Introduction
Lung cancer is the leading cause of cancer mortality
in the world and non-small-cell lung cancer (NSCLC) accounts for
the majority of lung cancer cases (1). Epidermal growth factor
receptor-tyrosine kinase inhibitors (EGFR-TKI), including
erlotinib, are a new class of anti-cancer agents that have been
used for almost a decade (2).
Erlotinib is an orally-available quinazoline that is a selective
inhibitor of the tyrosine kinase of EGFR. Erlotinib is the first
EGFR-TKI to demonstrate an increase in survival in a phase III
trial of NSCLC patients who had failed one or two previous
chemotherapy regimens (3). Several
studies have demonstrated that the tumor tissue EGFR mutation
status may be used to predict tumor response to EGFR-TKI treatment
and also possibly predict patient survival. In addition to the
usefulness of EGFR-TKI as second-line treatment (3), recent clinical trials have also
revealed a high efficacy of EGFR-TKIs as a first-line treatment for
EGFR-mutated NSCLC, compared with platinum-based doublets, in terms
of prolongation of progression-free survival (PFS) and reduced
toxicity (4–7). Thus, the use of EGFR-TKI in treating
patients with tumor EGFR-activating mutations is gaining in
significance and is becoming a first step in decision-making when
treating patients with metastatic NSCLC. However, the best way to
find patients with tumor EGFR-activating mutations remains
undetermined (8). In addition, only
approximately 36% of lung cancer patients had adequate tissue
samples available for EGFR mutation analysis (4).
Plasma-free DNA EGFR mutation analysis is a novel
tool that provides an easy, convenient and safe way of testing
patients, and is particularly useful for those patients who do not
have or have only limited pathological specimens (9–11). In
the present study, we prospectively collected and examined the
plasma-free DNA mutation status of our lung cancer patients with
adenocarcinoma who were due to receive erlotinib treatment, to
determine whether or not this method is effective in the detection
of the EGFR mutation status and in the prediction of treatment
response and PFS.
Patients and methods
Patients
The study protocol was approved by the institutional
review board of our hospital (VGHIRB No. 98-11-05). Patients with
adenocarcinoma of the lung who were due to receive erlotinib
treatment and who had measureable lesion(s) were entered into the
present study after informed consent had been obtained. Blood
samples were collected prior to delivery of the first dose of
erlotinib.
Tumor tissue EGFR sequencing
EGFR mutation analysis was performed using
nucleotide sequence analysis. The VarientSEQrTM Resequencing Primer
Set was selected for mutational analysis of the tyrosine kinase
domain, exons 18–21 of the EGFR gene. Genomic DNA was extracted
from paraffin blocks, exons 18–21 were amplified, and uncloned
polymerase chain reaction (PCR) fragments were sequenced and
analyzed in sense and antisense directions for the presence of
heterozygous mutations. Normal control DNA, provided by Applied
Biosystems (Carlsbad, CA, USA), was used for the wild-type control.
The sequence variations were confirmed by multiple, independent PCR
amplifications and repeated sequencing reactions. EGFR-activating
mutations were defined as those with exon 19 deletions or exon 21
L858R.
Plasma sample collection, DNA extraction
and sequencing
Plasma samples were collected in EDTA tubes and
centrifuged at 1500 rpm for 5 min. DNA was extracted from 1 ml of
plasma using the High Pure Viral Nucleic Acid kit (Roche
Diagnostics, Almere, The Netherlands). The PCR reaction is based on
the peptide nucleic acid-locked nucleic acid (PNA-LNA) PCR
clamp-based test (12). Briefly,
PCR reactions were performed in a total volume of 20 μl consisting
of 10 μl 2X Master mix, 1 μm clamp primer and 0.4 μm of each
primer. Thermocycling was performed in PCR tubes. Following a
10-min activation step at 95˚C, reactions were subjected to 45
cycles of 30 sec at 95˚C, 30 sec at 60˚C and 30 sec at 72˚C. The
amplification product of the PCR clamp was purified using Shrimp
alkaline phosphatase (SAP) and Exonuclease I (EXOI) treatments, and
was then subjected to DNA sequencing using an automatic DNA
sequencer. This type of PNA-LNA PCR clamp-based test is capable of
detecting mutations, including exon 18 G719C or G719S, exon 19
deletions between E746 and S752, exon 20 T790M, and exon 21 L858R
or L861Q mutations. As with tumor tissue EGFR sequencing, only exon
19 deletions and exon 21 L858R were considered to be
EGFR-activating mutations.
Efficacy evaluation
Baseline assessments were performed within 3 weeks
prior to erlotinib treatment. A chest computed tomography scan
(including liver and adrenal glands) was performed within 3 weeks
prior to starting erlotinib treatment, 1 month and 3 months
following commencement of erlotinib treatment, and then every 3
months thereafter, or when confirmation of treatment response or
disease progression was required. Treatment response evaluation was
performed according to the Response Evaluation Criteria in Solid
Tumors (RECIST) group criteria (13). PFS was calculated from the date
erlotinib treatment commenced to the earliest sign of disease
progression, as determined by the RECIST criteria (13), or mortality from any cause. If
disease progression had not occurred at the time of the last
follow-up visit, PFS was considered to have been censored at that
time.
Statistical analysis
Survival curves were drawn using the Kaplan-Meier
product method. Comparisons were made with the log-rank test.
Hazard ratios in the overall population and in the patient subsets
were calculated using the Cox proportional hazards model. The
Chi-square test was used to compare the response rates according to
the molecular profiles. P-values were 2-sided and p<0.05 was
considered to indicate a statistically significant difference.
Statistical analyses were performed using SPSS software (SPSS Inc.,
Chicago, IL, USA).
Results
Patients and EGFR mutation analysis
A total of 54 patients who received erlotinib
treatment were enrolled in the study, including 21 males and 33
females, with a mean age of 64 years (range, 30–88). ECOG
performance status was 0 or 1 in 40 patients and ≥2 in 14 patients.
Thirty-nine patients were non-smokers and 15 were smokers.
Erlotinib treatment was the first-line treatment in 4 patients and
the second-line or later treatment in 50 patients. Forty patients
had pathological specimens available for tumor EGFR mutation
analysis; however, 10 of the 40 patients had inadequate specimens
for analysis. Thus, only 30 patients had adequate pathological
specimens for tumor EGFR sequencing. The tumor EGFR mutation
analysis of these 30 patients revealed that 15 (50%) had activating
mutations (exon 19 deletions in 5 patients, L858R mutations in 9
and exon 19 deletions + L858R mutations in 1 patient). Among the
remaining 15 patients without activating mutations, 4 had atypical
mutations (exon 18 G719C + exon 20 S768I in 1, exon 19 P733L in 1,
exon 19 E749X in 1 and exon 21 R836P in 1 patient), and 11 patients
had wild-type mutations.
All 54 patients underwent plasma-free DNA EGFR
mutation analysis prior to erlotinib treatment. Activating
mutations were found in 25 patients (46.3%) (exon 19 deletions in
18 patients, L858R in 4 and exon 19 deletions + L858R in 3) and
wild-type in 29 patients (53.7%). No atypical mutations or T790M
mutations were detected in the plasma samples. The results of the
30 patients who had tumor tissue and plasma-free DNA EGFR mutation
analysis data are shown in Table
I.
 | Table ISequencing results of 30 patients who
had tumor tissue and plasma-free DNA EGFR mutation analysis. |
Table I
Sequencing results of 30 patients who
had tumor tissue and plasma-free DNA EGFR mutation analysis.
| Tissue | Plasma |
|---|
|
|
|---|
| Exon 19 deletion | L858R | Exon 19 deletion +
L858R | Wild-type |
|---|
| Exon 19 deletion,
n=5 | 4 | 0 | 1 | 0 |
| L858R, n=9 | 0 | 2 | 4 | 3 |
| Exon 19 deletion +
L858R, n=1 | 0 | 0 | 1 | 0 |
| Atypical mutation,
n=4 | 2 | 0 | 2 | 0 |
| Wild-type, n=11 | 3 | 0 | 8 | 0 |
Treatment response
Of the 54 patients, 26 (48.1%) patients had a
partial response to erlotinib treatment, 13 (24.1%) had stable
disease with erlotinib treatment and 15 (27.8%) had progressive
disease with erlotinib treatment. The objective response rate was
86.7% (13 of 15) in patients with tumor tissue EGFR-activating
mutations and 33.3% (5 of 15) in those without (p=0.003). The
objective response rate was 68% (17 of 25) in patients with
plasma-free DNA EGFR-activating mutations and 31% (9 of 29) in
those without (p=0.013). Among the 30 patients who had tumor tissue
and plasma-free DNA EGFR data, the response rate was 100% (10 of
10) in those with tumor tissue and plasma EGFR-activating
mutations, 60% (3 of 5) in those with only tumor tissue
EGFR-activating mutations, 50% (3 of 6) in those with only plasma
EGFR-activating mutations, and 22.2% (2 of 9) in those without an
EGFR-activating mutation from either sample (p=0.007).
Progression-free survival
Median PFS was 9 months in 26 patients who had a
partial response to erlotinib treatment [censor 5, 95% confidence
interval (CI) 6.3–11.7 months], 5.4 months in 13 patients who had
stable disease with erlotinib treatment (censor 2, 95% CI 2.1–8.7
months), and 1.9 months in 15 patients who had progressive disease
with erlotinib treatment (censor 0, 95% CI 1.9–2 months)
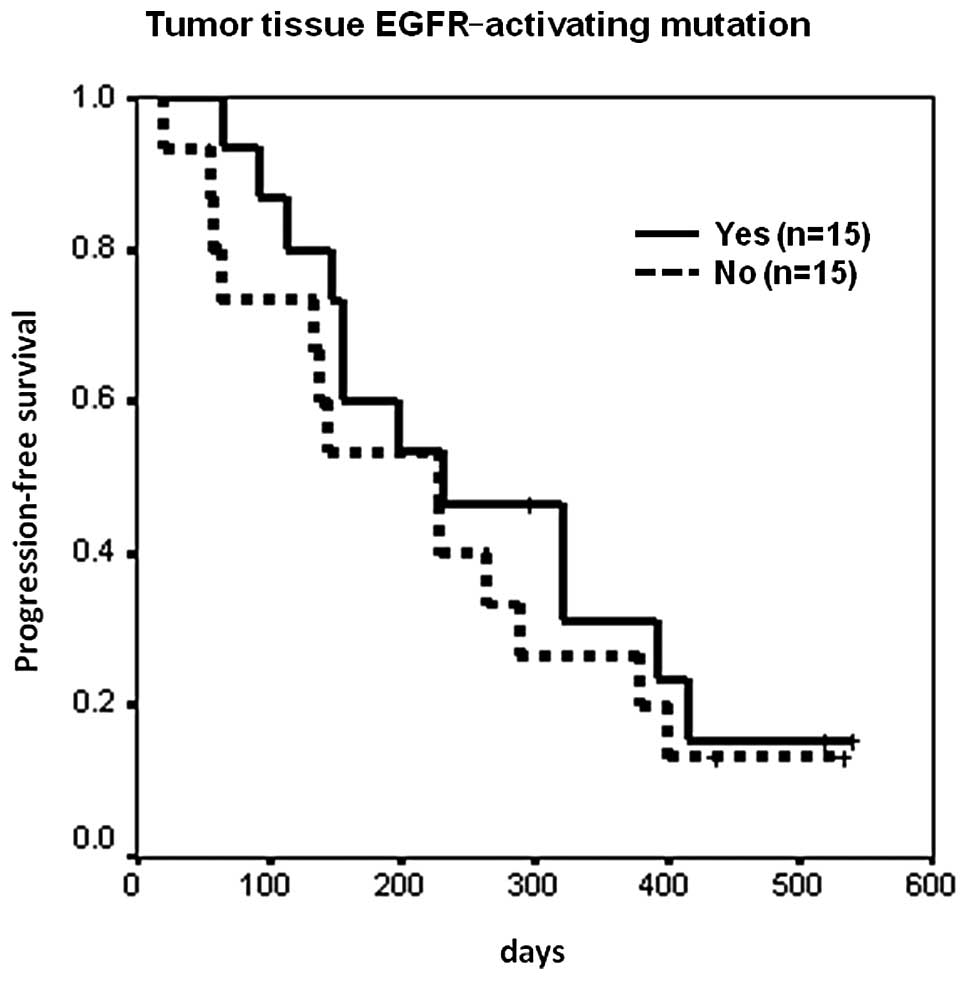
(p<0.0001). For those patients who had tumor tissue EGFR
sequencing data, median PFS was 7.7 months in 15 patients with
EGFR-activating mutations (censor 3, 95% CI 1.1–14.2 months), and
7.6 months in 15 patients without EGFR-activating mutations (censor
2, 95% CI 3.8–11.4 months) (p=0.4826, Fig. 1). The hazard ratio was 0.76 (95% CI
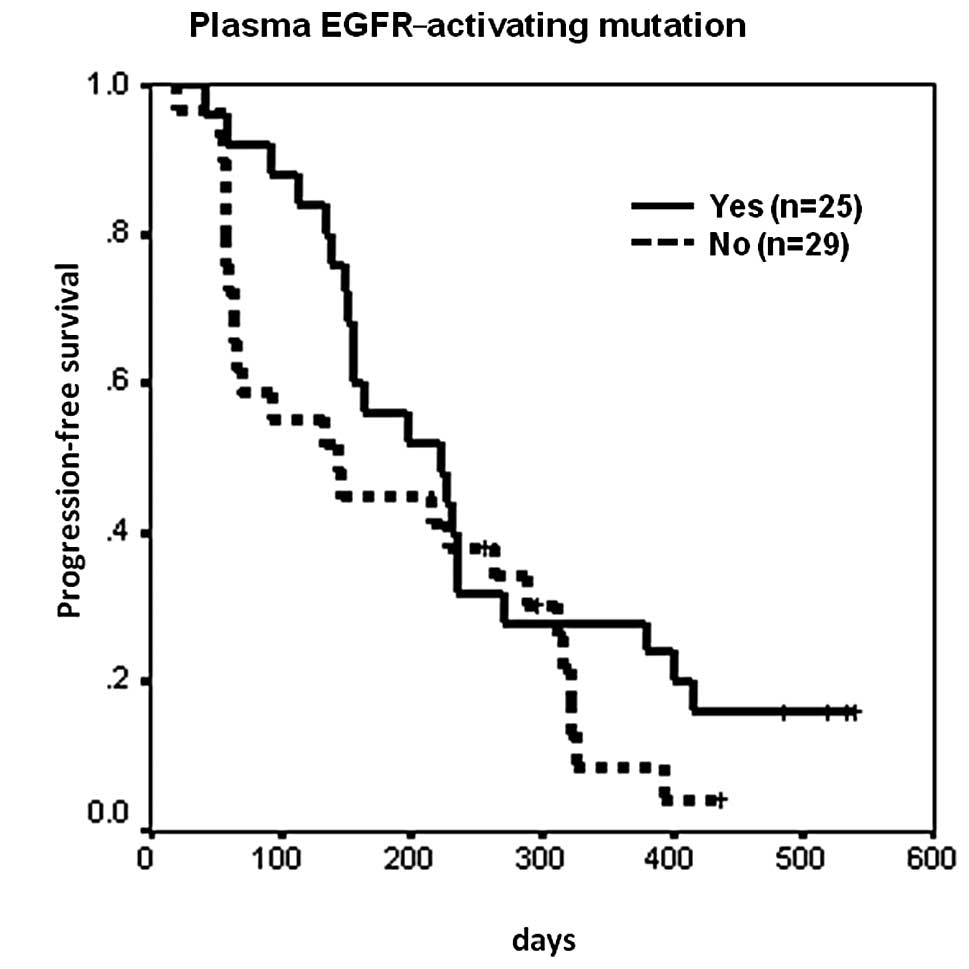
0.34–1.66, p=0.484). Median PFS was 7.4 months in 25 patients with
plasma EGFR-activating mutations (censor 4, 95% CI 3.9–10.9
months), and 4.8 months in 29 patients without EGFR-activating
mutations (censor 3, 95% CI 1.7–7.9 months) (p=0.1428, Fig. 2). The hazard ratio was 0.65 (95% CI
0.36–1.17, p=0.1471).
Of the 30 patients who had tumor tissue and plasma
EGFR sequencing data available, median PFS was 7.7 months in 21
patients who had EGFR-activating mutations detected in at least one
tumor or plasma specimen (censor 4, 95% CI 1.7–13.6 months), and
4.8 months in 9 patients who had no activating mutations detected
in either type of specimen (censor 1, 95% CI 3.8–5.8 months)
(p=0.2115). The hazard ratio was 0.59 (95% CI 0.25–1.37,
p=0.2168).
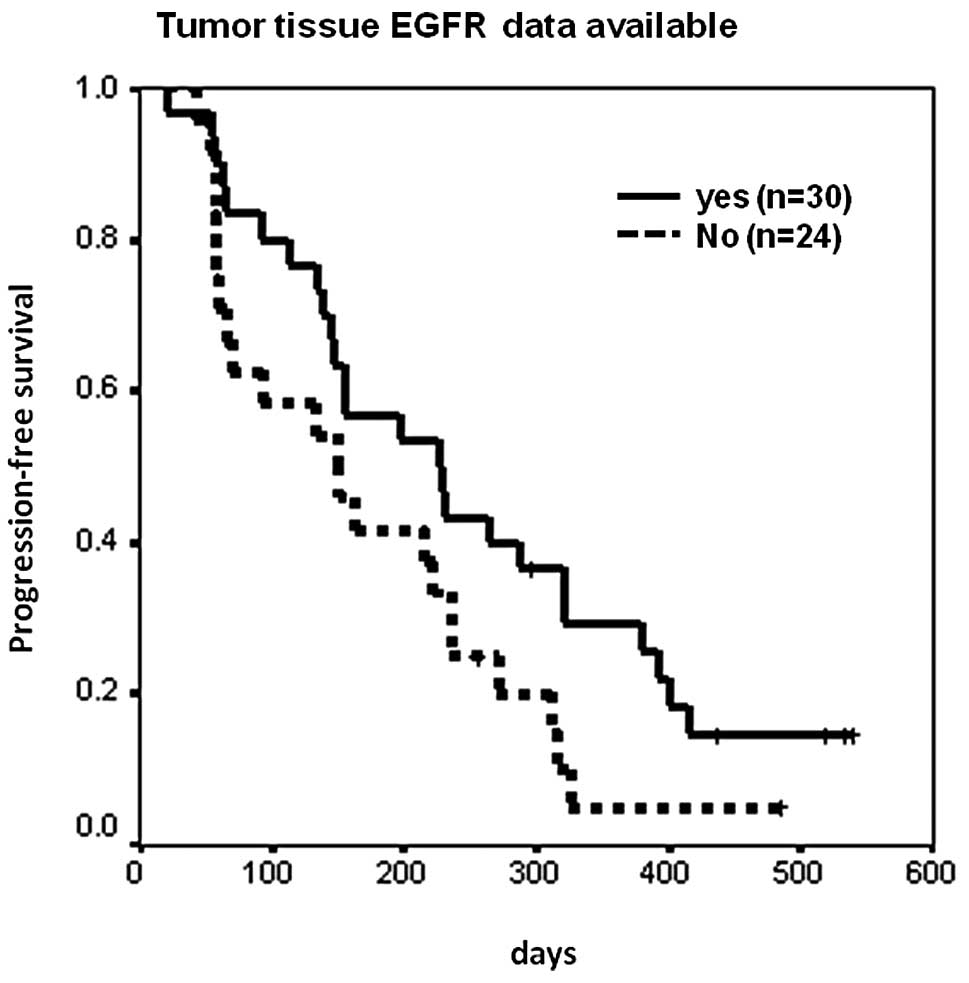
Patients without tumor tissue EGFR
mutation data
The tumor tissue EGFR mutation status of 24
patients, 44.4% of the total study population, was unavailable (10
had inadequate tissue samples and 14 had no tissue samples). The
overall response rate to erlotinib treatment of those 24 patients
was 33.3% (8 of 24), and 60% (18 of 30) for those patients who had
adequate tumor tissue samples for EGFR mutation analysis (p=0.046
and 0.061 for 1-sided and 2-sided χ2 tests,
respectively). PFS was also shorter for the 24 patients whose tumor
tissue EGFR mutation data were unavailable compared to the 30
patients who had adequate tissue samples for tumor EGFR analysis
(median 5 vs. 7.6 months, p=0.0704, Fig. 3). With regard to the 24 patients who
had no tissue samples or inadequate samples for EGFR mutation
analysis, the rate of response to erlotinib treatment was 45.5% (5
of 11) for those with plasma EGFR-activating mutations, and 23.1%
(3 of 13) for those without (p=0.39). Median PFS was 5.4 months for
11 patients with plasma EGFR-activating mutations, and 2.3 months
for 13 patients without mutations (p=0.6868).
Discussion
The use of molecular predictive markers to help
identify those patients who may benefit from a specific treatment
remains one of the most exciting areas of research in medical
oncology. The development of a rapid and sensitive test for the
early assessment of treatment response is also mandatory to avoid
futile treatments with ineffective agents. A number of studies have
documented that tumor tissue EGFR-activating mutations are useful
markers for predicting responses to EGFR-TKI treatment (4–7).
Determination of the tumor EGFR mutation status is significant for
non-squamous NSCLC, since first-line treatment with erlotinib or
gefitinib is recommended for patients with EGFR-activating
mutations, and cytotoxic chemotherapy is recommended for patients
without an EGFR-activating mutation status or with an unknown
status. The use of plasma or serum samples for EGFR mutation
analysis has been actively studied recently since more than half of
the patients did not have or had inadequate pathological samples
for tumor EGFR mutation analysis (9,10).
Several methods are used to detect EGFR mutations in
lung cancer specimens (14). The
sensitivity of direct sequencing is relatively poor and requires
more mutant DNA to detect EGFR mutations in specimens (10–25%
mutant DNA). The PNA-LNA PCR clamp is more sensitive and is able to
detect ≥1% mutant DNA in the specimens, as is the Scorpion
Amplified Refractory Mutation System (ARMS) method, which currently
has kits commercially available for testing (4,10,12,14).
However, direct sequencing is able to detect new mutations, while
the PNA-LNA PCR clamp and the Scorpion ARMS are capable of
detecting known mutations only (10,12,14).
There was no statistical difference in PFS between
the patients with and without a tumor EGFR-activating mutation in
the present study. This is possibly due to the low number of
patients enrolled and the relatively low sensitivity of the direct
tumor DNA sequencing (false negative of activating mutations).
Although there was also no statistical difference in the PFS of the
patients with and without plasma-free DNA EGFR-activating
mutations, the numerical difference in PFS between the 2 groups of
patients was larger than that detected by the direct tumor DNA
sequencing. This insignificant difference in the PFS detected by
the plasma-free DNA EGFR examination would be significant if
patient numbers were increased.
In the present study, patients with no tumor tissue
EGFR mutation data were examined, and, although there was no
statistically significant difference in the response rate and PFS
between the patients with (n=11) and without (n=13) plasma-free DNA
EGFR-activating mutations, the response rate was doubled and the
PFS was more than doubled in the patients with plasma-free DNA
EGFR-activating mutations. There would possibly be a statistical
significance if the patient number was increased. Thus, plasma-free
DNA EGFR mutation analysis using the PNA-LNA PCR clamp method is
useful for those patients with inadequate tumor specimens or
without tumor tissue available for tumor EGFR examinations. This
test may be of benefit to patients, in terms of predicting the
response to EGFR-TKI treatment. We concluded that in patients with
plasma-free DNA EGFR-activating mutations, the response to
erlotinib treatment was better and the PFS was longer than in those
without plasma-free DNA EGFR-activating mutations.
Acknowledgements
The study was supported in part by grants from the
National Science Council of the Republic of China, grant number
NSC99-2314-B-075-035-MY3, and Taipei Veterans General Hospital,
grant number VGH-100-C-015.
References
|
1
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J and
Thun MJ: Cancer statistics, 2009. CA Cancer J Clin. 59:225–249.
2009. View Article : Google Scholar
|
|
2
|
Azzoli CG, Baker S Jr, Temin S, Pao W,
Aliff T, Brahmer J and Johnson DH: American Society of Clinical
Oncology Clinical Practice Guideline update on chemotherapy for
stage IV non-small-cell lung cancer. J Clin Oncol. 27:6251–6266.
2009. View Article : Google Scholar
|
|
3
|
Shepherd FA, Pereira JR, Ciuleanu T, et
al: Erlotinib in previously treated non-small-cell lung cancer. N
Engl J Med. 353:123–132. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mok TS, Wu YL, Thongprasert S, et al:
Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma.
New Eng J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Maemondo M, Inoue A, Kobayashi K, et al:
Gefitinib or chemotherapy for non-small-cell lung cancer with
mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhou C, Wu YL, Chen G, et al: Efficacy
results from the randomized phase III OPTIMAL (CTONG 0802) study
comparing first-line erlotinib versus carboplatin (CBDCA) plus
gemcitabine (GEM), in Chinese advanced non-small-cell lung cancer
(NSCLC) patients (PTS) with EGFR activating mutations. Ann Oncol.
21c(Suppl 8): LBA132010.
|
|
7
|
Rosell R, Gervais R, Vergnenegre A, et al:
Erlotinib versus chemotherapy (CT) in advanced non-small cell lung
cancer (NSCLC) patients (p) with epidermal growth factor receptor
(EGFR) mutations: interim results of the European Erlotinib Versus
Chemotherapy (EURTAC) phase III randomized trial. Proc Am Soc Clin
Oncl A. 7503:2011.
|
|
8
|
Pao W and Ladanyi M: Epidermal growth
factor receptor mutation testing in lung cancer: searching for the
ideal method. Clin Cancer Res. 13:4954–4955. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kimura H, Kasahara K, Kawaishi M, et al:
Detection of epidermal growth factor receptor mutations in serum as
a predictor of the response to gefitinib in patients with
non-small-cell lung cancer. Clin Cancer Res. 12:3915–3921. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mack PC, Holland WS, Burich RA, et al:
EGFR mutations detected in plasma are associated with patient
outcomes in erlotinib plus docetaxel-treated non-small cell lung
cancer. J Thorac Oncol. 4:1466–1472. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pathak AK, Bhutani M, Kumar S, Mohan A and
Guleria R: Circulating cell-free DNA in plasma/serum of lung cancer
patients as a potential screening and prognostic tool. Clin
Chemistry. 52:1833–1842. 2006.PubMed/NCBI
|
|
12
|
Tanaka T, Nagai Y, Miyazawa H, et al:
Reliability of the peptide nucleic acid-locked nucleic acid
polymerase chain reaction clamp-based test for epidermal growth
factor receptor mutations integrated into the clinical practice for
non-small cell lung cancers. Cancer Sci. 98:246–252. 2007.
View Article : Google Scholar
|
|
13
|
Therasse P, Arbuck SG, Eisenhauer EA, et
al: New guidelines to evaluate the response to treatment in solid
tumors. European Organisation for Research and Treatment of Cancer,
National Cancer Institute of the United States, National Cancer
Institute of Canada. J Natl Cancer Inst. 92:205–216. 2000.
View Article : Google Scholar
|
|
14
|
Pao W and Ladanyi M: Epidermal growth
factor receptor mutation testing in lung cancer: searching for the
ideal method. Clin Cancer Res. 13:4954–4955. 2007. View Article : Google Scholar : PubMed/NCBI
|