Introduction
Early lung cancer detection is an important approach
for reducing disease mortality rates. Low-dose spiral computed
tomography (CT) scanning has demonstrated effectiveness in
detecting early-stage peripheral lung cancers (1–3).
However, the CT yield for early-stage central airway cancers is
relatively poor (4) and its costs
appear to limit wider implementation (5). Autofluorescence bronchoscopy (AFB) has
been shown to be highly sensitive for the detection of early-stage
(micro-) invasive carcinoma and pre-invasive lesions in the central
airways (6–10). Its high false-positive rate and
rather invasive approach hamper its wider use as a cost-effective
screening tool (8). The detection
of molecular biomarkers that are representative of the disease
state in less or non-invasively collected biological fluids, such
as blood or sputum, may be an alternative or addition to this
imaging technique and may improve the cost-effectiveness of
screening.
Analysis of free-circulating plasma DNA (cpDNA)
levels is a non-invasive method that has shown the potential to
detect patients with lung cancer (11–15).
Significantly higher cpDNA levels have been demonstrated in
patients with invasive lung cancer, independently of tumor stage,
as compared with controls (13,14).
However, it is currently not known whether cpDNA levels are
increased in subjects with high-grade pre-invasive squamous
endobronchial lesions or if cpDNA level quantification may be of
value as a marker of invasive growth in these subjects. This
information may contribute to our knowledge of cpDNA quantification
as a potential non-invasive screening tool for identifying
individuals at the highest risk of developing lung squamous cell
carcinoma (SqCC). In the present study, we evaluated cpDNA levels
in a cohort of subjects with AFB-visualized pre-invasive
endobronchial lesions comprising the full spectrum of premalignant
squamous disease, relative to patients with clinically overt lung
SqCC and cancer-free, healthy controls. The current study aimed to
assess whether cpDNA quantification was able to discriminate among
these subgroups.
Subjects and methods
Study subjects
Peripheral blood was collected with informed consent
from i) subjects with pre-invasive squamous endo-bronchial lesions;
ii) patients diagnosed with invasive lung SqCC (stage I–IV); and
iii) cancer-free, healthy individuals. Characteristics of the study
population are shown in Table I.
Pre-invasive endobronchial lesions were visualized by AFB in
subjects at risk of lung cancer on the basis of smoking habits
(>20 pack years), chronic obstructive pulmonary disease (COPD),
signs/symptoms and/or history of lung or head and neck cancer, but
without clinically overt lung cancer (16). For this study, the subjects were
selected in such a way that the AFB-visualized lesions included the
full spectrum of pre-invasive squamous endobronchial disease and
that variables that may potentially confound the analysis, such as
gender (P=0.49), age (P=0.14), smoking status (P=0.61), number of
pack years (P=0.42), COPD status (P=0.56) and storage time of
plasma specimens (P=0.19), were kept similar to those of the cancer
cases. Staging of lung cancers was performed according to the 6th
edition of the TNM classification system of malignant tumors
(17), and histology according to
the 2004 IASLC/WHO histological classification system of
pre-invasive and invasive squamous lesions of the bronchus
(18). This study followed the
ethical guidelines of the Institutional Review Board.
 | Table ICharacteristics of study
population. |
Table I
Characteristics of study
population.
| Characteristic | Subjects with
pre-invasive squamous endobronchial lesions | Patients diagnosed
with invasive lung SqCC | Cancer-free,healthy
individuals |
|---|
| Gender,
male:female | 14:6 | 9:7 | 11:5 |
| Age (years), median
(range) | 62 (46–71) | 63 (50–81) | 56 (28–87) |
| COPD,
yes:no:unknown | 10:9:1 | 11:4:1 | 5:9:2 |
| Smoking status,
C:F:N | 8:12:0 | 7:8:0a | 2:4:9a |
| No. of pack years,
median (range) | 40 (22–120) | 40 (15–60)a | 39
(20–46)a,b |
Sample handling and DNA isolation
Peripheral blood was processed within 1 h of
collection. The plasma component was carefully separated by
centrifuging twice at 3,000 rpm for 10 min at room temperature. The
plasma specimens were stored in 1-ml aliquots at −80°C until use.
DNA isolation was performed essentially as described previously
(13). Briefly, DNA was isolated
from a plasma aliquot using the Qiagen QIAamp DNA mini kit
(Westburg, Leusden, The Netherlands) according to the
manufacturer’s instructions for blood and body fluids. Specimens
were spiked with plasmid DNA (pHPV16) prior to DNA isolation to
control for DNA extraction efficiency.
Plasma DNA quantification
cpDNA levels were determined in quadruplicate by
means of quantitative real-time PCR amplification of the human
Fra-1 gene on the ABI/Prism 7300 Real-Time PCR system (Applied
BioSystems, Nieuwerkerk a/d IJssel, The Netherlands) and further
quantified using a standard calibrator curve of human placental DNA
(19). HPV16-specific quantitative
real-time PCR to specifically quantify the plasmid DNA was also
performed on the DNA isolates to assess DNA extraction efficiency
(20).
Statistical analysis
cpDNA quantification assays were performed in a
blinded fashion, and afterwards the results were correlated with
disease category. For analysis, the pre-invasive lesions graded as
hyperplasia, squamous metaplasia, mild dysplasia and moderate
dysplasia were categorized into low-grade pre-invasive disease
(LGD), and severe dysplasia and carcinoma in situ (CIS) were
categorized into high-grade pre-invasive disease (HGD). Statistical
analyses were performed using the SPSS Statistics v17.0 software
package (SPSS, Inc., Chicago, IL, USA). Differences in the
frequencies of patient characteristics between groups were examined
using Fisher’s exact and Mann-Whitney U tests. Median plasma DNA
levels between groups were compared using non-parametrical
Kruskal-Wallis testing.
Results
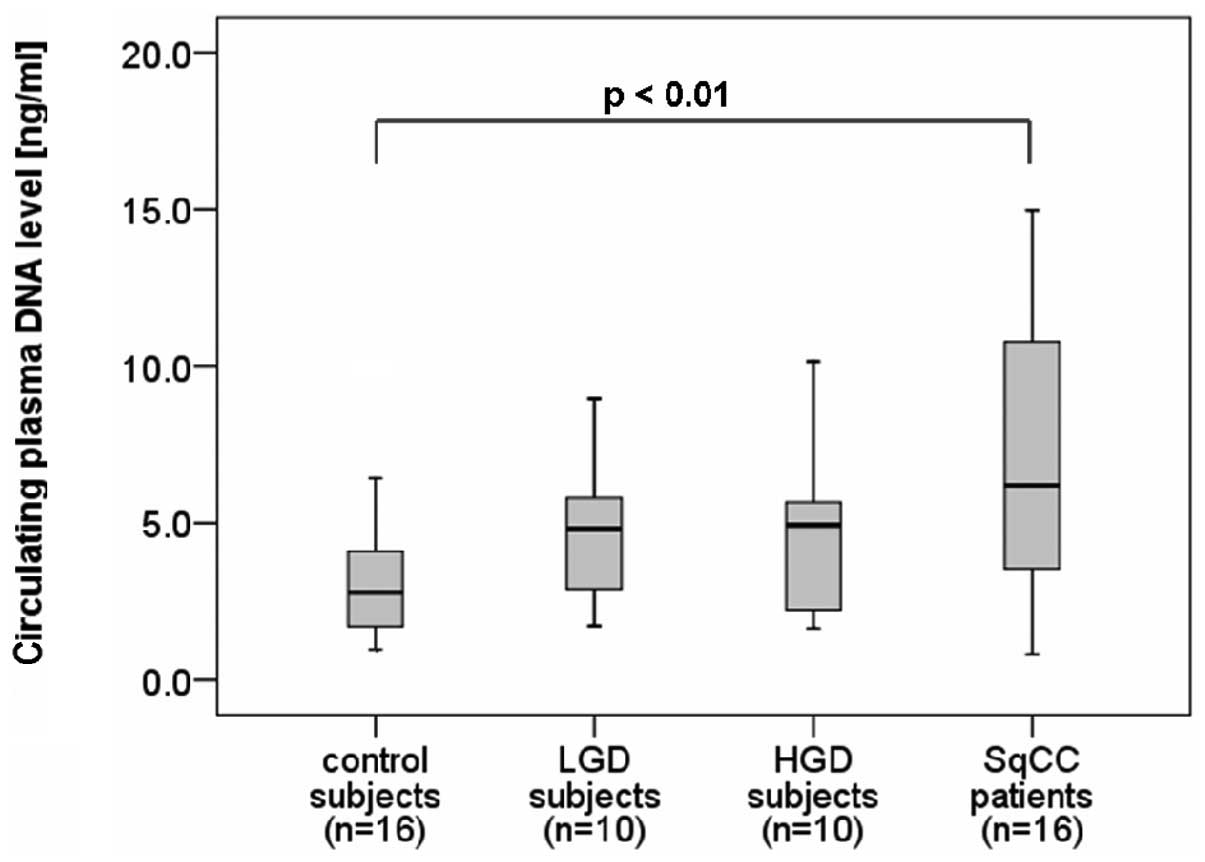
A total of 52 plasma samples were used for
comparison of cpDNA levels from i) 20 subjects with AFB-visualized
preinvasive endobronchial lesions (LGD, n=10; HGD, n=10); ii) 16
patients with clinically overt, invasive SqCC (stage I, n=7; stage
III, n=6; stage IV, n=3); and iii) 16 cancer-free, healthy
individuals (controls). The patients with clinically overt lung
cancers demonstrated significantly higher levels of cpDNA (median,
6.2 ng/ml; range, 0.8–77.6 ng/ml) as compared with the controls
(P<0.01; Fig. 1). By contrast,
cpDNA levels were unable to discriminate at-risk subjects with
pre-invasive lesions (median, 4.9 ng/ml; range, 1.6–10.2 ng/ml)
from controls (median, 2.8 ng/ml; range, 1.0–10.1 ng/ml), neither
in the case of LGD (P=0.10) nor HGD (P=0.29). Moreover, the cpDNA
levels in subjects who were diagnosed with HGD (median, 4.9 ng/ml;
range, 1.6–10.2 ng/ml) were highly similar to those in subjects
diagnosed with LGD (median, 4.8 ng/ml; range, 1.7–9.0 ng/ml;
P=0.85). Of note, 3 of the 10 individuals presenting with HGD at
the time of peripheral blood sampling were diagnosed with invasive
lung cancer within a follow-up period of 6 months, and none of them
had elevated cpDNA levels at the pre-invasive stage; their cpDNA
levels were 1.6, 2.2 and 4.8 ng/ml.
Discussion
The results of our study suggest that cpDNA levels
are not increased during the pre-invasive stages of lung squamous
carcinogenesis. Although cpDNA levels were significantly higher in
clinically overt lung cancer, consistent with previous data
(12–15), none of the subjects with
pre-invasive lesions, neither LGD nor HGD, could be discriminated
from controls on the basis of their cpDNA level. Our findings
suggest that the quantification of cpDNA in plasma may not be a
useful approach for identifying subjects with high-grade
pre-invasive lesions of lung SqCC, nor for prognostication in
potentially malignant conditions.
Sozzi et al(21,22)
suggested that the release of DNA in plasma is correlated with the
establishment of a relatively advanced grade of interaction between
the tumor and the microenvironment. The authors demonstrated that
plasma DNA levels in patients with CT-detected lung cancer, which
particularly consist of small, early-stage adenocarcinomas, were
comparable with those of disease-free subjects, and that only
patients with clinically overt lung cancers were observed to have
markedly higher levels of cpDNA. Studies on the quantification of
cpDNA in subjects with precancerous lesions are scarce. Shukla
et al(23) evaluated cpDNA
levels in subjects with mucosal precancerous lesions (epithelial
dysplasia) of oral squamous cell carcinoma. The authors concluded
that the levels of cpDNA in subjects with oral epithelial dysplasia
were not higher compared with healthy controls, which is consistent
with our data of subjects with pre-invasive lesions of lung SqCC.
In the study by Shukla et al(23), however, cpDNA levels were also not
elevated in patients with oral SqCC, an observation that does not
agree with our data and those of previous studies (12–15).
The authors suggested this to be a property inherent to the type of
neoplasm and its dissemination characteristics, which is different
for lung cancer and oral cancer. The possibility that cpDNA
quantification may provide a fingerprint of the aggressive behavior
of different types of tumors requires further testing. This will
also be of interest within screening trials in the effort to
improve the clinical management of CT-detected lung cancer.
Furthermore, in patients with overt cancer, the abundance of cpDNA
that likely originates from the cancerous cells offers the
possibility to use this source material as a non-invasive
monitoring system for applying companion diagnostics to determine
an appropriate lung cancer treatment, as was recently shown for the
detection of epidermal growth factor receptor (EGFR) mutations for
EGFR-tyrosine kinase inhibitors (24).
The strength of the current study lies in the
confirmatory results of cpDNA levels in patients with squamous
(pre-) cancerous lesions that well complement previous results from
studies, mainly including the adenocarcinoma histotype (21,22). A
limitation of this study may be the number of pre-invasive lesions
included, particularly in light of the fact that only a small
fraction progress to SqCC (25).
However, it should be noted that the analyzed series of subjects
with pre-invasive squamous endobronchial lesions form a unique
study population that had only become available by close AFB
surveillance of large numbers of individuals at risk of lung cancer
during recent years. This reflects the important difficulties faced
in studying pre-invasive endobronchial disease, given the low
prevalence of high-grade lesions in asymptomatic individuals within
an at-risk population and the low progression rate to SqCC
(25). Collecting sufficient
biomaterials representing the full spectrum of pre-invasive
squamous endobronchial disease to investigate the study concept
requires an extensive period of close surveillance. This
underscores the uniqueness of the series examined in the present
study.
In conclusion, although the median cpDNA levels of
patients with invasive lung SqCC were significantly higher as
compared with those of healthy controls, no elevated levels of
cpDNA were observed in subjects with either LGD or HGD. cpDNA
quantification does not appear to be a prognostic marker in
potentially malignant conditions and is unlikely to be of value as
an alternative or addition to the diagnostic algorithm of AFB for
identifying patients at highest risk of developing lung cancer. Our
study highlights the need to continue research efforts aiming to
identify biomarkers that can be appplied to non- or less invasively
collected biomaterial for the early prediction of invasive cancer
in the respiratory airways to improve screening and/or diagnostic
algorithms.
Acknowledgements
This study was supported by the Dutch
Cancer Society (VU-2007-3898).
References
|
1
|
National Lung Screening Trial Research
Team; Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom
RM, Gareen IF, Gatsonis C, Marcus PM and Sicks JD: Reduced
lung-cancer mortality with low-dose computed tomographic screening.
N Engl J Med. 365:395–409. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gohagan JK, Marcus PM, Fagerstrom RM,
Pinsky PF, Kramer BS, Prorok PC, Ascher S, Bailey W, Brewer B,
Church T, Engelhard D, Ford M, Fouad M, Freedman M, Gelmann E,
Gierada D, Hocking W, Inampudi S, Irons B, Johnson CC, Jones A,
Kucera G, Kvale P, Lappe K, Manor W, Moore A, Nath H, Neff S, Oken
M, Plunkett M, Price H, Reding D, Riley T, Schwartz M, Spizarny D,
Yoffie R and Zylak C; Lung Screening Study Research Group: Final
results of the Lung Screening Study, a randomized feasibility study
of spiral CT versus chest X-ray screening for lung cancer. Lung
Cancer. 47:9–15. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Henschke CI, Naidich DP, Yankelevitz DF,
McGuinness G, McCauley DI, Smith JP, Libby D, Pasmantier M, Vazquez
M, Koizumi J, Flieder D, Altorki N and Miettinen OS: Early lung
cancer action project: initial findings on repeat screenings.
Cancer. 92:153–159. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
McWilliams A, Mayo J, MacDonald S, LeRiche
JC, Palcic B, Szabo E and Lam S: Lung cancer screening: a different
paradigm. Am J Respir Crit Care Med. 168:1167–1173. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goulart BH, Bensink ME, Mummy DG and
Ramsey SD: Lung cancer screening with low-dose computed tomography:
costs, national expenditures, and cost-effectiveness. J Natl Compr
Canc Netw. 10:267–275. 2012.PubMed/NCBI
|
|
6
|
Chen W, Gao X, Tian Q and Chen L: A
comparison of autofluorescence bronchoscopy and white light
bronchoscopy in detection of lung cancer and preneoplastic lesions:
a meta-analysis. Lung Cancer. 73:183–188. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bota S, Auliac JB, Paris C, Métayer J,
Sesboüé R, Nouvet G and Thiberville L: Follow-up of bronchial
precancerous lesions and carcinoma in situ using fluorescence
endoscopy. Am J Respir Crit Care Med. 164:1688–1693. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lam S, Kennedy T, Unger M, Miller YE,
Gelmont D, Rusch V, Gipe B, Howard D, LeRiche JC, Coldman A and
Gazdar AF: Localization of bronchial intraepithelial neoplastic
lesions by fluorescence bronchoscopy. Chest. 113:696–702. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lam S and Palcic B: Re: Autofluorescence
bronchoscopy in the detection of squamous metaplasia and dysplasia
in current and former smokers. J Natl Cancer Inst. 91:561–562.
1999. View Article : Google Scholar
|
|
10
|
Loewen G, Natarajan N, Tan D, Nava E,
Klippenstein D, Mahoney M, Cummings M and Reid M: Autofluorescence
bronchoscopy for lung cancer surveillance based on risk assessment.
Thorax. 62:335–340. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fleischhacker M and Schmidt B: Free
circulating nucleic acids in plasma and serum (CNAPS) - Useful for
the detection of lung cancer patients? Cancer Biomark. 6:211–219.
2010.PubMed/NCBI
|
|
12
|
Paci M, Maramotti S, Bellesia E, Formisano
D, Albertazzi L, Ricchetti T, Ferrari G, Annessi V, Lasagni D,
Carbonelli C, De Franco S, Brini M, Sgarbi G and Lodi R:
Circulating plasma DNA as diagnostic biomarker in non-small cell
lung cancer. Lung Cancer. 64:92–97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sozzi G, Conte D, Mariani L, Lo Vullo S,
Roz L, Lombardo C, Pierotti MA and Tavecchio L: Analysis of
circulating tumor DNA in plasma at diagnosis and during follow-up
of lung cancer patients. Cancer Res. 61:4675–4678. 2001.PubMed/NCBI
|
|
14
|
Sozzi G, Conte D, Leon M, Ciricione R, Roz
L, Ratcliffe C, Roz E, Cirenei N, Bellomi M, Pelosi G, Pierotti MA
and Pastorino U: Quantification of free circulating DNA as a
diagnostic marker in lung cancer. J Clin Oncol. 21:3902–3908. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Szpechcinski A, Dancewicz M, Kopinski P,
Kowalewski J and Chorostowska-Wynimko J: Real-time PCR
quantification of plasma DNA in non-small cell lung cancer patients
and healthy controls. Eur J Med Res. 14(Suppl 4): 237–240. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
van Boerdonk RA, Sutedja TG, Snijders PJ,
Reinen E, Wilting SM, van de Wiel MA, Thunnissen FE, Duin S, Kooi
C, Ylstra B, Meijer CJ, Meijer GA, Grünberg K, Daniels JM, Postmus
PE, Smit EF and Heideman DA: DNA copy number alterations in
endobronchial squamous metaplastic lesions predict lung cancer. Am
J Respir Crit Care Med. 184:948–956. 2011.PubMed/NCBI
|
|
17
|
Sobin LH and Wittekind C: TNM
Classification of Malignant Tumours. 6th edition. Wiley-Liss; New
York, NY: 2002
|
|
18
|
Travis WD, Brambilla E, Muller-Hermelink
KM and Harris CC: World Health Organization Classification of
Tumours: Pathology and Genetics of Tumours of the Lung, Pleura,
Thymus and Heart. IARC Press; Lyon: 2004
|
|
19
|
de Wilde J, De-Castro AJ, Snijders PJ,
Meijer CJ, Rösl F and Steenbergen RD: Alterations in AP-1 and AP-1
regulatory genes during HPV-induced carcinogenesis. Cell Oncol.
30:77–87. 2008.PubMed/NCBI
|
|
20
|
Hesselink AT, van den Brule AJ,
Groothuismink ZM, Molano M, Berkhof J, Meijer CJ and Snijders PJ:
Comparison of three different PCR methods for quantifying human
papillomavirus type 16 DNA in cervical scrape specimens. J Clin
Microbiol. 43:4868–4871. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Roz L, Verri C, Conte D, Miceli R, Mariani
L, Calabro’ E, Andriani F, Pastorino U and Sozzi G: Plasma DNA
levels in spiral CT-detected and clinically detected lung cancer
patients: a validation analysis. Lung Cancer. 66:270–271. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sozzi G, Roz L, Conte D, Mariani L,
Andriani F, Lo Vollo S, Verri C and Pastorino U: Plasma DNA
quantification in lung cancer computed tomography screening:
five-year results of a prospective study. Am J Respir Crit Care
Med. 179:69–74. 2009.PubMed/NCBI
|
|
23
|
Shukla D, Kale AD, Hallikerimath S,
Yerramalla V and Subbiah V: Can quantifying free-circulating DNA be
a diagnostic and prognostic marker in oral epithelial dysplasia and
oral squamous cell carcinoma? J Oral Maxillofac Surg. Jun 29–2012,
(Epub ahead of print).
|
|
24
|
Nakamura T, Sueoka-Aragane N, Iwanaga K,
Sato A, Komiya K, Kobayashi N, Hayashi S, Hosomi T, Hirai M, Sueoka
E and Kimura S: Application of a highly sensitive detection system
for epidermal growth factor receptor mutations in plasma DNA. J
Thorac Oncol. 7:1369–1381. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Breuer RH, Pasic A, Smit EF, van Vliet E,
Vonk Noordegraaf A, Risse EJ, Postmus PE and Sutedja TG: The
natural course of preneoplastic lesions in bronchial epithelium.
Clin Cancer Res. 11(2 Pt 1): 537–543. 2005.PubMed/NCBI
|