Introduction
Lung cancer is the leading cause of cancer-related
mortality in China and the United States. Globally, the overall
5-year survival rate is still as low as 10–16% (1,2).
Non-small cell lung cancer (NSCLC) accounts for 85% of all lung
cancer cases, and surgical resection remains the most successful
option for cure for patients with operable NSCLC (1,2). The
5-year survival rate for resected stage I NSCLC ranges between
60–70%, however 30–40% of early-stage patients die within 5 years
of surgery, mostly as a result of metastatic disease presenting at
the time of surgical resection (3,4).
Investigating the genes involved in the processes of cell invasion
and metastasis in NSCLC, as well as understanding and elucidating
their molecular biological mechanisms, are essential steps for the
diagnosis, treatment and prognosis prediction of NSCLC.
A disintegrin and metalloproteinases (ADAMs) are
type I transmembrane proteins containing both a metalloproteinase
and disintegrin extracellular domain, and are involved in the
proteolytic processing of multiple transmembrane proteins, cell
adhesion, migration and cell signal transduction (5). ADAM9, a member of the ADAM family,
demonstrates proteinase activity which is important in the cleavage
of proHB-EGF, known as ectodomain shedding. ADAM9 is also
responsible for mediating EGF receptor activity (6) and is capable of regulating E-cadherin
and integrins (7,8), demonstrating its important role in
cancer cell invasion, migration and metastasis (5–8).
Recently, highly expressed ADAM9 was detected in
breast cancer (9), liver cell
carcinoma (10), gastric cancer
(11), pancreatic ductal
adenocarcinoma (12), prostate
cancer (13), renal cell carcinoma
(14) and cervical squamous
carcinoma (15), correlating with
cancer progression, metastasis and predicting a shortened survival
time in patients (9–15). However, the expression of ADAM9 in
human resected lung cancer tissue and its clinical significance
remain unclear.
We recently demonstrated that ADAM9 was highly
expressed in 39 cases of resected stage I NSCLC tissues compared
with normal control lung tissue (16). In the present study, we detect
further ADAM9 expression at the protein level in surgically
resected stage I NSCLC, attempting to confirm the findings of
highly expressed ADAM9 in NSCLC, and to further evaluate its
clinical significance, especially with regard to predicting the
prognosis of resected stage I NSCLC (abstract was published at the
14th World Conference on Lung Cancer, Amsterdam, 2011) (17).
Materials and methods
Patients and tissues
Formalin-fixed, paraffin-embedded tissue blocks were
obtained from 64 cases of completely resected NSCLC with
mediastinal N2 lymph node dissection who underwent surgery at the
Department of Thoracic Surgery, The First Hospital of China Medical
University (Shenyang, China) between April 2000 and May 2006. All
patients underwent standard lobectomy and mediastinal N2 lymph node
dissection. Preoperative examinations of liver ultrasound, brain
computed tomography (CT) and bone scintigraphy were performed to
exclude the presence of distant metastasis. The following criteria
were used to exclude patients: the patients received preoperative
chemotherapy or radiotherapy, died within 3 months of surgery or
succumbed to a cause other than NSCLC.
The total number of patients in this group (n=64)
consisted of 36 males and 28 females who ranged in age between 33
and 76 years old (median age, 60 years). Histological types were
determined according to the WHO 2000 classification: 16 cases of
squamous cell carcinoma and 48 cases of adenocarcinoma.
Postoperative pathological stage was classified according to the
UICC and AJCC TNM staging system (3): T1N0M0 stage IA, 24 cases (37.5%);
T2N0M0 stage IB, 40 cases (62.5%). Normal control lung tissue was
collected from >5 cm away from the lung tumor site in 12 cases
of completely resected stage IA lung cancer. The study was approved
by the Institutional Review Board (IRB) of the First Hospital of
China Medical University.
Immunohistochemistry staining
Sections (3 μm) were cut from formalin-fixed,
paraffin-embedded lung cancer tissue. After baking overnight at
60°C, the sections were dewaxed with xylene and gradually hydrated,
and then exposed to 3% H2O2 for 12 min to
quench endogenous tissue peroxidase. Antigen was exposed by heating
the sections under high pressure in citrate buffer (pH 6.0), cooked
for 2 min and then incubated for 20 min in goat serum. The primary
goat polyclonal ADAM9 antibody (AF949) was bought from R&D
Systems (Minneapolis, MN, USA) and diluted with PBS (1:50)
(12–14,16).
The specificity and sensitivity of the antibody used have been well
tested (12–14,16).
After incubation overnight at 4°C, biotin-labeled rabbit-anti goat
IgG (Maixin Bio, Fuzhou, China) was used as a secondary antibody
incubated for 20 min at room temperature, followed by
Streptavidin-Peroxidase (S-P; Maixin Bio, Fuzhou, China) incubated
for 20 min at room temperature. Immunohistochemistry staining was
visualized with 3,3′-diaminobenzidine (DAB) system for 2–3 min.
Afterwards, the slides were briefly counterstained with
hematoxylin. ADAM9-positive NSCLC slides were used as the positive
control, and the ADAM9-positive slides in which the primary
antibody was omitted during staining were used as the negative
control.
Standard of staining scores
The positive cells were stained from yellow to brown
in the cytoplasm and cell membrane. For each section, five fields
of vision were selected and total 1000 tumor cells were counted and
evaluated (200 tumor cells in each field of vision). The percentage
of positive tumor cells was calculated. The staining index was
evaluated semiquantitatively as negative, weak, moderate or strong
by the multiplication of the staining intensity (A) and the
percentage of positive tumor cells (B). The staining intensity was
scored as 1, buff; 2, buffy; and 3, puce. The percentage of
positive tumor cells was scored as: 0, positive tumor cells <5%;
1, 5–10%; 2, 11–50%; 3, 51–75%; 4, >75%. The total score
(immunostaining index) was the multiplication of A and B and was
classified as follows: a score of 0 was considered as negative (−),
1–4 was considered weak (+), 5–8 as moderate (++) and 9–12 as
strong (+++).
All of the cases were divided by average
immunostaining index (mean scores) into two groups, ADAM9 high
expression (ADAM9-high) group and ADAM9 low expression (ADAM9-low)
group. The immunostaining was evaluated independently by two
pathologists who were blinded to the patients’ score.
Statistical analysis
Statistical analysis was performed using SPSS
software version 17.0. A Chi-square test and Fisher’s exact test
were used to assess the correlation between clinicopathological
characteristics and ADAM9 expression. For the survival analysis,
the Kaplan-Meier method was used for a univariate analysis, and the
differences in survival curves were assessed with the Log-rank
test. The Cox regression model was used for multivariate survival
analysis. P<0.05 (two-tailed test) was considered to indicate a
statistically significant result.
Results
Highly expressed ADAM9 in NSCLC
tissue
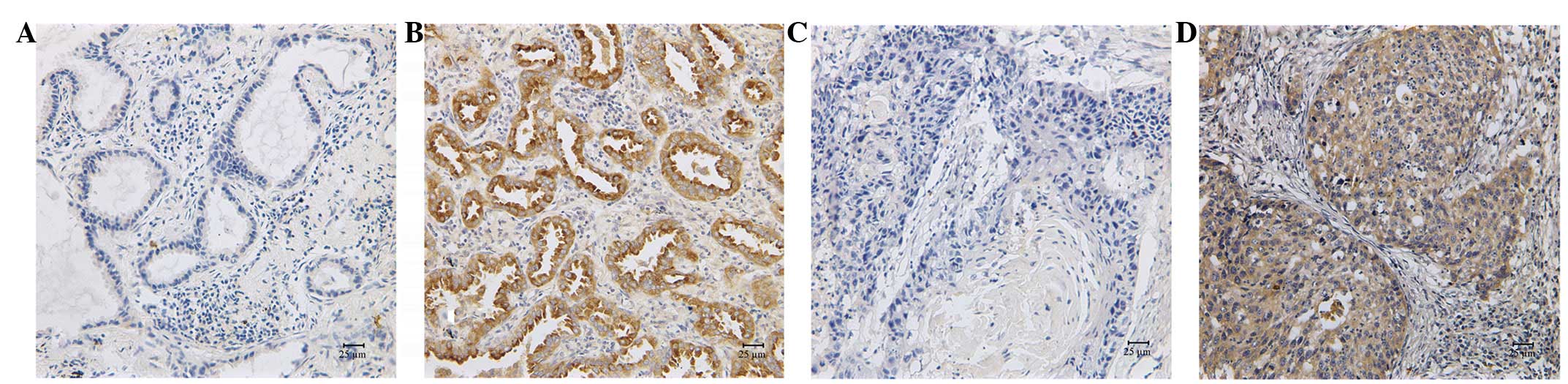
ADAM9 expression was mainly identified in the
cytoplasm. In normal control lung tissue, ADAM9 staining was mainly
observed to be negatively or weakly expressed and scores belonged
to the ADAM9-low group. The ADAM9-high rate was 0% (0/12) in normal
control lung tissues.
In 64 cases of completely resected stage I NSCLC,
53.1% (34/64) demonstrated highly expressed ADAM9 protein,
significantly higher when compared with normal control lung tissue
(P=0.001). No difference between the ADAM9-high rates between the
stage IA and IB groups was identified (P>0.05; Fig. 1).
Survival analysis: highly expressed ADAM9
predictes shortened survival
The overall 5-year survival rate for the group of 64
completely resected stage I NSCLC cases with performed lobectomy,
local hilar (N1) and mediastinal (N2) lymph node dissection was
71.8%. The 5-year survival rate in the ADAM9-low group (30 cases)
was as high as 88.9%, however, the 5-year survival rate sharply
decreased to 56.9% in the ADAM9-high group (34 cases). The
difference between these two groups was statistically significant
(P=0.012; Table I, Fig. 2).
 | Table IUnivariate analysis for 64 cases of
resected NSCLC. |
Table I
Univariate analysis for 64 cases of
resected NSCLC.
| Variable | n | Proportion (%) | 5-year survival
(%) | P-value |
|---|
| NSCLC | 64 | 100 | 71.8 | |
| ADAM9 expression | | | | 0.012a |
| Low expression | 30 | 46.9 | 88.9 | |
| High
expression | 34 | 53.1 | 56.9 | |
| Gender | | | | 0.938 |
| Male | 36 | 56.3 | 75.0 | |
| Female | 28 | 43.7 | 69.0 | |
| Age (years) | | | | 0.736 |
| <60 | 31 | 48.4 | 68.8 | |
| ≥60 | 33 | 51.6 | 74.8 | |
| Histological
type | | | | 0.227 |
| Squamous | 16 | 25.0 | 87.5 | |
| Adenocarcinoma | 48 | 75.0 | 67.0 | |
| Pathological
stage | | | | 0.526 |
| IA | 24 | 37.5 | 71.3 | |
| IB | 40 | 62.5 | 71.5 | |
In 24 stage IA cases, the 5-year survival rate for
the ADAM9-low group (8 cases) was 100%, which sharply decreased to
55.0% for the ADAM9-high group (16 cases). Again, the difference
was statistically significant (P=0.049). In the 40 stage IB cases,
the 5-year survival rate for the ADAM9-low group (22 cases) was as
high as 84.8%, but it decreased sharply to 55.6% for the ADAM9-high
group (18 cases), and the difference was statistically significant
(P=0.030; Table II, Fig. 2).
| Table IIHighly expressed ADAM9 predicts a
worse prognosis for 64 cases of resected NSCLC. |
Table II
Highly expressed ADAM9 predicts a
worse prognosis for 64 cases of resected NSCLC.
| Clinicopathological
factors | Cases (n) | 5-year survival, %
| P-value |
|---|
| ADAM9 low expression
(n) | ADAM9 high
expression (n) |
|---|
| Histological
type | | | | |
|
Adenocarcinoma | 48 | 86.5 (16) | 57.2 (32) | 0.071 |
| Squamous | 16 | 92.9 (14) | 50.0 (2) | 0.180 |
| Pathological
stage | | | | |
| IA | 24 | 100 (8) | 55.0 (16) | 0.049a |
| IB | 40 | 84.8 (22) | 55.6 (18) | 0.030a |
The Cox regression model was used for multivariate
survival analysis: patient gender, age, smoking status,
histological type, pathological stage (IA and IB) and ADAM9
high/low expression were entered into the Cox proportional hazard
regression model. The results demonstrated that ADAM9 high/low
expression was an independent predictor of prognosis for this group
of completely resected stage I NSCLC (HR, 3.385; 95% CI,
1.224–9.360; P=0.019).
Discussion
Even though ADAM9 has been observed to be highly
expressed in numerous solid malignant tumors (9–15),
correlating with cancer cells’ invasion, migration, metastasis,
involvement of lymph nodes and a worse prognosis (5–15), the
expression of ADAM9 at the protein level and its clinical
significance in human resected NSCLC cases remains unclear. In
NSCLC cell lines, ADAM9 overexpression in A549 cells was shown to
increase the ability of adhesion, invasion and metastasis to the
brain tissue of nude mice, through modulation of integrin α3β1
function in cancer cells (18). We
previously demonstrated that ADAM9 is downregulated when using
siRNA silencing hepatoma-derived growth factor (HDGF), inducing
inhibition of anchorage-independent growth of NSCLC cells and their
capability of migrating through the BD matrigel (19,20),
suggesting that ADAM9 participates in the HDGF pathway to promote
invasion and metastasis of NSCLC cells. HDGF was shown to be highly
expressed in NSCLC and highly expressed HDGF correlated with
shortened survival time in NSCLC patients (21). We then preliminarily detected ADAM9
expression at the protein level in the tissue samples of 39 cases
of resected stage I–III NSCLC (16), and revealed that ADAM9 was highly
expressed in NSCLC tissue, suggesting that ADAM9 may be important
in NSCLC growth, invasion and metastasis.
In this study, we confirmed that ADAM9 was
significantly more highly expressed in NSCLC when compared with
normal control lung tissue (53.1 vs. 0%, P=0.001). Survival
analysis revealed that the high expression of ADAM9 predicted a
shortened survival in the group of patients with completely
resected stage I NSCLC. The 5-year survival rate decreased sharply
from as high as 88.9% in the ADAM9-low group to 56.9% in the
ADAM9-high group. The difference was statistically significant
(P=0.012). Multivariate survival analysis revealed that ADAM9
expression, instead of other factors such as patients’ gender, age,
smoking status, histological type and pathological stage (IA and
IB), was an independent predictor of prognosis for this group of
surgically resected stage I NSCLC cases (HR, 3.385; 95% CI,
1.224–9.360; P=0.019). The results are consistent with the findings
that ADAM9 is highly expressed and high levels of ADAM9 expression
predict a worse prognosis in other types of solid malignant tumors
(9–15), suggesting that ADAM9 is a novel and
valuable prognostic biomarker for NSCLC. Adding sub-groups
stratified by ADAM9 expression into the lung cancer TNM stage
system may also help to supply more accurate information for
assessing prognosis.
Furthermore, sub-grouping by ADAM9 expression
clearly revealed that the sub-group of ADAM9-high stage I NSCLC,
having a 5-year survival rate of 56.9%, which is almost as low as
the 5-year survival rate in patients with resected stage II NSCLC
(3), should receive further
treatment, such as adjuvant chemotherapy, in order to obtain an
improved prognosis. ADAM9 may also become a predictive biomarker to
help improve the selection of certain stage I NSCLC patients to
receive adjuvant chemotherapy or not.
By contrast, for the sub-group of ADAM9-low stage I
NSCLC, with low expression of ADAM9, demonstrating a significantly
longer survival time, the 5-year survival rate was 88.9% in our
study, suggesting that no further adjuvant chemotherapy is
necessary for this group of stage I NSCLC, especially considering
long-term chemotherapy-associated toxicity (22,23).
Previously, Zhu et al(24) reported the use of prognostic
signatures to divide NSCLC patients into two groups; a high-risk
and a low-risk group. Patients who were predicted a ‘worse’
prognosis benefited significantly from adjuvant chemotherapy;
however, the patients who were predicted with ‘better’ prognosis
did not benefit from adjuvant chemotherapy, suggesting that
sub-grouping by valuable prognostic biomarkers is important in
prognosis judgment, especially in aiding the selection of adjuvant
chemotherapy (22,23,25).
Greater effort should be taken to test more novel and valuable
prognostic and predictive biomarkers, such as ADAM9 and HDGF
(21), in order to use more simple
but accurate methods, to aid decision-making in regard to NSCLC
patients receiving personalized adjuvant chemotherapy or not.
To the best of our knowledge, this is the first
study describing highly expressed ADAM9 protein in human resected
NSCLC tissues predicting a shortened survival. Limited cases have
provided us with sufficient evidence to obtain a preliminary
conclusion. Using a simple but clinically useful and accurate
method, ADAM9 was shown to be a novel prognostic biomarker and may
also be a valuable predictive biomarker for adjuvant chemotherapy
for completely resected stage I NSCLC patients. In addition, ADAM9
may become a potential target for molecular targeted therapeutics.
Further investigations of prospective case-control cohort studies
are required to confirm the role of ADAM9 in predicting prognosis
and effectiveness of adjuvant chemotherapy for completely resected
stage I NSCLC patients.
In conclusion, ADAM9 is highly expressed in NSCLC
and highly expressed ADAM9 correlates with shortened survival.
ADAM9 expression is an independent prognostic predictor for
resected stage I NSCLC, suggesting that ADAM9 is a novel biomarker
significantly and independently predicting worse prognosis of
resected stage I NSCLC. ADAM9 should also be a valuable predictive
biomarker for selection of adjuvant chemotherapy for completely
resected stage I NSCLC patients.
Abbreviations:
|
ADAM9
|
a disintegrin and
metalloproteinase-9;
|
|
NSCLC
|
non-small cell lung cancer;
|
|
EGF
|
epithelial growth factor;
|
|
CT
|
computed tomography;
|
|
AJCC
|
American Joint Committee on
Cancer;
|
|
UICC
|
Union Internationale Contre le
Cancer;
|
|
S-P
|
streptavidin-peroxidase;
|
|
DAB
|
3,3′-diaminobenzidine;
|
|
HDGF
|
hepatoma-derived growth factor
|
Acknowledgements
The authors would like to thank C.
Guan for technical assistance of immunohistochemistry staining, Dr
Y. Han and Dr X. Qiu for immunostaining evaluation and discussion.
This study was partly supported by IASLC/CRFA Prevention
Fellowship, grants from The Education Department of Liaoning
Province (No. 20060991) and from the Nature Science Foundation of
Liaoning Province, China (No. 20102285), and the Fund for
Scientific Research of The First Hospital of China Medical
University (No. FSFH1210).
References
|
1
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar
|
|
2
|
Molina JR, Yang P, Cassivi SD, Schild SE
and Adjei AA: Non-small cell lung cancer: epidemiology, risk
factors, treatment, and survivorship. Mayo Clin Proc. 83:584–594.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mountain CF: Revisions in the
International System for Staging Lung Cancer. Chest. 111:1710–1717.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nesbitt JC, Putnam JB Jr, Walsh GL, Roth
JA and Mountain CF: Survival in early-stage non-small cell lung
cancer. Ann Thorac Surg. 60:466–472. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Seals DF and Courtneidge SA: The ADAMs
family of metalloproteases: multidomain proteins with multiple
functions. Genes Dev. 17:7–30. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fischer OM, Hart S, Gschwind A, Prenzel N
and Ullrich A: Oxidative and osmotic stress signaling in tumor
cells is mediated by ADAM proteases and heparin-binding epidermal
growth factor. Mol Cell Biol. 24:5172–5183. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hirao T, Nanba D, Tanaka M, Ishiguro H,
Kinugasa Y, Doki Y, Yano M, Matsuura N, Monden M and Higashiyama S:
Overexpression of ADAM9 enhances growth factor-mediated recycling
of E-cadherin in human colon cancer cell line HT29 cells. Exp Cell
Res. 312:331–339. 2006.PubMed/NCBI
|
|
8
|
Mahimkar RM, Visaya O, Pollock AS and
Lovett DH: The disintegrin domain of ADAM9: a ligand for multiple
beta1 renal integrins. Biochem J. 385:461–468. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
O’Shea C, McKie N, Buggy Y, Duggan C, Hill
AD, McDermott E, O’Higgins N and Duffy MJ: Expression of ADAM-9
mRNA and protein in human breast cancer. Int J Cancer. 105:754–761.
2003.
|
|
10
|
Tannapfel A, Anhalt K, Häusermann P,
Sommerer F, Benicke M, Uhlmann D, Witzigmann H, Hauss J and
Wittekind C: Identification of novel proteins associated with
hepatocellular carcinomas using protein microarrays. J Pathol.
201:238–249. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Carl-McGrath S, Lendeckel U, Ebert M,
Roessner A and Röcken C: The disintegrin-metalloproteinases ADAM9,
ADAM12, and ADAM15 are upregulated in gastric cancer. Int J Oncol.
26:17–24. 2005.PubMed/NCBI
|
|
12
|
Grützmann R, Lüttges J, Sipos B, Ammerpohl
O, Dobrowolski F, Alldinger I, Kersting S, Ockert D, Koch R,
Kalthoff H, Schackert HK, Saeger HD, et al: ADAM9 expression in
pancreatic cancer is associated with tumour type and is a
prognostic factor in ductal adenocarcinoma. Br J Cancer.
90:1053–1058. 2004.
|
|
13
|
Fritzsche FR, Jung M, Tölle A, Wild P,
Hartmann A, Wassermann K, Rabien A, Lein M, Dietel M, Pilarsky C,
Calvano D, Grützmann R, et al: ADAM9 expression is a significant
and independent prognostic marker of PSA relapse in prostate
cancer. Eur Urol. 54:1097–1106. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fritzsche FR, Wassermann K, Jung M, Tölle
A, Kristiansen I, Lein M, Johannsen M, Dietel M, Jung K and
Kristiansen G: ADAM9 is highly expressed in renal cell cancer and
is associated with tumour progression. BMC Cancer. 8:1792008.
View Article : Google Scholar
|
|
15
|
Zubel A, Flechtenmacher C, Edler L and
Alonso A: Expression of ADAM9 in CIN3 lesions and squamous cell
carcinomas of the cervix. Gynecol Oncol. 114:332–336. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Qi J and Zhang J: Abnormal expression of
ADAM9 in non-small cell lung cancers. Zhongguo Yike Daxue Xuebao.
39:670–671. 2010.(In Chinese).
|
|
17
|
Zhang J, Qi J, Chen N, Guo Y, Fu W, Zhou B
and He A: Highly expressed ADAM9 in completed resected stage I
non-small cell lung cancer cases predicts a shortened survival. J
Thorac Oncol. 6:s1068–s1069. 2011.
|
|
18
|
Shintani Y, Higashiyama S, Ohta M,
Hirabayashi H, Yamamoto S, Yoshimasu T, Matsuda H and Matsuura N:
Overexpression of ADAM9 in non-small cell lung cancer correlates
with brain metastasis. Cancer Res. 64:4190–4196. 2004. View Article : Google Scholar
|
|
19
|
Zhang J, Ren H, Yuan P, Lang W, Zhang L
and Mao L: Down-regulation of hepatoma-derived growth factor
inhibits anchorage-independent growth and invasion of non-small
cell lung cancer cells. Cancer Res. 66:18–23. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang J and Mao L: SiRNA targeting
hepatoma-derived growth factor (HDGF) inhibits growth of non-small
cell lung cancer in xenograft models. Tumor Biology 35: Emerging
Molecules, Mechanisms, and Models. Proc Amer Assoc Cancer Res.
47:abstract #5135. 2006.
|
|
21
|
Zhang J, Qi J, Guo Y, Guo Y, Fu W, Zhou B,
Wu G, Han L and He A: Aberrant expression of HDGF and its
prognostic values in surgically resected non-small cell lung
cancer. Zhongguo Fei Ai Za Zhi. 211–218. 2011.(In Chinese).
|
|
22
|
Besse B and Le Chevalier T: Adjuvant
chemotherapy for non-small-cell lung cancer: a fading effect? J
Clin Oncol. 26:5014–5017. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Douillard JY and Gauducheau CR: Adjuvant
chemotherapy for non-small-cell lung cancer: it does not always
fade with time. J Clin Oncol. 28:3–5. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhu CQ, Ding K, Strumpf F, Weir BA,
Meyerson M, Pennell N, Thomas RK, Naoki K, Ladd-Acosta C, Liu N,
Pintilie M, Der S, et al: Prognostic and predictive gene signature
for adjuvant chemotherapy in resected non-small-cell lung cancer. J
Clin Oncol. 28:4417–4424. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xie Y and Minna JD: Non-small-cell lung
cancer mRNA expression signature predicting response to adjuvant
chemotherapy. J Clin Oncol. 28:4404–4407. 2010. View Article : Google Scholar : PubMed/NCBI
|