Introduction
Intraocular lymphoma is a rare ocular malignancy
that may arise in the retina or the uvea. The exact incidence of
intraocular lymphoma has not been reported, but it was previously
estimated by Chan et al that at least 100 cases were
diagnosed in a 3-year span during the past decade (1). Retina or vitreoretinal lymphoma
accounts for the majority of cases and are often secondary to
diffuse large B-cell lymphoma. These are highly aggressive tumors
often with coexistent central nervous system (CNS) lymphoma (80%),
but rarely with systemic lymphoma (2). The tumors are bilateral in up to 90%
of cases, and present as multiple creamy white or yellow
intraretinal, subretinal or sub-RPE deposits with vitritis that can
easily be mistaken for infectious or non-infectious uveitis. We
describe herein a case of metastatic diffuse large B-cell lymphoma
in a patient in apparent systemic remission. Institutional review
board approval was not required for this case report. Informed
consent was obtained from the patient for all diagnostic tests,
surgery and treatment.
Case report
A 66-year-old Caucasian male presented with a
one-month history of blurred vision in the left eye (OS). His past
medical history was significant for hypertension and Waldenstrom’s
macroglobulinemia, which was diagnosed 5 years previously. The
patient, who had a rash consistent with urticaria pigmentosa and an
elevated serum tryptase level to perform bone marrow aspiration and
biopsy to evaluate for systemic mastocytosis. No peripheral
adenopathy or splenomegaly was present on examination. The marrow
was inaspirable and the biopsy revealed extensive replacement by
small lymphoplasmacytic cells and scattered mast cells consistent
with reactive mast cells. Immunoglobulin stains for light and heavy
chains were inconclusive, CD20 staining was positive and a
diagnosis of Waldenstrom’s macroglobulinemia was made. Serum
protein electrophoresis demonstrated a monoclonal IgM paraprotein
present at 3570 mg/dl (normal 40 to 230), κ restricted. The patient
was initially treated with rituximab but demonstrated no response
in the IgM level after 6 months. He received a second course of
rituximab, but again there was no response to the treatment. The
patient was then started on rituximab, fludarabine and
cyclophosphamide but was unable to complete the full course of
therapy due to the development of marked pancytopenia requiring red
blood cell and platelet transfusions. Bone marrow biopsy at that
time revealed severe hypocellularity with residual involvement of
Waldenstrom’s macroglobulinemia. The IgM level had declined to 1330
mg/dl and remained stable as blood counts slowly improved over the
following 3 years.
On a routine three-month follow-up visit, the
patient was found to have a large left axillary mass, which he
noted had developed three weeks earlier. He had no other symptoms.
Fine needle aspiration was performed at that time and demonstrated
large discohesive lymphocytes with prominent nucleoli. Flow
cytometry demonstrated that the large lymphocytes expressed CD10,
CD19 and CD20 with monoclonal κ light chain restriction. A
diagnosis of diffuse large B-cell lymphoma was made based on the
microscopic and flow cytometric information. The serum IgM level
was 1098 mg/dl. The PET/CT fusion scan revealed bulky
hypermetabolic bilateral axillary, retroperitoneal, right common
iliac and inguinal adenopathy. Hypermetabolic activity was also
present in the left cervical, supraclavicular, subpectoral,
azygoesophageal recess and distal left external iliac node regions.
Uptake was noted in a subpleural pulmonary nodule in the posterior
basilar segment of the right lower lobe, which was suspicious for
lymphoma. No other extranodal uptake was present. Serum lactate
dehydrogenase level was elevated at 349 U/l (normal, 118 to 273).
Bilateral bone marrow biopsies revealed marrow involvement by a
B-cell lymphoproliferative process, morphologically consistent with
lymphoplasmacytic lymphoma (Waldenstrom’s macroglobulinemia), which
expressed monoclonal κ light chain restriction but was CD 10
negative. No involvement by large B-cell lymphoma was observed.
Lumbar puncture was not performed. Based on this information, the
patient was considered to have at least stage IIIA disease but
possibly stage IVA disease, due to the uptake in the subpleural
nodule.
The patient was treated with R-CHOP and
Pegfilgrastim but was hospitalized with neutropenia and a left
upper lobe pulmonary infiltrate after cycle 2. The CT scan revealed
marked improvement in the adenopathy. Fever resolved on
administration of antibiotics, but the patient had recurrent
episodes of neutropenic fever despite chemotherapy dose reductions
for cycles 3 and 4 with persistence of the left upper lobe
pulmonary infiltrate. Moreover, Pseudomonas bacteremia was
noted after cycle 4. Chemotherapy was postponed as the patient
continued to experience fevers and malaise, was found to have
significant narrowing of the superior segment of the lingula, and
was treated with a prolonged course of piperacillin-tazobactam. A
CT scan of the chest 3 months after the last chemotherapy revealed
improvement of the left upper lobe pulmonary infiltrate and no
pathological adenopathy. The serum IgM level was 548 mg/dl. The
pulmonary infiltrate had resolved by repeat CT scan of the chest 2
months later, with no pathological adenopathy present. Bone marrow
aspiration and biopsy at that time revealed no involvement of large
B-cell lymphoma but minimal persistent involvement of Waldenstrom’s
macroglobulinemia. Approximately one month after the patient
received cycle 4 of his chemotherapy, and while under treatment for
pneumonia, he noted a persistent painless blurring of vision in his
left eye. The blurring did not improve, and was subsequently
evaluated.
Visual acuity on initial presentation was 20/25 in
the right eye (OD) and 20/30 OS. Intraocular pressures and anterior
segment examination were normal in both eyes (OU) with the
exception of the presence of 2+ khaki-colored cells in the anterior
vitreous OS. Fundus examination OD was normal, whereas OS showed
intraretinal infiltrates with associated hemorrhage in the
superotemporal midperiphery and diffuse vitreous hemorrhage.
Considering the immunocompromised state of the patient with regards
to non-Hodgkin’s lymphoma and chemotherapy, differential diagnoses
included infectious [cytomegalovirus retinitis (CMV), syphilis,
toxoplasmosis, tuberculosis], inflammatory (retinal vasculitis
associated with autoimmune conditions) and malignant (metastatic
systemic lymphoma) diseases.
Concern for possible CMV retinitis resulted in the
initiation of oral valgancyclovir 900 mg twice daily and one
intravitreal injection of foscarnet (2.4 mg/0.1 ml) OS prior to the
results of diagnostic testing. Anterior chamber paracentesis and
vitreous biopsy were performed and tested for toxoplasmosis, herpes
simplex virus (HSV), varicella zoster virus (VZV), CMV, bacterial
and fungal cultures, all of which were negative. Systemic work-up
for tuberculosis (PPD, CXR), syphilis (RPR, FTA-ABS), Lyme disease
and retinal vasculitis (ANCA, ANCA, ACE, PR3/MPO) were
unremarkable, with the exception of a positive c-ANCA. A diagnostic
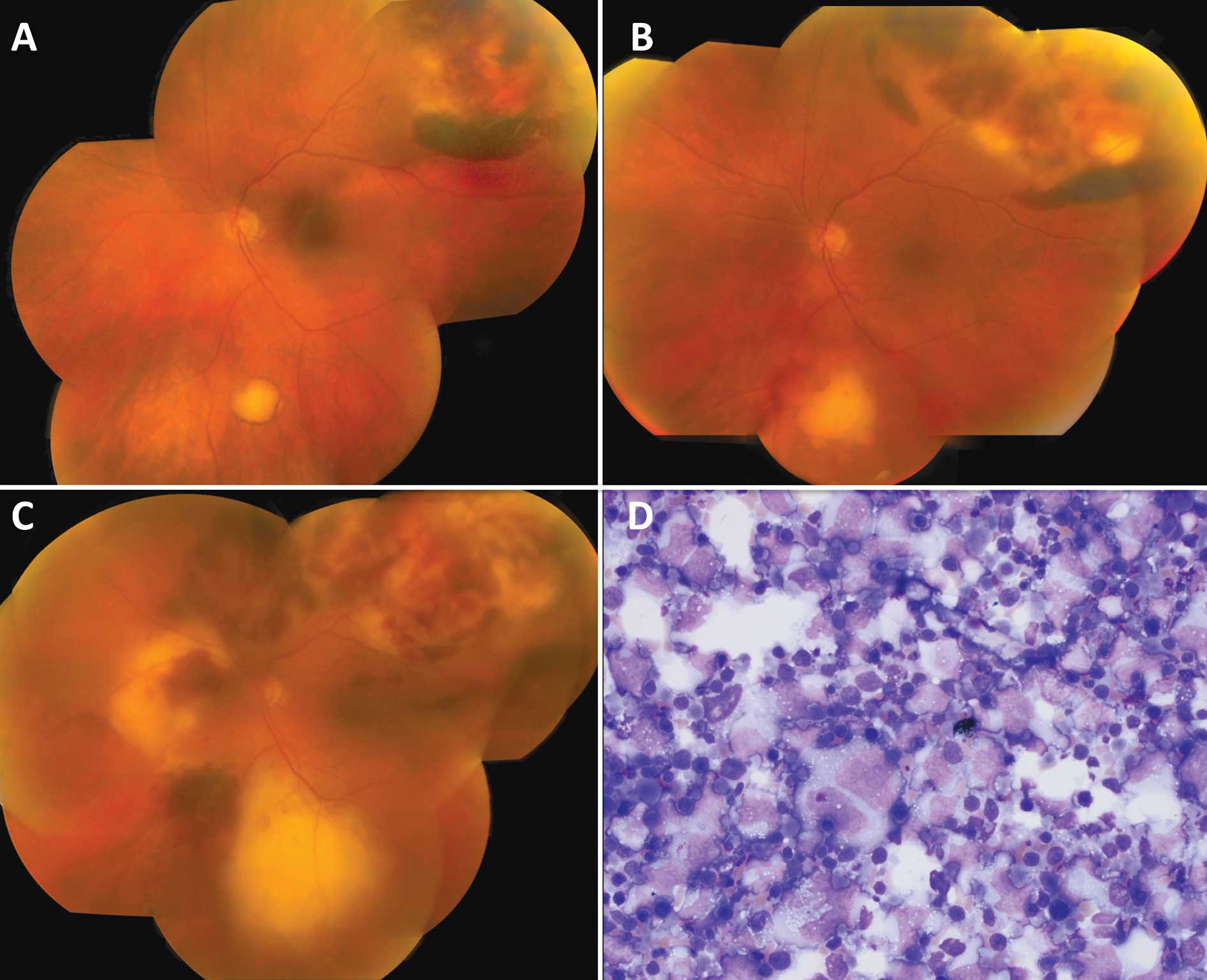
pars plana vitrectomy was also performed to exclude metastatic
lymphoma. Intraoperatively, diffuse vascular sheathing was
observed, along with a chorioretinal scar inferior to the optic
disc adjacent to an area of retinal whitening in addition to the
retinal infiltrates with intraretinal hemorrhage in the
superotemporal quadrant (Fig. 1A).
Valgancyclovir was discontinued and the patient was referred to
rheumatology for work up for possible ANCA-positive autoimmune
disease associated with retinal vasculitis. Further testing with
ANA, ENA, dsDNA, APLA, C3/C4, ESR, CRP, CBC, creatinine and brain
MRI/MRA were negative, with the exception of a mildly elevated ESR
and a low WBC count.
There was additional concern for possible
reactivated ocular toxoplasmosis associated with the chorioretinal
scar observed intraoperatively, and the patient was also started on
oral trimethoprim-sulfamethoxazole (800 mg/160 mg) twice daily. Two
weeks later, vision remained stable at 20/30, but new yellow
subretinal infiltrates appeared adjacent to the scar. The patient
was administered an injection of intravitreal clindamycin (1 mg/0.1
ml) and dexamethasone (400 μg/0.1 ml) for suspected worsening of
ocular toxoplasmosis. One week following the intravitreal
injection, the previously noted chorioretinal scar was not a scar
but an elevated lesion with presence of subretinal fluid, and new
infiltrates were observed from the nasal to the optic disc and
confirmed by optical coherence tomography (Fig. 1B). Concern regarding an indolent
fungal infection resulted in the administration of oral Levaquin
and voriconazole, but without improvement. The visual acuity of the
patient decreased to 20/250, and the retinal infiltrates continued
to increase in size following one week of treatment (Fig. 1C). A second pars plana vitrectomy
was applied with subretinal biopsy 3 months after the initial
presentation. Cytopathology and flow cytometry confirmed large
B-cell lymphoma, consistent with pathology observed on a previous
axillary node biopsy, leading to a diagnosis of metastatic B-cell
lymphoma (Fig. 1D). A restaging
work-up for lymphoma with PET/CT fusion scan revealed a
hypermetabolic left lung nodule measuring 1.9×1.7 cm, consistent
with active lymphoma. No other involvement in lymph nodes or other
extranodal sites, including the central nervous system was
observed. Lumbar puncture was not performed at this time.
The patient then underwent external beam
radiotherapy with a total dose of 3000 cGy to the left eye in 200
cGy fractions. Final visual acuity was no light perception OS. At
the conclusion of the radiation therapy, repeat PET/CT scan, as
compared to the scan at the original diagnosis of large B-cell
lymphoma a year earlier, demonstrated resolution of the activity in
the previously involved nodal sites and the small right subpleural
pulmonary nodule, but new extensive bilateral hypermetabolic
pulmonary nodules, the largest measuring 5 cm with extensive
hypermetabolic mediastinal and bilateral hilar adenopathy. No
extrathoracic hypermetabolic activity was present. The patient was
evaluated as a candidate for autologous stem cell transplantation
but declined due to difficulty tolerating the previous R-CHOP
chemotherapy; however, the patient agreed to rituximab and a
reduced dose of bendamustine therapy at 70 mg/m2. The
patient tolerated the first cycle well with an expected decrease in
blood counts, and the dose of bendamustine was increased to 100
mg/m2 for cycle 2 of therapy. He developed significant
diarrhea after this treatment but did not require hospitalization.
PET/CT scan after cycle 2 of treatment demonstrated interval
resolution of hypermetabolic mediastinal adenopathy and marked
improvement in the activity in the lungs with only low-level
activity remaining at the site of the largest pulmonary nodule,
which had decreased from 5 cm to a 1.5 cm wedge-shaped density. The
patient has continued on the rituximab and bendamustine
chemotherapy, but the bendamustine dose was reduced to 70
mg/m2 without significant toxicities. The patient is
presently alive after 6 cycles of this therapy with Eastern
Cooperative Oncology Group (ECOG) performance status 1.
Discussion
Intraocular lymphoma is often associated with a grim
prognosis due to associated central nervous system disease. In a
review by Mochizuki and Singh, ocular-CNS lymphoma was found to
occur in 61% of patients, primary intraocular lymphoma in 17%,
ocular-visceral lymphoma in 17% and ocular-visceral-CNS lymphoma in
5% of patients (2). Intraocular
lymphoma from the systemic dissemination of visceral lymphoma is
usually confined to the choroid and infrequently presents as
vitreoretinal lymphoma, similar to our case (3). The rarity of intraocular lymphoma, its
diverse clinical presentation, the ability to masquerade as
different uveitic entities, and in this case, an atypical site of
ocular involvement, makes diagnosis difficult. Additionally,
successful confirmatory biopsy by fine needle aspiration or
vitrectomy is a demanding procedure that requires significant skill
not only by the ophthalmologist, but also the cytopathologist.
These factors often cause a delay in the diagnosis and initiation
of treatment. A report by Karma et al showed a median of 8
months after onset of symptoms to the first ocular examination, and
a median of 13 months from onset of symptoms until diagnosis of
intraocular lymphoma (4).
Our patient presented with unilateral blurred vision
from vitreous hemorrhage accompanied by progressive increase in
size of the retinal infiltrates. Given the patient’s history of
neoplastic disease and his immunocompromised state while on
chemotherapy, important differential diagnoses included infectious
and non-infectious entities. The retinal infiltrates and vitreous
hemorrhage were both atypical for intraocular lymphoma secondary to
systemic metastases, as metastatic systemic lymphoma more commonly
presents with uveal involvement alone. The positive c-ANCA
associated with retinal infiltrates and hemorrhages was also
evaluated for a systemic vasculitis with ocular involvement. ANCA
positivity in our case was most likely secondary to systemic
lymphoma, which has previously been reported (5). Although vitreous and aqueous biopsies
for viral, bacterial and fungal infections, as well as
cytopathology for lymphoma cells were negative, empiric antibiotic
therapy for infectious retinitis was indicated considering the
sight-threatening nature of the disease. Initially, CMV retinitis
was considered the most likely cause due to the presence of retinal
infiltrates with adjacent subretinal, intraretinal and vitreous
hemorrhage, which is not commonly associated with ocular lymphoma,
particularly when the patient was systemically in remission from
lymphoma. Following a negative response to treatment, a diagnostic
vitrectomy was performed, revealing a new chorioretinal scar
inferior to the optic disc. A diagnosis of toxoplasmosis appeared
likely, and appropriate systemic and intravitreal
antibiotic-steroid regimens were administered, again without
response and with progression. It was not until subretinal biopsy
with pars plana vitrectomy was performed that a diagnosis of
metastatic lymphoma was confirmed, triggering a search for systemic
metastases, which was positive. This was 3 months after the
patient’s first ophthalmology evaluation and 4 months after the 4th
cycle of R-CHOP. With hindsight, a concurrent systemic staging
along with an earlier subretinal biopsy may have led to an earlier
diagnosis and a better visual outcome. The relapsing clinical
course of our patient may have led us to perform more aggressive
diagnostic procedures early on, in addition to coordinating a
repeat PET/CT scan and lumbar puncture with his oncologist.
Our case showed the difficulty in obtaining
confirmatory diagnosis in metastatic intraocular lymphoma, and
possibly a role for concurrent systemic restaging, even in patients
with ocular complaints and in systemic remission. More importantly,
a strong clinical suspicion should always be present and the
importance of repeated diagnostic biopsies should be emphasized,
particularly in an aggressive malignancy with a significant threat
to life.
Acknowledgements
Support was provided by an unrestricted grant from
Research to Prevent Blindness.
References
|
1
|
Chan CC, Buggage RR and Nussenblatt RB:
Intraocular lymphoma. Curr Opin Ophthalmol. 13:411–418. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mochizuki M and Singh AD: Epidemiology and
clinical features of intraocular lymphoma. Ocul Immunol Inflamm.
17:69–72. 2009. View Article : Google Scholar
|
|
3
|
Coupland SE and Damato B: Understanding
intraocular lymphoma. Clin Experiment Ophthalmol. 36:564–578. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Karma A, von Willebrand EO, Tommila PV,
Paetau AE, Oskala PS and Immonen IJ: Primary intraocular lymphoma:
improving the diagnostic procedure. Ophthalmology. 114:1372–1377.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee AS, Wiesner O, Gillespie DJ, Witzig
TE, Homburger H and Specks U: A 70-year-old man with pulmonary
infiltrates and a positive antineutrophil cytoplasmic autoantibody
test result. Chest. 127:1045–1050. 2005.PubMed/NCBI
|