Introduction
Hemostatic materials [e.g., Surgicel®
(oxidized regenerated cellulose)] are usually spread in general
surgery to assist in the control of capillary, venous and small
arterial hemorrhages and oozing blood when ligation, electrical
coagulation or other conventional methods of control are
impractical or ineffective (1). The
materials are often left in the surgical bed, as they are
bio-absorbable. However, retained hemostatic materials may mimic
abscesses or recurrent tumors, as inappropriate handling, marked
foreign-body reactions, chronic inflammation and infections are
able to cause foreign-body granuloma formation (2). The present study retrospectively
analyzed the case of an 83-year-old male Chinese patient who
presented with a recurrent gastrointestinal stromal tumor (GIST)
four months subsequent to surgical resection. The GIST was later
identified as an intra-abdominal foreign-body granuloma caused by
retained Surgicel residue that mimicked a local recurrent GIST. The
study was approved by the Ethics Committee of Su Bei People’s
Hospital of Jiangsu Province, Yangzhou, China. The patient
consented to the publication of this study.
Case report
An 83-year-old male Chinese patient was admitted to
the Department of Gastroenterology of Su Bei People’s Hospital of
Jiangsu Province (Yangzhou, China) due to left upper quadrant
abdominal pain lasting for 3 days. The patient complained that the
pain was accompanied by nausea and vomiting post-prandially, as
well as an intermittent low-grade fever for ∼4 months. The patient
experienced weight loss of 3 kg, but no diarrhea, constipation,
anorexia, chills or jaundice. According to the patient’s surgical
history, surgical resection for GIST had been performed four months
previously and right colon resection for ascending colon
adenocarcinoma five years previously.
At admission, the patient’s vital signs (blood
pressure, respiratory rate, temperature and heart rate) were
stable. An abdominal examination revealed a solid, firm, non-tender
mass in the left upper quadrant. The remainder of the examination
was normal.
The only abnormal laboratory parameter was an
increased neutrophil leukocyte measurement of 73.5% (normal,
42–70%). The routine laboratory parameters, including the white
blood cell count, erythrocyte sedimentation rate (ESR), C-reactive
protein (CRP), liver and pancreatic enzyme and tumor marker
[carcinoembryonic antigen (CEA), carcinoma antigen (CA)-125,
CA-199, prostate-specific antigen (PSA) and α-fetoprotein (AFP)]
levels, were all within the normal limits.
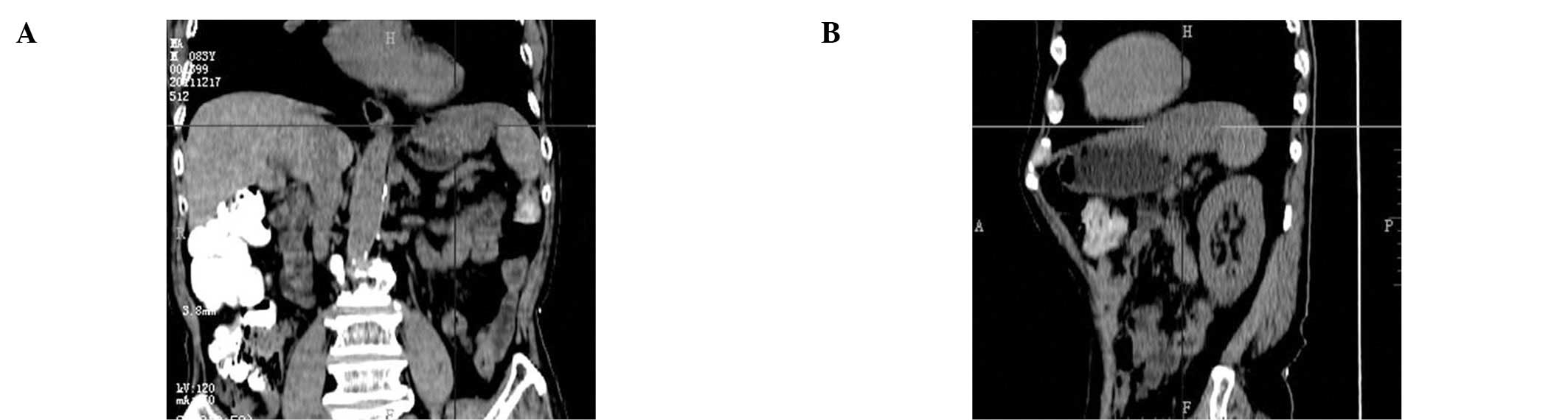
A computed tomography (CT) scan with intravenous
contrast medium revealed a heterogeneous mass, with a maximum
diameter of 8.3 cm and a density of −24 to 35 HU, located between
the stomach and spleen (Fig. 1A and
B). A positron emission tomography-computed tomography (PET/CT)
scan also revealed a lesion with an uneven, rim-shaped pattern,
rather than a global fludeoxyglucose (18F; FDG)-uptake
pattern (Fig. 2A–C). The abdominal
CT screen obtained prior to the GIST resection was reviewed and
revealed a homogeneous lesion measuring ∼4×4 cm and invading the
stomach wall (Fig. 3).
Taking into account the previous observations, an
explorative laparotomy was performed upon clinical diagnosis of a
local recurrent GIST. During the exploration, a mass wrapped in a
fibrous capsule that adhered to the gastric fundus and spleen was
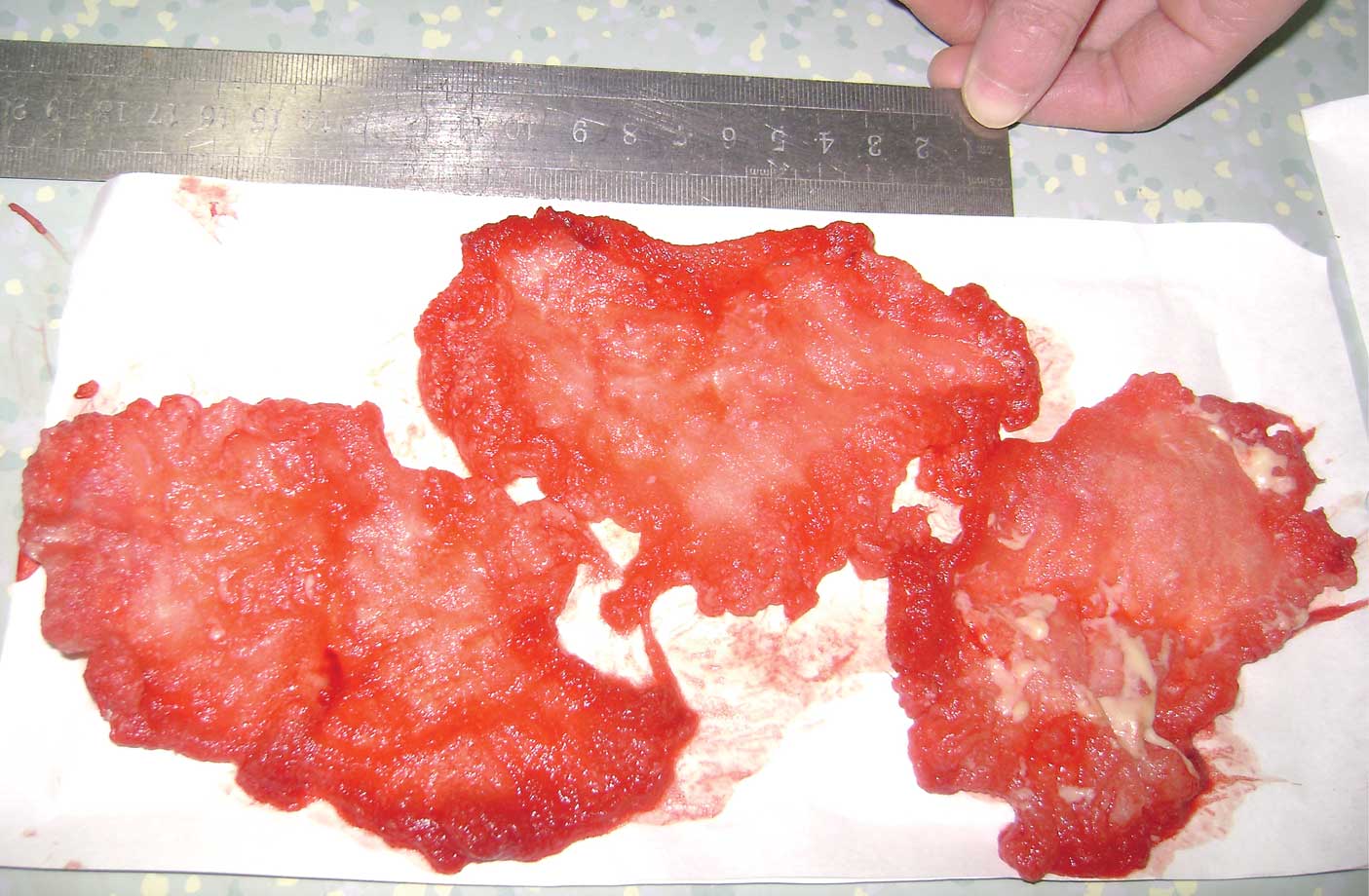
identified, with the same diameter as measured by CT. Following en
bloc removal, the mass was dissected and identified as a quantity
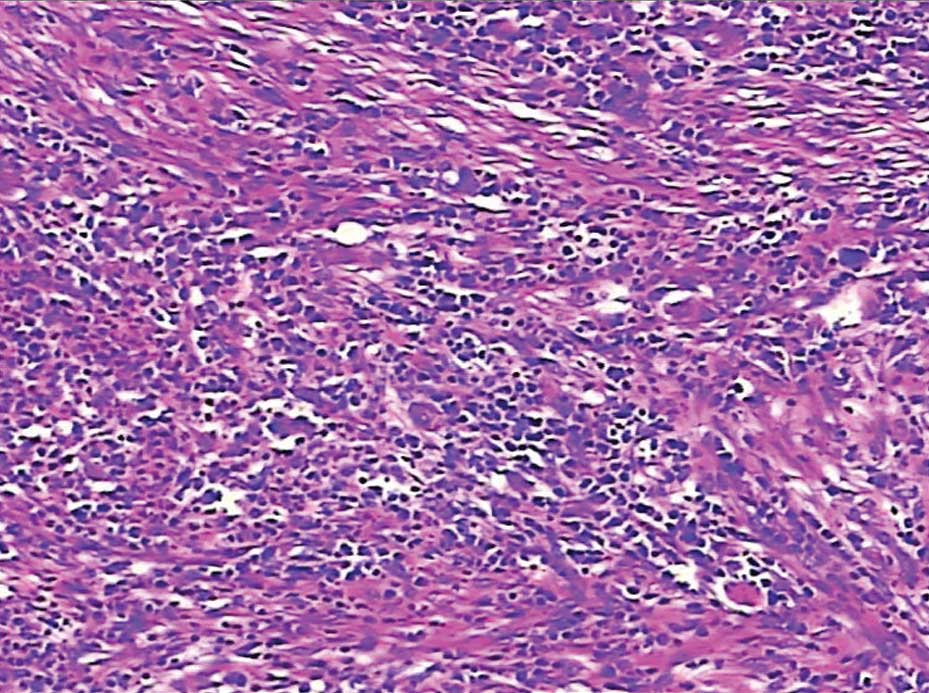
of retained local hemostat residue and pus (Fig. 4). Microscopic examination revealed a
fibrous encapsulation containing the foreign-body giant cell
reaction (Fig. 5). The surgeon who
performed the surgery on the patient four months previously was
contacted and they acknowledged that three pieces of Surgicel
(oxidized regenerated cellulose) had been implanted between the
stomach and spleen intraoperatively. The patient recovered well
post-operatively and was discharged on the 16th day. The patient
showed no signs of recurrence at an 11-month follow-up.
Discussion
Hemostat-associated masses, termed gauzomas,
gossypibomas, textilomas or even Surgicelomas (3), are actually foreign-body reactions
against retained local hemostatic residues. Unlike non-degradable
gauzes, which are occasionally accidentally left in the body
intraoperatively, bioabsorbable hemostatic agents (e.g. oxidized
regenerated cellulose) are intentionally placed in the surgical
field. Oxidized regenerated cellulose, which has been branded as
Surgicel by Ethicon (Johnson and Johnson, Somerville, NJ, USA), is
produced by decomposing wood pulp, then regenerating the cellulose
by manufacturing continuous cellulose fibers. Since it is
bioabsorbable, Surgicel is widely used to control bleeding when
ligation, electrical coagulation or other conventional hemostatic
methods are impractical or ineffective, and it is often left in the
surgical bed. However, misdiagnoses of Surgicel granulomas
mimicking recurrent tumors have resulted in secondary examinations
being reported in neurosurgeries, thoracic surgeries and
gynecological procedures (3–6). These
cases have revealed that the exact hemostasis and dissolving
mechanisms of Surgicel are often poorly understood by surgeons,
leading to its inappropriate use.
Surgicel decreases the pH of its surroundings. This
low pH has an antimicrobial effect against miscellaneous pathogenic
organisms. However, the acidic character may also increase
inflammation of the surrounding tissue and delay wound healing
(2). Hill (7) reported that a small quantity of local
hemostat enhanced infection. The dissolution of Surgicel depends on
the quantity, site of implantation and the environmental factors,
and the process may last for between two and six weeks (8). When a local hemostat is used and left
intraoperatively, surgeons often assume that is absorbed promptly.
However, the complicated degradation reactions of implanted local
hemostats include injury, blood-material interactions, provisional
matrix formation, acute or chronic inflammation, granulation tissue
development, foreign-body reactions and fibrous capsule development
(9). Histological evidence of
oxidized cellulose fibers several years subsequent to surgery has
been revealed in certain studies (5,10,11).
Moreover, cases have been reported where the Surgicel used for
hemorrhage control during a thoracotomy had passed through the
intervertebral foramen and caused spinal cord compression (3,12).
These cases indicate that only the smallest necessary quantity
should be used and any excess should be removed once the hemostatic
effect has been achieved to avoid post-operative foreign-body
granuloma formation.
A Surgiceloma may present in either the immediate or
delayed phase following surgery. The general complaints of patients
may be nausea, vomiting, a palpable mass, rectal bleeding or
changes in bowel habits. Surgiceloma may also present with a
non-specific fever, anorexia and weight loss, which may mimic a
malignant disease (13). The
present case presented with classic foreign-body granuloma induced
by retained Surgicel residues, which mimicked a local recurrent
GIST. GISTs are the most common mesenchymal neoplasms of the
gastrointestinal (GI) tract, with the most common locations being
the stomach (60%), jejunum and ileum (30%), duodenum (5%) and
colorectum (5%) (14). Among
patients with primary GIST who underwent complete resection, 7% had
an isolated local recurrence and there was a trend for tumors
>10 cm to recur earlier (15).
In the present case, the inappropriate use of Surgicel caused a
marked foreign-body reaction and a fibrous capsule surrounding the
Surgicel residues was formed. The Surgicel granuloma caused a
pyloric obstruction by a mass effect, while the persistent
inflammatory response resulted in a recurrent non-specific
fever.
O’Connor et al(16) described the CT appearances of
absorbable hemostats as mixed- or low-attenuation masses containing
focal central collections of gas. CT scans may reveal a faint
enhancement at the tumor periphery, which further contrasts with
the internal low density mass. Oto et al(17) described the appearance of oxidized
regenerated cellulose in post-operative T2-weighted magnetic
resonance (MR) images with a short relaxation time, which resulted
in a low signal intensity in the early post-operative period.
Yuh-Feng et al(18) reported
that reconstructed PET/CT images may reveal an uneven FDG uptake
(rim-shaped, rather than global, FDG-uptake pattern) at the mass
periphery in cases of gossypiboma. Together, all these imaging
observations may contribute to the identification of Surgicel
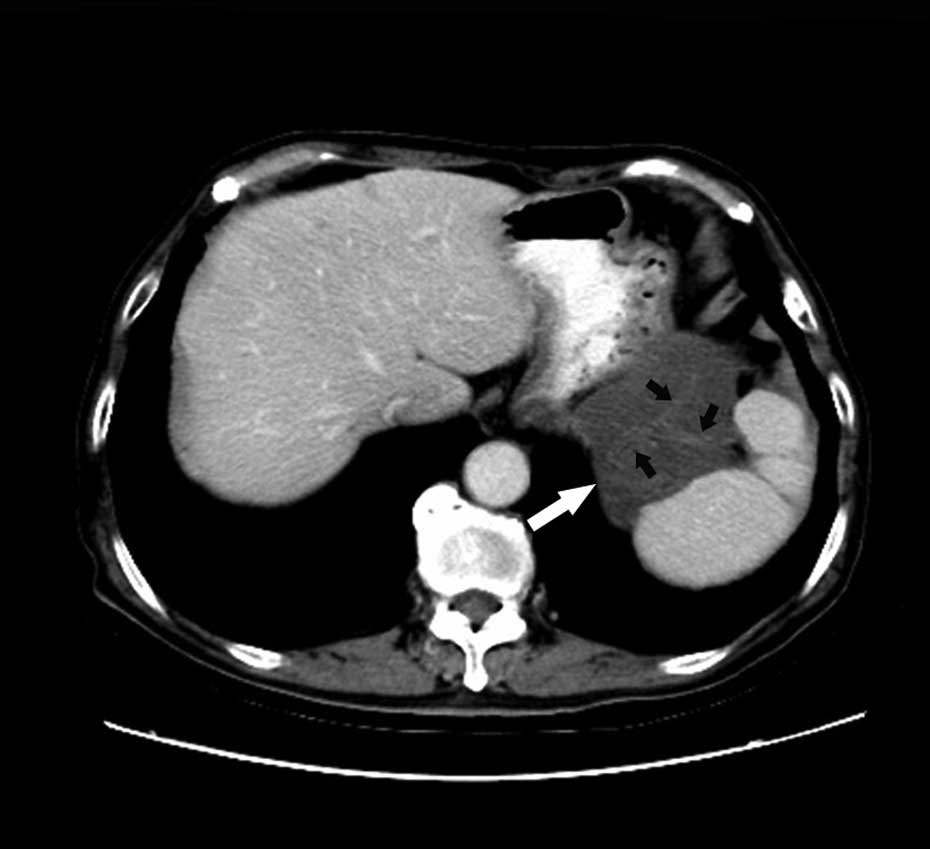
granulomas and recurrent tumors. In the present case, an enhanced
CT scan revealed an unenhanced gyrus-like mass (Fig. 6), with a heterogeneous density.
Furthermore, the PET/CT images showed a characteristic rim-shaped
uneven FDG-uptake pattern at the periphery of the ‘tumor’. These
findings should arouse suspicion with regard to the diagnosis of
foreign-body granuloma, since short-term local recurrence of GIST
is quite rare. However, in light of the patient having had two
previous surgical resections of tumors and not having received
Gleevec® chemotherapy, a diagnosis of recurrent GIST was
made pre-operatively.
In conclusion, Surgicel granulomas are uncommon and
mostly cause surgeons to provide an inaccurate diagnosis. Surgicel
granuloma should be included in the differential diagnosis of new
or recurrent soft-tissue masses detected in patients with a history
of prior surgery.
References
|
1
|
Loescher AR and Robinson PP: The effect of
surgical medicaments on peripheral nerve function. Br J Oral
Maxillofac Surg. 36:327–332. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tomizawa Y: Clinical benefits and risk
analysis of topical hemostats: a review. J Artif Organs. 8:137–142.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Banerjee T and Goldschmidt K:
‘Surgiceloma’ manifested as cauda equina syndrome. South Med J.
91:481–483. 1998.
|
|
4
|
Sandhu GS, Elexpuru-Camiruaga JA and
Buckley S: Oxidized cellulose (Surgicel) granulomata mimicking
tumour recurrence. Br J Neurosurg. 10:617–619. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Igari T, Iwaya F, Abe T, et al: A case of
foreign body granuloma after aortic valve replacement. Kyobu Geka.
43:550–552. 1990.(In Japanese).
|
|
6
|
Deger RB, LiVolsi VA and Noumoff JS:
Foreign body reaction (gossypiboma) masking as recurrent ovarian
cancer. Gynecol Oncol. 56:94–96. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hill GB: Enhancement of experimental
anaerobic infections by blood, hemoglobin, and hemostatic agents.
Infect Immun. 19:443–449. 1978.PubMed/NCBI
|
|
8
|
Frantz VK: Absorbable cotton, paper and
gauze: (oxidized cellulose). Ann Surg. 118:116–126. 1943.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Anderson JM, Rodriguez A and Chang DT:
Foreign body reaction to biomaterials. Semin Immunol. 20:86–100.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ibrahim MF, Aps C and Young CP: A foreign
body reaction to Surgicel mimicking an abscess following cardiac
surgery. Eur J Cardiothorac Surg. 22:489–490. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tomizawa Y, Endo M, Kitamura M, et al:
Coronary artery bypass graft stenosis suspected to be due to
hemostatic agents: a case report. Kyobu Geka. 44:764–766. 1991.(In
Japanese).
|
|
12
|
Brodbelt AR, Miles JB, Foy PM and Broome
JC: Intraspinal oxidised cellulose (Surgicel) causing delayed
paraplegia after thoracotomy - a report of three cases. Ann R Coll
Surg Engl. 84:97–99. 2002.PubMed/NCBI
|
|
13
|
Gawande AA, Studdert DM, Orav EJ, et al:
Risk factors for retained instruments and sponges after surgery. N
Engl J Med. 348:229–235. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Patil DT and Rubin BP: Gastrointestinal
stromal tumor: advances in diagnosis and management. Arch Pathol
Lab Med. 135:1298–1310. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
DeMatteo RP, Lewis JJ, Leung D, et al: Two
hundred gastrointestinal stromal tumors: recurrence patterns and
prognostic factors for survival. Ann Surg. 231:51–58. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
O’Connor AR, Coakley FV, Meng MV and
Eberhardt SC: Imaging of retained surgical sponges in the abdomen
and pelvis. AJR Am J Roentgenol. 180:481–489. 2003.PubMed/NCBI
|
|
17
|
Oto A, Remer EM, O’Malley CM, et al: MR
characteristics of oxidized cellulose (Surgicel). AJR Am J
Roentgenol. 172:1481–1484. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yuh-Feng T, Chin-Chu W, Cheng-Tau S and
Min-Tsung T: FDG PET CT features of an intraabdominal gossypiboma.
Clin Nucl Med. 30:561–563. 2005. View Article : Google Scholar : PubMed/NCBI
|