Introduction
Breast cancer is the most common type of cancer in
females, accounting for 29% of estimated new cancer cases and 14%
of estimated cancer-related mortalities (1). Although breast cancer became curable
during the last decade, individuals treated for breast carcinoma
remain at risk of local or distant recurrence indefinitely,
depending on various factors. Local recurrence is commonly
considered a first sign of treatment failure. This may occur
contralaterally (on the other breast) or ipsilaterally (on the same
side as the initial cancer, either in the remaining breast tissue
or on the chest wall). Approximately 30% of patients experience
local recurrence of breast cancer (2). Traditional options for the treatment
of local recurrence following mastectomy include surgery, radiation
therapy (RT), chemotherapy, hormonal therapy or a combination of
modalities (3). However, the
utility of chemotherapy following locoregional treatment for
isolated locoregional recurrence still remains controversial, and
has been investigated in a joint study by the International Breast
Cancer Study Group (IBSCG), the National Surgical Adjuvant Breast
and Bowel Project (NSABP) and the Breast International Group (BIG)
(4). The recurrence of tumors
invading the sternum and ribs following mastectomy is relatively
rare, but treatment problems are frequently encountered (5). The best treatment option is surgical
excision; however, the resection of the sternum and ribs
occasionally causes defects of the thoracic wall, resulting in
secondary complications and influencing the normal cardio-pulmonary
function (6). Many studies have
reported various techniques using different materials for chest
wall reconstruction (7–10) and recently titanium mesh has emerged
as a promising and reliable bone substitute (11–13).
In this report, a local recurrence of invasive
ductal breast carcinoma which invaded the sternum and several ribs
is described. A titanium mesh was used for chest wall construction,
which is not often reported in the field of breast cancer
treatment. This study was approved by the Ethics Committee of
Capital Medical University, Beijing, China Written informed consent
was obtained from the patient for the publication of this
study.
Case report
A 46-year-old Asian female who had not entered
menopause presented for routine follow-up in April 2012. She had
previously undergone a left modified radical mastectomy followed by
8 courses of CMF chemotherapy and tamoxifen treatment for 3 years,
for an estrogen receptor (ER) (+++)-positive, progesterone receptor
(PR) (+++)-positive, T1N0M0 invasive ductal breast carcinoma. On
routine follow-up with clinical and radiological examination the
patient was found to be free of any recurrence.
Physical examination revealed a 2×2-cm nodule in the
location of the mastectomy scar that was palpable and fixed to the
underlying tissue. Subsequent ultrasound demonstrated a 3-cm
hypoechoic nodule that corresponded to the mammographic
abnormality. Positron emission tomography (PET) showed no evidence
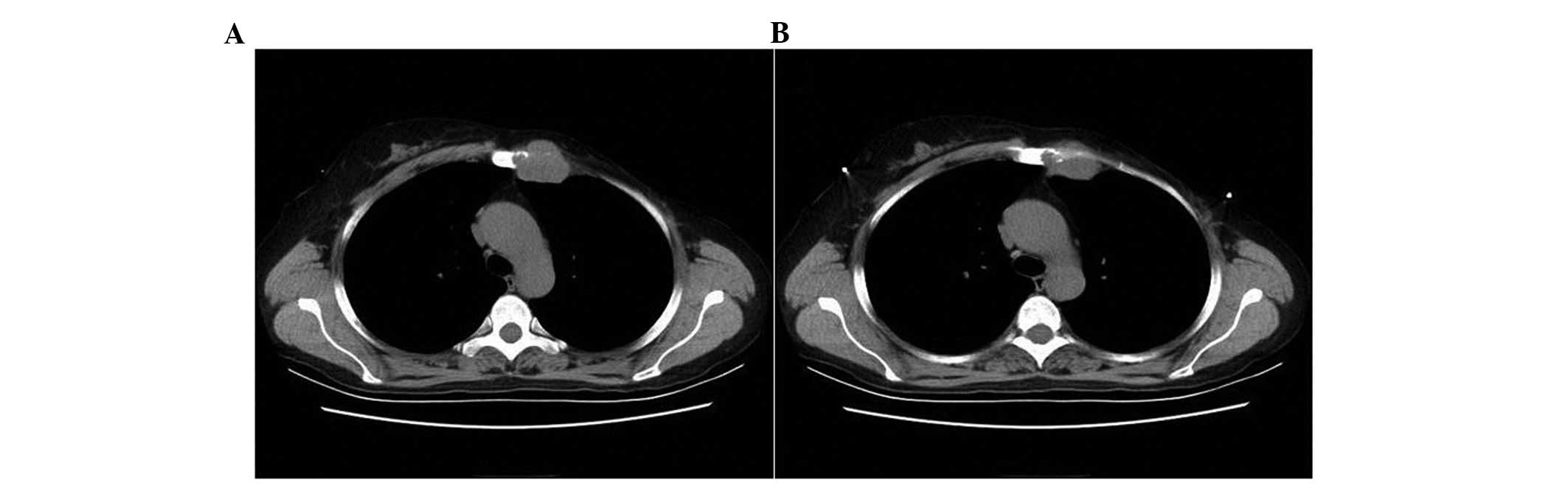
of distant metastases, while chest computed tomography (CT)
identified bone destruction of the left sternum and a 3.4×3.5-cm
mass which intruded into the left chest cavity (Fig. 1). Ultrasound-guided core needle
biopsy of the mass revealed an invasive ductal carcinoma that was
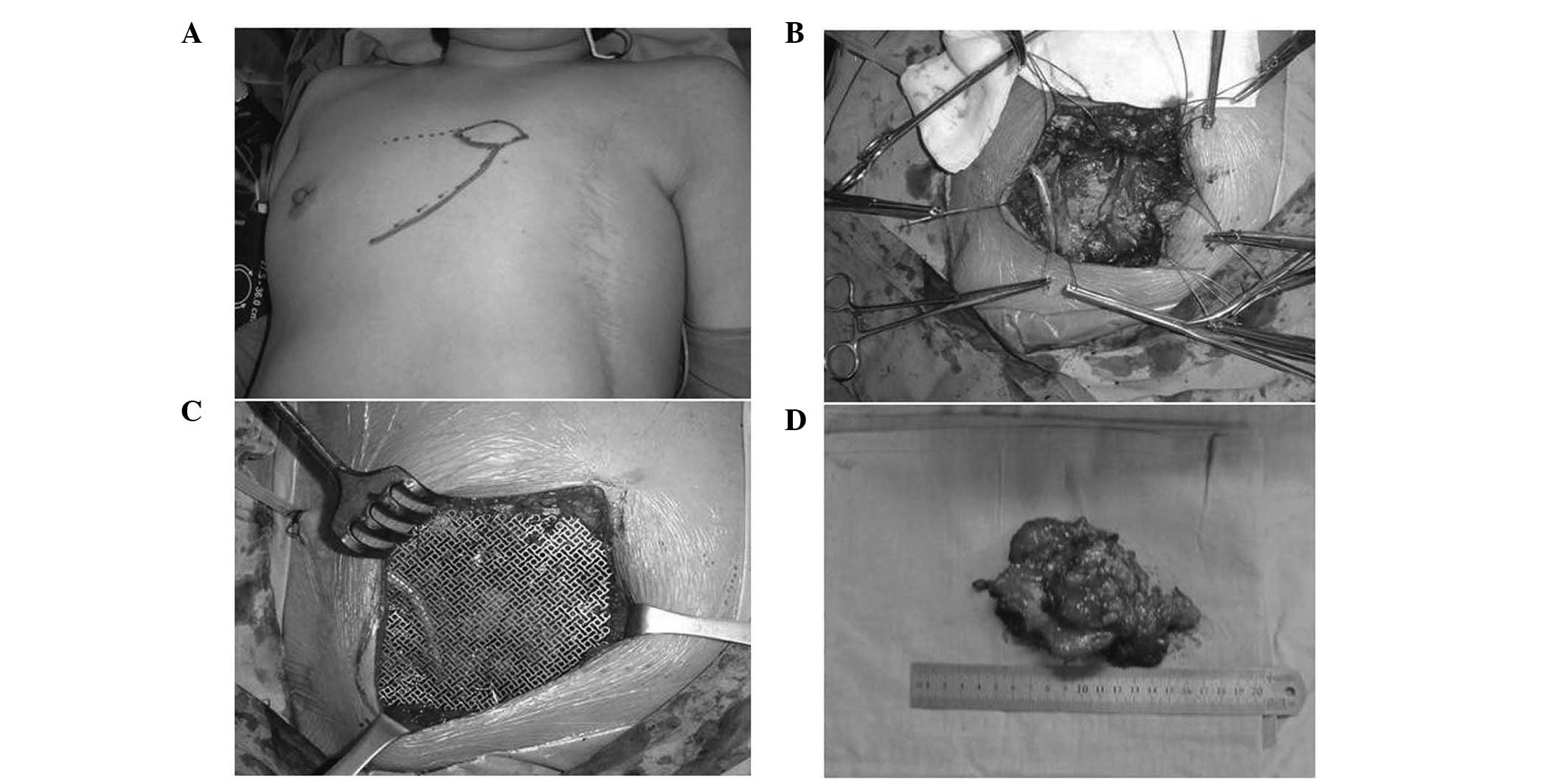
ER (+, 90%) and PR (+, 80%)-positive. Considering the local
recurrence of breast carcinoma invading the chest cavity along with
bone destruction, the patient underwent extended lumpectomy with
partial excision of the sternum and ribs (second, third and fourth)
and a titanium mesh was implanted for chest wall reconstruction
(Fig. 2). The final pathology
showed invasive ductal carcinoma invading the adjacent ribs and
soft tissues, and all margins were negative by >10 mm.
Immunostaining for ER and PR were both positive, while the
expression of human growth factor receptor 2 (HER-2) was negative.
Following the guidelines of the National Comprehensive Cancer
Network (NCCN), the patient chose to undergo local extended-field
RT and endocrine treatment following surgery.
Discussion
Local recurrence of breast cancer may occur as an
isolated event or concomitantly with systemic spread of disease.
Isolated local recurrences following breast conserving therapy are
highly curable by salvage mastectomy. However, local recurrence
after mastectomy may present as a first sign of widespread
metastatic disease. Therefore, patients suffering local recurrence
following mastectomy should undergo a workup for metastatic
disease. In the absence of distant metastases, surgical excision
followed by RT to the involved chest wall and regional lymphatics
is the standard treatment approach (3,14).
Fodor et al reported that certain factors such as
disease-free interval, initial tumor and lymph node stage, patient
age, extent and histology of the recurrent tumor are associated
with the risk of cause-specific mortality following local
recurrence in patients with early-stage invasive breast cancer
(15).
Chest wall breast cancer recurrence following
mastectomy is considered a difficult disease to treat, and usually
involves multiple cutaneous and subcutaneous tumor nodules.
Recurrences invading deeper chest wall structures similar to the
present case are far less prevalent (16). Many studies have shown that
postmastectomy RT is beneficial in reducing chest wall recurrence,
particularly in cases with larger tumors and axillary lymph node
involvement (5,17). Surgical excision followed by RT has
been acknowledged as the best treatment option. This was found to
be related with prognosis in cases where there is no metastasis and
when the recurrence develops more than 24 months after mastectomy
and patients are initially node-negative (6). According to the large randomized
trials being performed by the International Breast Cancer Study
Group (IBCSG), the National Surgical Adjuvant Breast and Bowel
Project (NSABP) and the Breast International Group (BIG), the use
of chemotherapy following radical local treatment of locoregional
relapse remains controversial (4).
In the present case, the oncologists did not recommend chemotherapy
for postoperative treatment considering the recurrence of invasive
ductal breast cancer after 8 complete courses of CMF
chemotherapy.
Furthermore, local recurrence involving the deep
chest wall results can result in thoracic defects generated by
surgery, and chest wall reconstruction is sometimes required
(18). Large anterior and lateral
resections render intrathoracic structures vulnerable to external
impact and necessitate rigid reconstructions. These include a
number of techniques using alloplastic materials such as methyl
methacrylate-based customized plates, neo-ribs, osteosynthesis
systems or a dedicated prosthesis (19). Currently, as a novel bone substitute
for reconstruction, titanium mesh merits attention. Titanium mesh
has been acknowledged as highly versatile and easy to implement. It
lacks the problems associated with other materials and is
substantial enough to provide the support required. In particular,
titanium mesh does not interfere with postoperative imaging such as
X-ray, CT and magnetic resonance imaging (MRI). Additionally, it
has been concluded that the dosimetric impact of titanium mesh is
minimal and does not require modification in radiotherapy treatment
parameters (20). Kim et al
found that a coronal flap with frontal craniotomy and orbital roof
reconstruction using titanium mesh provided good functional and
cosmetic results (21). Fabre et
al reported that following sternectomy for cancer,
reconstruction with a titanium rib bridge system had low morbidity
and permitted a rapid return to baseline pulmonary mechanics
(13). In the present case, the
titanium mesh was used for chest wall reconstruction as the left
sternum and three ribs were resected. The surgery went smoothly and
the prognosis of the patient and treatment outcome will be followed
up.
In summary, local recurrence of breast cancer
involving deep chest walls is relatively rare. According to the
guidelines, surgical excision followed by RT is the standard
treatment. The beneficial effect of chemotherapy after radical
local treatment of locoregional relapse remains contraversial, and
for this reason chemotherapy is not recommended. Recently, titanium
mesh has emerged as a promising and reliable bone substitute, and
was applied in the present case. The prognosis of the patient will
be followed up and the effectiveness of the titanium mesh implant
for chest wall reconstruction will be evaluated.
Acknowledgements
The study was supported by the Beijing
Municipal Health System Academic Leaders of High-Level Health
Personnel Program (No. 2011-2-28).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar
|
|
2
|
Pennery E: The role of endocrine therapies
in reducing risk of recurrence in postmenopausal women with hormone
receptor-positive breast cancer. Eur J Oncol Nurs. 12:233–243.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Halyard MY, Wasif N, Harris EE, et al: ACR
appropriateness criteria local-regional recurrence (LR) and salvage
surgery. Am J Clin Oncol. 35:178–182. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wapnir IL, Aebi S, Gelber S, et al:
Progress on BIG 1-02/IBCSG 27-02/NSABP B-37, a prospective
randomized trial evaluating chemotherapy after local therapy for
isolated locoregional recurrences of breast cancer. Ann Surg Oncol.
15:3227–3231. 2008. View Article : Google Scholar
|
|
5
|
Sersa G, Cufer T, Paulin SM, Cemazar M and
Snoj M: Electrochemotherapy of chest wall breast cancer recurrence.
Cancer Treat Rev. 38:379–386. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chagpar A, Meric-Bernstam F, Hunt KK, et
al: Chest wall recurrence after mastectomy does not always portend
a dismal outcome. Ann Surg Oncol. 10:628–634. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dell’amore A, Nizar A, Dolci G, et al:
Sternal resection and reconstruction for local recurrence of breast
cancer using the sternal allograft transplantation technique. Heart
Lung Circ 2012. (Epub ahead of print).
|
|
8
|
Noble J, Sirohi B, Ashley S, Ladas G and
Smith I: Sternal/parasternal resection for parasternal local
recurrence in breast cancer. Breast. 19:350–354. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chapelier AR, Missana MC, Couturaud B, et
al: Sternal resection and reconstruction for primary malignant
tumors. Ann Thorac Surg. 77:1001–1007. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Koppert LB, van Geel AN, Lans TE, van der
Pol C, van Coevorden F and Wouters MW: Sternal resection for
sarcoma, recurrent breast cancer, and radiation-induced necrosis.
Ann Thorac Surg. 90:1102–1108. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gabrielli MF, Monnazzi MS, Passeri LA,
Carvalho WR, Gabrielli M and Hochuli-Vieira E: Orbital wall
reconstruction with titanium mesh: retrospective study of 24
patients. Craniomaxillofac Trauma Reconstr. 4:151–156. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Luo JM, Liu B, Xie ZY, et al: Comparison
of manually shaped and computer-shaped titanium mesh for repairing
large frontotemporoparietal skull defects after traumatic brain
injury. Neurosurg Focus. 33:E132012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fabre D, El Batti S, Singhal S, et al: A
paradigm shift for sternal reconstruction using a novel titanium
rib bridge system following oncological resections. Eur J
Cardiothorac Surg. 42:965–970. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Willner J, Kiricuta IC and Kölbl O:
Locoregional recurrence of breast cancer following mastectomy:
always a fatal event? Results of univariate and multivariate
analysis. Int J Radiat Oncol Biol Phys. 37:853–863. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fodor J, Major T, Polgar C, Orosz Z,
Sulyok Z and Kásler M: Prognosis of patients with local recurrence
after mastectomy or conservative surgery for early-stage invasive
breast cancer. Breast. 17:302–308. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ragaz J, Olivotto IA, Spinelli JJ, et al:
Locoregional radiation therapy in patients with high-risk breast
cancer receiving adjuvant chemotherapy: 20-year results of the
British Columbia randomized trial. J Natl Cancer Inst. 97:116–126.
2005.
|
|
17
|
Van der Pol CC, Van Geel AN,
Menke-Pluymers MB, Schmitz PI and Lans TE: Prognostic factors in 77
curative chest wall resections for isolated breast cancer
recurrence. Ann Surg Oncol. 16:3414–3421. 2009.PubMed/NCBI
|
|
18
|
Thomas PA and Brouchet L: Prosthetic
reconstruction of the chest wall. Thorac Surg Clin. 20:551–558.
2010. View Article : Google Scholar
|
|
19
|
Rocco G: Overview on current and future
materials for chest wall reconstruction. Thorac Surg Clin.
20:559–562. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rakowski JT, Chin K and Mittal S: Effects
of titanium mesh implant on dosimetry during gamma knife
radiosurgery. J Appl Clin Med Phys. 13:38332012.PubMed/NCBI
|
|
21
|
Kim JW, Bae TH, Kim WS and Kim HK: Early
reconstruction of orbital roof fractures: clinical features and
treatment outcomes. Arch Plast Surg. 39:31–35. 2012. View Article : Google Scholar : PubMed/NCBI
|