Introduction
Chronic neutrophilic leukemia (CNL) is a rare
disorder characterized by a persistently elevated leukocyte count
due to an increase in the number of mature neutrophils with a high
neutrophil alkaline phosphatase (NAP) score, raised serum levels of
vitamin B12 and uric acid, the absence of the Philadelphia (Ph)
chromosome and hepatosplenomegaly, when a situation capable of
inducing a reactive leukemoid reaction, such as underlying
infectious disease or neoplasia, does not exist (1). These features, together with the lack
of eosinophilia, basophilia or monocytosis, and the absence of
BCR-ABL transcripts, distinguish CNL from chronic myeloid leukemia
(CML), atypical CML and chronic myelomonocytic leukemia, as defined
by the French-American-British (FAB) Cooperative Group (2). Unlike CML, no characteristic clonal
chromosomal or molecular markers have been confirmed. The present
study reports a case of CNL involving the deletion of chromosome
17, which, to the best of the authors’ knowledge, has not been
previously reported. The study was approved by the Ethics Committee
of the First Affliated Hospital of Harbin Medical University,
Harbin, China. Written informed consent was obtained from the
patient’s son.
Case report
A 61-year-old male patient presented a history of
upper abdomen heaviness and fatigue for one month in April 2010.
All systems appeared normal when examined, with the exception of an
enlarged spleen 5 cm below the costal margins with hardening, clear
boundaries, poor mobility and no tenderness. A complete blood count
showed hemoglobin at 136 g/l and a leukocyte count of
52.1×109/l, with a differential count of 79% stab and
segmented neutrophils and 21% lymphocytes. The platelet count was
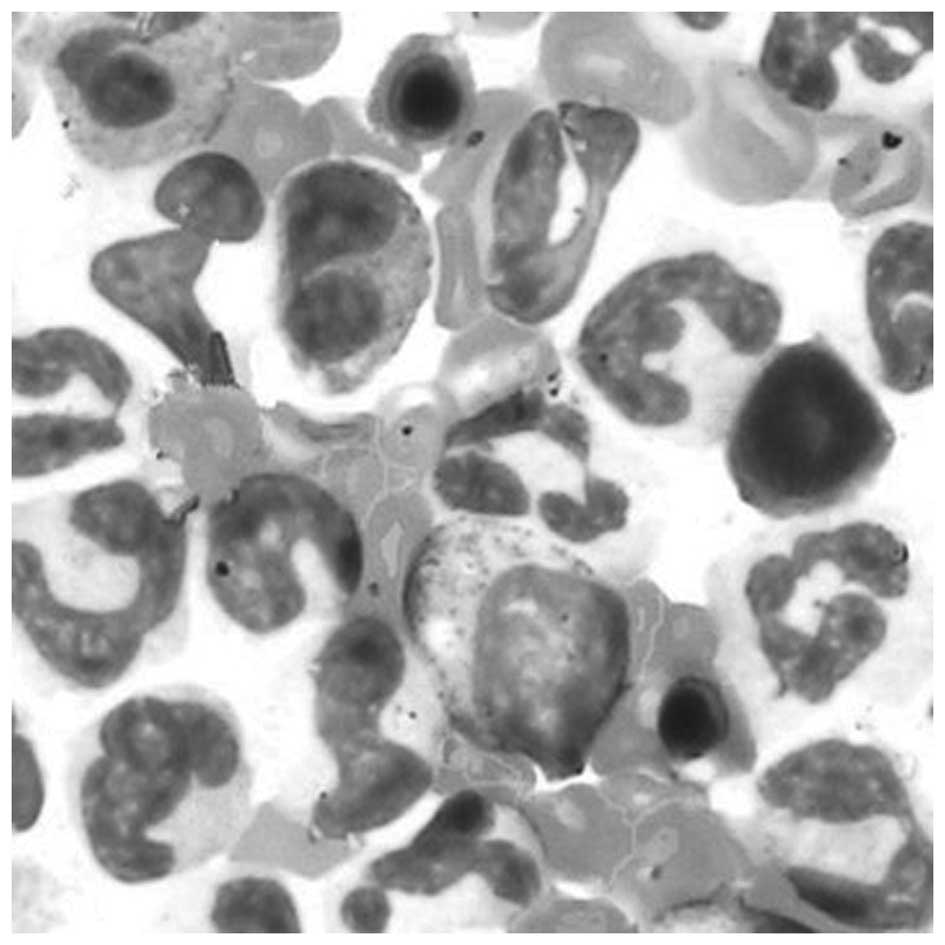
100×109/l. An aspirated bone marrow specimen was
extremely hypercellular with marked myeloid hyperplasia which was
predominantly mature neutrophilic expansion (Fig. 1). The myeloid-erythroid ratio was
4.5/1. Biochemical analyses were normal with the exception of
significant increases in serum vitamin B12 (2,000 pg/ml),
creatinine (108.8 μmol/l) and neutrophil alkaline
phosphatase (NAP) (361 U/l; normal range 180–250 U/l). Molecular
genetic analysis did not reveal somatic mutations in the JAK2 and
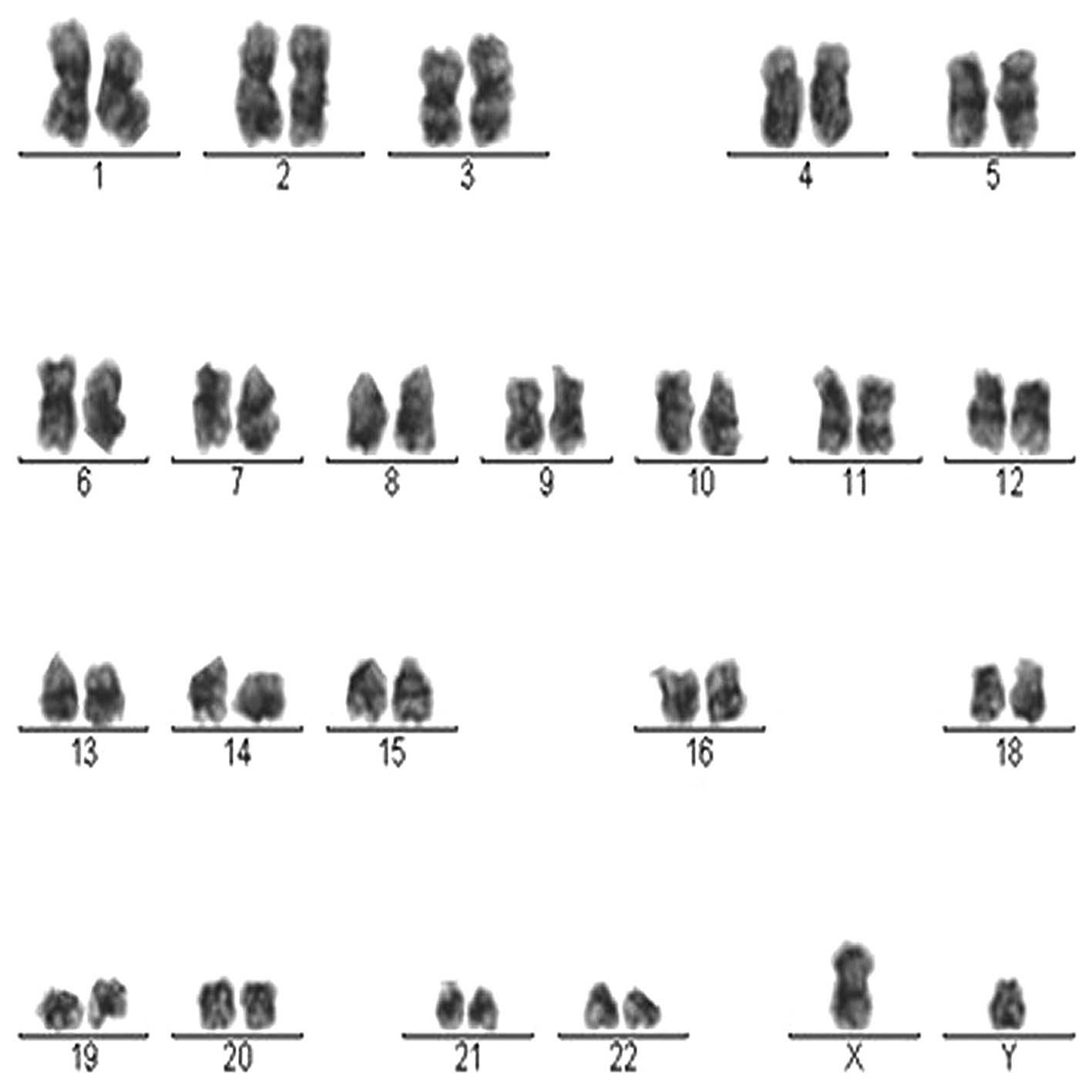
BCR-ABL fusion genes. Chromosome karyotype analysis showed a result
of 42, XY, -17, -17 in all 20 metaphase spreads (Fig. 2), while the Ph chromosome was not
detected. Thus, the patient was diagnosed with CNL associated with
the absence of chromosome 17. The patient was discharged and
received 3 mg homoharringtonine daily for 15 days. The neutrophil
count gradually declined to a normal level and physical examination
results were normal with no splenomegaly. Two weeks later, the
patient complained of left upper quadrant discomfort. The patient’s
spleen had enlarged to 12 cm below the left costal margin and his
white blood cell count increased to 40.8×109/l. The
patient has since been undergoing maintenance therapy with
hydroxyurea. In addition, the patient’s leukocyte count has been
stabilized at ≤30×109/l. At present, the patient has
remained well on subsequent follow-up visits for 31 months since
the initial diagnosis of CNL.
Discussion
Despite CNL being first reported in 1920 (3), the steering committee of the World
Health Organization (WHO) Classification of Neoplastic Diseases
only acknowledged CNL as a distinct myeloproliferative disorder in
2001 (4). The clinical and
laboratory findings of the patient in the present study
corresponded to the WHO classification criteria for the diagnosis
of CNL (5), so a diagnosis of CNL
was made. The disease appears to predominantly afflict older
individuals with a 2:1 male to female ratio and an overall median
survival of 30 months (6). The
clinical course is heterogeneous, with a definite risk of mortality
due to blastic transformation (4).
The clonal nature of CNL has been the subject of
controversy (7) as it may be
heterogenous from case to case (8).
Cytogenetic studies have identified various karyotypic
abnormalities in CNL to date, including a missing chromosome 2
replaced by a marker chromosome (9), trisomy 8 (10), trisomy 21 (11), trisomy of chromosome 9 and deletion
20(q) (12), deletion of 11q23
(13) and deletion of the entire
long arm of chromosome 20 (14).
The present patient exhibited the deletion of chromosome 17 in CNL,
which has not been reported previously. Human chromosome 17 has
been implicated in a wide range of human genetic diseases (15). For example, the tumor suppressor
gene p53 is located on 17p13.1. Herrera et al(16) reported that aneuploidy of chromosome
17 and deletion at the 17p13.1 locus of the TP53 gene were genetic
alterations observed often in solid tumors. p53 somatic alterations
are detected in ∼50% of human cancers (17), including cancer of the colon,
stomach, breast and esophagus. These findings suggest that deleted
tumor suppressor genes, such as p53 in chromosome 17, may be
associated with the development of CNL.
The present patient exhibited a chromosomal
abnormality which has not previously reported in connection to CNL.
At present, R banding and conventional karyotyping analysis have
identified numerous cases of numerical and structural abnormalities
of chromosome 17, including chromosome 17 polysomy in metastatic
breast cancer (18), isochromosome
17q in acute promyeloblastic leukemia (19), ring 17 chromosome in flecked retina
(20), prenatal diagnosis of
trisomy 17 mosaicism (21) and
monosomy 17 in CML (18).
Consequently, chromosome 17 is notable among the human chromosomes
in a number of respects.
A standard therapy for CNL remains to be defined.
The successful use of splenic irradiation, splenectomy,
interferon-alpha and oral cytoreductive agents, such as busulfan
and hydroxyurea, aid in the control of the high white cell counts
and splenomegaly, but are by no means curative. Bone marrow
transplantation may be an option for younger patients with a
suitable donor (22). The present
patient refused to undergo a bone marrow transplant due to his
economic status and old age. The patient appeared to have a
steadily poorer response to treatment with homoharringtonine.
However, the patient has exhibited a prolonged stable phase with
oral hydroxyurea treatment, although there is a definite risk of
mortality from leukemic transformation or progressive, refractory
neutrophilic leukocytosis.
Although the WHO classification reports a variable
prognosis, there are certain studies suggesting that the
progression of CNL is extremely rapid and the prognosis is poor
(23,24). Three-quarters of patients succumb to
the disease within two years, mainly due to cerebral bleeding
(25), the pathogenesis of which
remains unclear. In summary, abnormalities in chromosome 17 occur
infrequently in leukemia and to the best of the authors’ knowledge,
paired deletion involving chromosome 17 has not been previously
reported in CNL patients. Further studies are necessary to
investigate the clonality, molecular pathogenesis and optimal
therapy of CNL.
Acknowledgements
The present study was supported in
part by grants from the National Natural Science Foundation of
China (No. 81001051), Program for New Century Excellent Talents in
Heilongjiang Province (No. 1252-NCET-014) and Heilongjiang
Provincial Natural Science Foundation of China (No. QC2010019).
References
|
1
|
You W and Weisbrot IM: Chronic
neutrophilic leukemia: report of two cases and review of the
literature. Am J Clin Pathol. 72:233–242. 1979.PubMed/NCBI
|
|
2
|
Bennett JM, Catovsky D, Daniel MT, et al:
The chronic myeloid leukaemias: guidelines for distinguishing
chronic granulocytic, atypical chronic myeloid, and chronic
myelomonocytic leukaemia. Proposals by the French-American-British
Cooperative Leukaemia Group. Br J Haematol. 87:746–754. 1994.
View Article : Google Scholar
|
|
3
|
Tuohy EL: A case of splenomegaly with
polymorphonuclear neutrophil hyperleukocytosis. Am J Med Sci.
160:18–24. 1920. View Article : Google Scholar
|
|
4
|
Elliott MA, Dewald GW, Tefferi A and
Hanson A: Chronic neutrophilic leukemia (CNL): a clinical,
pathologic and cytogenetic study. Leukemia. 15:35–40. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Elliott MA, Hanson CA, Dewald GW, et al:
WHO-defined chronic neutrophilic leukemia: a long-term analysis of
12 cases and a critical review of the literature. Leukemia.
19:313–317. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sai P, Kalavar M, Raval M, et al: A case
of chronic neutrophilic leukemia with novel chromosomal
abnormalities. Clin Adv Hematol Oncol. 2:543–545. 2004.PubMed/NCBI
|
|
7
|
Böhm J, Kock S, Schaefer HE and Fisch P:
Evidence of clonality in chronic neutrophilic leukaemia. J Clin
Pathol. 56:292–295. 2003.
|
|
8
|
Yamamoto K, Nagata K, Kida A and Hamaguchi
H: Acquired gain of an X chromosome as the sole abnormality in the
blast crisis of chronic neutrophilic leukemia. Cancer Genet
Cytogenet. 134:84–87. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tanzer J, Harel P, Boiron M and Bernard J:
Cytochemical and cytogenetic findings in a case of chronic
neutrophilic leukemia of mature cell type. Lancet. 1:387–388. 1964.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Orazi A, Catoretti G and Sozzi G: A case
of chronic neutrophilic leukemia with trisomy 8. Acta Hematol.
81:148–151. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hasle H, Olesen G, Kerndrup G, et al:
Chronic neutrophil leukaemia in adolescence and young adulthood. Br
J Haematol. 94:628–630. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Di Donato C, Croci G, Lazzari S, et al:
Chronic neutrophilic leukemia: description of a new case with
karyotypic abnormalities. Am J Clin Pathol. 85:369–371.
1986.PubMed/NCBI
|
|
13
|
Terré C, Garcia I, Bastie JN, et al: A
case of chronic neutrophilic leukemia with deletion (11)(q23).
Cancer Genet Cytogenet. 110:70–71. 1999.PubMed/NCBI
|
|
14
|
Matano S, Nakamura S, Kobayashi K, et al:
Deletion of the long arm of chromosome 20 in a patient with chronic
neutrophilic leukemia: cytogenetic findings in chronic neutrophilic
leukemia. Am J Hematol. 54:72–75. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lupski JR: Genomic disorders: structural
features of the genome can lead to DNA rearrangements and human
disease traits. Trends Genet. 14:417–422. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Herrera JC, Isaza LF, Ramírez JL, et al:
Detection of chromosome 17 aneuploidy and TP53 gene deletion in a
broad variety of solid tumors by dual-color fluorescence in
situhybridization (FISH). Biomedica. 30:390–400. 2010.(In
Spanish).
|
|
17
|
Soussi T: The p53 tumor suppressor gene:
from molecular biology to clinical investigation. Ann NY Acad Sci.
910:121–137. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hayashi N, Nakamura S, Yagata H, et al:
Chromosome 17 polysomy in circulating tumor cells in patients with
metastatic breast cancer: a case series. Int J Clin Oncol.
16:596–600. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim M, Lee SA, Park HI, et al: Two
distinct clonal populations in acute promyelocytic leukemia, one
involving chromosome 17 and the other involving an isochromosome
17. Cancer Genet Cytogenet. 197:185–188. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kumari R, Black G, Dore J and Lloyd IC:
Flecked retina associated with ring 17 chromosome. Eye (Lond).
23:2134–2135. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Witters I, Cannie M and Fryns JP: Prenatal
diagnosis of trisomy 17 mosaicism. Prenat Diagn. 27:677–678. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Goto H, Hara T, Tsurumi H, et al: Chronic
neutrophilic leukemia with congenital Robertsonian translocation
successfully treated with allogeneic bone marrow transplantation in
a young man. Intern Med. 48:563–567. 2009. View Article : Google Scholar
|
|
23
|
Noguchi T, Ikeda K, Yamamoto K, et al:
Severe bleeding tendency caused by leukemic infiltration and
destruction of vascular walls in chronic neutrophilic leukemia. Int
J Hematol. 74:437–441. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Piliotis E, Kutas G and Lipton JH:
Allogeneic bone marrow transplantation in the management of chronic
neutrophilic leukemia. Leuk Lymphoma. 43:2051–2054. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Böhm J and Schaefer HE: Chronic
neutrophilic leukaemia: 14 new cases of an uncommon
myeloproliferative disease. J Clin Pathol. 55:862–864.
2002.PubMed/NCBI
|