 | 1 | 4 | 8 | Distant | 40 | Yes |
No significant associations were found between NGAL
presence and the various clinicopathological characteristics
(Table II), but when only positive
cases were examined, a significant association emerged between a
high NGAL expression (ID score >2) and the presence of distant
metastases at the initial diagnosis (P=0.017) or high TNM stage
(P=0.039) (Table III).
| Table IIStatistical correlations between the
NGAL immuno-expression and the various clinicopathological
characteristics in 24 NGAL-positive colorectal carcinomas. |
Table II
Statistical correlations between the
NGAL immuno-expression and the various clinicopathological
characteristics in 24 NGAL-positive colorectal carcinomas.
| NGAL ID score | |
|---|
|
| |
|---|
| 1–2 | >2 | P-value |
|---|
| Gender | | | 0.192 |
| M | 6 | 4 | |
| F | 12 | 2 | |
| Age | | | 0.665 |
| <70 years | 11 | 3 | |
| >70 years | 7 | 3 | |
| Site | | | 1.000 |
| Left colon | 11 | 4 | |
| Right colon | 7 | 2 | |
| Grade | | | 0.201 |
| 1 | 6 | 2 | |
| 2 | 12 | 3 | |
| 3 | 0 | 1 | |
| T | | | 0.418 |
| 1 | 1 | 0 | |
| 2 | 9 | 2 | |
| 3 | 3 | 3 | |
| 4 | 5 | 1 | |
| N | | | 1.000 |
| 0 | 11 | 4 | |
| 1–2 | 7 | 2 | |
| M | | | 0.017 |
| 0 | 16 | 2 | |
| 1 | 2 | 4 | |
| Stage | | | 0.039 |
| 1 | 7 | 0 | |
| 2 | 3 | 1 | |
| 3 | 6 | 1 | |
| 4 | 2 | 4 | |
| Table IIIStatistical correlations between NGAL
immuno-expression and the various clinicopathological
characteristics of the 64 analyzed colorectal carcinomas.a |
Table III
Statistical correlations between NGAL
immuno-expression and the various clinicopathological
characteristics of the 64 analyzed colorectal carcinomas.a
| NGAL ID score | |
|---|
|
| |
|---|
| 0 | >0 | P-value |
|---|
| Gender | | | 0.066 |
| M | 27 | 10 | |
| F | 13 | 14 | |
| Age | | | 0.438 |
| <70 years | 18 | 14 | |
| >70 years | 22 | 10 | |
| Site | | | 1.000 |
| Left colon | 26 | 15 | |
| Right colon | 14 | 9 | |
| Grade | | | 0.055 |
| 1 | 9 | 8 | |
| 2 | 26 | 5 | |
| 3 | 5 | 1 | |
| T | | | 0.932 |
| 1 | 1 | 1 | |
| 2 | 21 | 11 | |
| 3 | 10 | 6 | |
| 4 | 8 | 6 | |
| N | | | 0.419 |
| 0 | 29 | 15 | |
| 1–2 | 11 | 9 | |
| M | | | 1.000 |
| 0 | 30 | 18 | |
| 1 | 10 | 6 | |
| Stage | | | 0.201 |
| 1 | 21 | 7 | |
| 2 | 4 | 4 | |
| 3 | 5 | 7 | |
| 4 | 10 | 6 | |
Post-surgical follow-up ranged between 4 and 117
months. During the follow-up, 24 out of 64 patients developed
recurrent disease, with distant metastases in 23 cases and local
recurrence in 1 case. Patients who died of independent disease and
those with no evidence of disease progression (3/64) were censored.
A total of 23 out of 24 patients with recurrent disease died of
disease progression. Univariate survival analyses revealed TNM
stage, depth of infiltration, nodal metastases, chemotherapy and
NGAL immunoexpression to be significant prognostic factors for
progression-free survival (Table
IV). In particular, the length of survival to recurrent disease
was significantly shorter in those patients with a colorectal
carcinoma characterized by a high NGAL expression (P=0.0305)
(Table IV). Nevertheless, the
multivariate analysis suggested that NGAL expression was not an
independent prognostic factor, whereas the application of
chemotherapy was found to be an independent variable as compared to
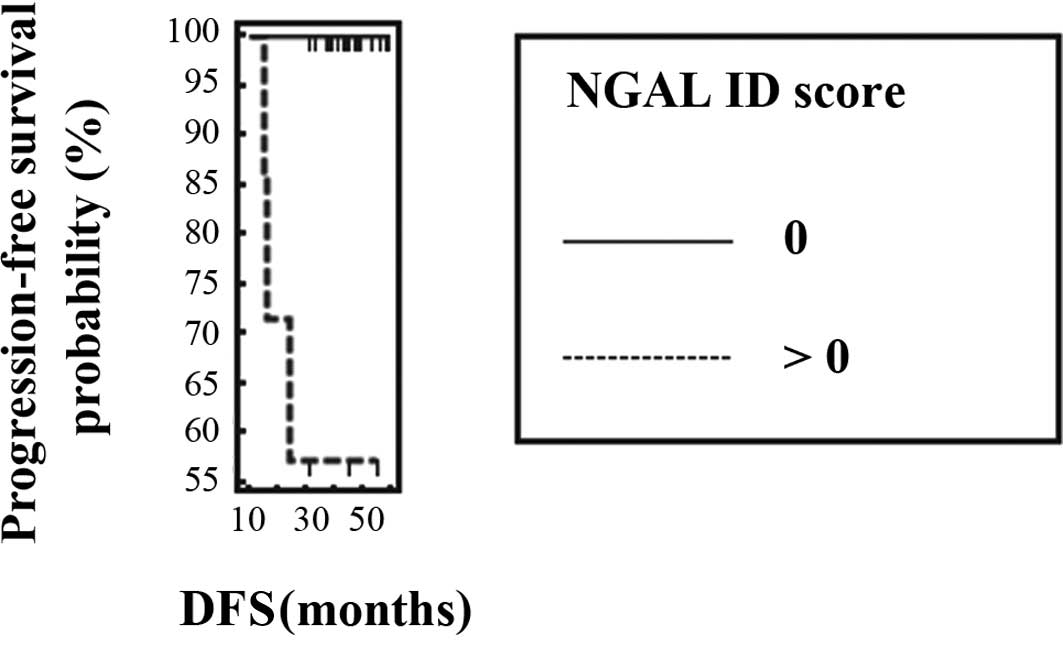
progression-free survival of patients (Table IV). When the prognostic value of
NGAL expression was specifically investigated according to the TNM
stage, the expression of this protein was evidenced as a negative
prognostic factor that correlated with a shorter progression-free
survival in stage I (P=0.001) (Fig.
2), but not in colorectal carcinomas of higher stages (Table V).
| Table IVUnivariate and multivariate analyses
for progression-free survival in 64 patients affected by colorectal
carcinoma. |
Table IV
Univariate and multivariate analyses
for progression-free survival in 64 patients affected by colorectal
carcinoma.
| A, Univariate
analysis. |
|---|
|
|---|
| Charateristics | χ2 | Df | P-value |
|---|
| Age | 0.9862 | 1 | 0.3207 |
| Gender | 0 | 1 | 0.9935 |
| Site | 1.1595 | 1 | 0.2816 |
| Grade | 2.2580 | 2 | 0.3234 |
| T | 9.1260 | 3 | 0.0088 |
| N | 7.3205 | 1 | 0.0068 |
| M | 3.3093 | 1 | 0.0689 |
| Stage | 16.2523 | 3 | 0.0010 |
| Chemotherapy | 8.8210 | 1 | 0.0030 |
| NGAL
immunoexpression | 4.6795 | 1 | 0.0305 |
|
| B, Multivariate
analysis. |
|
| Variable | β | SE | Exp (β) | P-value |
| Chemotherapy | 1.2116 | 0.4348 | 3 | 0.005 |
| Table VNGAL univariate analysis for
progression-free survival according to TNM staging of 64 colorectal
carcinomas. |
Table V
NGAL univariate analysis for
progression-free survival according to TNM staging of 64 colorectal
carcinomas.
| Univariate analysis
(Characteristic: NGAL expression) | χ2 | Df | P-value |
|---|
| Stage |
| I | 10.5775 | 1 | 0.0011 |
| II | 0.0079 | 1 | 0.9290 |
| III | 0.2400 | 1 | 0.6242 |
| IV | 0.1811 | 1 | 0.6704 |
Discussion
NGAL overexpression and correlation with disease
progression has been shown in malignancies of the gastro-intestinal
tract, including esophageal, gastric and colorectal carcinomas
(17,21,22).
We investigated for the first time the relationship between NGAL
prognostic value and progression-free survival of colorectal
carcinoma. In particular, NGAL immunohistochemical expression was
evaluated in a series of 64 colorectal carcinomas of different
stages and correlated with the various clinicopathological
characteristics, as well as with progression-free survival of the
patients.
A variable NGAL expression was found in 24 out of 64
cases. In accordance with previous reports (16–18),
NGAL immunoexpression was found in the neoplastic cells of positive
cases, but not in the adjacent normal epithelium, in line with its
suggestive role in colorectal carcinogenesis. Immunostaining was
localized at the cytoplasm of the neoplastic cells, as in the case
of breast cancer (13). This
localization suggests NGAL internalization to the inner cell
following its binding to membrane receptors. Since NGAL is involved
in iron uptake, we hypothesize that NGAL expression and cytoplasmic
localization reflect augmented iron requirement by the neoplastic
elements of colorectal carcinoma, as previously described (18). Notably, NGAL appears to play a role
in carcinogenesis by promoting iron uptake from the extracellular
space within the malignant cells, a fundamental process for the
maintenance of neoplastic cell multiplication (14,23).
Besides, it is well-known that iron overload promotes
carcinogenesis through the induction of oxidative DNA damage
(24), whereas iron depletion leads
to cell cycle arrest and apoptosis (25).
Notably, NGAL staining was mainly observed in the
invasive front of the tumor in positive cases. This may be related
to its ability to increase the invasive potential of tumor cells.
Studies have shown that NGAL forms a complex with matrix
metalloproteinase-9 (MMP-9), preventing MMP-9 degradation and
resulting in increased MMP-9 enzyme activity in vitro
(26). MMP-9 plays a role in cancer
progression by degrading the molecular components of the basement
membrane and extracellular matrix, releasing vascular endothelial
cell growth factor (VEGF) from the extracellular matrix, and
enabling angiogenesis, invasion and distant metastasis (26–28).
Thus, NGAL may play a role in cancer progression by causing
increased MMP-9 enzymatic activity, thereby promoting the invasive
and metastatic potential of cancer cells in vivo and in
vitro (28). However, NGAL was
recently shown to increase invasiveness of colorectal cancer cells
through an MMP-9-independent process (18). It has been shown that NGAL
overexpression enhances the invasive and metastatic potential of
colon cancer cells by decreasing e-cadherin-mediated cell-cell
adhesion through an iron-dependent mechanism (18). In contrast to other authors
(17), we failed to demonstrate any
significant correlation between NGAL and the depth of infiltration
of tumors. Nevertheless, the role of NGAL in the invasiveness of
colorectal carcinoma was confirmed by a significant association
between a high NGAL expression and the presence of distant
metastases or a high TNM stage at the time of initial diagnosis of
the analyzed colorectal carcinomas. Notably, NGAL involvement in
the development of metastases had previously been hypothesized,
since inhibition of this protein results in the blockage of lung
metastases from breast carcinoma (29).
NGAL overexpression was previously considered to be
a negative prognostic factor in colorectal cancer due to its
significant association with the presence of adverse factors, such
as lymph node metastases or venous invasion (17). However, its impact on specific
survival in relation to neoplasia has yet to be investigated. Our
results showed that patients with tumors characterized by NGAL
immunohistochemical expression exhibited a significantly shorter
progression-free survival in comparison to patients with absent
NGAL staining. Thus, NGAL appears to act as a negative prognostic
factor for colorectal cancer, as in the case of breast cancer
(13). Notably, when the
relationship between NGAL predictive value and disease-progression
risk was evaluated according to the TNM stage of neoplasias, the
presence of NGAL appeared to be a significant predictor of
progression risk in stage I colorectal carcinoma, but not in the
remaining TNM stages. Only the former group of patients had not
been submitted to chemotherapy, which emerged as an independent
prognostic factor for progression-free survival in our cohort.
In conclusion, the present study showed that NGAL
immunoexpression is a negative prognostic marker associated with
shorter disease-specific survival in stage I colorectal carcinomas.
If our findings are confirmed on larger cohorts of stage I
colorectal carcinomas, NGAL assessment in colon cancer tissue may
be used as a prognostic tool to determine tumors with a higher
progression risk, so that selected patients may undergo adjuvant
treatments in order to prevent adverse outcome. Moreover, the
inhibition of NGAL expression or function may represent the target
for novel therapeutic strategies in order to prevent disease
progression in NGAL-positive colorectal carcinomas. Colorectal
carcinomas showing NGAL expression may benefit from therapies with
iron chelators as anti-cancer agents. Notably, since iron
deprivation caused by iron chelators inhibits cell proliferation,
iron and its corresponding transport proteins have become new
targets in cancer therapy (30,31).
Finally, since the efficacy of anti-NGAL antibodies has been shown
by blocking cancer metastasis in mice (29), NGAL expression and involvement in
colorectal cancer progression and metastatic disease may be
exploited for such novel anti-cancer therapies.
References
|
1
|
Landis H, Murray T, Bolden S and Wingo PA:
Cancer statistics. Cancer J Clin. 49:8–31. 1999.
|
|
2
|
Wiggers T, Arends JW, Schutter B, Volovics
L and Bosman FT: A multivariate analysis of pathologic prognostic
indicators in large bowel cancer. Cancer. 61:386–389. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wu XC, Chen VW, Steele B, Ruiz B, Fulton
J, Liu L, Carozza SE and Greenlee R: Subsite-specific incidence
rate and stage of disease in colorectal cancer by race, gender, and
age group. Cancer. 92:2547–2554. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Di Gregorio C, Benfatti P, Losi L,
Roncucci L, Rossi G, Ponti G, Marino M, Pedroni M, Scarselli A,
Roncari B and Ponz de Leon M: Incidence and survival of patients
with Dukes’ A (stages T1 and T2) colorectal carcinoma: a 15-year
population-based study. Int J Colorectal Dis. 20:147–154. 2005.
|
|
5
|
Cowland JB and Borregaard N: Molecular
characterization and pattern of tissue expression of the gene for
neutrophil gelatinase-associated lipocalin from humans. Genomics.
45:17–23. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bratt T: Lipocalins and cancer. Biochim
Biophys Acta. 1482:318–326. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang J, Goetz D, Li JY, Wang W, Mori K and
Setlik D: An iron delivery pathway mediated by a lipocalin. Mol
Cell. 10:1045–1056. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Goetz DH, Willie ST, Arme RS, Bratt T,
Borregaard N and Strong RK: Ligand preference inferred from the
structure of neutrophil gelatinase associated lipocalin.
Biochemistry. 39:1935–1941. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Goetz DH, Holmes MA, Borregaard N, Bluhm
ME, Raymond KN and Strong RK: The neutrophil lipocalin NGAL is a
bacteriostatic agent that interferes with siderophore-mediated iron
acquisition. Mol Cell. 10:1033–1043. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gwira JA, Wei F, Ishibe S, Ueland JM,
Barasch J and Cantley LG: Expression of neutrophil
associated-gelatinase lipocalin regulates epithelial morphogenesis
in vitro. J Biol Chem. 280:7875–7882. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bolignano D, Donato V, Lacquaniti A, et
al: Neutrophil gelatinase-associated lipocalin (NGAL) in human
neoplasias: a new protein enters the scene. Cancer Lett. 288:10–16.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hannai J, Mammoto T, Seth P, Mori K,
Karumanchi SA, Barasch J and Sukhatme VP: Lipocalin 2 diminishes
invasiveness and metastasis of Ras-transformed cells. J Biol Chem.
280:3641–3647. 2005.PubMed/NCBI
|
|
13
|
Bauer M, Eickhoff JC, Gould MN, Mundhenke
C, Maas N and Friedl A: Neutrophil gelatinase-associated lipocalin
(NGAL) is a predictor of poor prognosis in human primary breast
cancer. Breast Cancer Res Treat. 108:389–397. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Iannetti A, Pacifico F, Acquaviva R, et
al: The neutrophil gelatinase-associated lipocalin (NGAL), a
NF-kappaB-regulated gene, is a survival factor for thyroid
neoplastic cells. Proc Natl Acad Sci USA. 105:14058–14063. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Barresi V, Ieni A, Bolignano D, Magno C,
Buemi M and Barresi G: Neutrophil gelatinase-associated lipocalin
immunoexpression in renal tumors: correlation with histotype and
histological grade. Oncol Rep. 24:305–310. 2010. View Article : Google Scholar
|
|
16
|
Nielsen BS, Borregaard N, Bundgaard JR,
Timshel S, Sehested M and Kjeldsen L: Induction of NGAL synthesis
in epithelial cells of human colorectal neoplasia and inflammatory
bowel diseases. Gut. 38:414–420. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhang XF, Zhang Y, Zhang XH, Zhou SM, Yang
GG, Wang OC, Guo GL, Yang GY and Hu XQ: Clinical significance of
Neutrophil gelatinase-associated lipocalin (NGAL) expression in
primary rectal cancer. BMC Cancer. 91:342009.PubMed/NCBI
|
|
18
|
Hu L, Hittelman W, Lu T, Ji P, Arlinghaus
R, Shmulevich I, Hamilton SR and Zhang W: NGAL decreases
E-cadherin-mediated cell-cell adhesion and increases cell motility
and invasion through Rac1 in colon carcinoma cells. Lab Invest.
89:531–548. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Friedl A, Stoesz SP, Buckley P and Gould
MN: Neutrophil gelatinase-associated lipocalin in normal and
neoplastic human tissues. Cell type-specific pattern of expression.
Histochem J. 31:433–441. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Moniaux N, Chakraborty S, Yalniz M, et al:
Early diagnosis of pancreatic cancer: neutrophil
gelatinase-associated lipocalin as a marker of pancreatic
intraepithelial neoplasia. Br J Cancer. 98:1540–1547. 2008.
View Article : Google Scholar
|
|
21
|
Kubben FJ, Sier CF, Hawinkels LJ, et al:
Clinical evidence for a protective role of lipocalin-2 against
MMP-9 autodegradation and the impact for gastric cancer. Eur J
Cancer. 43:1869–1876. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang H, Xu L, Xiao D, et al: Upregulation
of neutrophil gelatinase-associated lipocalin in oesophageal
squamous cell carcinoma: significant correlation with cell
differentiation and tumour invasion. J Clin Pathol. 60:555–561.
2007. View Article : Google Scholar
|
|
23
|
Devireddy LR, Gazin C, Zhu X and Green MR:
A cell-surface receptor for lipocalin 24p3 selectively mediates
apoptosis and iron uptake. Cell. 23:1293–1305. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Toyokuni S: Role of iron in
carcinogenesis: cancer as a ferrotoxic disease. Cancer Sci.
100:9–16. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Le NTV and Richardson DN: The role of iron
in cell cycle progression and the proliferation of neoplastic
cells. Biochim Biophys Acta. 1603:31462002.
|
|
26
|
Fernandez CA, Yan L, Louis G, Yang J,
Kutok JL and Moses MA: The matrix metallo-proteinase-9/neutrophil
gelatinase associated lipocalin complex plays a role in breast
tumor growth and is present in the urine of breast cancer patients.
Clin Cancer Res. 11:5390–5395. 2005. View Article : Google Scholar
|
|
27
|
Lee S, Jilani SM, Nikolova GV, Carpizo D
and Iruela-Arispe M: Processing of VEGF-A by matrix
metalloproteinases regulates bioavailability and vascular
patterning in tumors. J Cell Biol. 169:681–691. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yan L, Borregaard N, Kjeldsen L and Moses
MA: The high molecular weight urinary matrix metalloproteinase
(MMP) activity is a complex of gelatinase B/MMP-9 and neutrophil
gelatinase-associated lipocalin (NGAL). Modulation of MMP-9
activity by NGAL. J Biol Chem. 276:37258–37265. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Leng X, Ding T, Lin H, et al: Inhibition
of lipocalin 2 impairs breast tumorigenesis and metastasis. Cancer
Res. 69:8579–8784. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Buss JL, Greene BT, Turner J, Torti FM and
Torti SV: Iron chelators in cancer chemotherapy. Curr Top Med Chem.
4:1623–1635. 2004. View Article : Google Scholar
|
|
31
|
Jones DT, Trowbridge IS and Harris AL:
Effects of transferrin receptor blockade on cancer cell
proliferation and hypoxia-inducible factor function and their
differential regulation by ascorbate. Cancer Res. 66:2749–2756.
2006. View Article : Google Scholar : PubMed/NCBI
|