Introduction
Pulmonary sequestration (PS) is an uncommon
congenital disease defined as a segment of lung parenchyma
separated from the tracheobronchial tree and receiving its blood
supply from a systemic artery rather than a pulmonary arterial
branch (1).
Pulmonary carcinoid tumorlet is a nodular
proliferation of neuroendocrine cells which is not larger than 5 mm
(2). It is rarely observed in
conjunction with pulmonary sequestration and pulmonary
neuroendocrine tumorlets (3). This
report presents a rare clinical case of carcinoid tumorlet in
pulmonary sequestration with bronchiectasis following breast
cancer. This study was approved by the ethics committee of Peking
University Shenzhen Hospital, China. Written informed consent was
obtained from the patient.
Case report
A 64-year-old female first presented to the
Department of Thyroid and Breast Surgery, Peking University
Shenzhen Hospital with a palpable mass in her left breast in
February 2009. The color ultrasound and mammary gland molybdenum
revealed breast cancer. The patient underwent lump resection and
rapid pathological examination revealed breast cancer, therefore
she subsequently underwent mastectomy with axillary lymph node
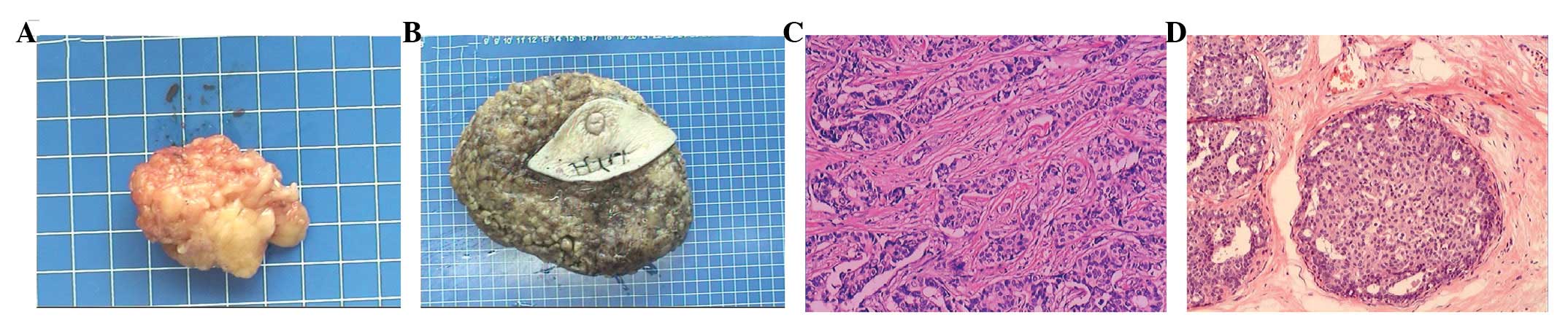
dissection. The pathological diagnosis was infiltrating ductal
carcinoma of the left breast (pT1, N1, M0, estrogen
receptor-positive, progesterone receptor-positive) in February 2009
(Fig. 1). The patient received four
cycles of adjuvant chemotherapy with epirubicin and
cyclophosphamide, followed by four cycles of docetaxel. She
completed treatment in August 2009. She underwent regular
reexamination every 6 months, and there were no signs of recurrence
or metastasis for several years.
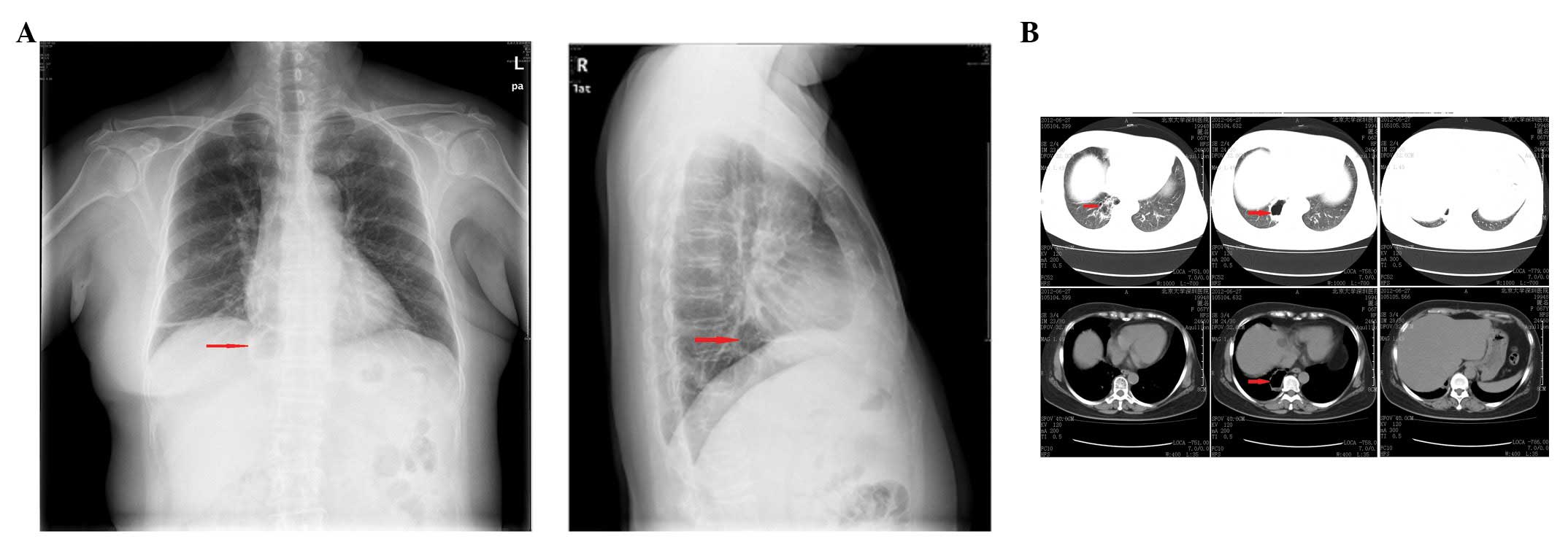
In July 2012, a chest X-ray showed a striped
high-density mass in the right lung above the diaphragmatic surface
upon routine reexamination. Chest computer tomography (CT) revealed
a cystic low-density mass of ∼2.5×4.7 cm in the right lower lung
field, as well as cystic bronchiectasis in the right lower lobe
(Fig. 2). The patient was diagnosed
with a pulmonary cyst with infection and bronchiectasis in the
right lower lobe and was treated with antibiotics. After the
infection was controlled, a right lower lobectomy was performed. In
the surgery, systemic arterial supply from the descending thoracic
aorta was observed, as well as venous drainage to the left inferior
pulmonary vein. Therefore, intralobar pulmonary sequestration was
diagnosed. The pathologists supported this diagnosis.
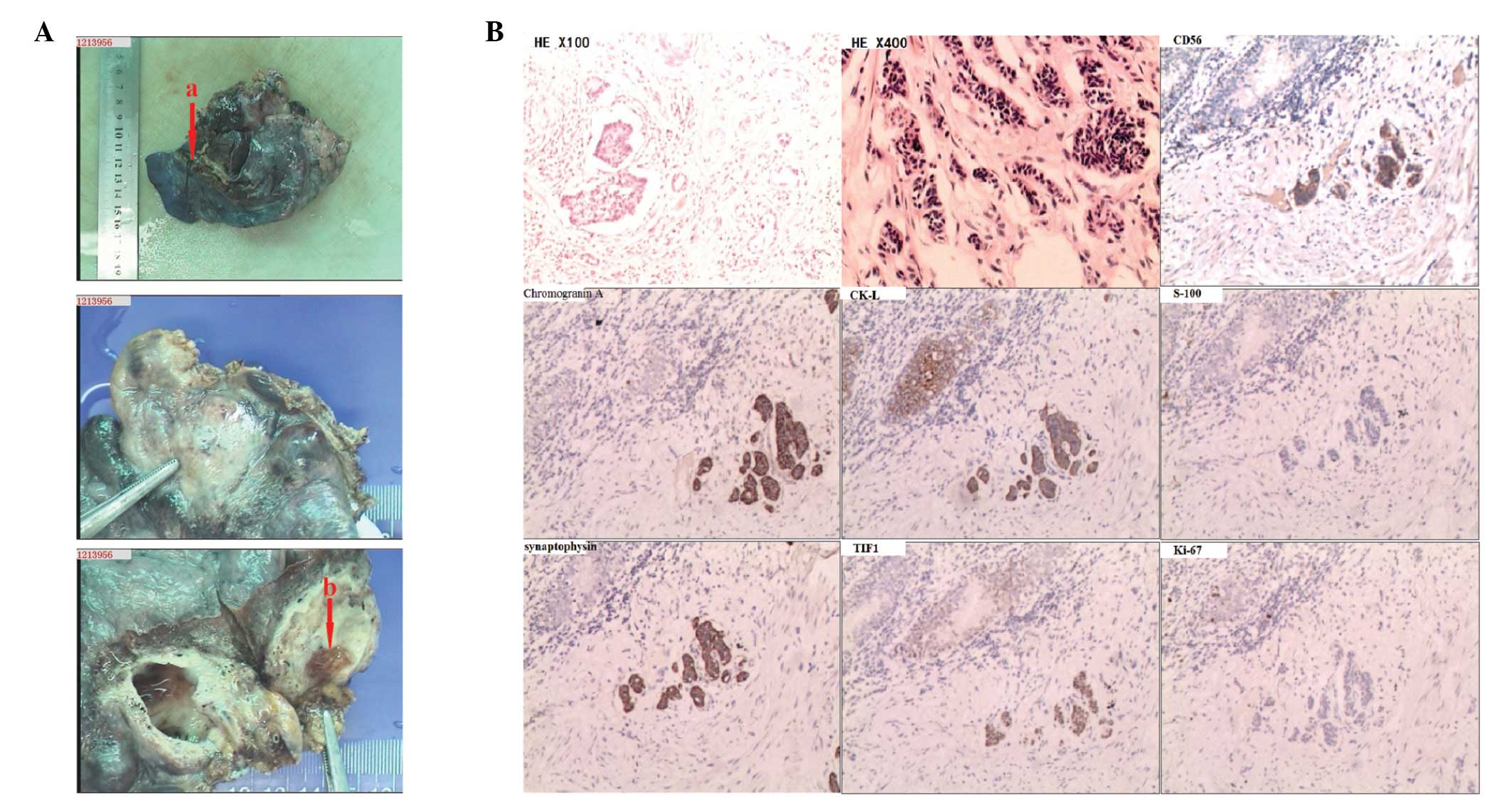
The resected mass measured 5×4×1 cm and showed
cystic space interposed by bronchial sample ciliated columnar
epithelium and cartilage structures. A nodule was identified in the
cystic wall, spanning 0.4 cm. The cells were arranged in nests and
cords without stromal reaction, and showed salt-and-pepper type
nuclear features without prominent nucleoli (Fig. 3). The immnohistochemical study
revealed that the tumor cells were positive for synaptophysin,
chromogranin A, CK-L, Ki-67 (<1% positive), TIF1 and CD56, and
negative for S-100 (Fig. 4). The nest and cord-like growth pattern
and cellular features suggested a carcinoid tumorlet.
Discussion
PS is deemed a rare congenital malformation. It
comprises 0.15–6.4% of all congenital pulmonary anomalies and is
more common in the left lung and lower lobes (4). Anatomically, it has been classically
described in two different forms: intralobar and extralobar. With
intralobar pulmonary sequestration, which comprises 75% of all PS,
the abnormal tissue is partly surrounded by normal lung, so it
shares the same pleura as normal lung tissue, while the extralobar
form is separated from normal lung tissue with its own pleura and
maintains complete anatomical and physiological separation between
the cyst and the adjacent normal lung (5). In the case presented here, the lung
parenchyma was found to share the same pleura with normal lung
tissue, and is therefore the intralobar type.
It has also been claimed that intralobar
sequestration may arise as an acquired lesion, possibly secondary
to local infection, such as bronchiectasis (6,7). In
the present case, the chest CT showed bronchiectasis in right lower
lung field and a cystic low-density mass, which was confirmed to be
PS following surgery. It was therefore assumed that the PS was
connected with bronchiectasis in this patient.
Carcinoid tumorlet is a nodular proliferation of
neuroendocrine cells and arises from focal areas of bronchial and
bronchiolar Kultschitsky cells, usually associated with diffuse
bronchiectasis and intralobar sequestration (7–10). It
is not larger than 5 mm (2).
D’Agati and Perzin found that pulmonary tumor-lets had tumor
characteristics since they could metastasize to the lymph nodes
(11). Chromogranin A, CD56 and
synaptophysin are the most useful neuroendocrine
immunohistochemical markers (12),
and low levels of Ki-67 can help to distinguish neuroendocrine from
small-cell carcinoma. In the present case the nodule was 0.4 cm,
and positive for synaptophysin, chromogranin A, CK-L, Ki-67 (<1%
positive), TIF1 and CD56, and negative for S-100, so carcinoid
tumorlet was diagnosed. Certain studies claim that carcinoid
tumorlet may be induced by hypoxia caused by bronchiectasis or
other chronic bronchitis lesions (13). In the case presented here, both
bronchiectasis and carcinoid tumorlet in PS were found in the left
lower lung field.
Hocking et al found that the risk of
developing carcinoid tumors with breast cancer is more than double
the expected rate (14); however,
the reasons for this are not understood. In the present case, the
patient was diagnosed with breast cancer before the appearance of
the carcinoid tumorlet.
In the case presented here, the patient suffered PS
and bronchiectasis as well as carcinoid tumorlet in PS following
the diagnosis of breast cancer three years earlier. It is possible
that both breast cancer and bronchiectasis are the result of a
carcinoid tumorlet, and that PS may be acquired and secondary to
occluding carcinoid tumorlet.
References
|
1
|
Corbett HJ and Humphrey GM: Pulmonary
sequestration. Paediatr Respir Rev. 5:59–68. 2004. View Article : Google Scholar
|
|
2
|
Koo CW, Baliff JP, Torigian DA, Litzky LA,
Gefter WB and Akers SR: Spectrum of pulmonary neuroendocrine cell
proliferation: diffuse idiopathic pulmonary neuroendocrine cell
hyperplasia, tumorlet, and carcinoids. AJR Am J Roentgenol.
195:661–668. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pelosi G, Zancanaro C, Sbabo L, Bresaola
E, Martignoni G and Bontempini L: Development of innumerable
neuroendocrine tumorlets in pulmonary lobe scarred by intralobar
sequestration. Immunohistochemical and ultrastructural study of an
unusual case. Arch Pathol Lab Med. 116:1167–1174. 1992.
|
|
4
|
Savic B, Birtel FJ, Tholen W, Funke HD and
Knoche R: Lung sequestration: report of seven cases and review of
540 published cases. Thorax. 34:96–101. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Carter R: Pulmonary sequestration. Ann
Thorac Surg. 7:68–88. 1969. View Article : Google Scholar
|
|
6
|
Stocker JT: Sequestrations of the lung.
Semin Diagn Pathol. 3:106–121. 1986.
|
|
7
|
Dewan M, Malatani TS, Osinowo O, al-Nour M
and Zahrani ME: Carcinoid tumourlets associated with diffuse
bronchiectasis and intralobar sequestration. J R Soc Promot Health.
120:192–195. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Churg A and Warnock ML: Pulmonary
tumorlet. A form of peripheral carcinoid. Cancer. 37:1469–1477.
1976. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ranchod M: The histogenesis and
development of pulmonary tumorlets. Cancer. 39:1135–1145. 1977.
View Article : Google Scholar
|
|
10
|
Miller MA, Mark GJ and Kanarek D: Multiple
peripheral pulmonary carcinoids and tumorlets of carcinoid type,
with restrictive and obstructive lung disease. Am J Med.
65:373–378. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
D’Agati VD and Perzin KH: Carcinoid
tumorlets of the lung with metastasis to a peribronchial lymph
node. Report of a case and review of the literature. Cancer.
55:2472–2476. 1985.PubMed/NCBI
|
|
12
|
Travis WD: Advances in neuroendocrine lung
tumors. Ann Oncol. 21(Suppl 7): vii65–71. 2010.
|
|
13
|
Resl M, Král B and Simek J: Carcinoid
tumorlets and pulmonary hypoxia. Cesk Patol. 31:84–86. 1995.(In
Czech).
|
|
14
|
Hocking JA, Mitchell J, Harp M, Ejiofor J
and DiMaio JM: Risk of developing pulmonary carcinoid tumors
following breast cancer. J Clin Oncol. 28:e120252010.
|