Introduction
Colorectal cancer (CRC) is one of the most common
neoplasms in elderly patients. Currently, the median age at
diagnosis of colorectal cancer in the United States is 72 years, in
Europe 74 years, and in Japan, the late 60s (1). The incidence of colorectal cancer
increases with age. As the world’s population is aging, providing
optimal care for elderly patients with CRC is highly relevant.
Findings of a previous study showed that making
three active drugs (5-FU, irinotecan and oxaliplatin) available to
any patient with advanced CRC who is a candidate for such therapy
maximizes overall survival (OS) (2). In the metastatic setting, the case for
the benefits of chemotherapy is compelling as CRC survival without
treatment is only 6 months, exceeding 20 months for patients
treated with chemotherapy with combination regimens, such as
FOLFOX, FOLFIRI and XELOX, and currently exceeding 24 months when
chemotherapy is supple-mented with biological agents, such as
bevacitumab, cetuximab and panitumumab (3). However, the use of palliative
chemotherapy for metastatic CRC (mCRC) also appears to decline with
patient age. Although 70% of patients younger than 70 receive some
chemotherapy for metastatic CRC, only 43% of patients older than 70
receive palliative chemotherapy (4).
Aging is often associated with physiological,
sociological and psychological changes. One of the hallmarks of
aging is gradual loss of physiologic reserve involving loss of the
body’s ability to compensate when exposed to stressors such as
infection, cancer and chemotherapy (5,6).
Declining reserves results in a gradual decline in normal organ
function. For example, glomerular filtration rate, cardiac
motility, hepatic volume, and blood flow all decline with age, as
does immunologic and hematologic function (7,8). Each
of these changes has the potential to increase the risk and
decrease the tolerance to adverse effects from chemotherapeutics.
Therefore, elderly patients presenting with CRC are often
under-represented or excluded from clinical trials. Occasionally,
selected elderly patients have been treated with chemotherapy in
clinical trials. These selected elderly patients have few
comorbidities, given their excellent performance status and organ
function (9). To address this
issue, multiple pooled analyses and meta-analyses have been
conducted, all of which have concluded that the efficacy and
toxicity of CRC chemotherapy among younger and older patients who
were in good health and were willing to enroll in clinical trials
were essentially equivalent.
In 2001, a pooled analysis of seven trials randomly
assigning patients to fluorouracil (FU) with leucovorin (LV) or
levamizole versus observation in an adjuvant setting found no
association between age and the effect of treatment on disease-free
survival or OS, suggesting equal efficacy of chemotherapy in the
elderly (10). Combination
chemotherapy also appears to be beneficial in healthy older
patients. Results of pooled analyses of both oxaliplatin-and
irinotecan-based regimens have been found to be the same as those
of FU trials (11–13). In contrast, in a smaller phase III
trial that compared weekly versus every-third-week irinotecan,
patients >70 years of age had significantly increased odds of
suffering grade 3 or 4 diarrhea and neutropenia than younger
patients (14). Thus, the extent to
which older patients treated with irinotecan have an increased risk
of toxicity warrants further investigation. Given the current
evidence, the use of oxaliplatin-and irinotecan-based regimens
(FOLFOX, FOLFIRI and XELOX) as first-line chemotherapy in healthy
elderly patients may be feasible.
However, data concerning the effect of three active
cytotoxic agents on OS and safety in elderly patients are not yet
available. Additionally, no data from clinical trials are currently
available regarding chemotherapy using first-line FOLFOX4 followed
by second-line FOLFIRI in elderly patients. Therefore, we analyzed
retrospectively and reported the results of the tolerance and
efficacy of second-line FOLFIRI for mCRC in elderly patients
treated at the Cancer Institute Hospital of the Japanese Foundation
for Cancer Research.
Patients and methods
Patients
Data were collected retrospectively from medical
records available from 35 patients treated at the Cancer Institute
Hospital of the Japanese Foundation for Cancer Research. Our
analysis of outcome data included all patients over 70 years of age
treated with second-line FOLFIRI from March 2005 to January 2008
following first-line FOLFOX4 failure for mCRC. All patients had
histologically confirmed colorectal adenocarcinoma.
Treatment plan
The chemotherapy regimens used were first-line
FOLFOX4 (LV 200 mg/m2/day as a 2-h infusion followed by
bolus 5-FU 400 mg/m2/day and a 22-h 5-FU infusion of 600
mg/m2/day, repeated for 2 consecutive days every 2
weeks; 85 mg/m2 of oxaliplatin was administered on day 1
as a 2-h infusion concurrent with LV) and second-line FOLFIRI (LV
200 mg/m2/day as a 2-h infusion followed by bolus 5-FU
400 mg/m2/day and a 46-h 5-FU infusion of 2400
mg/m2/day, every 2 weeks; 150 mg/m2 of
irinotecan was administered on day 1 as a 1.5-h infusion concurrent
with LV).
According to evidence-based medicine, treatment was
continued until disease progression or unacceptable toxicity
occurred or until the patient chose to discontinue treatment.
Evaluation of efficacy and toxicity
Patients were evaluated for adverse events prior to
each cycle and graded according to NCI Common Toxicity Criteria
(version 3.0). When measurable, tumor response was assessed using
computed tomography (CT) approximately every 3 months according to
the Response Evaluation Criteria in Solid Tumors criteria (RECIST)
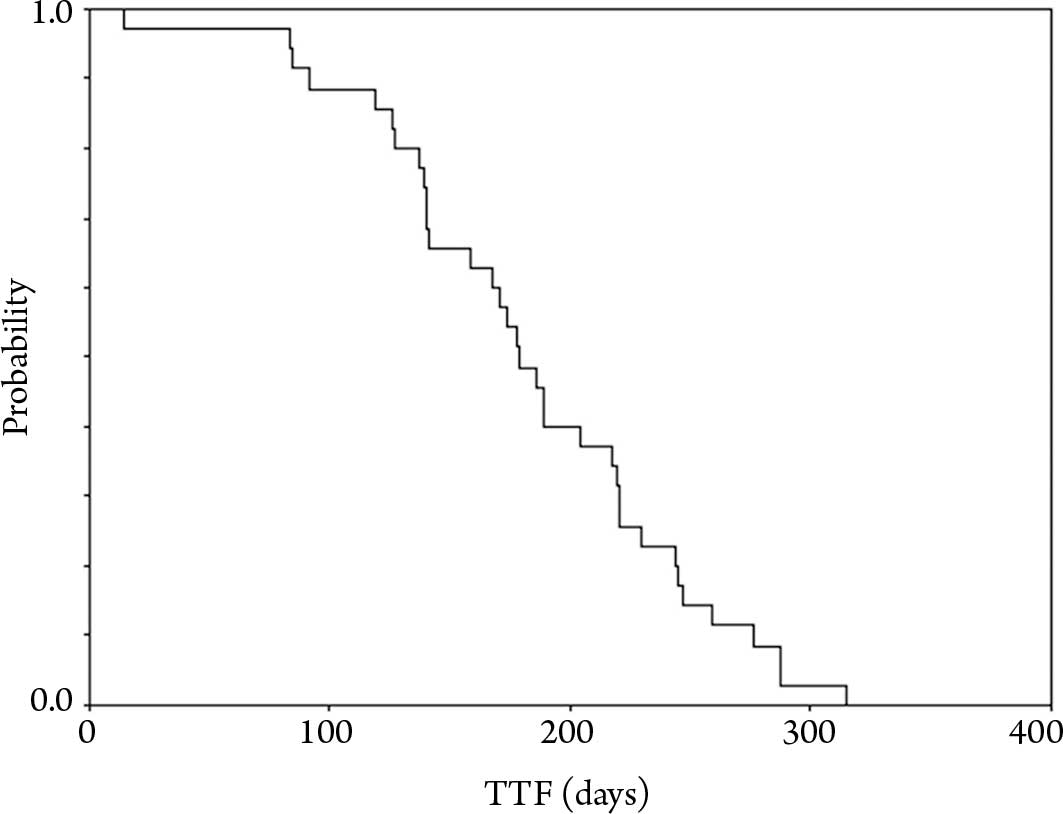
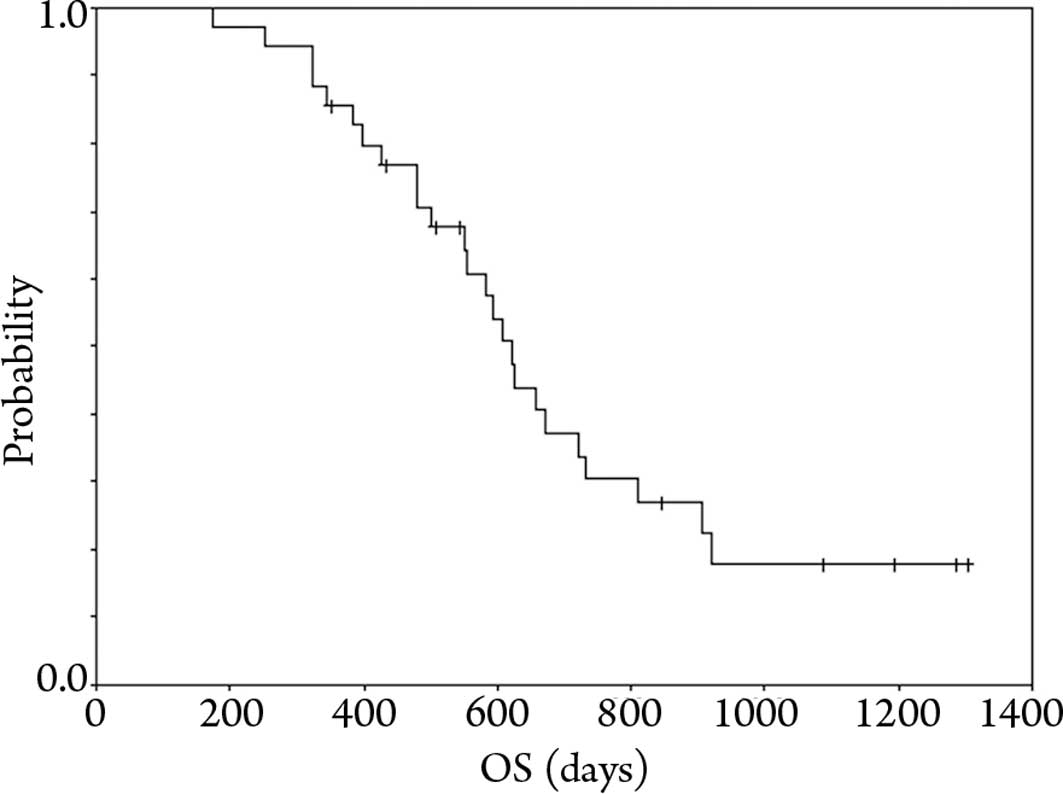
(15). Treatment outcome was
determined by OS and time to treatment failure (TTF). OS was
calculated from the beginning of first-line chemotherapy until
documentation of death. TTF was defined as the time from the
beginning of second-line chemotherapy to the progression or failure
of treatment or the patient succumbing due to any cause.
Statistical analysis
OS and TTF were calculated using the Kaplan-Meier
method. Multivariate logistic regression stepwise models were used
to explore the correlation between the incidence of severe
hematological toxicity (grade 3 and 4 neutropenia) and age, gender,
Eastern Cooperative Oncology Group (ECOG) performance status (PS),
comorbidity, number of first-line FOLFOX4 cycles received, number
of metastatic locations, relative dose intensity values in
second-line FOLFIRI and presence of adjuvant treatment. Data were
analyzed using the SPSS package version 17.0 (SPSS Inc., Chicago,
IL) and two-sided P<0.05 were considered to be statistically
significant.
Results
Patient characteristics
Patient characteristics are shown in Table I. The median age was 74 years (range
71–77). All 35 patients had a favorable ECOG PS of 0 or 1. Eleven
patients were metastatic at the time of diagnosis. The main
metastatic locations were the liver (63%), lung (63%), and lymph
nodes (57%). A total of 18 patients received prior adjuvant
FU-based chemotherapy. In total, 19 patients (54%) experienced
comorbidity, mainly hypertension, diabetes, ulcer disease or
another type of cancer. Comorbidity was present in 11 (31%)
patients when using the Charlson comorbidity index (CCI) (Charlson
et al, 1987). All 35 patients received FOLFOX4 regimen as
the first-line treatment. A total of 394 cycles of treatment with
FOLFOX4 regimen were administered, with a median of 10 cycles per
patient (range 5–26 cycles). The efficacy and toxicity in the
patients receiving first-line FOLFOX4 are listed in Table II.
 | Table IBaseline characteristics at the
beginning of second-line chemotherapy. |
Table I
Baseline characteristics at the
beginning of second-line chemotherapy.
| Characteristics | No. of patients |
|---|
| Total no. of
patients | 35 |
| Age (years) |
| Median | 74 |
| Range | 71–77 |
| Gender |
| Male | 18 (51.4%) |
| Female | 17 (48.6%) |
| ECOG performance
status |
| 0 | 23 (65.7%) |
| 1 | 12 (34.3%) |
| Primary tumor
site |
| Colon | 21 (60%) |
| Rectum | 14 (40%) |
| Number of metastatic
sites |
| 1 | 9 (25.7%) |
| >1 | 26 (74.3%) |
| Adjuvant
chemotherapy |
| Yes | 16 (45.7%) |
| No | 19 (54.3%) |
| Charlson comorbidity
index |
| 0 | 24 (68.6%) |
| 1 | 9 (25.7%) |
| 2 | 2 (5.7%) |
| Clinical history |
| Hypertension | 11 (31.4%) |
| Diabetes
mellitus | 1 (2.8%) |
| Thromboembolic
disease | 1 (2.8%) |
| Heart disease | 2 (5.7%) |
| Another cancer | 3 (8.6%) |
| Table IIEfficacy and toxicities in first-line
FOLFOX4. |
Table II
Efficacy and toxicities in first-line
FOLFOX4.
| First-line result, %
(95% CI) |
| Objective response
rate | 31.4
(16.1–46.7%) |
| Disease control
rate | 62.8
(46.8–78.8%) |
| Median PFS in
months | 6.0 (5.4–6.5) |
| Range | 2.8–10.5 |
| Reasons for
discontinuing treatment, (n, %) |
| Disease
progression | 25 (71.4) |
| Neurotoxicity | 3 (8.6) |
| Allergy | 7 (20.0) |
| Hematological
toxicity (grade ≥3), (n, %) |
| Leukopenia | 4 (11.4) |
| Neutropenia | 20 (57.1) |
| Anemia | 1 (2.8) |
| Febrile
neutropenia | 1 (2.8) |
Treatment duration of FOLFIRI
A total of 279 cycles of treatment were
administered, with a median of 5 cycles per patients (range 2–37
cycles). Nine patients (26%) required a dose reduction, usually for
hematologic toxicity (78%). Seven patients started with a lower
dose (irinotecan 120 mg/m2, bolus 5-FU 320
mg/m2 and 5-FU infusion 1920 mg/m2) after
undergoing a dose reduction due to hematologic toxicity with prior
chemotherapy. The median relative dose-intensity values were 81.6%
for CPT-11. Treatment was discontinued due to non-progression of
disease in 10 (29%) patients; 4 of them with worsening PS. Other
reasons for discontinuation included interstitial lung disease in 2
patients, febrile neutropenia (FN) in 3 patients (these patients
refused treatment), and treatment-related death in 1 patient. Five
patients (14%) discontinued treatment before the first evaluation
of response was performed. The reasons were interstitial lung
disease in 2 patients, FN in 2 patients, and death in 1
patient.
Toxicity of FOLFIRI
In total, 29 (83%) patients experienced grade 3 and
4 toxicity (Table III). The main
severe toxicities were neutropenia in 25 (71%) patients and
leukopenia in 16 (46%) patients. Four (11%) patients had FN.
However, these patients experienced less non-hematological
toxicity. Three (9%) patients had grade 3 mucositis, 3 (9%)
patients had grade 3 nausea and vomiting, and 2 (6%) patients had
grade 3 anorexia. Only one patient had diarrhea. There was 1
treatment-related death due to grade 3 hyponatremia. No patient
experienced worsening comorbidity.
| Table IIIMost common drug-related adverse
events in FOLFIRI. |
Table III
Most common drug-related adverse
events in FOLFIRI.
| Grade ≥3
toxicity | No. | % |
|---|
| Any drug-related
adverse event | 29 | 82.8 |
| Neutropenia | 25 | 71.4 |
| Leukopenia | 16 | 45.7 |
| Anemia | 1 | 2.8 |
| Febrile
neutropenia | 4 | 11.4 |
| Infection | 1 | 2.8 |
| Diarrhea | 1 | 2.8 |
|
Nausea/Vomiting | 3 | 8.6 |
| Anorexia | 1 | 2.8 |
| Mucositis | 3 | 8.6 |
| Hepatic
toxicity | 1 | 2.8 |
In an exploratory multivariate analysis, the
presence of severe neutropenia (grade 3 and 4) in first-line
FOLFOX4 was associated with a significant increase in the presence
of grade 3 and 4 neutropenia in second-line FOLFIRI (P=0.049,
Table IV). However, no significant
correlation was observed between the presence of grade 3 and 4
neutropenia in second-line FOLFIRI and patient age (70–74 vs. ≥75
years), gender, PS (0 vs. 1), comorbidity (CCI 0 vs. ≥1), number of
first-line FOLFOX4 cycles (9 vs. >9), number of metastatic
locations (1 vs. >1), relative dose intensity values in
second-line FOLFIRI (<80 vs. ≥80) or presence of adjuvant
treatment (yes vs. no).
| Table IVMultivariate analysis of the
association between severe neutropenia in second-line FOLFIRI and
patient characteristics. |
Table IV
Multivariate analysis of the
association between severe neutropenia in second-line FOLFIRI and
patient characteristics.
| Outcome | Estimate | SE | OR | 95% CI | P-value |
|---|
| Severe neutropenia
in first-line FOLFOX4 | 1.601 | 0.812 | 4.958 | 1.009–24.370 | 0.049 |
Efficacy of FOLFIRI
A total of 30 patients were considered to be
assessable for response. The best objective responses were achieved
as follows: non-complete response (CR), 1 (3.3%) partial response
(PR), 12 (40%) stable diseases (SD) and 17 (57%) treatment
failures.
Figs. 1 and 2 show the TTF in second-line FOLFIRI and
OS from the beginning of first-line chemotherapy, respectively.
After a median follow-up of 19.5 months (range 5.8–43.5) at the
time of analysis, all 35 patients experienced treatment failure,
and 25 patients succumbed to the disease. We were unable to follow
up 5 patients after their disease progression. The median TTF in
second-line FOLFIRI was 3.0 months (95% CI, 1.2–4.7 months), and
the median OS time from the commencement of the first-line
chemotherapy was 20.7 months (95% CI, 18.9–22.5 months). No
patients had undergone surgery. Among the patients who progressed
to further chemotherapy, third-line treatment was administered to 6
(17%) patients. This comprised cetuximab-based regimens in 3
patients (not assessed for KRAS mutation status) and hepatic
arterial infusion chemotherapy in 3 patients. Few patients received
third-line chemotherapy for the reason that cetuximab and
panitumunab were not approved in Japan until June 2008.
Discussion
The modern era of combination chemotherapy commenced
when it was shown that irinotecan prolonged median OS in patients
resistant to 5-FU (16). Since
then, the use of combination chemotherapy, both as first- and
second-line, has increased life expectancy by nearly two years. OS
is correlated with the percentage of patients who receive the three
agents of 5-FU, irinotecan and oxaliplatin. Consequently, the use
of first- and second-line combination chemotherapy confirms the
assumption that more patients should be exposed to the three key
drugs (2).
An oxaliplatin-based investigation pooled the
results of patients of 70 years of age or older who were treated
with oxaliplatin with infusional FU and LV (FOLFOX) for mCRC in
three clinical trials and in one adjuvant trial (11). The rate of hematologic toxicity was
statistically significantly higher in this group of older patients,
although absolute differences between the age cohorts were small.
The incidence of non-hematologic grade 3 or 4 toxicity was similar
across age groups. The results of the pooled and pre-trial analyses
showed that the response rate, disease-free survival and OS were
not affected by age. In addition, the irinotecan-based
investigation pooled data from 1484 patients, 303 (20%) of whom
were 70 years or older, in three randomized trials comparing
irinotecan/FU/LV with FU/LV in first-line therapy. No difference
was found in the response rate, time to progression, or survival
with regards to age for patients treated with FU/LV or
irinotecan/FU/LV. Additionally, no difference was noted in the
incidence of any grade 3 or 4 toxicity between age group in
patients treated with irinotecan combinations (17).
A shorter survival was noted in elderly patients
when the proportion of patients who received second-line
chemotherapy was low. Subsequently, irinotecan was not widely used
as a second-line therapy (18).
Therefore, it may be necessary to increase the proportion of
elderly to whom second-line treatment is administered following
disease progression. However, the majority of the previously
mentioned systematic reviews only include studies that evaluate
first-line palliative chemotherapy (19). Therefore, it is unclear from our
evidence whether combination second-line chemotherapy with elderly
patients is safe and efficacious.
The present study aimed to analyze the efficacy and
safety of a second-line FOLFIRI regimen (following first-line
FOLFOX4 failure) in elderly patients (≥70 years of age) with mCRC.
Our results, with a response rate of 3.3%, a median
progression-free survival (PFS) of 3.0 months, and a median OS of
20.7 months were similar to those obtained in a previous study with
first-line FOLFOX4 followed by second-line FOLFIRI that included
patients aged <70 years (22).
Our results suggest that the use of all three active drugs in mCRC
produces the longest OS in elderly patients (≥70 years) as well as
in younger ones.
However, second-line FOLFIRI regimen following
first-line FOLFOX4 may not be entirely safe. In total, 83% of the
patients experienced grade 3/4 adverse events, particularly severe
neutropenia (grade 3/4), and the incidence of FN was 71 and 11%,
respectively. A high rate of toxicity was found when compared with
the 44% (all toxicity), the 21% (severe neutropenia) and 1% (FN)
reported in a V-308 trial including younger patients (median age
was 65 years; range 40–75) (20).
On the other hand, non-hematological toxicity was similar to that
found in a previous report and was deemed acceptable. Additionally,
findings of our analysis revealed a correlation between the
presence of grade 3 and 4 neutropenia for second-line FOLFIRI and
the presence of severe neutropenia in first-line FOLFOX4. This
suggests that the toxicity of previous treatment is a prognostic
factor of tolerability with elderly patients to second-line
FOLFIRI. Baseline characteristics such as female gender, the
presence of comorbidity, and PS are normally associated with
increased toxicity (21,22). We did not find such a correlation in
this analysis. However, it is crucial to note that the power of
this report, due to the low number of unhealthy patients, may be
insufficient to detect such a correlation. In other words, even
healthy elderly patients experienced severe neutropenia at a very
high rate.
To avoid such a high rate of toxicity in a
second-line setting following FOLFOX failure, single-agent
irinotecan may be an appropriate approach in particular for elderly
patients who experience severe neutropenia in first-line treatment.
Single-agent irinotecan following fluoropyrimidine and oxaliplatin
failure has been reported to be efficacious in mCRC patients,
including the elderly (23). The
outcome, with an overall response rate (RR) of 4.2% and a median
PFS of 2.6 months was similar to our results. In elderly patients
treated with fluoropyrimidine-based chemotherapy, single-agent
irinotecan has proven to be safe in second-line therapy (severe
neutropenia 22/35% for patients <70/≥70 years) (24).
The use of biological agents has not been well
studied, even in healthy elderly patients. Cetuximab and irinotecan
were found to improve PFS and RR in patients with wild-type KRAS in
second-line treatment after fluoropyrimidine and oxaliplatin
failure (23). A single
retrospective study examined efficacy and safety of cetuximab with
irinotecan in elderly patients with mCRC (25). Neutropenia and diarrhea were more
frequent with cetuximab and irinotecan than irinotecan as a
monotherapy. Therefore, more data are needed regarding toxicity in
the elderly upon the addition of cetuximab.
Previous studies have focused on the UGT1A1
polymorphism as a determinant of irinotecan toxicity (26–28).
It has been found that patients either heterozygous or homozygous
for UGT1A1*28, a variant sequence in the promoter
region, experienced more severe toxicity to irinotecan (29). However, to ascertain whether a
reduced dose of irinotecan based on UGT1A1 polymorphism is
appropriate requires prospective evaluation. It has been suggested
that UGT1A7*3 is a marker for severe hematologic
toxicity following the first cycle and that haplotype 1 is a
predictor of severe hematologic toxicity during the entire course
of therapy (30). The issue may be
significant in treatment decision-making, particulary for elderly
patients in second-line treatment due to the high rate of
hematologic toxicity.
In conclusion, the use of all three active drugs in
mCRC produces the longest OS in elderly patients as well as younger
ones. However, second-line FOLFIRI may be toxic due to the high
rate of severe hematological toxicity in the elderly. Further
investigation is warranted in the second-line setting with elderly
patients. This investigation should include the use of biological
agents and the UGT1A polymorphisms. However, our data should be
extrapolated to the majority of elderly patients undergoing
second-line FOLFIRI with caution, even when in good health. In
addition, we suggest that further investigation is needed involving
more frail elderly patient cohorts.
Acknowledgements
The authors are grateful to Masato Ozaka, Mariko
Ogura, Mitsukuni Suenaga, Eiji Shinozaki for assisting with the
treatment of patients at the Cancer Institute Hospital.
References
|
1
|
Gatta G, Faivre J, Capocaccia R and Ponz
de Leon M: Survival of colorectal cancer patients in Europe during
the period 1978–1989. Eur J Cancer. 34:2176–2183. 1998.
|
|
2
|
Grothey A, Sargent D, Goldberg RM and
Schmoll HJ: Survival of patients with advanced colorectal cancer
improves with the availability of fluorouracil-leucovorin,
irinotecan, and oxaliplatin in the course of treatment. J Clin
Oncol. 22:1209–1214. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kelly H and Goldberg RM: Systemic therapy
for metastatic colorectal cancer: current options, current
evidence. J Clin Oncol. 23:4553–4560. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ho C, Ng K, O’Reilly S and Gill S:
Outcomes in elderly patients with advanced colorectal cancer
treated with capecitabine: a population-based analysis. Clin
Colorectal Cancer. 5:279–282. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ferrucci L, Guralnik JM, Cavazzini C,
Bandinelli S, Lauretani F, Bartali B, Repetto L and Longo DL: The
frailty syndrome: a critical issue in geriatric oncology. Crit Rev
Oncol Hematol. 46:127–137. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Walston J, Hadley EC, Ferrucci L, Guralnik
JM, Newman AB, Studenski SA, Ershler WB, Harris T and Fried LP:
Research agenda for frailty in older adults: toward a better
understanding of physiology and etiology: summary from the American
Geriatrics Society/National Institute on Aging Research Conference
on frailty in older adults. J Am Geriatr Soc. 54:991–1001. 2006.
View Article : Google Scholar
|
|
7
|
Sawhney R, Sehl M and Naeim A: Physiologic
aspects of aging: impact on cancer management and decision making,
part I. Cancer J. 11:449–460. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sehl M, Sawhney R and Naeim A: Physiologic
aspects of aging: impact on cancer management and decision making,
part II. Cancer J. 11:461–473. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Given B, Given C, Azzouz F and Stommel M:
Physical functioning of elderly cancer patients prior to diagnosis
and following initial treatment. Nurs Res. 50:222–232. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sargent DJ, Goldberg RM, Jacobson SD,
Macdonald JS, Labianca R, Haller DG, Shepherd LE, Seitz JF and
Francini G: A pooled analysis of adjuvant chemotherapy for resected
colon cancer in elderly patients. N Engl J Med. 345:1091–1097.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Goldberg RM, Tabah-Fisch I, Bleiberg H, de
Gramont A, Tournigand C, Andre T, Rothenberg ML, Green E and
Sargent DJ: Pooled analysis of safety and efficacy of oxaliplatin
plus fluorouracil/leucovorin administered bimonthly in elderly
patients with colorectal cancer. J Clin Oncol. 24:4085–4091. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sastre J, Marcuello E, Masutti B, Navarro
M, Gil S, Antón A, Abad A, Aranda E, Maurel J, Valladares M, Maestu
I, Carrato A, Vicent JM and Díaz-Rubio E; Cooperative Group for the
Treatment of Digestive Tumors. Irinotecan in combination with
fluorouracil in a 48-hour continuous infusion as first-line
chemotherapy for elderly patients with metastatic colorectal
cancer: a Spanish Cooperative Group for the Treatment of Digestive
Tumors study. J Clin Oncol. 23:3545–3551. 2005. View Article : Google Scholar
|
|
13
|
Souglakos J, Pallis A, Kakolyris S,
Mavroudis D, Androulakis N, Kouroussis C, Agelaki S, Xenidis N,
Milaki G and Georgoulias V: Combination of irinotecan (CPT-11) plus
5-fluorouracil and leucovorin (FOLFIRI regimen) as first line
treatment for elderly patients with metastatic colorectal cancer: a
phase II trial. Oncology. 69:384–390. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fuchs CS, Moore MR, Harker G, Villa L,
Rinaldi D and Hecht JR: Phase III comparison of two irinotecan
dosing regimens in second-line therapy of metastatic colorectal
cancer. J Clin Oncol. 21:807–814. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
Organization for Research and Treatment of Cancer, National Cancer
Institute of the United States, National Cancer Institute of
Canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar
|
|
16
|
Cunningham D, Pyrhönen S, James RD, Punt
CJ, Hickish TF, Heikkila R, Johannesen TB, Starkhammar H, Topham
CA, Awad L, Jacques C and Herait P: Randomised trial of irinotecan
plus supportive care versus supportive care alone after
fluorouracil failure for patients with metastatic colorectal
cancer. Lancet. 352:1413–1418. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Folprecht G, Seymour MT, Saltz L,
Douillard JY, Hecker H, Stephens RJ, Maughan TS, Van Cutsem E,
Rougier P, Mitry E, Schubert U and Köhne CH:
Irinotecan/fluorouracil combination in first-line therapy of older
and younger patients with metastatic colorectal cancer: combined
analysis of 2.691 patients in randomized controlled trials. J Clin
Oncol. 26:1443–1451. 2008. View Article : Google Scholar
|
|
18
|
Feliu J, Salud A, Escudero P, Lopez-Gómez
L, Bolanos M, Galán A, Vicent JM, Yubero A, Losa F, De Castro J, de
Mon MA, Casado E and González-Barón M: XELOX (capecitabine plus
oxaliplatin) as first-line treatment for elderly patients over 70
years of age with advanced colorectal cancer. Br J Cancer.
94:969–975. 2006.PubMed/NCBI
|
|
19
|
Au HJ, Mulder KE and Fields AL: Systematic
review of management of colorectal cancer in elderly patients. Clin
Colorectal Cancer. 3:165–171. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tournigand C, André T, Achille E, Lledo G,
Flesh M, Mery-Mignard D, Quinaux E, Couteau C, Buyse M, Ganem G,
Landi B, Colin P, Louvet C and de Gramont A: FOLFIRI followed by
FOLFOX6 or the reverse sequence in advanced colorectal cancer: a
randomized GERCOR study. J Clin Oncol. 22:229–237. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Balducci L and Extermann M: Management of
cancer in the older person: a practical approach. Oncologist.
5:224–237. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Macdonald JS: Vive la difference: gender
and fluorouracil toxicity. J Clin Oncol. 20:1439–1341. 2002.
|
|
23
|
Sobrero AF, Maurel J, Fehrenbacher L,
Scheithauer W, Abubakr YA, Lutz MP, Vega-Villegas ME, Eng C,
Steinhauer EU, Prausova J, Lenz HJ, Borg C, Middleton G, Kröning H,
Luppi G, Kisker O, Zubel A, Langer C, Kopit J and Burris HA III:
EPIC: phase III trial of cetuximab plus irinotecan after
fluoropyrimidine and oxaliplatin failure in patients with
metastatic colorectal cancer. J Clin Oncol. 26:2311–2319. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chau I, Norman AR, Cunningham D, Waters
JS, Topham C, Middleton G, Hill M, Ross PJ, Katopodis R, Stewart G
and Oates JR: Elderly patients with fluoropyrimidine and
thymidylate synthase inhibitor-resistant advanced colorectal cancer
derive similar benefit without excessive toxicity when treated with
irinotecan monotherapy. Br J Cancer. 91:1453–1458. 2004. View Article : Google Scholar
|
|
25
|
Bouchahda M, Macarulla T, Spano JP, Bachet
JB, Lledo G, Andre T, Landi B, Tabernero J, Karaboué A, Domont J,
Levi F and Rougier P: Cetuximab efficacy and safety in a
retrospective cohort of elderly patients with heavily pretreated
metastatic colorectal cancer. Crit Rev Oncol Hematol. 67:255–262.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Iyer L, Das S, Janisch L, Wen M, Ramírez
J, Karrison T, Fleming GF, Vokes EE, Schilsky RL and Ratain MJ:
UGT1A1*28 polymorphism as a determinant of irinotecan
disposition and toxicity. Pharmacogenomics J. 2:43–47. 2002.
|
|
27
|
Innocenti F, Undevia SD, Iyer L, Chen PX,
Das S, Kocherginsky M, Karrison T, Janisch L, Ramírez J, Rudin CM,
Vokes EE and Ratain MJ: Genetic variants in the
UDP-glucuronosyltransferase 1A1 gene predict the risk of severe
neutropenia of irinotecan. J Clin Oncol. 22:1382–1388. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Toffoli G, Cecchin E, Corona G, Russo A,
Buonadonna A, D’Andrea M, Pasetto LM, Pessa S, Errante D, De
Pangher V, Giusto M, Medici M, Gaion F, Sandri P, Galligioni E,
Bonura S, Boccalon M, Biason P and Frustaci S: The role of
UGT1A1*28 polymorphism in the pharmacodynamics and
pharmacokinetics of irinotecan in patients with metastatic
colorectal cancer. J Clin Oncol. 24:3061–3068. 2006.PubMed/NCBI
|
|
29
|
Ruzzo A, Graziano F, Loupakis F, Santini
D, Catalano V, Bisonni R, Ficarelli R, Fontana A, Andreoni F,
Falcone A, Canestrari E, Tonini G, Mari D, Lippe P, Pizzagalli F,
Schiavon G, Alessandroni P, Giustini L, Maltese P, Testa E,
Menichetti ET and Magnani M: Pharmacogenetic profiling in patients
with advanced colorectal cancer treated with first-line FOLFIRI
chemotherapy. Pharmacogenomics J. 8:278–288. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cecchin E, Innocenti F, D’Andrea M, Corona
G, De Mattia E, Biason P, Buonadonna A and Toffoli G: Predictive
role of the UGT1A1, UGT1A7, and UGT1A9 genetic variants and their
haplotypes on the outcome of metastatic colorectal cancer patients
treated with fluorouracil, leucovorin, and irinotecan. J Clin
Oncol. 27:457–465. 2009. View Article : Google Scholar
|